A Comparative Assessment of Pain Caused by the Placement of Banded Orthodontic Appliances with and without Low-Level Laser Therapy: A Randomized Controlled Prospective Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Intervention
2.3. Assessment of Pain
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Abdelrahman, R.S.; Al-Nimri, K.S.; Al Maaitah, E.F. Pain experience during initial alignment with three types of nickel-titanium archwires: A prospective clinical trial. Angle Orthod. 2015, 85, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Nucera, R.; Perillo, L.; Paiusco, A.; Caccianiga, G. Is low-level laser therapy an effective method to alleviate pain induced by active orthodontic alignment archwire? A randomized clinical trial. J. Evid. Based Dent. Pract. 2019, 19, 71–78. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Nucera, R.; Leonardi, R.; Paiusco, A.; Baldoni, M.; Caccianiga, G. A comparative assessment of the efficiency of orthodontic treatment with and without photobiomodulation during mandibular de-crowding in young subjects: A single-center, single blind randomized controlled trial. Photobiomodul. Photomed. Laser Surg. 2020, in press. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isola, G.; Anastasi, G.P.; Matarese, G.; Williams, R.C.; Cutroneo, G.; Bracco, P.; Piancino, M.G. Functional and molecular outcomes of the human masticatory muscles. Oral Dis. 2018, 24, 1428–1441. [Google Scholar] [CrossRef] [PubMed]
- Tortamano, A.; Lenzi, D.C.; Haddad, A.C.; Bottino, M.C.; Dominguez, G.C.; Vigorito, J.W. Low-level laser therapy for pain caused by placement of the first orthodontic archwire: A randomized clinical trial. Am. J. Orthod. Dentofacial. Orthop. 2009, 136, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Nucera, R.; Matarese, G.; Portelli, M.; Cervino, G.; Lo Giudice, G.; Militi, A.; Caccianiga, G.; Cicciù, M.; Cordasco, G. Analysis of resistance to sliding expressed during first order correction with conventional and self-ligating brackets: An in-vitro study. Int. J. Clin. Exp. Med. 2016, 9, 15575–15581. [Google Scholar]
- Isola, G.; Perillo, L.; Migliorati, M.; Matarese, M.; Dalessandri, D.; Grassia, V.; Alibrandi, A.; Matarese, G. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur. J. Orthod. 2019, 41, 117–124. [Google Scholar] [CrossRef]
- Cutroneo, G.; Piancino, M.G.; Ramieri, G.; Bracco, P.; Vita, G.; Isola, G.; Vermiglio, G.; Favaloro, A.; Anastasi, G.; Trimarchi, F. Expression of muscle-specific integrins in masseter muscle fibers during malocclusion disease. Int. J. Mol. Med. 2012, 30, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Marie, S.S.; Powers, M.; Sheridan, J.J. Vibratory stimulation as a method of reducing pain after orthodontic appliance adjustment. J. Clin. Orthod. 2003, 37, 205–208. [Google Scholar]
- Roth, P.M.; Thrash, W.J. Effect of transcutaneous electrical nerve stimulation for controlling pain associated with orthodontic tooth movement. Am. J. Orthod. Dentofacial. Orthop. 1986, 90, 132–138. [Google Scholar] [CrossRef]
