Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Specimens
2.2. Each Selected Site Had to Show
- (1)
- (2)
- Bone height ≥12 mm.
- (3)
- Bone thickness ≥6 mm.
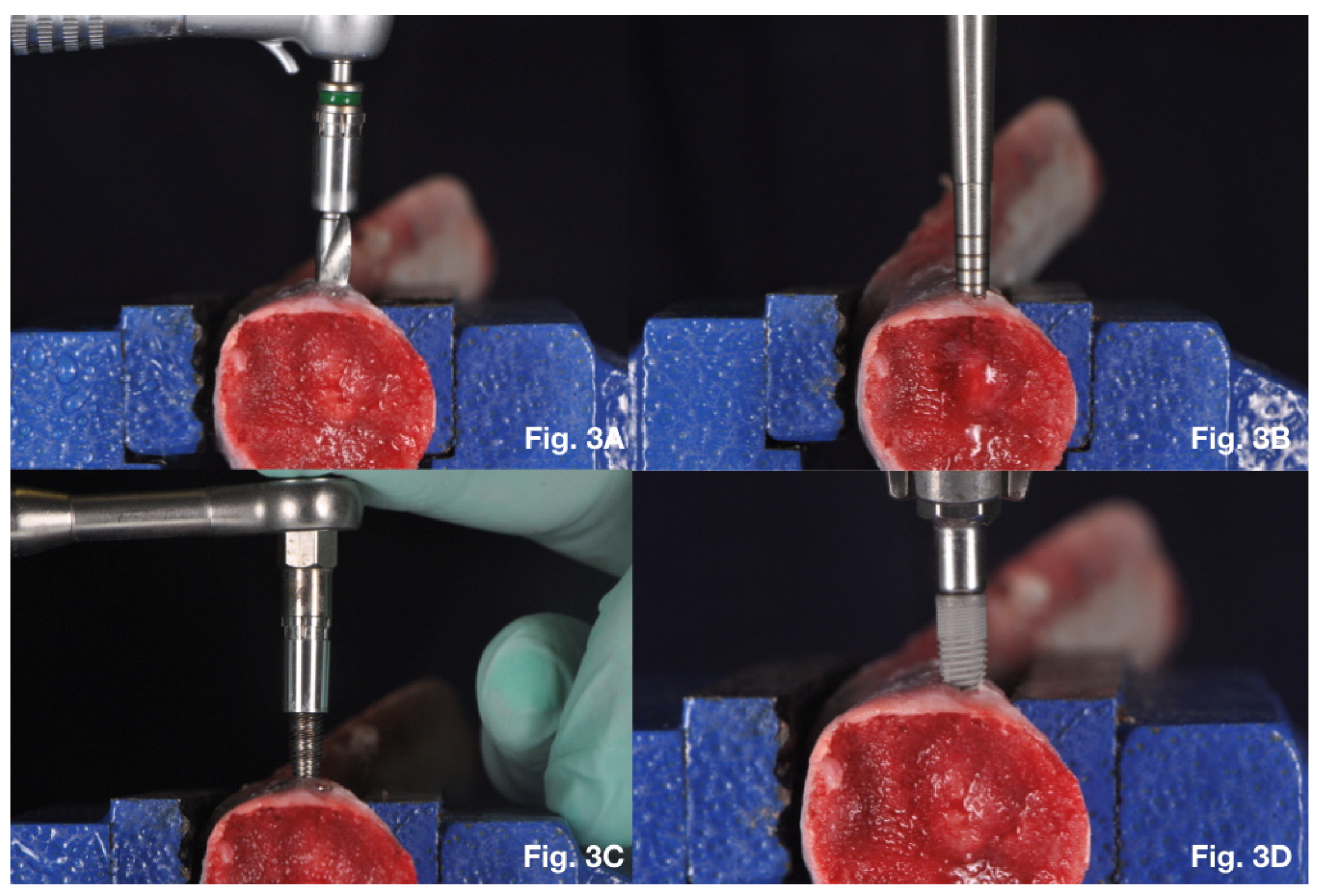
2.3. Surgical Procedures
2.4. Twist Drills Protocol
2.5. Summers Osteotomes Protocol
2.6. Bone Compactors Protocol
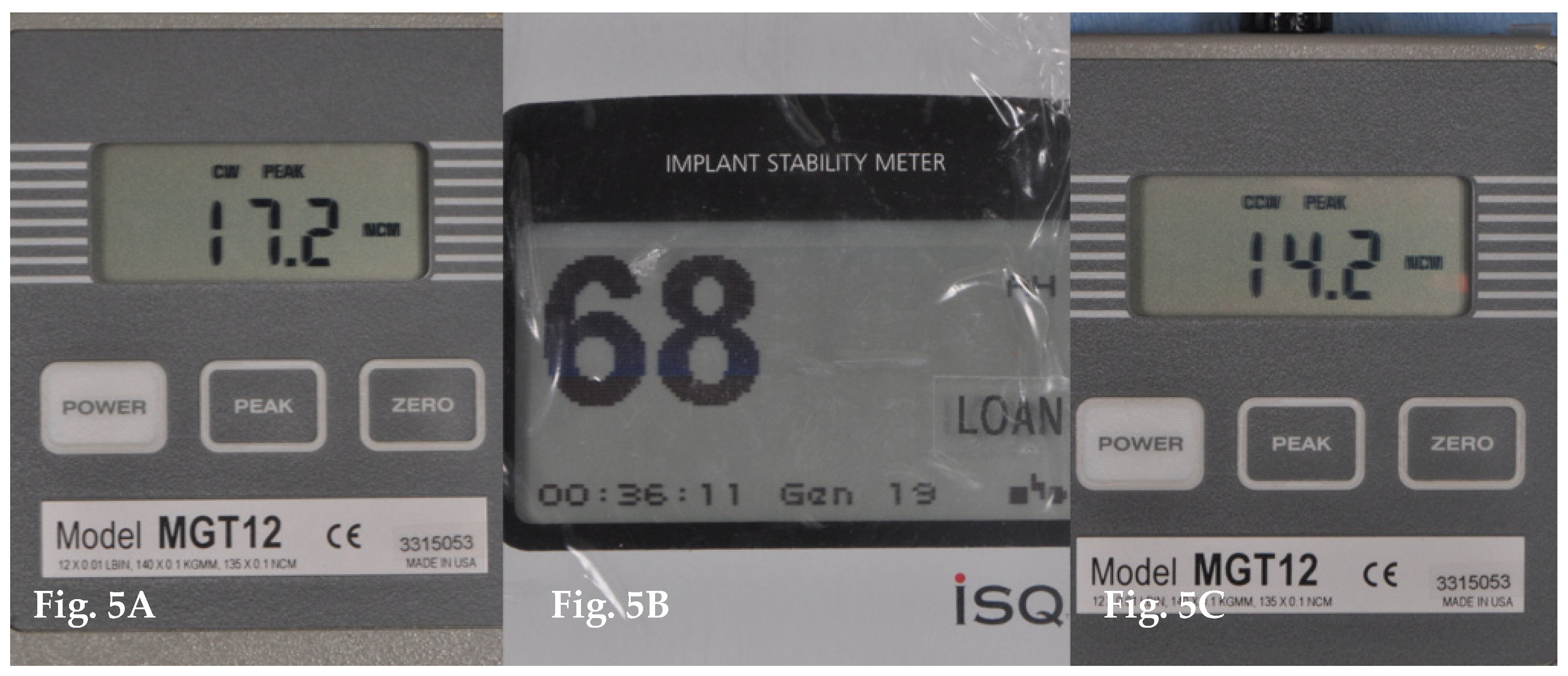
2.7. Analysis of Primary Implant Stability
Statistical Analysis
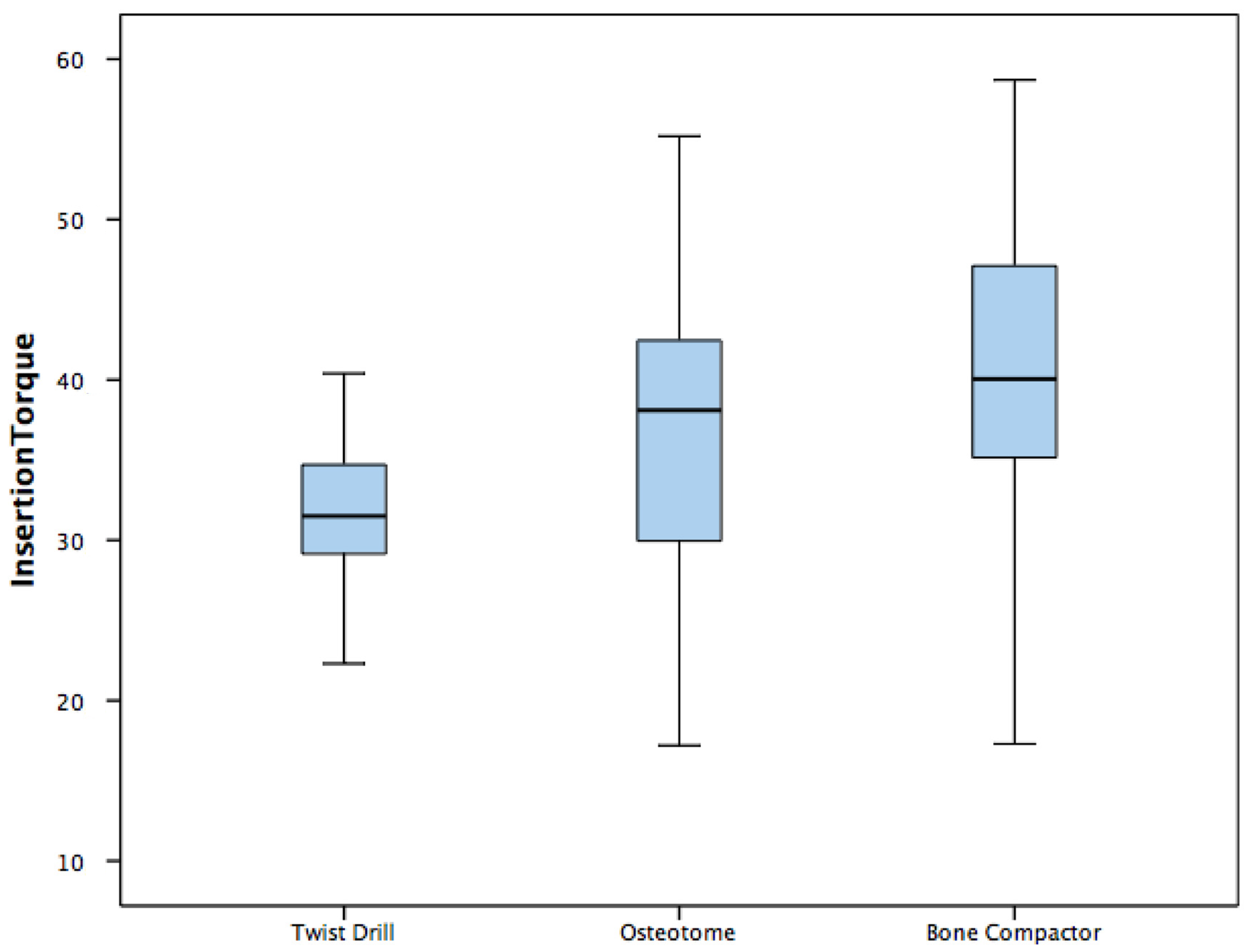
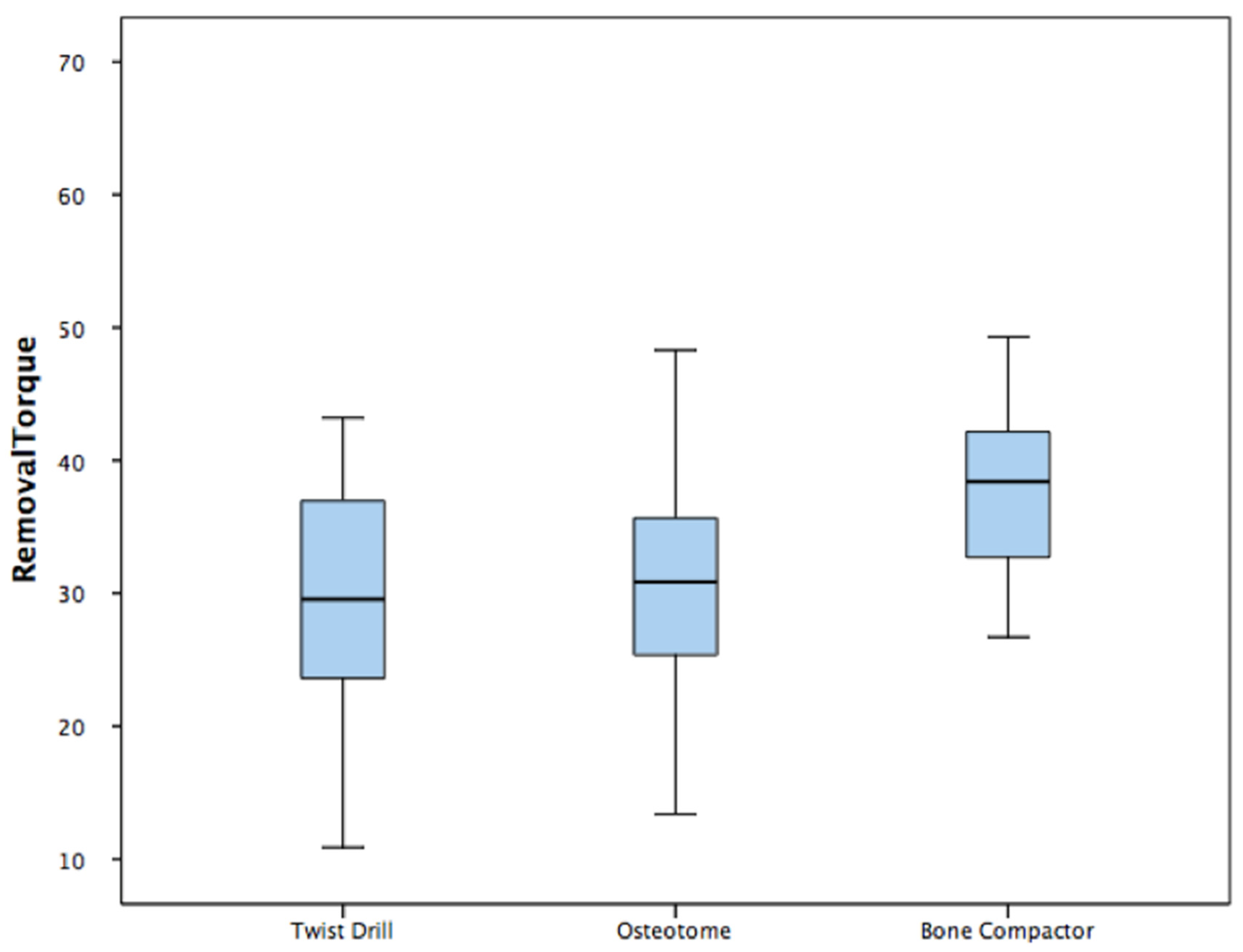
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| PS | primary implant stability |
| PIT | peak insertion torque |
| RFA | resonance frequency analysis |
| ISQ | implant stability quotient |
| PRT | peak removal torque |
References
- Figliuzzi, M.M.; Giudice, A.; Fortunato, L. Advanced implant-prosthetic rehabilitation: How to obtain a correct restoration of both functions and aesthetics in patients with complex combined dental and maxillofacial trauma: A case report and topical review of the literature. Case Rep. Dent. 2017, 2017, 7146126. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Branemark, P.I.; Hansson, H.A.; Lindstrom, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, I.; Tsuboi, Y.; Wada, E.; Suwa, H.; Iizuka, T. Influence of cortical bone thickness and implant length on implant stability at the time of surgery—Clinical, prospective, biomechanical, and imaging study. Bone 2005, 37, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Pagliani, L.; Sennerby, L.; Peterson, A.; Verrocchi, D.; Volpe, S.; Andersson, P. The relationship between resonance frequency analysis (RFA) and lateral displacement of dental implants: An in vitro study. J. Oral Rehab. 2013, 40, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Trisi, P.; Perfetto, G.; Baldwin, E.; Berardi, D.; Colagiovanni, M.; Scogna, G. Implant micromotion is related to peak insertion torque and bone density. Clin. Oral Implants Res. 2009, 20, 467–471. [Google Scholar] [CrossRef]
