Oral Hygiene Awareness and Practices among a Sample of Primary School Children in Rural Bangladesh

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
- Ne:
- Age:
- Sex:
- Which class do you read in:
- Bushing frequency
- Once daily
- Twice daily
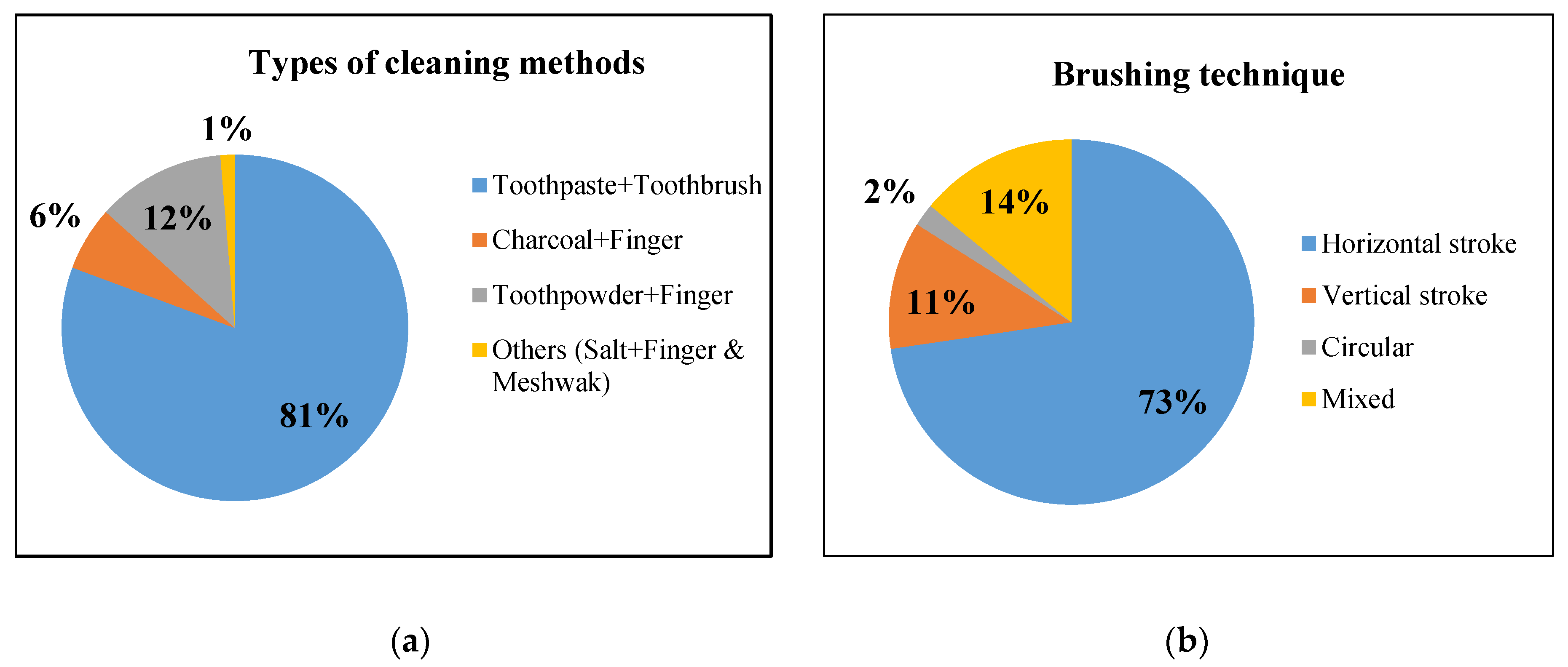
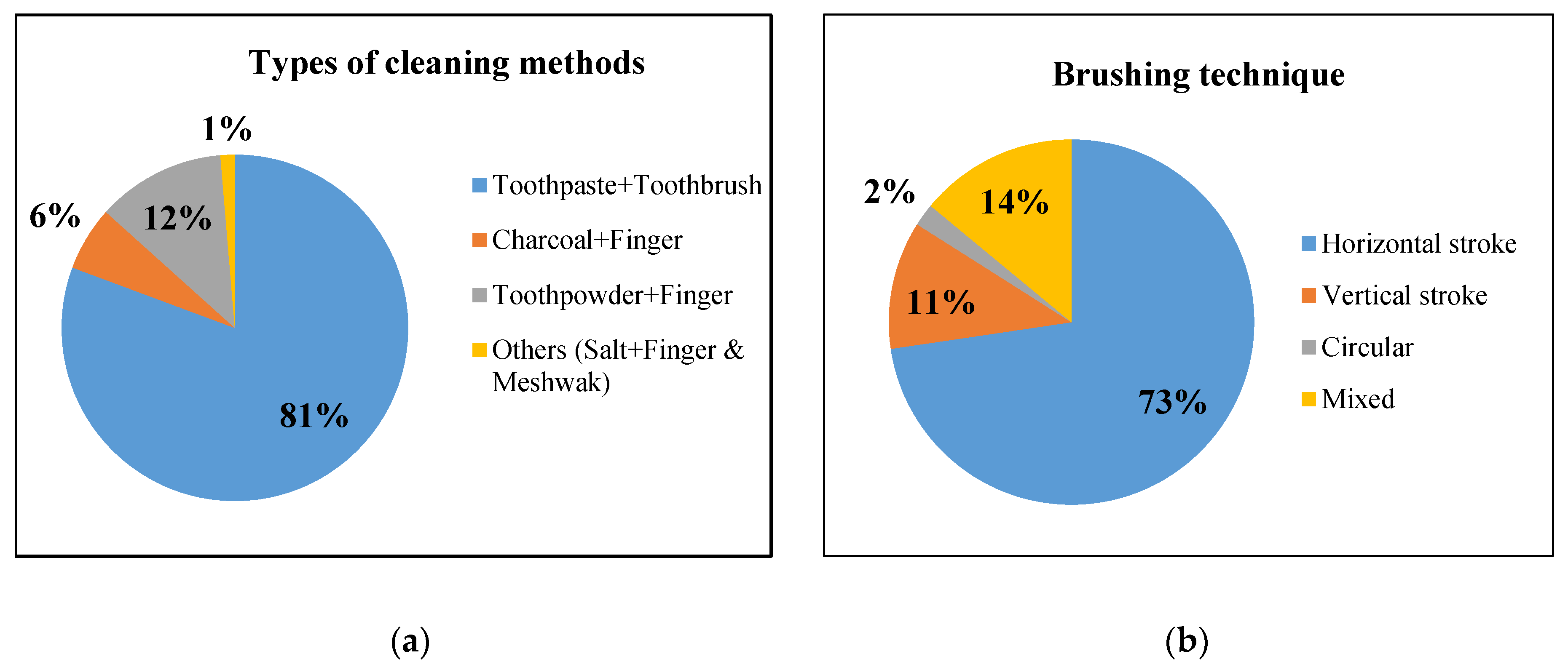
- Uing of toothbrush and toothpaste
- Toothpaste + Toothbrush
- Charcoal + Finger
- Toothpowder + Finger
- Others (Salt+Finger & Meshwak)
- Meshwak (Neem stick)
- Tpes of toothpaste/powder use?
- Branded Toothpaste
- Local toothpaste
- Tooth powder
- Coal
- Salt
- Meshwak (Neem stick)
- Brushing time
- Brushing in the morning before meal
- Brushing in the morning after meal
- Brushing at night after meal
- Brushing technique
- Horizontal stroke
- Vertical stroke
- Circular
- Mixed
- Mouth rinsing after meal
- Yes
- No
- Types of toothbrush
- Soft bristle brush
- Don’t know
- Finger
- Meshwak
- Medium or Hard
- Inter-dental cleaning
- Tooth pick/stick
- Don’t use
- Dental floss/dental thread
- Regular thread
- Others
- How often change the toothbrush?
