Adjunctive Effects of a Sub-Antimicrobial Dose of Doxycycline on Clinical Parameters and Potential Biomarkers of Periodontal Tissue Catabolism

 ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Study Design
2.3. Gingival Crevicular Fluid (GCF) Sampling
2.4. MPO, MMP-9, MMP-13, OPG, and TRAP-5 in GCF by Enzyme-Linked Immunosorbent Assay (ELISA) and MMP-8 by Immunofluorometric Assay (IFMA) Analysis
3. Statistical Analysis
4. Results
4.1. Patient Disposition and Demographics
4.2. Clinical Results (Whole Mouth)
4.3. Clinical Results (Sampling Sites)
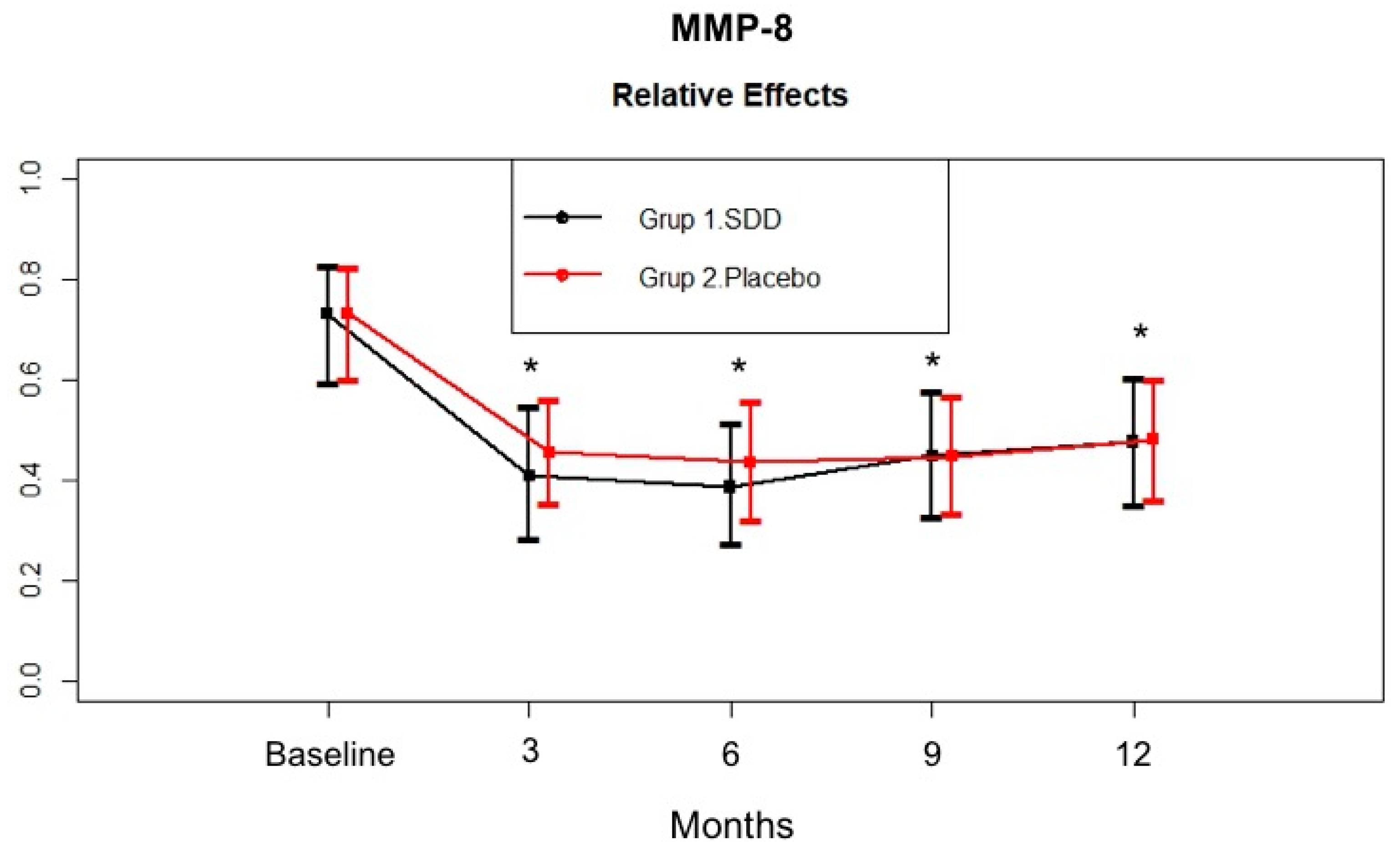
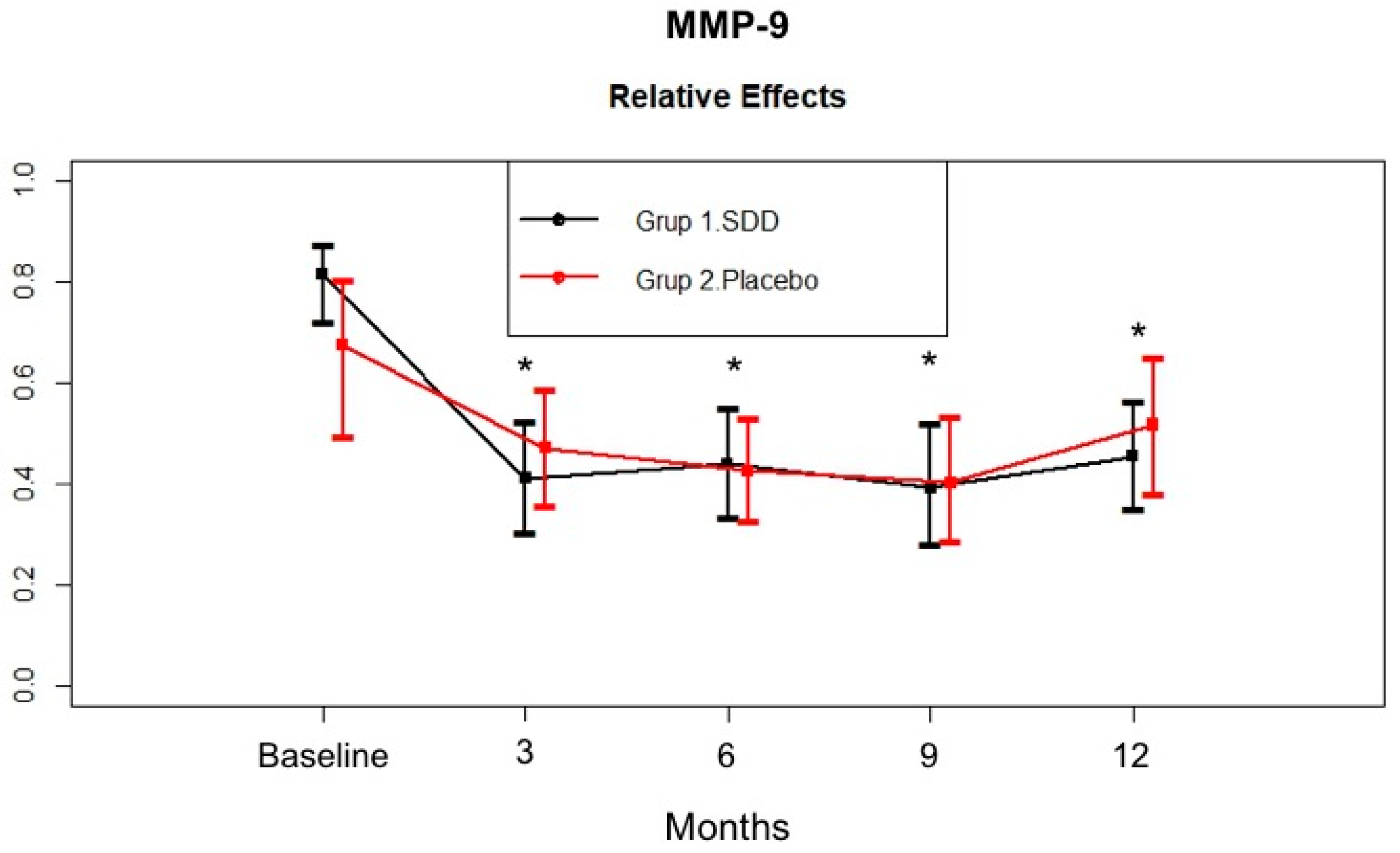
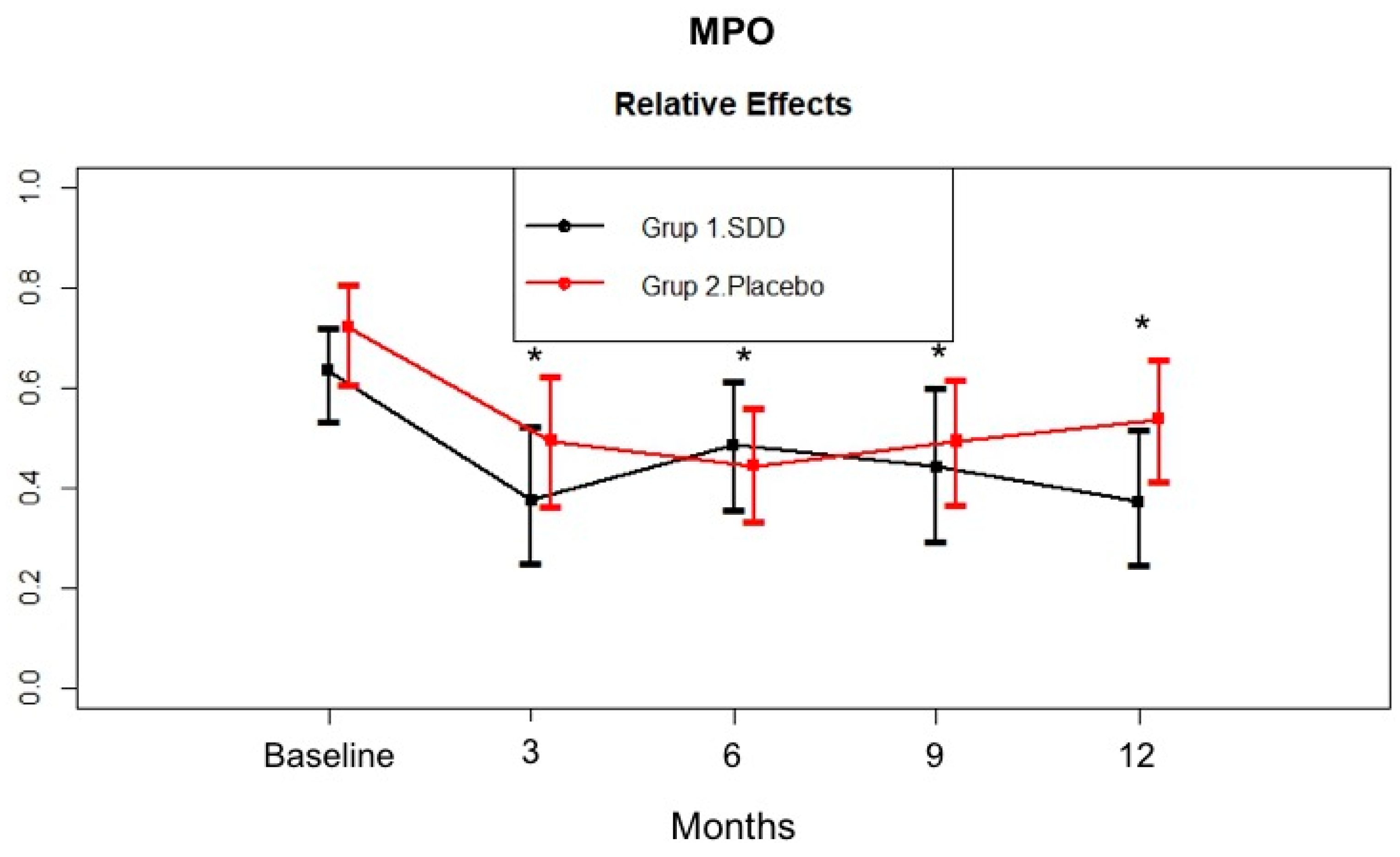
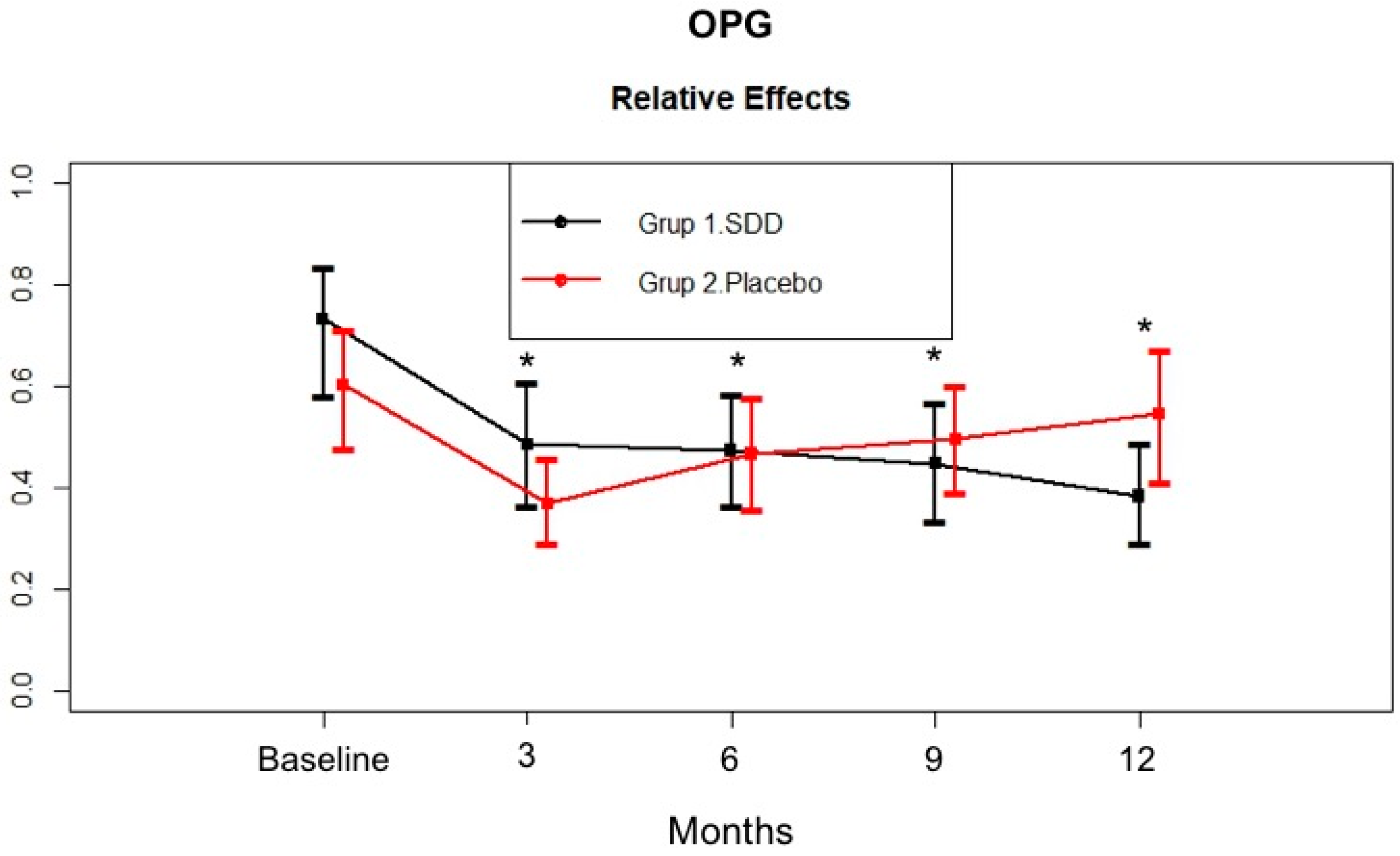
4.4. GCF MMP-8, MMP-9, MPO, and OPG Levels
5. Discussion
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SDD Group | Placebo Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 3 months | 6 months | 9 months | 12 months | Baseline | 3 months | 6 months | 9 months | 12 months | |
| PD (mm) | 4.03 ± 0.82 | 2.65 ± 0.40 * | 2.53 ± 0.39 *¶ | 2.45 ± 0.52 *¶ | 2.42 ± 0.55 *¶ | 4.15 ± 0.80 | 2.86 ± 0.46 * | 2.85 ± 0.57 * | 2.88 ± 0.61 * | 2.89 ± 0.62 * |
| CAL (mm) | 4.71 ± 1.14 | 4.13 ± 1.03 * | 4.16 ± 0.98 *¶ | 4.09 ± 1.03 *¶ | 4.16 ± 1.00 * | 5.19 ± 1.20 | 4.73 ± 1.01 * | 4.86 ± 1.05 | 4.84 ± 1.06 | 4.84 ± 1.10 |
| GI | 1.82 ± 0.40 | 0.76 ± 0.33 *¶ | 0.83 ± 0.25 *¶ | 0.70 ± 0.29 *¶ | 0.70 ± 0.35 * | 1.89 ± 0.29 | 1.00 ± 0.30 * | 1.02 ± 0.28 * | 0.97 ± 0.33 * | 0.92 ± 0.33 * |
| PI | 3.84 ± 0.89 | 1.96 ± 0.74 * | 1.97 ± 0.80 * | 1.69 ± 0.97 * | 1.41 ± 0.73 * | 4.18 ± 0.75 | 2.07 ± 0.72 * | 1.95 ± 0.72 * | 1.89 ± 0.73 * | 1.87 ± 0.70 * |
| SDD Group | Placebo Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 3 months | 6 months | 9 months | 12 months | Baseline | 3 months | 6 months | 9 months | 12 months | |
| PD (mm) | 7.05 ± 0.72 | 3.66 ± 1.00 * | 3.16 ± 0.75 * | 2.94 ± 1.10 * | 2.90 ± 1.04 * | 6.68 ± 1.15 | 3.63 ± 1.37 * | 3.58 ± 1.46 * | 3.38 ± 1.37 * | 3.55 ± 1.40 * |
| CAL (mm) | 7.58 ± 1.49 | 5.53 ± 2.31 * | 5.26 ± 1.81 * | 5.21 ± 1.84 * | 4.90 ± 2.16 * | 7.90 ± 1.69 | 6.35 ± 1.93 * | 6.53 ± 1.98 * | 6.13 ± 2.09 * | 6.35 ± 2.09 * |
| GI | 2.11 ± 0.49 | 0.50 ± 0.62 * | 0.61 ± 0.52 * | 0.32 ± 0.45 * | 0.26 ± 0.39 * | 1.78 ± 0.59 | 0.68 ± 0.49 * | 0.65 ± 0.67 * | 0.58 ± 0.65 * | 0.43 ± 0.61 * |
| PI | 3.68 ± 0.87 | 1.92 ± 0.92 * | 1.82 ± 1.26 * | 1.82 ± 1.38 * | 1.32 ± 0.84 * | 4.05 ± 1.18 | 1.85 ± 1.01 * | 1.78 ± 0.94 * | 2.00 ± 1.15 * | 2.18 ± 1.31 * |
| GCF (μl) | 1.12 ± 0.35 | 0.54 ± 0.22 * | 0.38 ± 0.16 * | 0.55 ± 0.26 * | 0.50 ± 0.24 * | 0.98 ± 0.40 | 0.42 ± 0.23 * | 0.48 ± 0.31 * | 0.49 ± 0.26 * | 0.53 ± 0.28 * |
References
