Biofilm Formation on Dental Implant Surface Treated by Implantoplasty: An In Situ Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimens Preparation
2.2. Volunteer Selection and Tray Preparation
2.3. In Situ Procedures
2.4. Macroscopic Evaluation
2.5. Microscopic Evaluation
3. Results
3.1. Macroscopic Evaluation
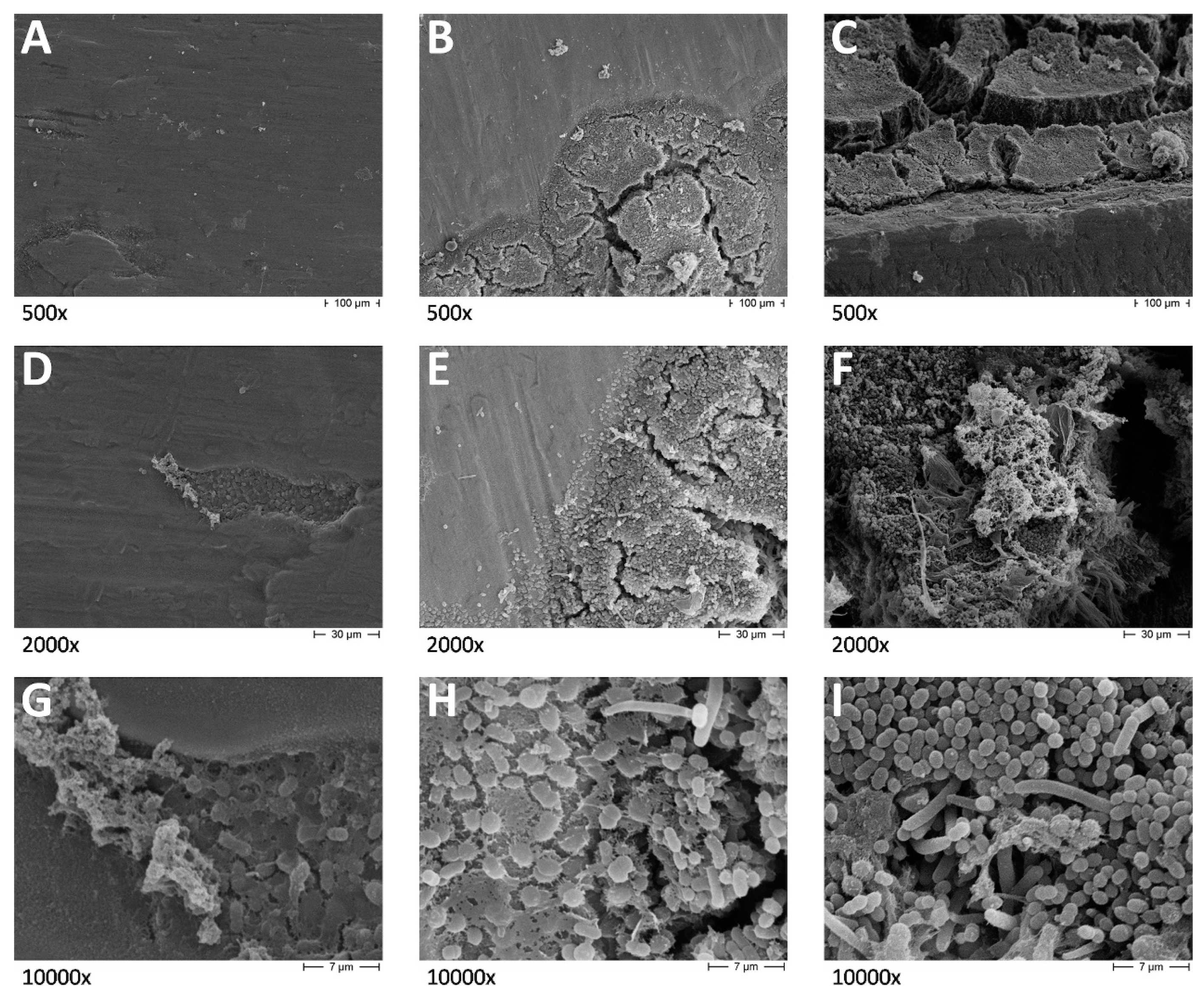
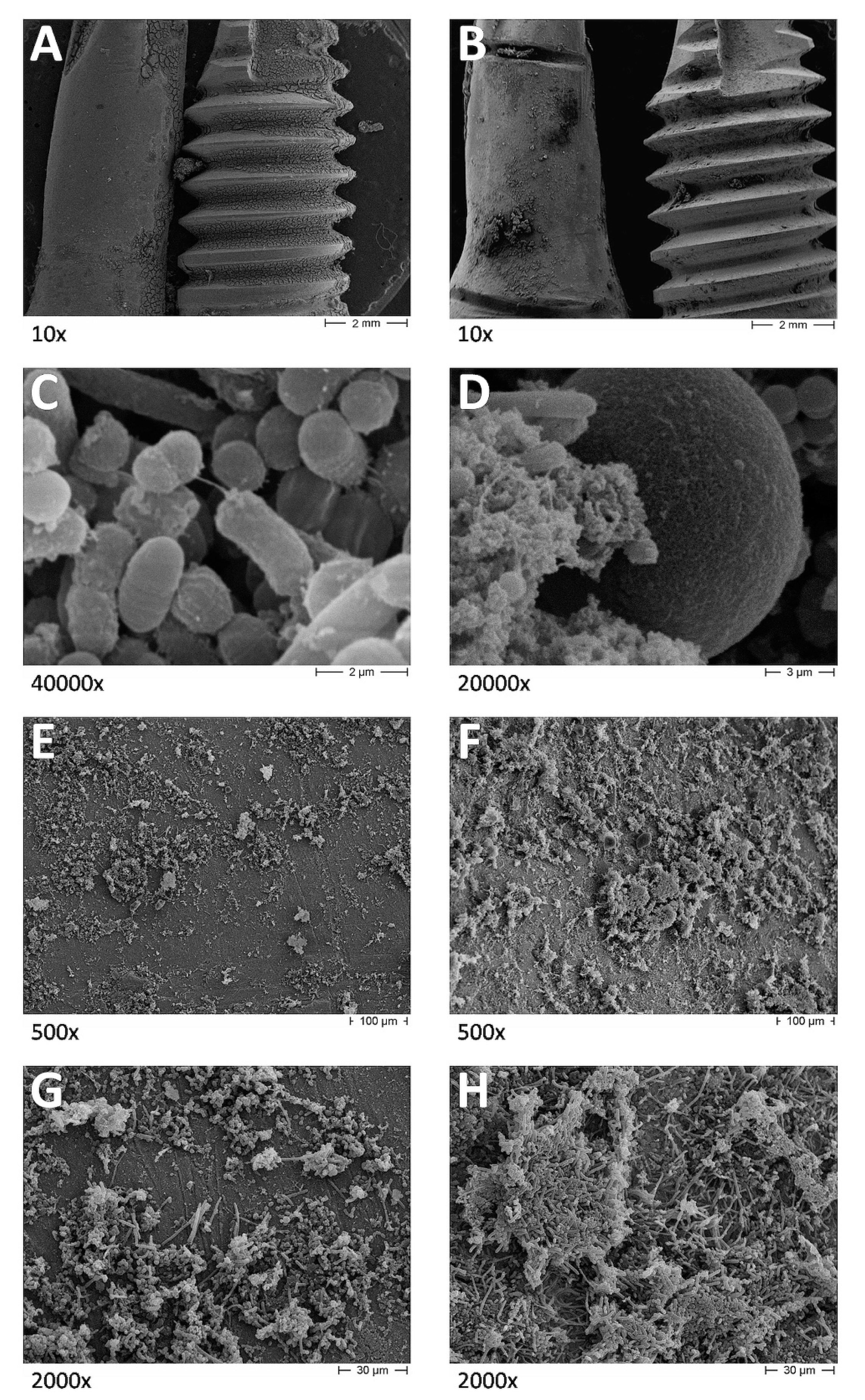
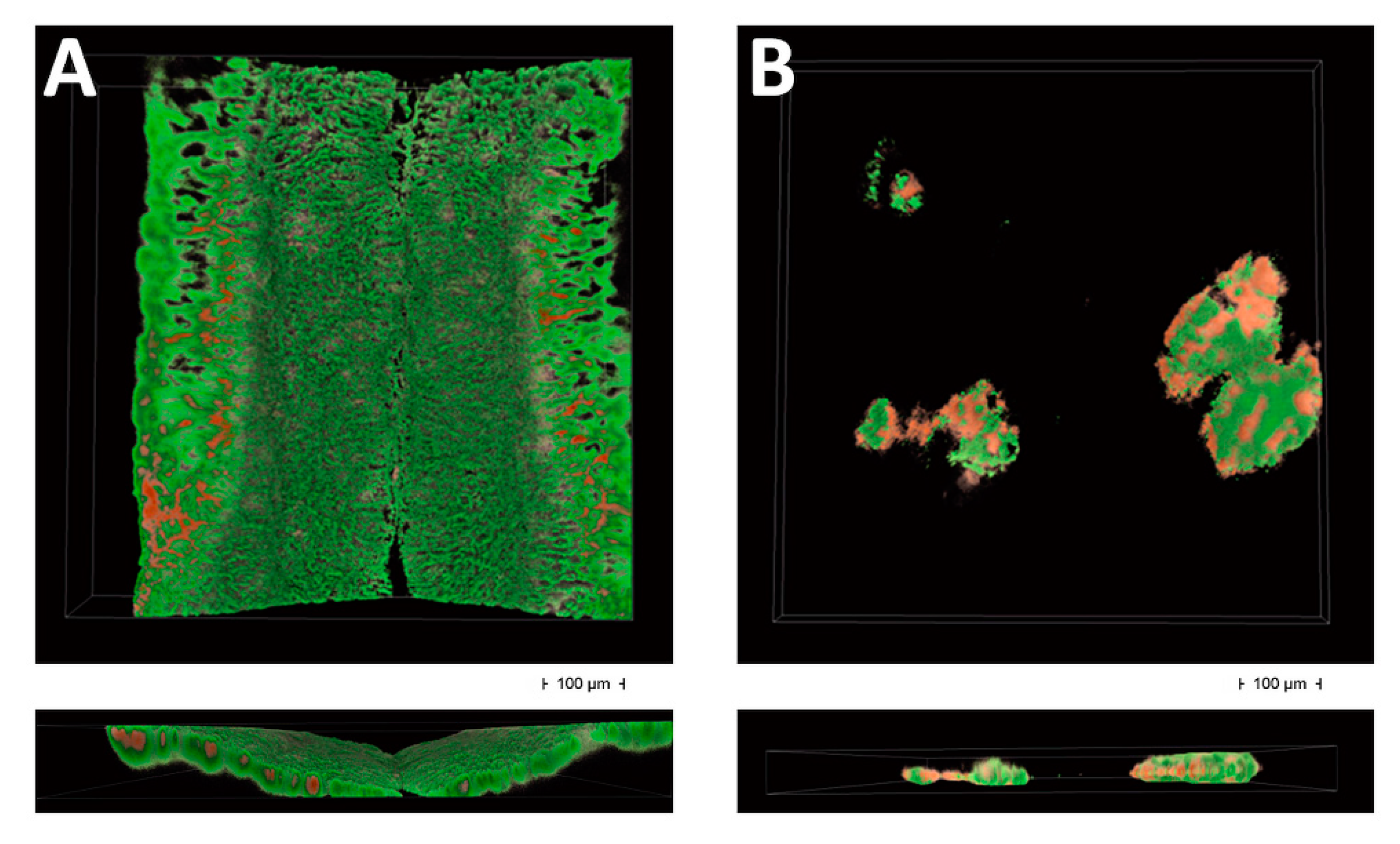
3.2. Microscopic Evaluation
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Levignac, J. Periimplantation osteolysis- periimplantosis—periimplantitis. Rev. Fr. Odontostomatol. 1965, 12, 1251–1260. [Google Scholar] [PubMed]
- Mombelli, A.; van Oosten, M.A.; Schurch, E., Jr.; Land, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Karring, T. Proceedings of the 1st European Workshop On Periodontology: Charter House at Ittingen, Thurgau, Switzerland, 1–4 February 1993; Quintessence Pub. Co.: London, UK, 1994. [Google Scholar]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant dieases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Pontoriero, R.; Tonelli, M.P.; Carnevale, G.; Mombelli, A.; Nyman, S.R.; Lang, N.P. Experimentally induced peri-implant mucositis. A clinical study in humans. Clin. Oral Implant. Res. 1994, 5, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Vogels, R.; Peeters, W.; van Steenberghe, D.; Naert, I.; Haffajee, A. Dynamics of initial subgingival colonization of ‘pristine’ peri-implant pockets. Clin. Oral Implant. Res. 2006, 17, 25–37. [Google Scholar] [CrossRef]
