
Effect of Long-Term Consumption of Lactobacillus paracasei SD1 on Reducing Mutans streptococci and Caries Risk: A Randomized Placebo-Controlled Trial

Abstract
:1. Introduction
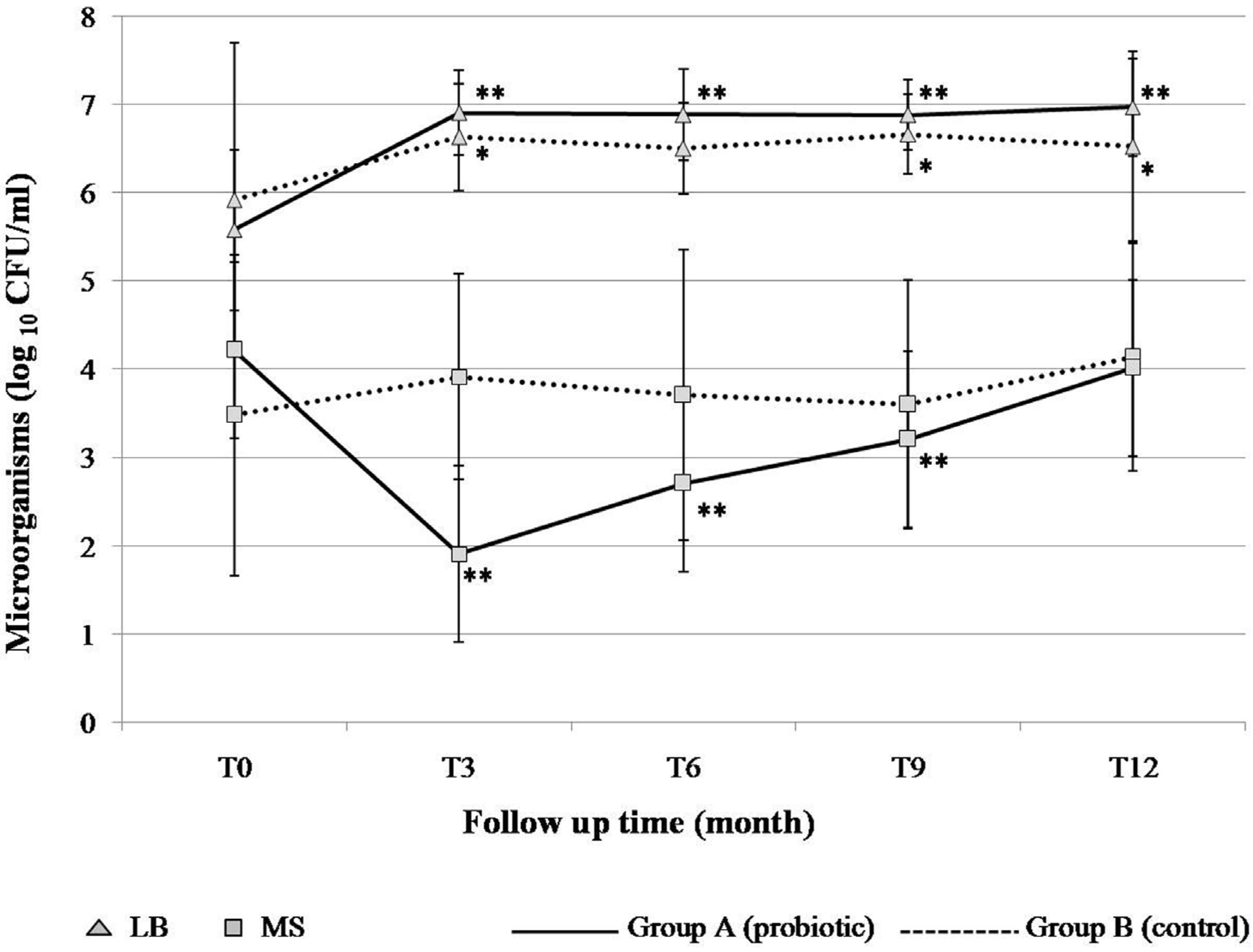
2. Results and Discussion


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Control | Probiotic |
|---|---|---|
| Age (years) | 13.13 ± 0.71 | 13.25 ± 0.73 |
| Sex: | ||
| male | 41 | 23 |
| female | 22 | 36 |
| DMFT at baseline | 0.91 ± 1.40 | 0.86 ± 1.12 |
| pH of saliva: | ||
| T0 | 7.47 ± 0.29 | 7.50 ± 0.30 |
| T3 | 7.18 ± 0.42 | 7.38 ± 0.49 |
| T6 | 7.60 ± 0.60 | 7.78 ± 0.36 |
| T9 | 7.70 ± 0.41 | 7.57 ± 0.49 |
| T12 | 7.32 ± 0.47 | 7.30 ± 0.56 |


| Dental caries | Control group | Probiotic group |
|---|---|---|
| Total: (n = 110) | ||
| DT at T0 | 0.61 ± 1.10 | 0.68 ± 0.98 |
| ∆ DT at T12 | 0.57 ± 0.95 | 0.30 ± 0.57 |
| Low caries risk: (n = 56) | ||
| DT at T0 | 0.0 | 0.0 |
| ∆ DT at T12 | 0.30 ± 0.79 | 0.35 ± 0.56 |
| High caries risk: (n = 54) | ||
| DT at T0 | 1.43 ± 1.31 | 1.26 ± 1.03 |
| ∆ DT at T12* | 0.91 ± 1.04 | 0.26 ± 0.57 |
| Dental caries | Number of children (%) with | |||
|---|---|---|---|---|
| Low caries risk (n = 56) | High caries risk (n = 54)* | |||
| Control | Probiotic | Control | Probiotic | |
| No caries increase | 25 (83.3) | 18 (69.2) | 11 (47.8) | 25(80.6) |
| Caries increase ≥ 1 | 5 (16.7) | 8 (30.8) | 12 (52.2) | 6 (19.4) |
| Total | 30 (100) | 26 (100) | 23 (100) | 31 (100) |
| OR | 0.45 | 4.55 | ||
3. Experimental Section
3.1. Subjects
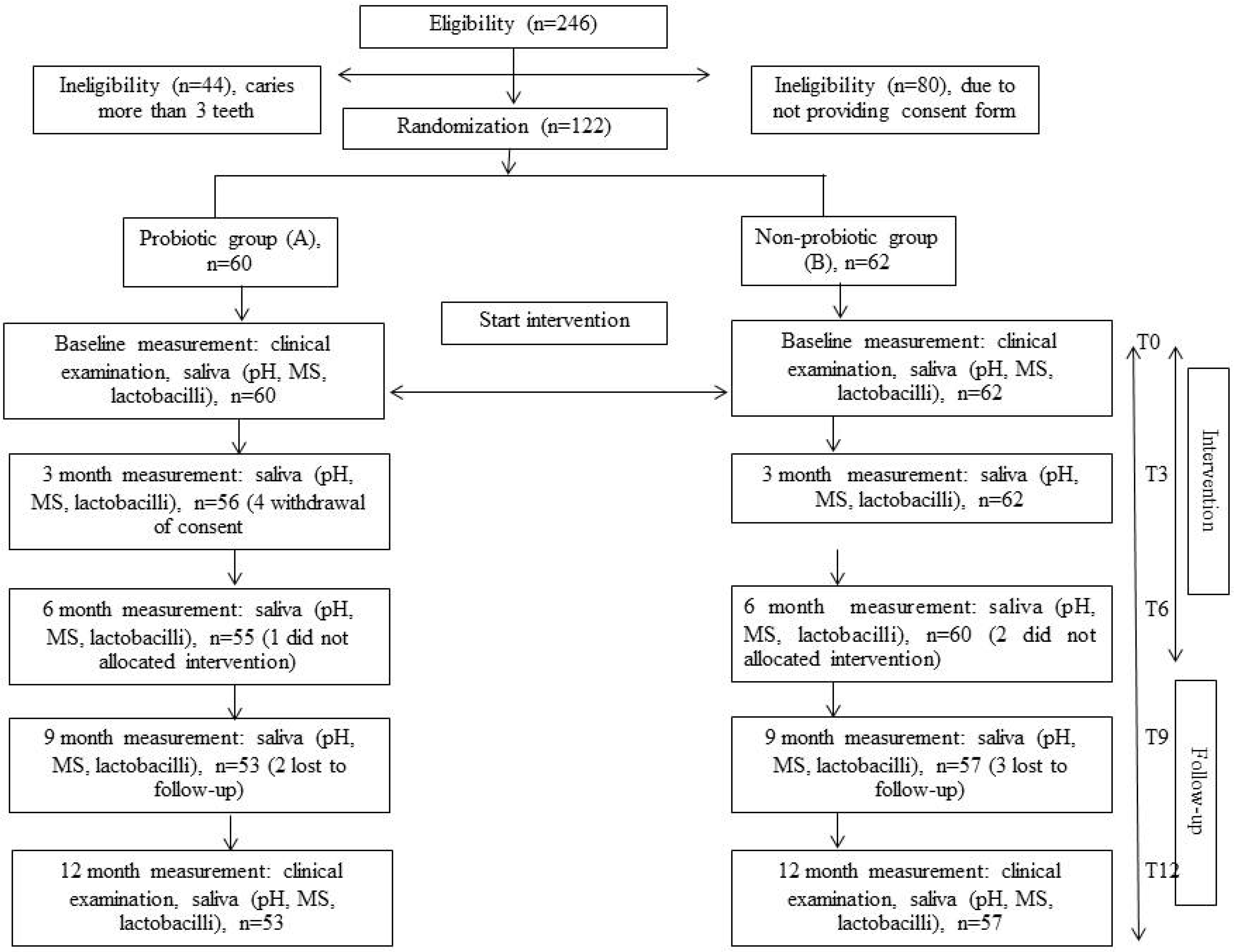
3.2. Study Design
3.3. Intervention
3.4. Oral Examination
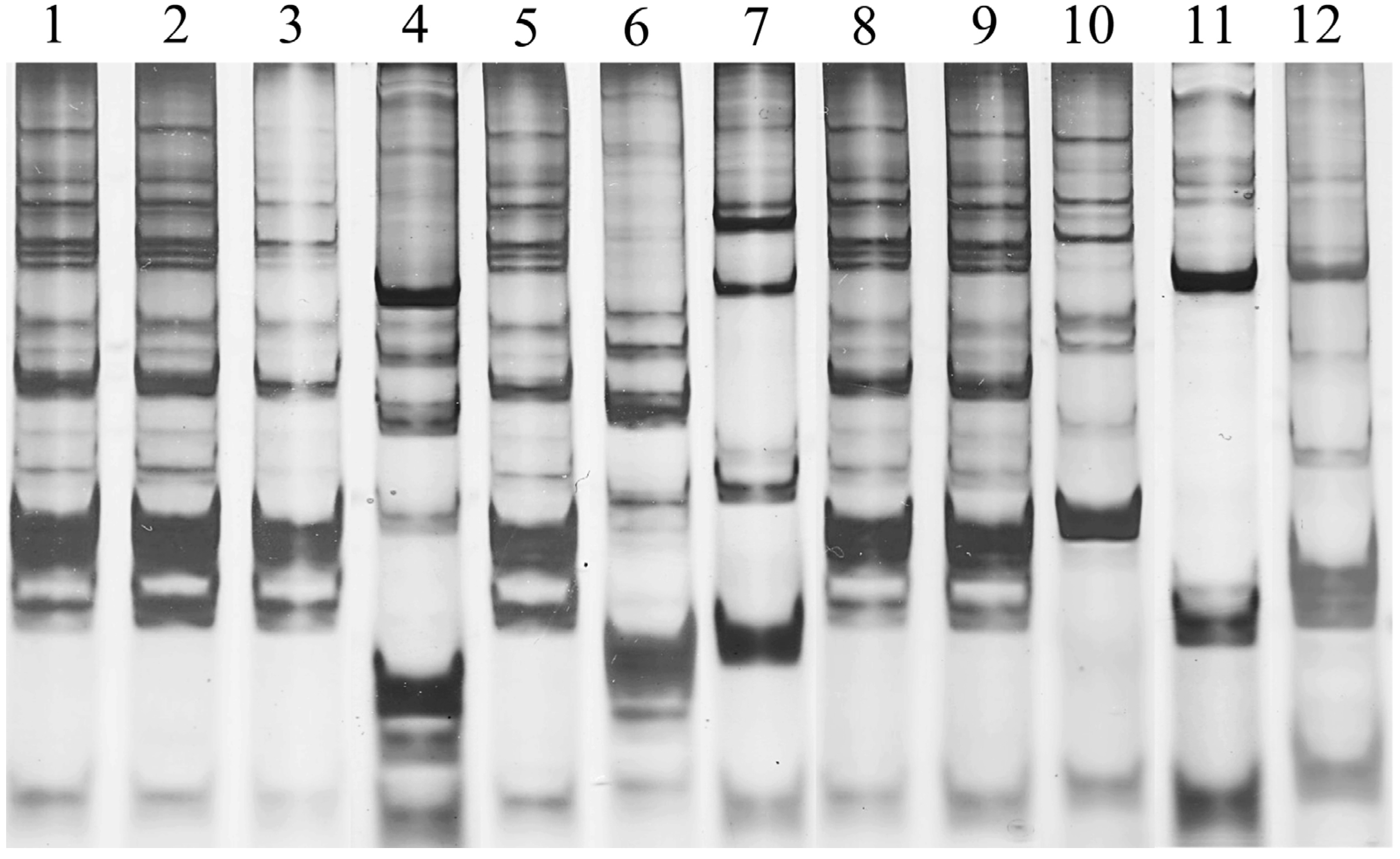
3.5. Microbial Evaluation
3.6. Analysis of Data