- Sousa, M.V.; Pinzan, A.; Consolaro, A.; Henriques, J.F.; de Freitas, M.R. Systematic literature review: Influence of low level laser on orthodontic movement and pain control in humans. Photomed. Laser Surg. 2014, 32, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Matarese, G.; Currò, M.; Isola, G.; Caccamo, D.; Vecchio, M.; Giunta, M.L.; Ramaglia, L.; Cordasco, G.; Williams, R.C.; Ientile, R. Transglutaminase 2 up-regulation is associated with RANKL/OPG pathway in cultured HPDL cells and THP-1-differentiated macrophages. Amino Acids 2015, 47, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Currò, M.; Matarese, G.; Isola, G.; Caccamo, D.; Ventura, V.P.; Cornelius, C.; Lentini, M.; Cordasco, G.; Ientile, R. Differential expression of transglutaminase genes in patients with Chronic Periodontitis. Oral Dis. 2014, 20, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Caccianiga, G.; Paiusco, A.; Perillo, L.; Nucera, R.; Pinsino, A.; Maddalone, M.; Cordasco, G.; Lo Giudice, A. Does Low-Level Laser Therapy Enhance the Efficiency of Orthodontic Dental Alignment? Results from a Randomized Pilot Study. Photomed. Laser Surg. 2017, 35, 421–426. [Google Scholar] [CrossRef]
- Isola, G.; Alibrandi, A.; Pedullà, E.; Grassia, V.; Ferlito, S.; Perillo, L.; Rapisarda, E. Analysis of the effectiveness of Lornoxicam and Flurbiprofen on management of pain and sequelae following third molar surgery: A randomized, controlled, clinical trial. J. Clin. Med. 2019, 8, 325. [Google Scholar] [CrossRef] [Green Version]
- Piancino, M.G.; Isola, G.; Cannavale, R.; Cutroneo, G.; Vermiglio, G.; Bracco, P.; Anastasi, G.P. From periodontal mechanoreceptors to chewing motor control: A systematic review. Arch. Oral Biol. 2017, 78, 109–121. [Google Scholar] [CrossRef]
- Caccianiga, G.; Crestale, C.; Cozzani, M.; Piras, A.; Mutinelli, S.; Lo Giudice, A.; Cordasco, G. Low-level laser therapy and invisible removal aligners. J. Biol. Regul. Homeost. Agents. 2016, 30, 107–113. [Google Scholar]
- Sonesson, M.; De Geer, E.; Subraian, J.; Petrén, S. Efficacy of low-level laser therapy in accelerating tooth movement, preventing relapse and managing acute pain during orthodontic treatment in humans: A systematic review. BMC Oral Health 2017, 17, 11. [Google Scholar] [CrossRef] [Green Version]
- Caccianiga, G.; Lo Giudice, A.; Paiusco, A.; Portelli, M.; Militi, A.; Baldoni, M.; Nucera, R. Maxillary Orthodontic Expansion Assisted by Unilateral Alveolar Corticotomy and Low-Level Laser Therapy: A Novel Approach for Correction of a Posterior Unilateral Cross-Bite in Adults. J. Lasers Med. Sci. 2019, 10, 225–229. [Google Scholar] [CrossRef]
- Nucera, R.; Militi, A.; Lo Giudice, A.; Longo, V.; Fastuca, R.; Caprioglio, A.; Cordasco, G.; Papadopoulos, M.A. Skeletal and Dental Effectiveness of Treatment of Class II Malocclusion With Headgear: A Systematic Review and Meta-analysis. J. Evid. Based Dent. Pract. 2018, 18, 41–58. [Google Scholar] [CrossRef]
- Cronshaw, M.; Parker, S.; Anagnostaki, E.; Lynch, E. Systematic Review of Orthodontic Treatment Management with Photobiomodulation Therapy. Photobiomodul. Photomed. Laser Surg. 2019, 37, 862–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo Giudice, A.; Fastuca, R.; Portelli, M.; Militi, A.; Bellocchio, M.; Spinuzza, P.; Briguglio, F.; Caprioglio, A.; Nucera, R. Effects of rapid vs slow maxillary expansion on nasal cavity dimensions in growing subjects: A methodological and reproducibility study. Eur. J. Paediatr. Dent. 2017, 18, 299–304. [Google Scholar] [PubMed]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain. 2018, 18, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Shapiro Wilk Test. Available online: http://sdittami.altervista.org/shapirotest/ShapiroTest.html (accessed on 3 March 2020).
