
The Impact of a Postgraduate Learning Experience on the Confidence of General Dental Practitioners


Abstract
:1. Introduction
2. Materials and Methods
3. Results
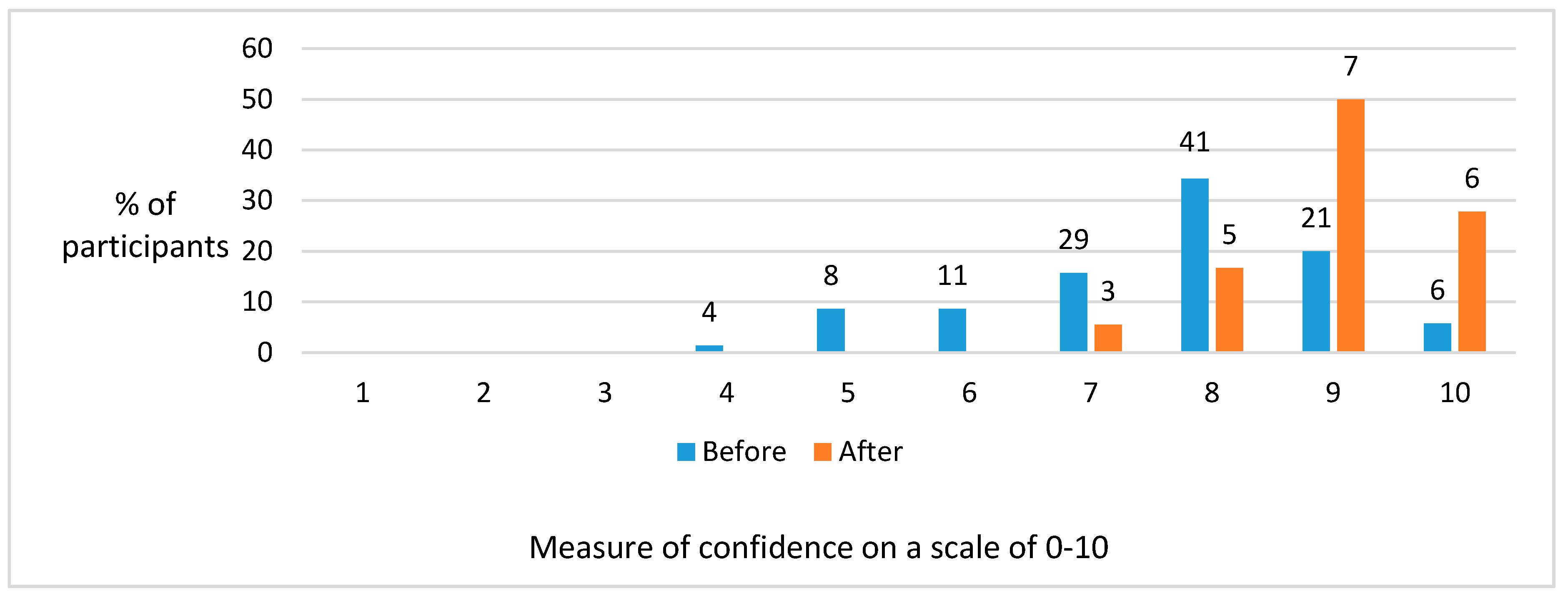
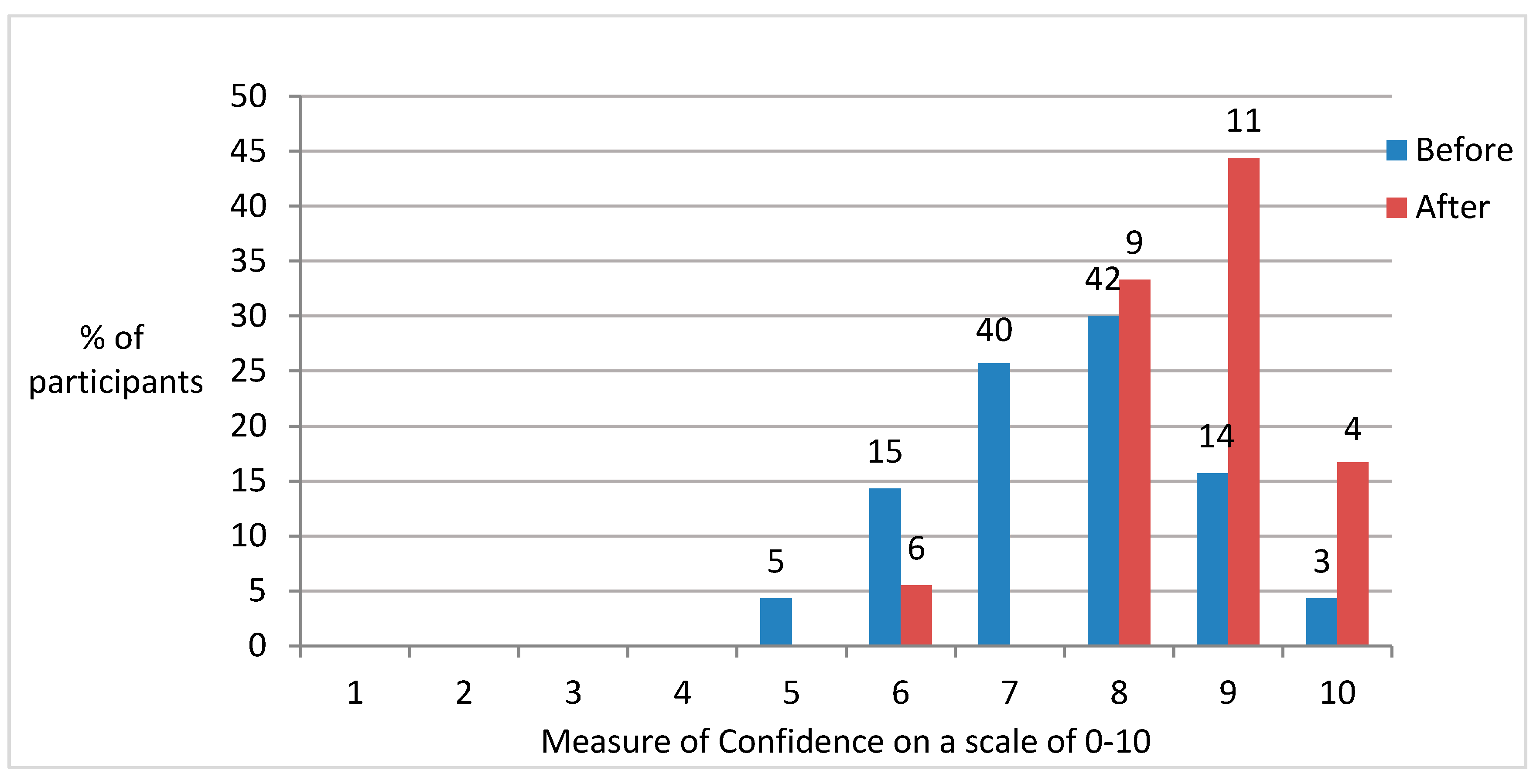
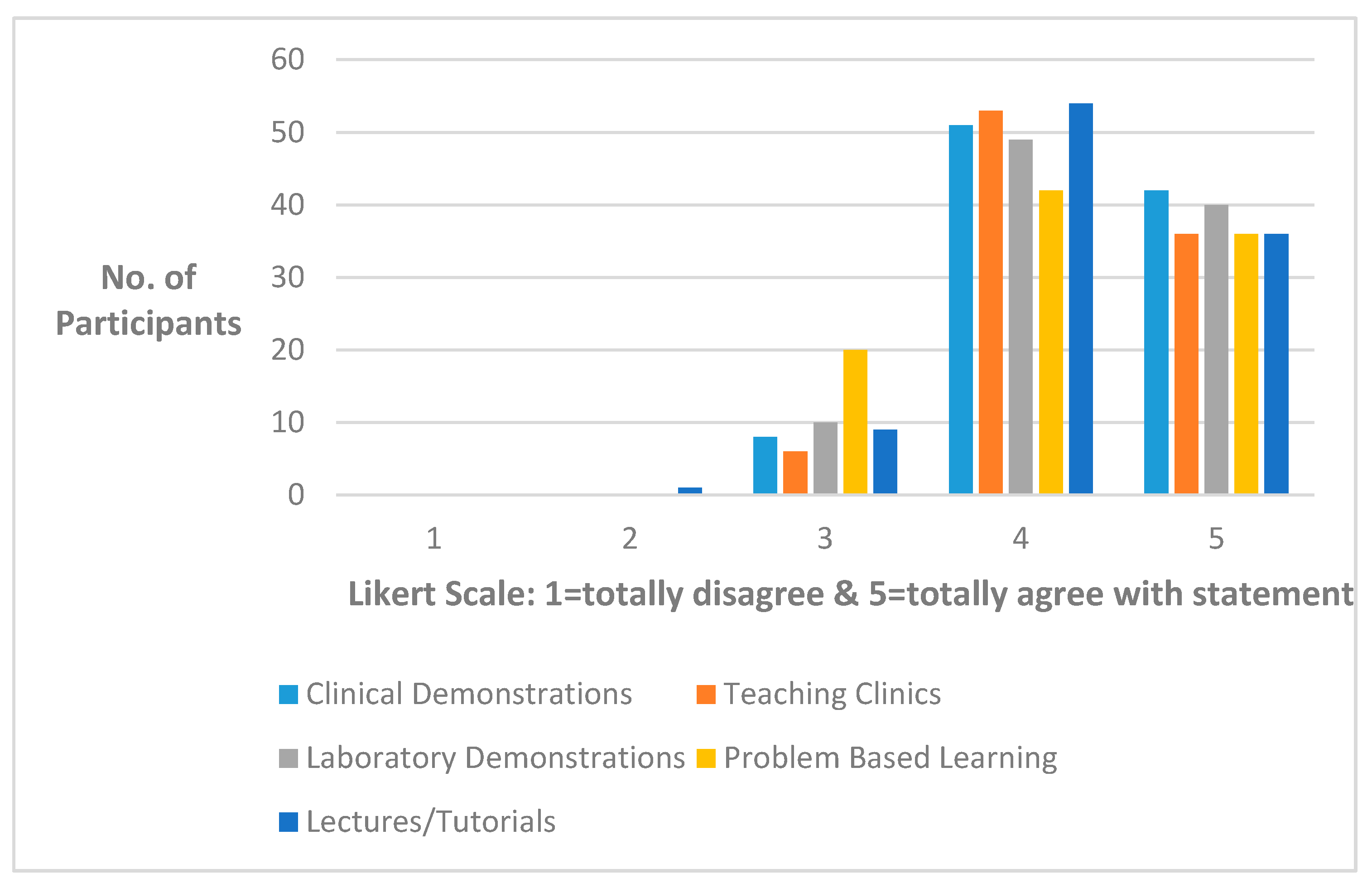
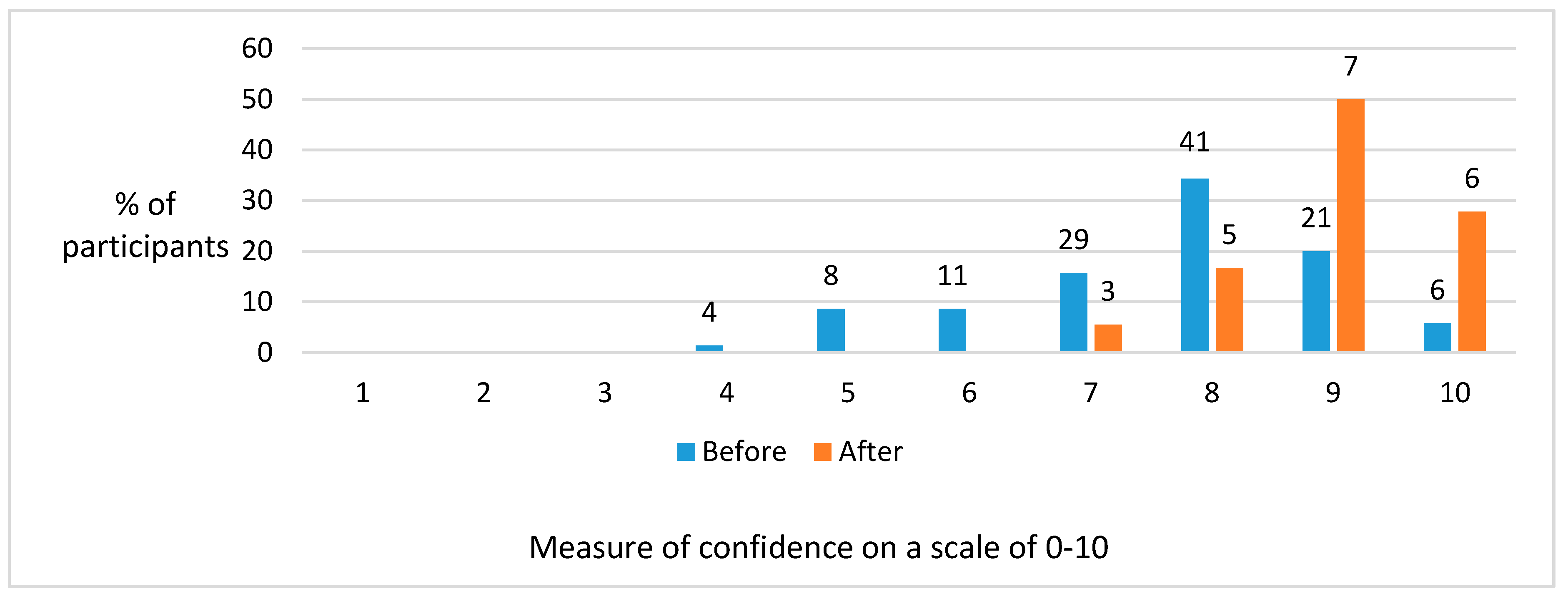
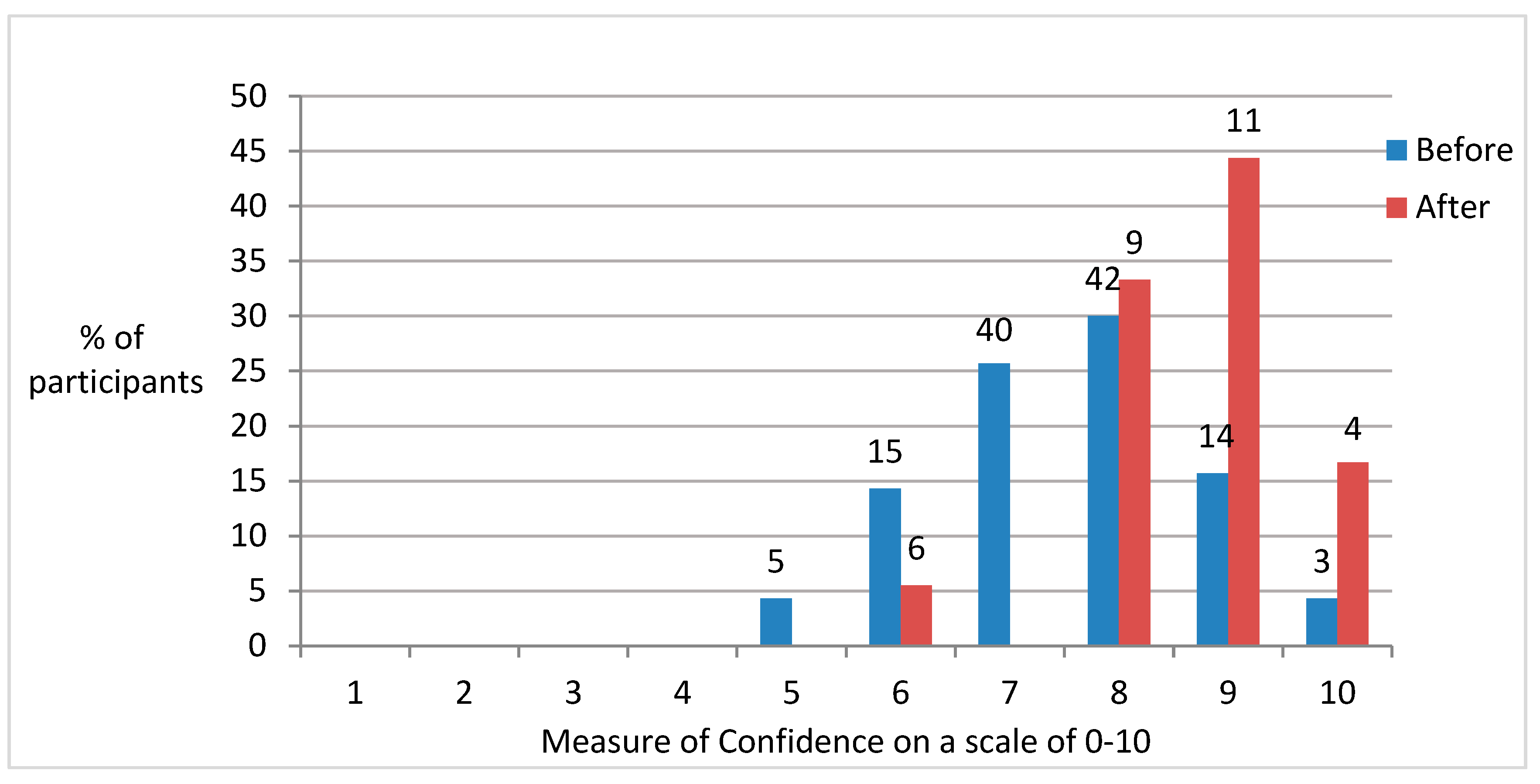
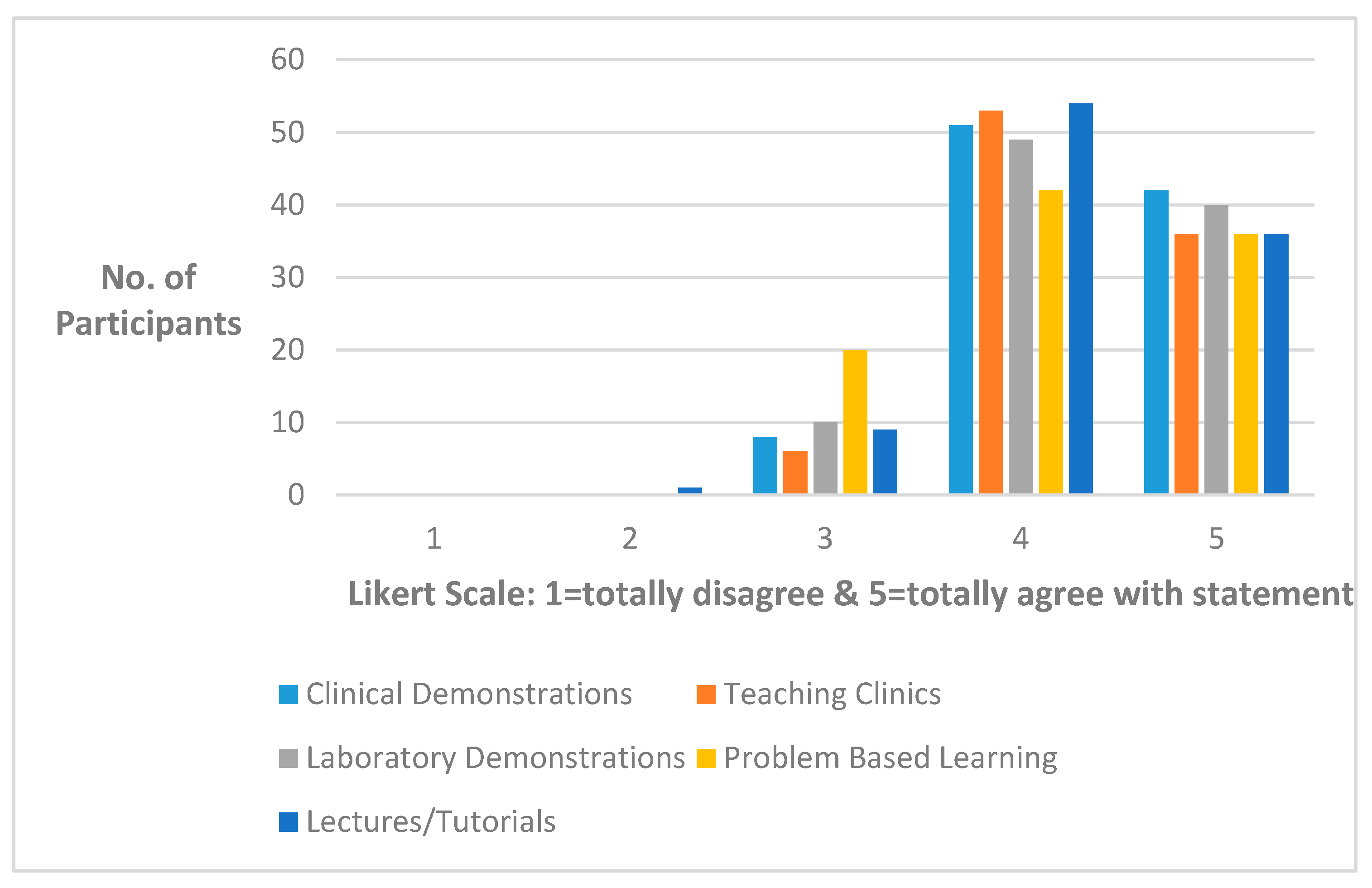
3.1. Quantitative Results
3.2. Qualitative Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Stankov, L.; Morony, S.; Lee, Y. Confidence: The best non-cognitive predictor of academic achievement? Educ. Psychol. 2014, 34, 9–28. [Google Scholar] [CrossRef]
- Premadasa, I.G.; Shehab, D.; Al-Jarallat, K.F.; Thalib, L. Frequency and Confidence in performing clinical skills among medical interns in Kuwait. Med. Teach. 2008, 30, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Oxford English Dictionary. March 2017. Available online: https://en.oxforddictionaries.com/ (accessed on 24 April 2017).