- Renvert, S.; Roos-Jansaker, A.M.; Lindahl, C.; Renvert, H.; Rutger Persson, G. Infection at titanium implants with or without a clinical diagnosis of inflammation. Clin. Oral Implant. Res. 2007, 18, 509–516. [Google Scholar] [CrossRef]
- Shibli, J.A.; Melo, L.; Ferrari, D.S.; Figueiredo, L.C.; Faveri, M.; Feres, M. Composition of supra- and subgingival biofilm of subjects with healthy and diseased implants. Clin. Oral Implant. Res. 2008, 19, 975–982. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Mombelli, A. The therapy of peri-implantitis: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 325–345. [Google Scholar] [CrossRef] [Green Version]
- Renvert, S.; Polyzois, I.; Claffey, N. Surgical therapy for the control of peri-implantitis. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 84–94. [Google Scholar] [CrossRef]
- Romeo, E.; Ghisolfi, M.; Murgolo, N.; Chiapasco, M.; Lops, D.; Vogel, G. Therapy of peri-implantitis with resective surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part I: Clinical outcome. Clin. Oral Implant. Res. 2005, 16, 9–18. [Google Scholar] [CrossRef]
- Romeo, E.; Lops, D.; Chiapasco, M.; Ghisolfi, M.; Vogel, G. Therapy of peri-implantitis with resective surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part II: Radiographic outcome. Clin. Oral Implant. Res. 2007, 18, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Matarasso, S.; Iorio Siciliano, V.; Aglietta, M.; Andreuccetti, G.; Salvi, G.E. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: A prospective case series. Clin. Oral Implant. Res. 2014, 25, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sahm, N.; Becker, J. Combined surgical therapy of advanced peri-implantitis lesions with concomitant soft tissue volume augmentation. A case series. Clin. Oral Implant. Res. 2014, 25, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sahm, N.; Mihatovic, I.; Golubovic, V.; Becker, J. Surgical therapy of advanced ligature-induced peri-implantitis defects: Cone-beam computed tomographic and histological analysis. J. Clin. Periodontol. 2011, 38, 939–949. [Google Scholar] [CrossRef]
- Suh, J.J.; Simon, Z.; Jeon, Y.S.; Choi, B.G.; Kim, C.K. The use of implantoplasty and guided bone regeneration in the treatment of peri-implantitis: Two case reports. Implant. Dent. 2003, 12, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Ramel, C.F.; Lussi, A.; Ozcan, M.; Jung, R.E.; Hammerle, C.H.; Thoma, D.S. Surface roughness of dental implants and treatment time using six different implantoplasty procedures. Clin. Oral Implant. Res. 2016, 27, 776–781. [Google Scholar] [CrossRef]
- De Winter, J.C.F. Using the Student’s t-test with extremely small sample sizes. Pract. Assess. Res. Eval. 2013, 18, 1–12. [Google Scholar]
- Mierau, H.D. Relations between plaque formation, tooth surface roughness and self-cleaning. Beziehungen zwischen Plaquebildung. Rauhigkeit der Zahnoberfläche und Selbstreinigung. Dtsch. Zahnarztl. Z. 1984, 39, 691–698. [Google Scholar]