- Farrar, J.T.; Young, P., Jr.; La Moreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Brewer, I.; Leonardi, R.; Roberts, N.; Bagnato, G. Pain threshold and temporomandibular function in systemic sclerosis: Comparison with psoriatic arthritis. Clin. Rheumatol. 2018, 37, 1861–1867. [Google Scholar] [CrossRef]
- Turhani, D.; Scheriau, M.; Kapral, D.; Benesch, T.; Jonke, E.; Bantleon, H.P. Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapy. Am. J. Orthod. Dentofacial. Orthop. 2006, 130, 371–377. [Google Scholar] [CrossRef]
- Doshi–Mehta, G.; Bhad–Patil, W.A. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: A clinical investigation. Am. J. Orthod. Dentofacial. Orthop. 2012, 141, 289–297. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Lo Giudice, G.; Briguglio, F.; Alibrandi, A.; Crupi, A.; Cordasco, G.; Ramaglia, L. A New Approach for the Treatment of Lateral Periodontal Cysts with an 810-nm Diode Laser. Int. J. Periodontics Restor. Dent. 2017, 37, e120–e129. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Muraglie, S.; Leonardi, R.M.; Lo Giudice, A. Assessment Of vitamin C And Antioxidants Profiles In Saliva And Serum In Patients With Periodontitis And Ischemic Heart Disease. Nutrients 2019, 11, 2956. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Matarese, G.; Ramaglia, L.; Pedullà, E.; Rapisarda, E.; Iorio-Siciliano, V. Association between periodontitis and glycosylated haemoglobin before diabetes onset: A cross-sectional study. Clin. Oral. Investig. 2019. [Google Scholar] [CrossRef]
- Nucera, R.; Lo Giudice, A.; Bellocchio, A.M.; Spinuzza, P.; Caprioglio, A.; Perillo, L.; Matarese, G.; Cordasco, G. Bone and cortical bone thickness of mandibular buccal shelf for mini-screw insertion in adults. Angle Orthod. 2017, 87, 745–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, J. Relief from chronic pain by low power laser irradiation. Neurosci. Lett. 1983, 43, 339–344. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, M.; Ramaglia, L.; Cicciù, M.; Matarese, G. Evaluation of the efficacy of celecoxib and ibuprofen on postoperative pain, swelling, and mouth opening after surgical removal of impacted third molars: A randomized, controlled clinical trial. Int. J. Oral Maxillofac. Surg. 2019, 48, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, G.; Lo Giudice, R.; Matarese, G.; Isola, G.; Cicciù, M.; Terranova, A.; Palaia, G.; Romeo, U. Evaluation of magnification systems in restorative dentistry. An in-vitro study. Dent. Cadmos 2015, 83, 296–305. [Google Scholar] [CrossRef]
- Harris, D.M. Biomolecular mechanisms of laser biostimulation. J. Clin. Laser Med. Surg. 1991, 277–280. [Google Scholar] [CrossRef]