- Bandura, A. Social Foundations of Thought and Action; Prentice-Hall: London/Englewood Cliffs, UK, 1986; p. 19. [Google Scholar]
- Pajares, F. Frank Pajares on Nurturing Academic Confidence; Emory Report; 14 February 2000; Volume 52, p. 21. [Google Scholar]
- Pajares, F. Current Directions in Self-efficacy Research. In Advances in Motivation and Achievement; Maehr, M.L., Pintrich, P.R., Eds.; JAI Press: London, UK, 1997. [Google Scholar]
- Pajares, F. Self-Efficacy Beliefs in Academic Contexts: An Outline. 2002. Available online: http://des.emory.edu/mfp/efftalk.html (accessed on 24 April 2017).
- Crozier, R. Individual Learners: Personality Differences in Education; Routledge: London, UK, 1997. [Google Scholar]
- Koriat, A.; Lichtenstein, S.; Fischoff, B. Reasons for Confidence. J. Exp. Psychol. Hum. Learn. Mem. 1980, 6, 107–118. [Google Scholar] [CrossRef]
- NatCen Learning. The Framework Approach to Qualitative Data Analysis; NatCen Learning: London, UK, 2012. [Google Scholar]
- Rogers, C. A Way of Being; Houghton Mifflin Company: Boston, MA, USA, 1980. [Google Scholar]
- Creswell, J. Qualitative Inquiry and Research Design-Choosing among Five Approaches; SAGE Publications: London, UK; New Delhi, India; Singapore, 2013. [Google Scholar]
- Mouatt, R.B.; Veale, B.; Archer, K. Continuing education in the GDS. An England survey 1991. Br. Dent. J. 1991, 170, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Likert, R. A Technique for the Measurment of Attitude; Archives of Psychology; The Science Press: New York, NY, USA, 1932; Volume 140, pp. 1–55. [Google Scholar]