- Hernández, M.; Dutzan, N.; García-Sesnich, J.; Abusleme, L.; Dezerega, A.; Silva, N.; González, F.E.; Vernal, R.; Sorsa, T.; Gamonal, J. Host-pathogen interactions in progressive chronic periodontitis. J. Dent. Res. 2011, 90, 1164–1170. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M.; Taylor, J.J. How has research into cytokine interactions and their role in driving immune responses impacted our understanding of periodontitis? J. Clin. Periodontol. 2011, 38, 60–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinane, D.F. Regulators of tissue destruction and homeostasis as diagnostic aids in periodontology. Periodontol 2000 2000, 24, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Tjäderhane, L.; Konttinen, Y.T.; Lauhio, A.; Salo, T.; Lee, H.M.; Golub, L.M.; Brown, D.L.; Mäntylä, P. Matrix metalloproteinases: Contribution to pathogenesis, diagnosis and treatment of periodontal inflammation. Ann. Med. 2006, 38, 306–321. [Google Scholar] [CrossRef] [PubMed]
- Uitto, J.; Overall, C.M.; McCulloch, C. Proteolytic host cell enzymes in gingival crevice fluid. Periodontol 2000 2003, 31, 77–104. [Google Scholar] [CrossRef] [PubMed]
- Fields, G.B. Interstitial collagen catabolism. J. Biol. Chem. 2013, 288, 8785–8793. [Google Scholar] [CrossRef] [PubMed]
- Vandooren, J.; Van den Steen, P.E.; Opdenakker, G. Biochemistry and molecular biology of gelatinase B or matrix metalloproteinase-9 (MMP-9): The next decade. Crit. Rev. Biochem. Mol. Biol. 2013, 48, 222–272. [Google Scholar] [CrossRef] [PubMed]
- Tardif, G.; Reboul, P.; Pelletier, J.P.; Martel-Pelletier, J. Ten years in the life of an enzyme: The story of the human MMP-13 (collagenase-3). Mod. Rheumatol. 2004, 14, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Hernández Ríos, M.; Sorsa, T.; Obregón, F.; Tervahartiala, T.; Valenzuela, M.A.; Pozo, P.; Dutzan, N.; Lesaffre, E.; Molas, M.; Gamonal, J. Proteolytic roles of matrix metalloproteinase (MMP)-13 during progression of chronic periodontitis: Initial evidence for MMP-13/MMP-9 activation cascade. J. Clin. Periodontol. 2009, 36, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Hernández, M.; Gamonal, J.; Tervahartiala, T.; Mäntylä, P.; Rivera, O.; Dezerega, A.; Dutzan, N.; Sorsa, T. Associations between matrix metalloproteinase-8 and -14 and myeloperoxidase in gingival crevicular fluid from subjects with progressive chronic periodontitis: A longitudinal study. J. Periodontol. 2010, 81, 1644–1652. [Google Scholar] [CrossRef] [PubMed]
- Gursoy, U.K.; Könönen, E.; Pradhan-Palikhe, P.; Tervahartiala, T.; Pussinen, P.J.; Suominen-Taipale, L.; Sorsa, T. Salivary MMP-8, TIMP-1, and ICTP as markers of advanced periodontitis. J. Clin. Periodontol. 2010, 37, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Ejeil, A.L.; Igondjo-Tchen, S.; Ghomrasseni, S.; Pellat, B.; Godeau, G.; Gogly, B. Expression of matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs) in healthy and diseased human gingiva. J. Periodontol. 2003, 74, 188–195. [Google Scholar] [CrossRef]