- Isola, G.; Alibrandi, A.; Rapisarda, E.; Matarese, G.; Williams, R.C.; Leonardi, R. Association of vitamin d in patients with periodontal and cardiovascular disease: A cross-sectional study. J. Periodontal. Res. 2020, in press. [Google Scholar] [CrossRef]
- Esper, M.A.; Nicolau, R.A.; Arisawa, E.A. The effect of two phototherapy protocols on pain control in orthodontic procedure—A preliminary clinical study. Lasers Med. Sci. 2011, 26, 657–663. [Google Scholar] [CrossRef]
- Eslamian, L.; Borzabadi-Farahani, A.; Hassanzadeh-Azhiri, A.; Badiee, M.R.; Fekrazad, R. The effect of 810-nm low-level laser therapy on pain caused by orthodontic elastomeric separators. Lasers Med. Sci. 2014, 29, 559–564. [Google Scholar] [CrossRef]
- Almallah, M.M.; Almahdi, W.H.; Hajeer, M.Y. Evaluation of Low Level Laser Therapy on Pain Perception Following Orthodontic Elastomeric Separation: A Randomized Controlled Trial. Clin. Diagn. Res. 2016, 10, ZC23–ZC28. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, M.; Ramaglia, L.; Iorio-Siciliano, V.; Cordasco, G.; Matarese, G. Efficacy of a drug composed of herbal extracts on postoperative discomfort after surgical removal of impacted mandibular third molar: A randomized, triple-blind, controlled clinical trial. Clin. Oral Investig. 2019, 23, 2443–2453. [Google Scholar] [CrossRef]
- Bicakci, A.A.; Kocoglu-Altan, B.; Toker, H.; Mutaf, I.; Sumer, Z. Efficiency of low-level laser therapy in reducing pain induced by orthodontic forces. Photomed. Laser Surg. 2012, 30, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Heidari, S.; Torkan, S. Laser Applications in Orthodontics. J. Lasers Med. Sci. 2013, 4, 151–158. [Google Scholar] [PubMed]
- Isola, G.; Polizzi, A.; Santonocito, S.; Alibrandi, A.; Ferlito, S. Expression of Salivary And Serum Malondialdehyde And Lipid Profile Of Patients With Periodontitis And Coronary Heart Disease. Int. J. Mol. Sci. 2019, 20, 6061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, H.M.; Lew, K.K.; Tay, D.K. A clinical investigation of the efficacy of low level laser therapy in reducing orthodontic post adjustment pain. Am. J. Orthod. Dentofacial. Orthop. 1995, 108, 614–622. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Alibrandi, A.; Indelicato, F.; Ferlito, S. Analysis of Endothelin-1 concentrations in individuals with periodontitis. Sci. Rep. 2020, 10, 1652. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Alibrandi, A.; Currò, M.; Matarese, M.; Ricca, S.; Matarese, G.; Ientile, R.; Kocher, T. Evaluation of salivary and serum ADMA levels in patients with periodontal and cardiovascular disease as subclinical marker of cardiovascular risk. J. Periodontol 2020. [Google Scholar] [CrossRef]