- Marsh, H. Student Evaluations. Int. J. Educ. Res. 1987, 11, 235–388. [Google Scholar]
- Bandura, A.; Cervone, D. Self-evaluation and Self-efficacy Mechanisms Governing the Motivational Effects of Goal Systems. J. Personal. Soc. Psychol. 1983, 45, 1017–1028. [Google Scholar] [CrossRef]
- Cohen, L.; Manion, L.; Morrison, K. Research Methods in Education, 6th ed.; Routledge: London, UK, 2007; pp. 22–25. [Google Scholar]
- Sander, P.; Sttevenson, K.; King, M.; Coates, D. University Students’ Expectations of Teaching. Stud. High. Educ. 2000, 25, 309–323. [Google Scholar] [CrossRef]
- Sander, P.; Sanders, L. Measuring Confidence in academic study: A Summary report. Res. Educ. Psychol. Psychopedagogy 2002, 1, 1–17. [Google Scholar]
- Bandura, A. Perceived Self-Efficacy in Cognitive Development and Functioning. Educ. Psychol. 1993, 28, 117–148. [Google Scholar] [CrossRef]
- Stewart, J.; O’halloran, C.; Barton, R.; Singleton, S.; Harrigman, P.; Spencer, J. Clarifying the concept of confidence and competence to produce appropriate self-evaluation measurement scales. Med. Educ. 2000, 34, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Lave, J.; Wenger, E. Situated Learning. Legitimate Peripheral Participation; Cambridge University Press: London, UK, 1991; pp. 98–100. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Age | Range: 25–46 + Years Mean: 35 |
|---|---|
| Gender | Male: 9 Female: 9 |
| Number of Years Qualified | Range: 8–34 years; Mean: 14.2 years |
| Primary place of work | National Health Service Practice: Before the programme = 4 After the programme = 0 |
| Mixed NHS/Private Practice: Before the programme = 12 After the programme = 12 | |
| Private Practice: Before the programme = 2 After the programme = 5 | |
| Community Practice: Before the programme = 0 After the programme = 1 | |