- Sorsa, T.; Hernández, M.; Leppilahti, J.; Munjal, S.; Netuschil, L.; Mäntylä, P. Detection of gingival crevicular fluid MMP-8 levels with different laboratory and chair-side methods. Oral Dis. 2010, 16, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorsa, T.; Gursoy, U.K.; Nwhator, S.; Hernández, M.; Tervahartiala, T.; Leppilahti, J.; Gursoy, M.; Könönen, E.; Emingil, G.; Pussinen, P.J.; et al. Analysis of matrix metalloproteinases, especially MMP-8, in gingival crevicular fluid, mouthrinse and saliva for monitoring periodontal diseases. Periodontol 2000 2016, 70, 142–163. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Gieselmann, D.; Arweiler, N.B.; Hernández, M. A quantitative point-of-care test for periodontal and dental peri-implant diseases. Nat. Rev. Dis. Primers 2017, 3, 17069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, C.F.; Smith, Q.T. Crevicular fluid myeloperoxidase at healthy, gingivitis and periodontitis sites. J. Clin. Periodontol. 1989, 16, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Wei, P.F.; Ho, K.Y.; Ho, Y.P.; Wu, Y.M.; Yang, Y.H.; Tsai, C.C. The investigation of glutathione peroxidase, lactoferrin, myeloperoxidase and interleukin-1beta in gingival crevicular fluid: Implications for oxidative stress in human periodontal diseases. J. Period. Res. 2004, 39, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Borges, I., Jr.; Moreira, E.A.; Filho, D.W.; de Oliveira, T.B.; da Silva, M.B.; Fröde, T.S. Proinflammatory and oxidative stress markers in patients with periodontal disease. Mediat. Inflamm. 2007, 2007, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.J.; Peppin, G.J. Collagenolytic metalloenzymes of the human neutrophil. Characteristics, regulation and potential function in vivo. Biochem. Pharmacol. 1986, 35, 3189–3197. [Google Scholar] [CrossRef]
- Vissers, M.C.; Winterbourn, C.C. Myeloperoxidase-dependent oxidative inactivation of neutrophil neutral proteinases and microbicidal enzymes. Biochem. J. 1987, 245, 277–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saari, H.; Suomalainen, K.; Lindy, O.; Konttinen, Y.T.; Sorsa, T. Activation of latent human neutrophil collagenase by reactive oxygen species and serine proteases. Biochem. Biophys. Res. Commun. 1990, 171, 979–987. [Google Scholar] [CrossRef]
- Wang, Y.; Rosen, H.; Madtes, D.K.; Shao, B.; Martin, T.R.; Heinecke, J.W.; Fu, X. Myeloperoxidase inactivates TIMP-1 by oxidizing its N-terminal cysteine residue: An oxidative mechanism for regulating proteolysis during inflammation. J. Biol. Chem. 2007, 282, 31826–31834. [Google Scholar] [CrossRef] [PubMed]