- Isola, G.; Ramaglia, L.; Cordasco, G.; Lucchese, A.; Fiorillo, L.; Matarese, G. The effect of a functional appliance in the management of temporomandibular joint disorders in patients with juvenile idiopathic arthritis. Minerva Stomatol. 2017, 66, 1–8. [Google Scholar] [CrossRef]
- Matarese, G.; Isola, G.; Alibrandi, A.; Lo Gullo, A.; Bagnato, G.; Cordasco, G.; Perillo, L. Occlusal and MRI characterizations in systemic sclerosis patients: A prospective study from Southern Italian cohort. Jt. Bone Spine 2016, 83, 57–62. [Google Scholar] [CrossRef]
- Cavuoti, S.; Matarese, G.; Isola, G.; Abdolreza, J.; Femiano, F.; Perillo, L. Combined orthodontic-surgical management of a transmigrated mandibular canine. Angle Orthod. 2016, 86, 681–691. [Google Scholar] [CrossRef] [Green Version]
- Lo Giudice, G.; Lo Giudice, A.; Isola, G.; Fabiano, F.; Artemisia, A.; Fabiano, V.; Nucera, R.; Matarese, G. Evaluation of bond strength and detachment interface distribution of different bracket base designs. Acta Medica Mediterr. 2015, 31, 585. [Google Scholar]
- Isola, G.; Matarese, G.; Alibrandi, A.; Dalessandri, D.; Migliorati, M.; Pedullà, E.; Rapisarda, E. Comparison of Effectiveness of Etoricoxib and Diclofenac on Pain and Perioperative Sequelae After Surgical Avulsion of Mandibular Third Molars: A Randomized, Controlled, Clinical Trial. Clin. J. Pain 2019, 35, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Matarese, G.; Isola, G.; Ramaglia, L.; Dalessandri, D.; Lucchese, A.; Alibrandi, A.; Fabiano, F.; Cordasco, G. Periodontal biotype: Characteristic, prevalence and dimensions related to dental malocclusion. Minerva Stomatol. 2016, 65, 231–238. [Google Scholar] [PubMed]
- Isola, G.; Lo Giudice, A.; Polizzi, A.; Alibrandi, A.; Patini, R.; Ferlito, S. Periodontitis and Tooth Loss Have Negative Systemic Impact on Circulating Progenitor Cell Levels: A Clinical Study. Genes (Basel) 2019, 10, 1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perillo, L.; Isola, G.; Esercizio, D.; Iovane, M.; Triolo, G.; Matarese, G. Differences in craniofacial characteristics in Southern Italian children from Naples: A retrospective study by cephalometric analysis. Eur. J. Paediatr. Dent. 2013, 14, 195–198. [Google Scholar]
- Briguglio, F.; Briguglio, E.; Briguglio, R.; Cafiero, C.; Isola, G. Treatment of intrabony periodontal defects by a re-absorbable biopolymer of hyaluronic acid: A randomized clinical trial. Quintessence Int. 2013, 3, 231–240. [Google Scholar]