| Level of Enjoyment on a scale of 0–10 (0 = no enjoyment; 10 = total enjoyment) | Range: 2–10; Mean: 6.9 |
| Received a Satisfactory Learning Experience | Totally satisfactory = 6 Satisfactory = 9 Reasonably satisfactory = 2 Unsatisfactory = 1 Totally unsatisfactory = 0 |
| Reasons for Attendance | Percentage |
|---|---|
| To increase confidence | 42% |
| To increase level of knowledge | 41% |
| To increase level of skill | 42% |
| To be up to date with cutting edge technology | 29% |
| Course Participant | Confidence Range | Mean | SD |
|---|---|---|---|
| Gender | |||
| Male | 7–10 | 9.00 | 1.069 |
| Female | 9–10 | 9.25 | 0.500 |
| Age | |||
| 25–35 years | 9–10 | 9.50 | 0.548 |
| 36–45 years | 0 | 0 | 0 |
| 46+ | 7–10 | 8.67 | 1.033 |
| No. Years Qual. | |||
| 2–10 | 9–10 | 9.20 | 0.548 |
| 11–20 | 9–10 | 9.20 | 0.447 |
| 21+ | 7–8 | 7.50 | 0.707 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fine, P.; Louca, C.; Leung, A. The Impact of a Postgraduate Learning Experience on the Confidence of General Dental Practitioners. Dent. J. 2017, 5, 16. https://doi.org/10.3390/dj5020016
Fine P, Louca C, Leung A. The Impact of a Postgraduate Learning Experience on the Confidence of General Dental Practitioners. Dentistry Journal. 2017; 5(2):16. https://doi.org/10.3390/dj5020016
Chicago/Turabian StyleFine, Peter, Chris Louca, and Albert Leung. 2017. "The Impact of a Postgraduate Learning Experience on the Confidence of General Dental Practitioners" Dentistry Journal 5, no. 2: 16. https://doi.org/10.3390/dj5020016
APA StyleFine, P., Louca, C., & Leung, A. (2017). The Impact of a Postgraduate Learning Experience on the Confidence of General Dental Practitioners. Dentistry Journal, 5(2), 16. https://doi.org/10.3390/dj5020016