- Capparé, P.; Vinci, R.; Di Stefano, D.A.; Traini, T.; Pantaleo, G.; Gherlone, E.F.; Gastaldi, G. Correlation between Initial BIC and the Insertion Torque/Depth Integral Recorded with an Instantaneous Torque-Measuring Implant Motor: An in vivo Study. Clin. Implant Dent. Relat. Res. 2015, 17, e613–e620. [Google Scholar] [CrossRef]
- Makary, C.; Menhall, A.; Zammarie, C.; Lombardi, T.; Lee, S.Y.; Stacchi, C.; Park, K.B. Primary Stability Optimization by Using Fixtures with Different Thread Depth According To Bone Density: A Clinical Prospective Study on Early Loaded Implants. Materials 2019, 12, 2398. [Google Scholar] [CrossRef] [Green Version]
- Akca, K.; Chang, T.L.; Tedemir, I. Biomechanical aspects of initial intraosseous stability and implant design: A quantitative micro-morphometric analysis. Clin. Oral Implants Res. 2006, 17, 465–472. [Google Scholar] [CrossRef]
- Summers, R.B. A new concept in maxillary implant surgery: The osteotome technique. Compendium 1994, 15, 152–154. [Google Scholar]
- Slete, F.B.; Olin, P.; Prasad, H. Histomorphometric Comparison of 3 Osteotomy Techniques. Implant Dent. 2018, 27, 424–428. [Google Scholar] [CrossRef]
- Peñarrocha, M.; Pérez, H.; García, A.; Guarinos, J. Benign paroxysmal positional vertigo as a complication of osteotome expansion of the maxillary alveolar ridge. J. Oral Maxillofac. Surg. 2001, 59, 106–107. [Google Scholar] [CrossRef]
- Michael, R.N.; Carole, G. Bone classification: An objective scale of bone density using the computerized tomography scan. Clin. Oral Implants Res. 2001, 12, 79–84. [Google Scholar]
