Systematic Review on the Role of Lasers in Endodontic Therapy: Valuable Adjunct Treatment?

 , , ,
, , , 

Abstract
:1. Introduction
1.1. Pulpitis—Apical Periodontitis
1.2. Endodontic Therapy
1.3. Lasers in Endodontic Therapy
1.4. Post-operative-endodontic Pain
1.5. Photobiomodulation (PBM)
1.6. Aims of the Study
- Conventional laser use inside the root canal as an additional disinfection method;
- Lasers combined with a photosensitizer inside the root canal in antimicrobial photodynamic therapy (aPDT);
- Lasers in post-operative-endodontic pain management, coupled with photobiomodulation therapy (PBMT).
2. Materials and Methods
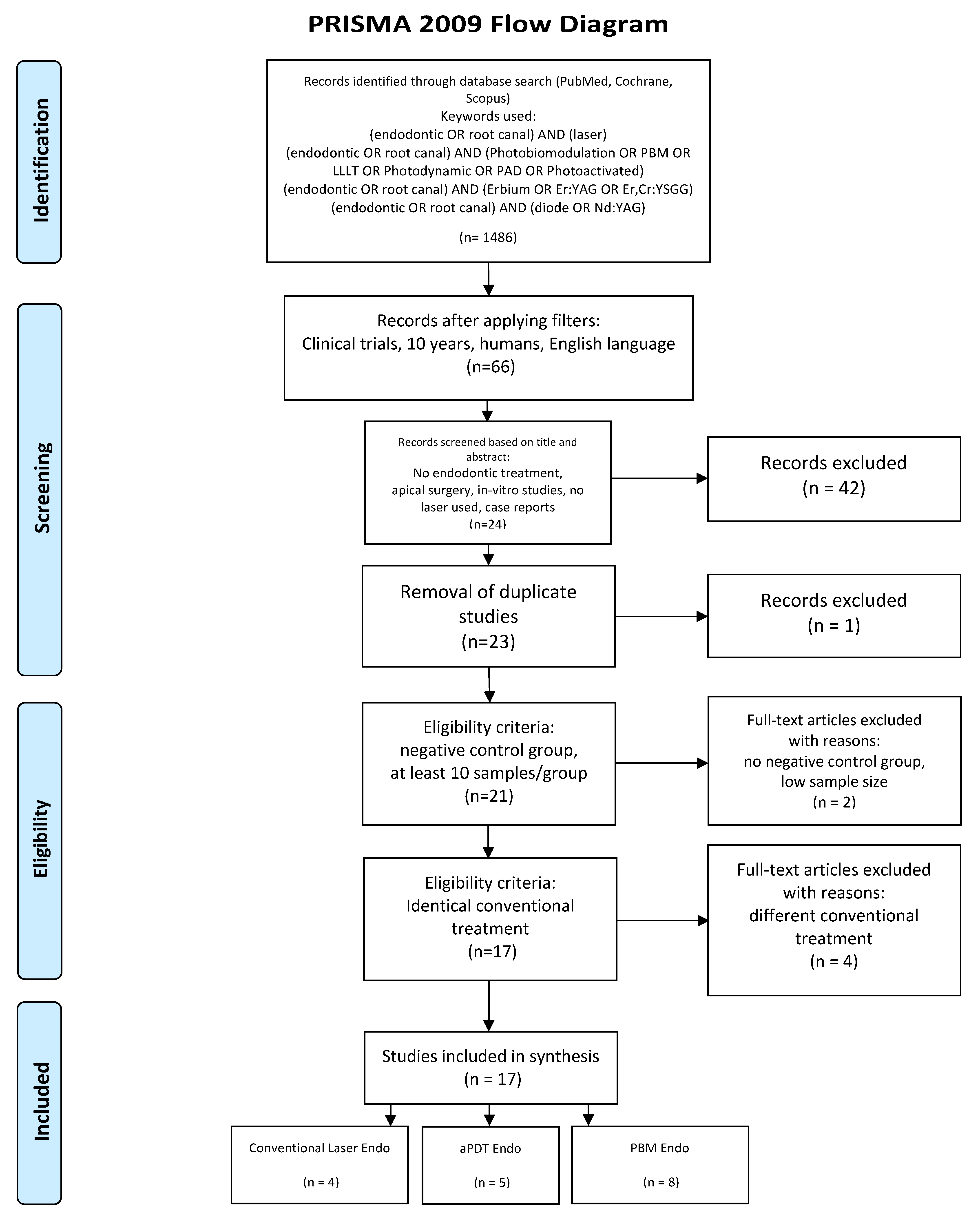
2.1. Search Strategy
- (Endodontic OR root canal) AND (laser);
- (Endodontic OR root canal) AND (photobiomodualtion OR PBM OR LLLT OR photodynamic OR PAD OR photoactivated);
- (Endodontic OR root canal) AND (diode OR Nd:YAG OR erbium OR Er:YAG OR Er, Cr:YSGG)
- Only randomized controlled clinical trials;
- Laser employed as an adjunctive therapy;
- Identical conventional endodontic treatment performed to all groups;
- Negative control group;
- At least 10 participants per group;
- In case of aPDT applied, correct combination of photosensitizer (PS) and laser used.