- Quirynen, M.; Marechal, M.; Busscher, H.J.; Weerkamp, A.H.; Darius, P.L.; van Steenberghe, D. The influence of surface free energy and surface roughness on early plaque formation: An in vivo study in man. J. Clin. Periodontol. 1990, 17, 138–144. [Google Scholar] [CrossRef]
- Quirynen, M.; Van Der Mei, H.C.; Bollen, C.; Schotte, A.; Marechal, M.; Doornbusch, G.; Naert, I.; Busscher, H.; Van Steenberghe, D. An in vivo study of the influence of the surface roughness of implants on the microbiology of supra- and subgingival plaque. J. Dent. Res. 1993, 72, 1304–1309. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Abrahamsson, I.; Berglundh, T.; Lindhe, J. Soft tissue reactions to plaque formation at implant abutments with different surface topography. An experimental study in dogs. J. Clin. Periodontol. 2002, 29, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Mihatovic, I.; Golubovic, V.; Eick, S.; Iglhaut, T.; Becker, J. Experimental peri-implant mucositis at different implant surfaces. J. Clin. Periodontol. 2014, 41, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Polyzois, I.; Claffey, N. How do implant surface characteristics influence peri-implant disease? J. Clin. Periodontol. 2011, 38 (Suppl. 11), 214–222. [Google Scholar] [CrossRef] [PubMed]
- Albouy, J.P.; Abrahamsson, I.; Berglundh, T. Spontaneous progression of experimental peri-implantitis at implants with different surface characteristics: An experimental study in dogs. J. Clin. Periodontol. 2012, 39, 182–187. [Google Scholar] [CrossRef] [PubMed]