- Lekholm, U. Patient Selection and Preparation. Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry; Quintessence Publishing: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Figliuzzi, M.M.; Giudice, A.; Pileggi, S.; Pacifico, D.; Marrelli, M.; Tatullo, M.; Fortunato, L. Implant-prosthetic rehabilitation in bilateral agenesis of maxillary lateral incisors with a mini split crest. Case Rep. Dent. 2016, 2016, 3591321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsoulis, J.; Pazera, P.; Mericske-Stern, R. Prosthetically driven, computer-guided implant planning for the edentulous maxilla: A model study. Clin. Implant Dent. Relat. Res. 2009, 11, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, I.; Lekholm, U.; Holm, S.; Kultje, C. Evaluation of patient and implant characteristics as potential prognostic factors for oral implant failures. Int. J. Oral Maxillofac. Implant. 2005, 20, 220–230. [Google Scholar]
- Stacchi, C.; Lombardi, T.; Baldi, D.; Bugea, C.; Rapani, A.; Perinetti, G.; Verardi, S. Immediate Loading of Implant-Supported Single Crowns after Conventional and Ultrasonic Implant Site Preparation: A Multicenter Randomized Controlled Clinical Trial. Biomed Res. Int. 2018, 2018, 6817154. [Google Scholar] [CrossRef] [Green Version]
- Engquist, B.O.; Bergendal, T.; Kallus, T.; Linden, U. A retrospective multicenter evaluation of osseointegrated implants supporting overdentures. Int. J. Oral Maxillofac. Implants 1988, 3, 129–134. [Google Scholar]
- Friberg, B.; Jemt, T.; Lekholm, U. Early failures in 4641 consecutively placed Brånemark dental implants: A study from stage 1 surgery to the connection of completed prostheses. Int. J. Oral Maxillofac. Implants 1991, 6, 142–146. [Google Scholar]
- Sennerby, L.; Neil, M. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2000 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Elias, C.N.; Rocha, F.A.; Nascimento, A.L. Influence of implant shape, surface morphology, surgical technique and bone quality on the primary stability of dental implants. J. Mech. Behav. Biomed. Mater. 2012, 16, 169–180. [Google Scholar] [CrossRef]