- Leonardi, R.; Lo Giudice, A.; Rugeri, M.; Muraglie, S.; Cordasco, G.; Barbato, E. Three-dimensional evaluation on digital casts of maxillary palatal size and morphology in patients with functional posterior crossbite. Eur. J. Orthod. 2018, 40, 556–562. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Caccianiga, G.; Crimi, S.; Cavallini, C.; Leonardi, R. Frequency and type of ponticulus posticus in a longitudinal sample of nonorthodontically treated patients: relationship with gender, age, skeletal maturity, and skeletal malocclusion. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 291–297. [Google Scholar] [CrossRef]
- Leonardi, R.; Muraglie, S.; Lo Giudice, A.; Aboulazm, K.S.; Nucera, R. Evaluation of mandibular symmetry and morphology in adult patients with unilateral posterior crossbite: a CBCT study using a surface-to-surface matching technique. Eur. J. Orthod. 2020, cjz106. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Cordasco, G.; Rotondo, F.; Crupi, A.; Ramaglia, L. Anticoagulant therapy in patients undergoing dental interventions: a critical review of the literature and current perspectives. Minerva Stomatol. 2015, 64, 21–46. [Google Scholar]
- Cannavale, R.; Matarese, G.; Isola, G.; Grassia, V.; Perillo, L. Early treatment of an ectopic premolar to prevent molar-premolar transposition. Am. J. Orthod. Dentofacial Orthop. 2013, 143, 559–569. [Google Scholar] [CrossRef]
- Matarese, G.; Isola, G.; Anastasi, G.P.; Cutroneo, G.; Favaloro, A.; Vita, G.; Cordasco, G.; Milardi, D.; Zizzari, V.L.; Tetè, S.; et al. Transforming Growth Factor Beta 1 and Vascular Endothelial Growth Factor levels in the pathogenesis of periodontal disease. Eur. J. Inflamm. 2013, 11, 479–488. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Matarese, M.; Briguglio, F.; Grassia, V.; Picciolo, G.; Fiorillo, L.; Matarese, G. Effectiveness of Low-Level Laser Therapy during Tooth Movement: A Randomized Clinical Trial. Materials (Basel). 2019, 12, 2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isola, G.; Williams, R.C.; Lo Gullo, A.; Ramaglia, L.; Matarese, M.; Iorio-Siciliano, V.; Cosio, C.; Matarese, G. Risk association between scleroderma disease characteristics, periodontitis, and tooth loss. Clin. Rheumatol. 2017, 36, 2733–2741. [Google Scholar] [CrossRef]
- Perillo, L.; Padricelli, G.; Isola, G.; Femiano, F.; Chiodini, P.; Matarese, G. Class II malocclusion division 1: a new classification method by cephalometric analysis. Eur. J. Paediatr. Dent. 2012, 13, 192–196. [Google Scholar] [PubMed]
- Seifi, M.; Vahid-Dastjerdi, E. Tooth Movement Alterations by Different Low Level Laser Protocols: A Literature Review. J. Lasers Med. Sci. 2015, 6, 1–5. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sample Characteristics | Total Sample (n = 56) | TG (n = 19) | CG (n = 17) | PG (n = 20) | Significance * |