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Meurman, J.H.; Stamatova, I. Probiotics: contributions to oral health. Oral Dis 2007, 13, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Cagetti, M.G.; Mastroberardino, S.; Milia, E.; Cocco, F.; Lingström, P.; Campus, G. The use of probiotic strains in caries prevention: a systematic review. Nutrients 2013, 5, 2530–2550. [Google Scholar] [CrossRef] [PubMed]
- Simark-Mattsson, C.; Emilson, C.G.; Hakansson, E.G.; Jacobsson, C.; Roos, K.; Holm, S. Lactobacillus.-mediated interference of mutans streptococci in caries-free vs. caries-active subjects. Eur J. Oral Sci. 2007, 115, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Strahinic, I.; Busarcevic, M.; Pavlica, D.; Milasin, J.; Golic, N.; Topisirovic, L. Molecular and biochemical characterizations of human oral lactobacilli as putative probiotic candidates. Oral Microbiol. Immunol. 2007, 22, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Teanpaisan, R.; Piwat, S.; Dahlen, G. Inhibitory effect of oral Lactobacillus against oral pathogens. Lett. Appl. Microbiol. 2011, 53, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.R.; Martean, P. On the safety of lactic acid bacteria from food. Int J. Food. Microbiol. 1995, 27, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Yli-Knuuttila, H.; Snall, J.; Kari, K.; Meurman, J.H. Colonization of Lactobacillus rhamnosus GG in the oral cavity. Oral Microbiol. Immunol. 2006, 21, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Caglar, E.; Topcuoglu, N.; Cildir, S.K.; Sandalli, N.; Kulekci, G. Oral colonization by Lactobacillus reuteri ATCC 55730 after exposure to probiotics. Int. J. Paediatr. Dent. 2009, 19, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Ravn, I.; Dige, I.; Meyer, R.L.; Nyvad, B. Colonization of the oral cavity by probiotic bacteria. Caries Res. 2012, 46, 107–112. [Google Scholar] [CrossRef]