- Nuria, G.V.; Rodrigo, A.G.; Vicente, R.S. In vitro evaluation of the type of implant bed preparation with osteotomes in bone type IV and its influence on the stability of two implant systems. Med. Oral Patol. Oral Cir. Bucal. 2009, 14, e455–e460. [Google Scholar]
- Yao, C.J.; Ma, L.; Mattheos, N. Can resonance frequency analysis detect narrow marginal bone defects around dental implants? An ex vivo animal pilot study. Aust. Dent. J. 2017, 62, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Misch, C.E. Density of bone: Effect on treatment plans, surgical approach, healing and progressive loading. Int. J. Oral Implant 1990, 6, 23–31. [Google Scholar]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implants Res. 2006, 17, 244–250. [Google Scholar] [CrossRef]
- Turkyilmaz, I.; Aksoy, U.; McGlumphy, E.A. Two alternative surgical techniques for enhancing primary implant stability in the posterior maxilla: A clinical study including bone density, insertion torque, and resonance frequency analysis data. Clin. Implant Dent. Relat. Res. 2008, 10, 231–237. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Piattelli, A. Influence of underpreparation on primary stability of implants inserted in poor quality bone sites: An in vitro study. J. Oral Maxillofac. Surg. 2015, 73, 1084–1088. [Google Scholar] [CrossRef]
- Tabassum, A.; Meijer, G.J.; Walboomers, X.F.; Jansen, J.A. Evaluation of primary and secondary stability of titanium implant using different surgical techniques. Clin. Oral Implants Res. 2014, 25, 487–492. [Google Scholar] [CrossRef]
- Glauser, G.; Naef, R.; Scharer, P. The osteotome technique—A different method of implant placement in the posterior maxilla. Implantologie 1998, 2, 103–120. [Google Scholar]