|---|---|---|---|---|---|
| Gender: male/female | 29/27 | 9/10 | 10/7 | 8/12 | NS |
| Age, year: mean (SD) | 12.03 (1.30) | 12.05(1.31) | 12.41 (1.32) | 11.7 (1.26) | NS |
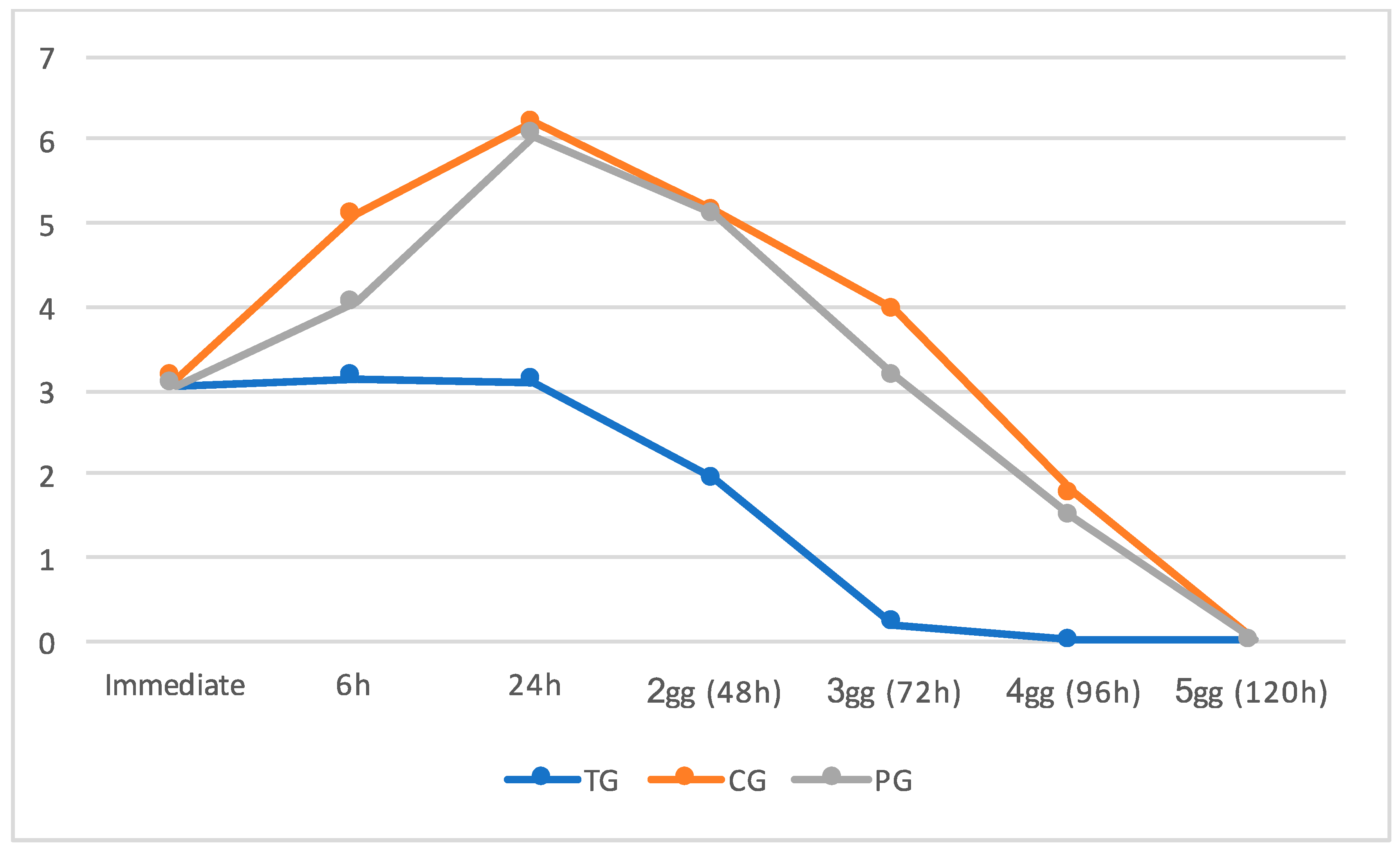
| Time Schedule | TG (n = 27) Median (Min-Max) | CG (n = 29) Median (Min-Max) | PG (n = 28) Median (Min-Max) | Significance * |
|---|---|---|---|---|
| MPS | 4 (2–4), 95% CI: 3.05–3.79 | 6 (5–7), 95% CI: 5.72–6.52 | 6 (5–7), 95% CI: 5.87–6.53 | <0.001 |
| Immediate | 3 (2–4), 95% CI: 2.75–3.35 | 3 (2–4), 95% CI: 2.67–3.44 | 3 (2–4), 95% CI: 2.80–3.50 | NS |
| 6 h | 3 (2–4), 95% CI: 2.83–3.49 | 4 (3–5), 95% CI: 3.67–4.44 | 5 (4–6), 95% CI: 4.76–5.44 | <0.001 |
| 24 h | 3 (2–4), 95% CI: 2.72–3.50 | 6 (5–7), 95% CI: 5.67–6.44 | 6 (5–7), 95% CI: 5.87–6.53 | <0.001 |
| 48 h | 2 (1–3), 95% CI: 1.65–2.25 | 5 (4–6), 95% CI: 4.76–5.48 | 5 (3–7), 95% CI: 4.64–5.66 | <0.001 |
| 72 h | 0 (0–1), 95% CI: 0.01–0.41 | 3 (2–5), 95% CI: 2.72–3.63 | 4 (1–5), 95% CI: 3.44–4.46 | <0.001 |
| 96 h | 0 (0–0), 95% CI: 0.00–0.00 | 1 (0–3), 95% CI: 1.10–1.84 | 2 (0–3), 95% CI: 1.35–2.15 | <0.001 |
| 120 h | 0 (0–0), 95% CI: 0.00–0.00 | 0 (0–0), 95% CI: 0.00–0.00 | 0 (0–0), 95% CI: 0.00–0.00 | Not Significant |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicotra, C.; Polizzi, A.; Zappalà, G.; Leonida, A.; Indelicato, F.; Caccianiga, G. A Comparative Assessment of Pain Caused by the Placement of Banded Orthodontic Appliances with and without Low-Level Laser Therapy: A Randomized Controlled Prospective Study. Dent. J. 2020, 8, 24. https://doi.org/10.3390/dj8010024
Nicotra C, Polizzi A, Zappalà G, Leonida A, Indelicato F, Caccianiga G. A Comparative Assessment of Pain Caused by the Placement of Banded Orthodontic Appliances with and without Low-Level Laser Therapy: A Randomized Controlled Prospective Study. Dentistry Journal. 2020; 8(1):24. https://doi.org/10.3390/dj8010024
Chicago/Turabian StyleNicotra, Carmelo, Alessandro Polizzi, Graziano Zappalà, Alessandro Leonida, Francesco Indelicato, and Gianluigi Caccianiga. 2020. "A Comparative Assessment of Pain Caused by the Placement of Banded Orthodontic Appliances with and without Low-Level Laser Therapy: A Randomized Controlled Prospective Study" Dentistry Journal 8, no. 1: 24. https://doi.org/10.3390/dj8010024
APA StyleNicotra, C., Polizzi, A., Zappalà, G., Leonida, A., Indelicato, F., & Caccianiga, G. (2020). A Comparative Assessment of Pain Caused by the Placement of Banded Orthodontic Appliances with and without Low-Level Laser Therapy: A Randomized Controlled Prospective Study. Dentistry Journal, 8(1), 24. https://doi.org/10.3390/dj8010024