- Monthly
- 3 monthly
- 6 monthly
- Change when broken
- Don’t know about changing
- Tongue cleaning/brushing
- Yes
- No
- Don’t know
- Brushes tongue by regular toothbrush
- Yes
- No
- Don’t know
- Do you visit dentist for dental checkup? (if Yes)
- Yes
- No
- Don’t know
- If yes, then how often?
- 6 monthly
- Yearly
- On pain/if any problem
- Never
- Occupation of the parents (Father)
- Agriculture
- Daily laborer
- Rickshaw/van puller
- CNG/bus/truck driver
- Business/shopkeepers
- Teacher
- Office worker
- Education of the household parents:
- No education
- Primary level
- Secondary level
- Higher secondary level and above
References
- Dixit, P.B.; Dixit, S.; Singh, R.; Khanal, P. Oral Hygiene awareness and practices among the Nepalese school children in Bhaktapur. J. Nepal Dent. Assoc. 2013, 13, 22–25. [Google Scholar]
- Choudhury, A.R.; Choudhury, K.N.; Islam, S.M.S. Relationship of dental diseases with coronary artery diseases and diabetes in Bangladesh. Cardiovasc. Diagn. Ther. 2016, 6, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Kolltceit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin. Microbiol. Rev. 2000, 13, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Alkarimi, H.A.; Watt, R.G.; Pikhart, H.; Sheiham, A.; Tsakos, G. Dental caries and growth in school-age children. Pediatrics 2014, 133, e616–e623. [Google Scholar] [CrossRef] [Green Version]
- Mishu, M.P.; Hobdell, M.; Khan, M.H.; Hubbard, R.M.; Sabbah, W. Relationship between untreated dental caries and weight and height of 6-to 12-year-old primary school children in Bangladesh. Int. J. Dent. 2013, 1–5. [Google Scholar] [CrossRef]
- Mishu, M.P.; Tsakos, G.; Heilmann, A.; Watt, R.G. Dental caries and anthropometric measures in a sample of 5-to 9-year-old children in Dhaka, Bangladesh. Community Dent. Oral Epidemiol. 2018, 46, 449–456. [Google Scholar] [CrossRef]
- Sheiham, A. Dental caries affects body weight, growth and quality of life in pre-school children. Br. Dent. J. 2006, 201, 625–626. [Google Scholar] [CrossRef] [Green Version]
- Jain, N.; Matra, D.; Ashok, K.P.; Soni, S.; Ahmed, S. Oral hygiene-awareness and practice among patients attending OPD at Vyas Dental College and Hospital, Jodhpur. J. Indian Soc. Periodontol. 2012, 16, 524. [Google Scholar] [CrossRef]
- Ullah, M.S.; Aleksejuniene, J.; Eriksen, H.M. Oral health of 12-year-old Bangladeshi children. Acta Odontol. Scand. 2002, 60, 117–122. [Google Scholar] [CrossRef]
- Jürgensen, N.; Petersen, P. Promoting oral health of children through schools-Results from a WHO global survey 2012. Community Dent Health 2013, 30, 204–218. [Google Scholar]
- Mehta, A.; Pradhan, S. The oral hygiene habits and general oral awareness in public schools in Mumbai. Int. J. Laser Dent. 2013, 3, 60. [Google Scholar]
- Zhu, L.; Petersen, P.E.; Wang, H.Y.; Bian, J.Y. Oral health knowledge, attitudes and behaviour of children and adolescents in China. Int. Dent. J. 2003, 53, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Grewal, N.; Kaur, M. Status of oral health awareness in Indian children as compared to Western children: A thought provoking situation (a pilot study). J. Indian Soc. Pedod. Prev. Dent. 2007, 25, 15. [Google Scholar] [PubMed]