- Teanpaisan, R.; Piwat, S. Lactobacillus paracasei SD1, a novel probiotic, reduces mutans streptococci in human volunteers: a randomized placebo-controlled trial. Clin. Oral Investig. 2014, 18, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Ritthagol, W.; Saetang, C.; Teanpaisan, R. Effect of probiotics containing Lactobacillus paracasei SD1 on salivary mutans streptococci and lactobacilli in orthodontic cleft patients: A double-blinded, randomized, placebo-controlled study. Cleft Palate Craniofac. J. 2014, 51, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Nase, L.; Hatakka, K.; Savilahti, E.; Saxelin, M.; Ponka, A.; Poussa, T.; Korpela, R.; Meurman, J.H. Effect of long-term consumption of a probiotic bacterium, Lactobacillus rhamnosus GG, in milk on dental caries and caries risk in children. Caries Res. 2001, 35, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Cildir, S.K.; Germec, D.; Sandalli, N.; Ozdemir, F.I.; Arun, T.; Twetman, S.; Caglar, E. Reduction of salivary mutans streptococci in orthodontic patients during daily consumption of yoghurt containing probiotic bacteria. Eur. J. Orthod. 2009, 31, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Cildir, S.K.; Sandalli, N.; Nazli, S.; Alp, F.; Caglar, E. A novel delivery system of probiotic drop and its effect on dental caries risk factors in cleft lip/palate children. Cleft Palate Craniofac. J. 2012, 49, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Caglar, E.; Cildir, S.K.; Sandallin, N.; Ergeneli, S.; Twetman, S. Salivary mutans streptococci and lactobacilli levels after ingestion of the probiotic bacterium Lactobacillus reuteri ATCC 55730 by straws or tablets. Acta. Odontol. Scand. 