- Leppilahti, J.M.; Hernández-Ríos, P.A.; Gamonal, J.A.; Tervahartiala, T.; Brignardello-Petersen, R.; Mantyla, P.; Sorsa, T.; Hernández, M. Matrix metalloproteinases and myeloperoxidase in gingival crevicular fluid provide site-specific diagnostic value for chronic periodontitis. J. Clin. Periodontol. 2014, 41, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Kirstein, B.; Chambers, T.J.; Fuller, K. Secretion of tartrate-resistant acid phosphatase by osteoclasts correlates with resorptive behavior. J. Cell. Biochem. 2006, 98, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Halleen, J.M. Tartrate-resistant acid phosphatase 5B is a specific and sensitive marker of bone resorption. Anticancer Res. 2003, 23, 1027–1029. [Google Scholar] [PubMed]
- Hienz, S.A.; Paliwal, S.; Ivanovski, S. Mechanisms of Bone Resorption in Periodontitis. J. Immunol. Res. 2015, 2015, 1–10. [Google Scholar] [CrossRef]
- Jin, Q.; Cirelli, J.A.; Park, C.H.; Sugai, J.V.; Taba, M., Jr.; Kostenuik, P.J.; Giannobile, W.V. RANKL inhibition through osteoprotegerin blocks bone loss in experimental periodontitis. J. Periodontol. 2007, 78, 1300–1308. [Google Scholar] [CrossRef]
- Page, R.C. Periodontal therapy: Prospects for the future. J. Periodontol. 1993, 64, 744–753. [Google Scholar] [CrossRef]
- Loesche, W.J. The antimicrobial treatment of periodontal disease: Changing the treatment paradigm. Crit. Rev. Oral Biol. Med. 1999, 10, 245–275. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Williams, R.C.; Siciliano, V.I.; Alibrandi, A.; Cordasco, G.; Ramaglia, L. The effects of a desiccant agent in the treatment of chronic periodontitis: A randomized, controlled clinical trial. Clin. Oral Investig. 2018, 22, 791–800. [Google Scholar] [CrossRef]
- Tabenski, L.; Moder, D.; Cieplik, F.; Schenke, F.; Hiller, K.A.; Buchalla, W.; Schmalz, G.; Christgau, M. Antimicrobial photodynamic therapy vs. local minocycline in addition to non-surgical therapy of deep periodontal pockets: A controlled randomized clinical trial. Clin. Oral Investig. 2017, 21, 2253–2264. [Google Scholar] [CrossRef] [PubMed]
- Matarese, G.; Ramaglia, L.; Cicciù, M.; Cordasco, G.; Isola, G. The Effects of Diode Laser Therapy as an Adjunct to Scaling and Root Planing in the Treatment of Aggressive Periodontitis: A 1-Year Randomized Controlled Clinical Trial. Photomed. Laser Surg. 2017, 35, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Lang, N.P. Host modulation in the management of periodontal diseases. J. Clin. Periodontol. 2005, 32, 108–129. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Lee, H.M.; Ryan, M.E.; Giannobile, W.V.; Payne, J.; Sorsa, T. Tetracyclines inhibit connective tissue breakdown by multiple non-antimicrobial mechanisms. Adv. Dent. Res. 1998, 12, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Caton, J.G.; Ciancio, S.G.; Blieden, T.M.; Bradshaw, M.; Crout, R.J.; Hefti, A.F.; Massaro, J.M.; Polson, A.M.; Thomas, J.; Walker, C. Treatment with subantimicrobial dose doxycycline improves the efficacy of scaling and root planing in patients with adult periodontitis. J. Periodontol. 2000, 71, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Emingil, G.; Attila, G.; Sorsa, T.; Luoto, H.; Kırılmaz, L.; Baylas, H. The effect of adjunctive low-dose doxycycline therapy on clinical parameters and gingival crevicular fluid matrix metalloproteinase-8 levels in chronic periodontitis. J. Periodontol. 2004, 75, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M.; Hefti, A.F.; Jepsen, S.; Etienne, D.; Walker, C.; Bradshaw, M.H. Subantimicrobial dose doxycycline as adjunctive treatment for periodontitis. J. Clin. Periodontol. 2004, 31, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.G.; Metheny, R.J.; Karakiozis, J.M.; Wetzel, J.M.; Crout, R.J. Long-term sub-antimicrobial doxycycline (Periostat®) as adjunctive management in adult periodontitis: Effects on subgingival bacterial population dynamics. Adv. Dent. Res. 1998, 12, 32–39. [Google Scholar] [CrossRef]
- Walker, C.; Thomas, J.; Nango, S.; Lennon, J.; Wetzel, J.; Powala, C. Long-term treatment with subantimicrobial dose doxycycline exerts no antibacterial effect on the subgingival microflora associated with adult periodontitis. J. Periodontol. 2000, 71, 1465–1471. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef]
- Löe, H.; Silness, J. Periodontal disease in pregnancy. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 532–551. [Google Scholar] [CrossRef]
- Turesky, S.; Gilmore, N.D.; Glickman, I. Reduced plaque formation by the chloromethyl analogue of Vitamin C. J. Periodontol. 1970, 41, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Badersten, A.; Nilveus, R.; Egelberg, J. Effect of non-surgical periodontal therapy (IV). Operator variability. J. Clin. Periodontol. 1985, 12, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Lamster, I.B.; Hartley, L.J.; Oshrain, R.L. Evaluation and modification of spectrophotometric procedures for analysis of lactate dehydrogenase, beta-glucuronidase and arylsulphatase in human gingival crevicular fluid collected with filter-paper strips. Arch. Oral Biol. 1985, 30, 235–242. [Google Scholar] [CrossRef]
- The American Academy of Periodontology. Parameter on periodontal maintenance. J. Periodontol. 2000, 71, 849–850. [Google Scholar] [CrossRef] [PubMed]
- Cobb, C.M. Non-surgical pocket therapy: Mechanical. Ann. Periodontol. 1996, 1, 443–490. [Google Scholar] [CrossRef]