- Doichinova, L.; Mitova, N. Assessment of oral hygiene habits in children 6 to 12 years. J. IMAB Ann. Proc. Sci. Pap. 2014, 20, 664–668. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, M.S.; Mamun, M.A.A.; Islam, M.S. Oral hygiene practice and oral health status of geriatric population in selected area of Rangpur, Bangladesh. KYAMC J. 2018, 9, 48–52. [Google Scholar] [CrossRef]
- Nayana, U.J. Knowledge of children regarding oral hygiene: A school based descriptive study. J. Sci. Innov. Res. 2014, 3, 134–138. [Google Scholar]
- Benner, P. Interpretive Phenomenology: Embodiment, Caring, and Ethics in Health and Illness; Sage Publications: California, CA, USA, 1994; pp. 1–374. [Google Scholar]
- Bureau, C.H.E. Report of Seminar on School Health Services; Central Health Education Bureau: New Delhi, India, 1965. [Google Scholar]
- Martignon, S.; Faculty, D. Schoolchildren’s tooth brushing characteristics and oral hygiene habits assessed with video-recorded sessions at school and a questionnaire. Acta Odontol. Latinoam. 2012, 25, 163–170. [Google Scholar]
- Barboza, E.P. Periodontite crônica: Uma discussão sobre o tratamento não cirúrgico. Rev. Flum. Odontol. 2017, 2, 1–11. [Google Scholar]
- Haque, S.E.; Rahman, M.; Itsuko, K.; Islam, M.J.; Kayako, S. Effect of a school-based oral health education in preventing untreated dental caries and increasing knowledge, attitude, and practices among adolescents in Bangladesh. BMC Oral Health 2016, 16, 44. [Google Scholar] [CrossRef] [Green Version]
- De Farias, I.A.; Araujo Souza, G.C.d.; Ferreira, M.Â.F. A health education program for Brazilian public schoolchildren: The effects on dental health practice and oral health awareness. J. Public Health Dent. 2009, 69, 225–230. [Google Scholar] [CrossRef]
- Al-Omiri, M.K.; Al-Wahadni, A.M.; Saeed, K.N. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J. Dent. Educ. 2006, 70, 179–187. [Google Scholar] [PubMed]
- Anaise, J. Plaque-removing effect of dental floss and toothpicks in children 12–13 years of age. Community Dent. Oral Epidemiol. 1976, 4, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Imoisili, M.A.; Bonwit, A.M.; Bulas, D.I. Toothpick puncture injuries of the foot in children. Pediatr. Infect. Dis. J. 2004, 23, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Budnick, L.D. Toothpick-related injuries in the United States, 1979 through 1982. JAMA 1984, 252, 796–797. [Google Scholar] [CrossRef] [PubMed]
- Yaegaki, K.; Coil, J.M.; Miyazaki, M. Tongue brushing and mouth rinsing as basic treatment measures for halitosis. Int. Dent. J. 2002, 52, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Bass, C.C. The optimum characteristics of toothbrushes for personal oral hygiene. Dent Items Int. 1948, 70, 697–718. [Google Scholar]
- Attin, T.; Hornecker, E. Tooth brushing and oral health: How frequently and when should tooth brushing be performed? Oral Health Prev. Dent. 2005, 3, 133–140. [Google Scholar]
- Addy, M.; Hunter, M. Can tooth brushing damage your health? Effects on oral and dental tissues. Int. Dent. J. 2003, 53, 177–186. [Google Scholar]
- Saied-Moallemi, Z.; Virtanen, J.I.; Murtomaa, H. Influence of mothers’ oral health knowledge and attitudes on their children’s dental health. Eur. Archiv. Paediatr. Dent. 2008, 9, 79–83. [Google Scholar] [CrossRef]
- Poutanen, R.; Lahti, S.; Hausen, H. Parental influence on children’s oral health-related behavior. Acta Odontol. Scand. 2006, 64, 286–292. [Google Scholar] [CrossRef]