2006, 64, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Caglar, E.; Kuscu, O.O.; Cildir, S.K.; Kuvvetli, S.S.; Sandallin, N. A probiotic lozenge administered medical device and its effect on salivary mutans streptococci and lactobacilli. Int. J. Paediatr. Dent. 2008, 18, 35–39. [Google Scholar] [PubMed]
- Aminabadi, N.A.; Erfanparast, L.; Ebrahimi, A.; Oskouei, S.G. Effect of chlorhexidine pretreatment on the stability of salivary lactobacilli probiotic in six- to twelve-year-old children: A randomized controlled trial. Caries Res. 2011, 45, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Jindal, G.; Pandey, R.K.; Agarwal, J.; Singh, M. A comparative evaluation of probiotics on salivary mutans streptococci counts in Indian children. Eur. Arch. Paediatr. Dent. 2011, 12, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Parvez, S.; Malik, K.A.; Ah Kang, S.; Kim, H.Y. Probiotics and their fermented food products are beneficial for health. J. Appl. Microbiol. 2006, 100, 1171–1185. [Google Scholar] [CrossRef] [PubMed]
- Piwat, S.; Teanpaisan, R.; Dahlén, G.; Thitasomakul, S.; Douglas, C.W. Acid production and growth by oral Lactobacillus species in vitro. J. Investig. Clin. Dent. 2012, 3, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for the Evaluation of Probiotics in Food; Joint FAO/WHO Working Group: London, UK, 2002.
- Wannun, P.; Piwat, S.; Teanpaisan, R. Purification and characterization of bacteriocin produced by oral Lactobacillus paracasei SD1. Anaerobe 2014, 15, 17–21. [Google Scholar] [CrossRef]