- Greenstein, G. Periodontal response to mechanical non-surgical therapy: A Review. J. Periodontol. 1992, 63, 118–130. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Effect of therapy on periodontal infections. J. Periodontol. 1993, 64, 754–759. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, Y.M.; Shin, S.Y.; Seol, Y.J.; Ku, Y.; Rhyu, I.C.; Chung, C.P.; Han, S.B. Effect of subantimicrobial dose doxycycline as an effective adjunct to scaling and root planing. J. Periodontol. 2004, 75, 1500–1508. [Google Scholar] [CrossRef]
- Golub, L.M.; McNamara, T.F.; Ryan, M.E.; Kohut, B.; Blieden, T.; Payonk, G.; Sipos, T.; Baron, H.J. Adjunctive treatment with subantimicrobial doses of doxcycline: Effects on gingival fluid collagenase activity and attachment loss in adult periodontitis. J. Clin. Periodontol. 2001, 28, 146–156. [Google Scholar] [CrossRef]
- Golub, L.M.; Lee, H.M.; Greenwald, R.A.; Ryan, M.E.; Sorsa, T.; Salo, T.; Giannobile, W.V. A matrix metalloproteinase inhibitor reduces bone-type collagen degradation fragments and specific collagenases in gingival crevicular fluid during adult periodontitis. Inflamm. Res. 1997, 46, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Cianci, S.; Ramamurthy, N.S.; Leung, M.; McNamara, T.F. Low-dose doxycycline therapy: Effect on gingival and crevicular fluid collagenase activity in humans. J. Periodont. Res. 1990, 25, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Demirel, K.; Baer, P.N.; McNamara, T.F. Topical application of doxycycline on periodontally involved root surfaces in vitro: Comparative analysis of substantivity on cementum and dentin. J. Periodontol. 1991, 62, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Aras, H.; Cağlayan, F.; Güncü, G.N.; Berberoğlu, A.; Kilinç, K. Effect of systemically administered naproxen sodium on clinical parameters and myeloperoxidase and elastase-like activity levels in gingival crevicular fluid. J. Periodontol. 2007, 78, 868–873. [Google Scholar] [CrossRef]
- Dagar, M.; Deepa, D.K.; Molly, M.; Sharma, A.; Khattak, B.P. Effect of nonsurgical periodontal therapy on salivary myeloperoxidase levels: A biochemical study. J. Indian Soc. Periodontol. 2015, 19, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Marcaccini, A.M.; Meschiari, C.A.; Zuardi, L.R.; de Sousa, T.S.; Taba, M., Jr.; Teofilo, J.M.; Jacob-Ferreira, A.L.; Tanus-Santos, J.E.; Novaes, A.B., Jr.; Gerlach, R.F. Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. J. Clin. Periodontol. 2010, 37, 180–190. [Google Scholar] [CrossRef]
- Nizam, N.; Gümüş, P.; Pitkänen, J.; Tervahartiala, T.; Sorsa, T.; Buduneli, N. Serum and salivary matrix metalloproteinases, neutrophil elastase, myeloperoxidase in patients with chronic or aggressive periodontitis. Inflammation 2014, 37, 1771–1778. [Google Scholar] [CrossRef]