- Siddiqui, A.A.; Sosovicka, M. Lateral bone condensing and expansion for placement of endosseous dental implants: A new technique. J. Oral Implantol. 2006, 32, 87–94. [Google Scholar] [CrossRef]
- Nishioka, R.S.; Souza, F.A. Bone spreading and standardized dilation of horizontally resorbed bone: Technical considerations. Implant Dent. 2009, 18, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Di Fiore, A.; Sivolella, S.; Stocco, E.; Favero, V.; Stellini, E. Experimental Analysis of Temperature Differences During Implant Site Preparation: Continuous Drilling Technique Versus Intermittent Drilling Technique. J. Oral Implantol. 2018, 44, 46–50. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, A.; Assenza, B.; Carinci, F.; Donato, L.D.; Romani, G.L.; Merla, A. Infrared thermographic evaluation of temperature modifications induced during implant site preparation with cylindrical versus conical drills. Clin. Implant Dent. Relat. Res. 2011, 13, 319–323. [Google Scholar] [CrossRef]
- Baldi, D.; Lombardi, T.; Colombo, J.; Cervino, G.; Perinetti, G.; Di Lenarda, R.; Stacchi, C. Correlation between insertion torque and implant stability quotient in tapered implants with knife-edge thread design. Biomed. Res. Int. 2018, 2018, 7201093. [Google Scholar] [CrossRef]
- Lages, F.S.; Dhelfeson, W.D.-d.O.; Fernando, O.C. Relationship between implant stability measurements obtained by insertion torque and resonance frequency analysis: A systematic review. Clin. Implant Dent. Relat. Res. 2018, 20, 26–33. [Google Scholar] [CrossRef]
- Meredith, N.; Alleyne, D.; Cawley, P. Quantitative determination of the stability of the implant-tissue interface using resonance frequency analysis. Clin. Oral Implants Res. 1996, 7, 261–267. [Google Scholar] [CrossRef]