- Teanpaisan, R.; Chooruk, A.; Wannun, A.; Wichienchot, S.; Piwat, S. Survival rates of human-derived probiotic Lactobacillus paracasei SD1 in milk powder using spray drying. Songklanakarin. J. Sci. Technol. 2012, 34, 241–245. [Google Scholar]
- World Health Organization. Oral Health Surveys, Basic Methods, 3rd ed.; World Health Organization: Geneva, Switzerland, 1987. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teanpaisan, R.; Piwat, S.; Tianviwat, S.; Sophatha, B.; Kampoo, T. Effect of Long-Term Consumption of Lactobacillus paracasei SD1 on Reducing Mutans streptococci and Caries Risk: A Randomized Placebo-Controlled Trial. Dent. J. 2015, 3, 43-54. https://doi.org/10.3390/dj3020043
Teanpaisan R, Piwat S, Tianviwat S, Sophatha B, Kampoo T. Effect of Long-Term Consumption of Lactobacillus paracasei SD1 on Reducing Mutans streptococci and Caries Risk: A Randomized Placebo-Controlled Trial. Dentistry Journal. 2015; 3(2):43-54. https://doi.org/10.3390/dj3020043
Chicago/Turabian StyleTeanpaisan, Rawee, Supatcharin Piwat, Sukanya Tianviwat, Benchamat Sophatha, and Thanyanan Kampoo. 2015. "Effect of Long-Term Consumption of Lactobacillus paracasei SD1 on Reducing Mutans streptococci and Caries Risk: A Randomized Placebo-Controlled Trial" Dentistry Journal 3, no. 2: 43-54. https://doi.org/10.3390/dj3020043
APA StyleTeanpaisan, R., Piwat, S., Tianviwat, S., Sophatha, B., & Kampoo, T. (2015). Effect of Long-Term Consumption of Lactobacillus paracasei SD1 on Reducing Mutans streptococci and Caries Risk: A Randomized Placebo-Controlled Trial. Dentistry Journal, 3(2), 43-54. https://doi.org/10.3390/dj3020043