- Buchmann, R.; Hasilik, A.; Nunn, M.E.; Van Dyke, T.E.; Lange, D.E. PMN responses in chronic periodontal disease: Evaluation by gingival crevicular fluid enzymes and elastase-alpha-1-proteinase inhibitor complex. J. Clin. Periodontol. 2002, 29, 563–572. [Google Scholar] [CrossRef]
- Suomalainen, K.; Sorsa, T.; Golub, L.M.; Ramamurthy, N.; Lee, H.M.; Uitto, V.J.; Saari, H.; Konttinen, Y.T. Specificity of the anticollagenase action of tetracyclines: Relevance to their anti-inflammatory potential. Antimicrob. Agents Chemother. 1992, 36, 227–229. [Google Scholar] [CrossRef]
- Emingil, G.; Atilla, G.; Sorsa, T.; Tervahartiala, T. The effect of adjunctive subantimicrobial dose doxycycline therapy on GCF EMMPRIN levels in chronic periodontitis. J. Periodontol. 2008, 79, 469–476. [Google Scholar] [CrossRef]
- Emingil, G.; Gürkan, A.; Atilla, G.; Berdeli, A.; Cinarcik, S. Adjunctive low-dose doxycycline therapy effect on clinical parameters and gingival crevicular fluid tissue plasminogen activator levels in chronic periodontitis. Inflamm. Res. 2006, 55, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Emingil, G.; Atilla, G.; Sorsa, T.; Savolainen, P.; Baylas, H. Effectiveness of adjunctive low-dose doxycycline therapy on clinical parameters and gingival crevicular fluid laminin-5 gamma2 chain levels in chronic periodontitis. J. Periodontol. 2004, 75, 1387–1396. [Google Scholar] [CrossRef]
- Emingil, G.; Gürkan, A.; Atilla, G.; Kantarci, A. Subantimicrobial-dose doxycycline and cytokine-chemokine levels in gingival crevicular fluid. J. Periodontol. 2011, 82, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Gürkan, A.; Çınarcık, S.; Hüseyinov, A. Adjunctive subantimicrobial dose doxycycline: Effect on clinical parameters and gingival crevicular fluid transforming growth factor- beta levels in severe, generalized chronic periodontitis. J. Clin. Periodontol. 2005, 32, 244–253. [Google Scholar] [CrossRef]
- Choi, D.H.; Moon, I.S.; Choi, B.K.; Paik, J.W.; Kim, Y.S.; Choi, S.H.; Kim, C.K. Effects of sub-antimicrobial dose doxycycline therapy on crevicular fluid MMP-8, and gingival tissue MMP-9, TIMP-1 and IL-6 levels in chronic periodontitis. J. Period. Res. 2004, 39, 20–26. [Google Scholar] [CrossRef]
- Shibutani, T.; Murahashi, Y.; Tsukada, E.; Iwayama, Y.; Heersche, J.N. Experimentally induced periodontitis in beagle dogs causes rapid increases in osteoclastic resorption of alveolar bone. J. Periodontol. 1997, 68, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Crotti, T.; Smith, M.D.; Hirsch, R.; Soukoulis, S.; Weedon, H.; Capone, M.; Ahern, M.J.; Haynes, D. Receptor activator NF kappaB ligand (RANKL) and osteoprotegerin (OPG) protein expression in periodontitis. J. Period. Res. 2003, 38, 380–387. [Google Scholar] [CrossRef]