- Meredith, N.; Books, K.; Fribergs, B.; Jemt, T.; Sennerby, L. Resonance frequency measurements of implant stability in viva. A cross-sectional and longitudinal study of resonance frequency measurements on implants in the edentulous and partially dentate maxilla. Clin. Oral Implants Res. 1997, 8, 226–233. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Insertion Torque | RFA | Removal Torque | Insertion Torque | RFA | Removal Torque | Insertion Torque | RFA | Removal Torque | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 22.4 | 68 | 23.4 | 1 | 24.8 | 72 | 23.8 | 1 | 33.2 | 73 | 38.4 |
| 2 | 46.3 | 74 | 42.2 | 2 | 47.1 | 78 | 66.8 | 2 | 53.1 | 75 | 44.9 |
| 3 | 22.3 | 67 | 10.9 | 3 | 25 | 65 | 26.9 | 3 | 29 | 75 | 30.3 |
| 4 | 30.5 | 71 | 21.6 | 4 | 29.5 | 65 | 13.4 | 4 | 37.5 | 65 | 26.7 |
| 5 | 44.5 | 68 | 29.9 | 5 | 44 | 62 | 33.9 | 5 | 46.9 | 70 | 40.7 |
| 6 | 40.4 | 79 | 37.7 | 6 | 39.9 | 65 | 30.2 | 6 | 47.2 | 78 | 47.3 |
| 7 | 32.7 | 68 | 43.2 | 7 | 38.2 | 72 | 23.8 | 7 | 37.2 | 73 | 38.4 |
| 8 | 34.3 | 72 | 36.2 | 8 | 45.9 | 75 | 35.9 | 8 | 47 | 75 | 49.3 |
| 9 | 32.1 | 69 | 30.9 | 9 | 47.9 | 80 | 32.1 | 9 | 55.4 | 77 | 39.5 |
| 10 | 29.9 | 67 | 22.8 | 10 | 35.6 | 74 | 29.2 | 10 | 39.9 | 75 | 36.2 |
| 11 | 29.2 | 68 | 27.8 | 11 | 28.3 | 67 | 30.3 | 11 | 36.2 | 76 | 31.3 |
| 12 | 35.1 | 69 | 28.8 | 12 | 40.9 | 72 | 35.9 | 12 | 41.7 | 82 | 43.6 |
| 13 | 29.7 | 69 | 29.2 | 13 | 38 | 73 | 31.4 | 13 | 48.9 | 76 | 37.2 |
| 14 | 48.2 | 70 | 43.1 | 14 | 55.2 | 74 | 48.3 | 14 | 58.7 | 77 | 57 |
| 15 | 32 | 67 | 31 | 15 | 38.3 | 71 | 35.4 | 15 | 40.2 | 73 | 38.2 |
| 16 | 29.1 | 62 | 27.8 | 16 | 35.7 | 72 | 34.6 | 16 | 34.1 | 75 | 34.1 |
| 17 | 31 | 70 | 43.2 | 17 | 36.2 | 73 | 23.8 | 17 | 39.9 | 75 | 38.4 |
| 18 | 34.2 | 72 | 32.2 | 18 | 40.1 | 76 | 38.6 | 18 | 40.5 | 80 | 40 |