- Garbin, C.A.S.; Lima, D.; Dos Santos, K. Oral health education in schools: Promoting health agents. Int. J. Dent. Hyg. 2009, 7, 212–216. [Google Scholar] [CrossRef]
- Petersen, P.E.; Tai, B.J.; Peng, B.; Fan, M.W. Effect of a school-based oral health education programme in Wuhan City, Peoples Republic of China. Int. Dent. J. 2004, 54, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.C.; Oliveira, M.J.; Pordeus, I.A. Comparison between observed children’s tooth brushing habits and those reported by mothers. BMC Oral Health 2011, 11, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turska-Szybka, A.; Gozdowski, D.; Olczak-Kowalczyk, D. Impact of individual health-oriented parent education on eating and hygienic habits, oral hygiene level, and dentition condition in children with high risk of caries. Dev. Period Med. 2014, 18, 233–240. [Google Scholar] [PubMed]

{kind=link}
| Characteristics | Total Number | % |
|---|---|---|
| Age group (in years) 5–7 7–9 9–12 | 48 59 43 | 32% 39% 29% |
| Gender Boys Girls | 68 82 | 45.3% 54.7% |
| Education * No education Primary Secondary Higher secondary and above | 14 60 49 27 | 9% 40% 33% 18% |
| Occupation * Agriculture Daily laborer Rickshaw/van puller CNG/bus/truck driver Business/shopkeepers Teacher Office worker | 70 40 9 3 11 2 15 | 47% 27% 6% 2% 7% 1% 10% |
| Variable | Frequency (n) | % |
|---|---|---|
| Brushing frequency | ||
| Once/daily | 121 | 80.7% |
| Twice/daily | 29 | 19.3% |
| Brushing time | ||
| Brushing in the morning before meal | 133 | 88.7% |
| Brushing in the morning after meal | 6 | 4% |
| Brushing at night after meal | 11 | 7.3% |
| Mouth rinsing after meal | ||
| Yes | 37 | 24.7% |
| No | 113 | 75.3% |
| Types of toothbrush | ||
| Don’t know | 92 | 61.3% |
| Soft bristle brush | 5 | 3.3% |
| Medium/Hard | 8 | 5.3% |
| Finger | 29 | 19.3% |
| Meshwak | 16 | 10.7% |
| Inter-dental cleaning | ||
| Toothpick/stick | 93 | 62% |
| Don’t use | 48 | 32% |
| Dental floss/dental thread | - | - |
| Regular thread | 9 | 6% |
| How often change the toothbrush | ||
| Monthly | - | - |
| 3 months | 2 | 1.3% |
| 6 months | 13 | 8.7% |
| Change when broken | 53 | 35.3% |
| Don’t know about changing | 82 | 54.7% |
| Tongue cleaning/brushing | ||
| Yes | 11 | 7% |
| No | 16 | 10.7% |
| Don’t know | 123 | 82% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhuiyan, M.A.-A.; Anwar, H.B.; Anwar, R.B.; Ali, M.N.; Agrawal, P. Oral Hygiene Awareness and Practices among a Sample of Primary School Children in Rural Bangladesh. Dent. J. 2020, 8, 36. https://doi.org/10.3390/dj8020036
Bhuiyan MA-A, Anwar HB, Anwar RB, Ali MN, Agrawal P. Oral Hygiene Awareness and Practices among a Sample of Primary School Children in Rural Bangladesh. Dentistry Journal. 2020; 8(2):36. https://doi.org/10.3390/dj8020036
Chicago/Turabian StyleBhuiyan, Md. Al-Amin, Humayra Binte Anwar, Rezwana Binte Anwar, Mir Nowazesh Ali, and Priyanka Agrawal. 2020. "Oral Hygiene Awareness and Practices among a Sample of Primary School Children in Rural Bangladesh" Dentistry Journal 8, no. 2: 36. https://doi.org/10.3390/dj8020036
APA StyleBhuiyan, M. A.-A., Anwar, H. B., Anwar, R. B., Ali, M. N., & Agrawal, P. (2020). Oral Hygiene Awareness and Practices among a Sample of Primary School Children in Rural Bangladesh. Dentistry Journal, 8(2), 36. https://doi.org/10.3390/dj8020036