- John, G.; Becker, J.; Schwarz, F. Rotating titanium brush for plaque removal from rough titanium surfaces—An in vitro study. Clin. Oral Implant. Res. 2014, 25, 838–842. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Right | Control Left | Test Right | Test Left | Control | Test | |
|---|---|---|---|---|---|---|
| Plaque Presence/150 Squares, (%) | Mean % (±SD) | |||||
| Day 1 | 6 (4.00%) | 4 (2.67%) | 5 (3.33%) | 0 (0.00%) | 3.35 (0.92) | 1.65 (2.33) |
| Day 2 | 37 (24.67%) | 47 (31.33%) | 9 (6.00%) | 12 (8.00%) | 27.95 (4.74) | 7.00 (1.41) |
| Day 3 | 50 (33.33%) | 50 (33.33%) | 15 (10.00%) | 15 (10.00%) | 33.30 (0.00) | 10.00 (0.00) |
| Day 4 | 93 (62.00%) | 56 (37.33%) | 18 (12.00%) | 18 (12.00%) | 49.65 (17.47) | 12.00 (0.00) |
| Day 5 | 105(70.00%) | 90 (60.00%) | 24 (16.00%) | 24 (16.00%) | 65.00 (7.07) | 16.00 (0.00) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azzola, F.; Ionescu, A.C.; Ottobelli, M.; Cavalli, N.; Brambilla, E.; Corbella, S.; Francetti, L. Biofilm Formation on Dental Implant Surface Treated by Implantoplasty: An In Situ Study. Dent. J. 2020, 8, 40. https://doi.org/10.3390/dj8020040
Azzola F, Ionescu AC, Ottobelli M, Cavalli N, Brambilla E, Corbella S, Francetti L. Biofilm Formation on Dental Implant Surface Treated by Implantoplasty: An In Situ Study. Dentistry Journal. 2020; 8(2):40. https://doi.org/10.3390/dj8020040
Chicago/Turabian StyleAzzola, Francesco, Andrei Cristian Ionescu, Marco Ottobelli, Nicolò Cavalli, Eugenio Brambilla, Stefano Corbella, and Luca Francetti. 2020. "Biofilm Formation on Dental Implant Surface Treated by Implantoplasty: An In Situ Study" Dentistry Journal 8, no. 2: 40. https://doi.org/10.3390/dj8020040