| 19 | 14.1 | 75 | 11.2 | 19 | 17.2 | 68 | 14.2 | 19 | 17.3 | 75 | 14.2 |
| 20 | 24.8 | 68 | 23.8 | 20 | 30.4 | 71 | 30 | 20 | 33.2 | 73 | 31 |
| Variable | Twist Drills (TD) | Summers Osteotomes (SO) | Bone Compactors (BC) | P (Anova) |
|---|---|---|---|---|
| Insertion Torque (Ncm) | 32.14 ± 8.27 | 36.94 ± 9.3 | 40.85 ± 9.57 | 0.013 * |
| RFA (ISQ) | 69.95 ± 3.57 | 71.25 ± 4.66 | 74.9 ± 3.51 | 0.0001 * |
| Removal Torque (Ncm) | 29.84 ± 9.48 | 31.92 ± 11.42 | 37.83 ± 8.98 | 0.039 * |
| Variable | P (Post Hoc Tukey) | |
|---|---|---|
| Insertion Torque | Twist Drill vs Osteotome Twist Drill vs Bone Compactor Osteotome vs Bone Compactor | 0.226 0.01 * 0.36 |
| ISQ | Twist Drill vs Osteotome Twist Drill vs Bone Compactor Osteotome vs Bone Compactor | 0.41 0.0001 * 0.014 * |
| Removal Torque | Twist Drill vs Osteotome Twist Drill vs Bone Compactor Osteotome vs Bone Compactor | 0.79 0.038 * 0.16 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attanasio, F.; Antonelli, A.; Brancaccio, Y.; Averta, F.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dent. J. 2020, 8, 21. https://doi.org/10.3390/dj8010021
Attanasio F, Antonelli A, Brancaccio Y, Averta F, Figliuzzi MM, Fortunato L, Giudice A. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dentistry Journal. 2020; 8(1):21. https://doi.org/10.3390/dj8010021
Chicago/Turabian StyleAttanasio, Ferdinando, Alessandro Antonelli, Ylenia Brancaccio, Fiorella Averta, Michele Mario Figliuzzi, Leonzio Fortunato, and Amerigo Giudice. 2020. "Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study" Dentistry Journal 8, no. 1: 21. https://doi.org/10.3390/dj8010021
APA StyleAttanasio, F., Antonelli, A., Brancaccio, Y., Averta, F., Figliuzzi, M. M., Fortunato, L., & Giudice, A. (2020). Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dentistry Journal, 8(1), 21. https://doi.org/10.3390/dj8010021