- Da Costa, T.A.; Silva, M.J.; Alves, P.M.; Chica, J.E.; Barcelos, E.Z.; Giani, M.A.; Garlet, G.P.; da Silva, J.S.; Rodrigues Júnior, V.; Rodrigues, D.B.; et al. Inflammation Biomarkers of Advanced Disease in Nongingival Tissues of Chronic Periodontitis Patients. Mediat. Inflamm. 2015, 2015, 1–10. [Google Scholar] [CrossRef]
- Simonet, W.S.; Lacey, D.L.; Dunstan, C.R.; Kelley, M.; Chang, M.S.; Lüthy, R.; Nguyen, H.Q.; Wooden, S.; Bennett, L.; Boone, T.; et al. Osteoprotegerin: A novel secreted protein involved in the regulation of bone density. Cell 1997, 89, 309–319. [Google Scholar] [CrossRef]
- Bostanci, N.; Ilgenli, T.; Emingil, G.; Afacan, B.; Han, B.; Töz, H.; Atilla, G.; Hughes, F.J.; Belibasakis, G.N. Gingival crevicular fluid levels of RANKL and OPG in periodontal diseases: Implications of their relative ratio. J. Clin. Periodontol. 2007, 34, 370–376. [Google Scholar] [CrossRef]
- Mogi, M.; Otogoto, J.; Ota, N.; Togari, A. Differential expression of RANKL and osteoprotegerin in gingival crevicular fluid of patients with periodontitis. J. Dent. Res. 2004, 83, 166–169. [Google Scholar] [CrossRef] [PubMed]




| SDD Group | Placebo Group | |
|---|---|---|
| Male/Female | 11:4 | 10:5 |
| Mean age, years | 48.9 ± 6.6 | 49.2 ± 7.3 |
| Age range | 38–59 | 40–61 |
| Smokers (n) | 7 | 6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emingil, G.; Gürkan, A.; Tervahartiala, T.; Hernandez, M.; Özgül, S.; Sorsa, T.; Alassiri, S. Adjunctive Effects of a Sub-Antimicrobial Dose of Doxycycline on Clinical Parameters and Potential Biomarkers of Periodontal Tissue Catabolism. Dent. J. 2019, 7, 9. https://doi.org/10.3390/dj7010009
Emingil G, Gürkan A, Tervahartiala T, Hernandez M, Özgül S, Sorsa T, Alassiri S. Adjunctive Effects of a Sub-Antimicrobial Dose of Doxycycline on Clinical Parameters and Potential Biomarkers of Periodontal Tissue Catabolism. Dentistry Journal. 2019; 7(1):9. https://doi.org/10.3390/dj7010009
Chicago/Turabian StyleEmingil, Gülnur, Ali Gürkan, Taina Tervahartiala, Marcela Hernandez, Semiha Özgül, Timo Sorsa, and Saeed Alassiri. 2019. "Adjunctive Effects of a Sub-Antimicrobial Dose of Doxycycline on Clinical Parameters and Potential Biomarkers of Periodontal Tissue Catabolism" Dentistry Journal 7, no. 1: 9. https://doi.org/10.3390/dj7010009
APA StyleEmingil, G., Gürkan, A., Tervahartiala, T., Hernandez, M., Özgül, S., Sorsa, T., & Alassiri, S. (2019). Adjunctive Effects of a Sub-Antimicrobial Dose of Doxycycline on Clinical Parameters and Potential Biomarkers of Periodontal Tissue Catabolism. Dentistry Journal, 7(1), 9. https://doi.org/10.3390/dj7010009