- No endodontic treatment applied;
- Apical surgery;
- Duplicates or studies with the same ethical approval number;
- No negative control group;
- Different conventional endodontic treatment applied to the test group;
- Low sample size (less than 10 per group);
- No randomized controlled clinical trials, case series or pilot studies;
- In vitro studies;
- LED used as light source.
- Conventional laser-assisted endodontic treatment (4 articles);
- aPDT in endodontics (5 articles);
- PBM in endodontics (8 articles)
2.2. Data Extraction
- Citation (first author and publication year);
- Type of study/number of sampling participants;
- Test/control group;
- Aim/approach;
- Laser/protocol;
- Follow-up;
- Outcome.
2.3. Quality Assessment
- Randomization?
- Sample size calculation and required sample number included?
- Allocation ratio of 1:1?
- Baseline situation similar?
- Blinding?
- Parameters of laser use described appropriately, and calculations correct?
- Power meter used?
- Numerical results available (statistics)?
- Outcome data complete?
- Correct interpretation of data?
- High risk: 0–4
- Moderate risk: 5–7
- Low risk: 8–10.
3. Results
3.1. Primary Outcome
3.2. Data Presentation
3.3. Quality Assessment Presentation
3.4. Analysis of Data
- Radiographic healing: [33].
- Power: 1/5;
- Tip or spot size: 2/5;
- Fluence incorrectly calculated (consequently, either tip or energy was incorrect): 3/5;
- Pulse duration: 4/5;
- Energy per pulse: 1/5;
- Frequency: 1/5;
- Wet or dry canal: 1/5.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ogle, O.E. Odontogenic Infections. Dent. Clin. N. Am. 2017, 61, 235–252. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, P.; Romero, M.; Vera, J.; Daood, U.; Khan, A.U.; Yan, A.; Cheung, G.S.P. Biofilms in Endodontics-Current Status and Future Directions. Int. J. Mol. Sci. 2017, 18, 1748. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.; Wesselink, P.; Buijs, J.; VanWinkelhoff, A. Viable Bacteria in Root Dentinal Tubules of Teeth with Apical Periodontitis. J. Endod. 2001, 27, 76–81. [Google Scholar] [CrossRef]
- De Meyer, S.; Meire, M.A.; Coenye, T.; De Moor, R.J.G. Effect of laser-activated irrigation on biofilms in artificial root canals. Int. Endod. J. 2017, 50, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Berutti, E.; Marini, R.; Angeretti, A. Penetration ability of different irrigants into dentinal tubules. J. Endod. 1997, 23, 725–727. [Google Scholar] [CrossRef]
- Haapasalo, M.; Udnaes, T.; Endal, U. Persistent, recurrent, and acquired infection of the root canal system post-treatment. Endod. Top. 2003, 6, 29–56. [Google Scholar] [CrossRef]
- Moreira, M.S.; Anuar, A.S.N.S.; Tedesco, T.K.; dos Santos, M.; Morimoto, S. Endodontic Treatment in Single and Multiple Visits: An Overview of Systematic Reviews. J. Endod. 2017, 43, 864–870. [Google Scholar] [CrossRef]
- Riis, A.; Taschieri, S.; Del Fabbro, M.; Kvist, T. Tooth Survival after Surgical or Nonsurgical Endodontic Retreatment: Long-term Follow-up of a Randomized Clinical Trial. J. Endod. 2018, 44, 1480–1486. [Google Scholar] [CrossRef]
- Teo, C.Y.J.; George, R.; Walsh, L.J. Dispersion of near-infrared laser energy through radicular dentine when using plain or conical tips. Lasers Med. Sci. 2018, 33, 251–255. [Google Scholar] [CrossRef]
- Kasić, S.; Knezović, M.; Beader, N.; Gabrić, D.; Malčić, A.I.; Baraba, A. Efficacy of Three Different Lasers on Eradication of Enterococcus faecalis and Candida albicans Biofilms in Root Canal System. Photomed. Laser Surg. 2017, 35, 372–377. [Google Scholar] [CrossRef]
- Granevik Lindström, M.; Wolf, E.; Fransson, H. The Antibacterial Effect of Nd:YAG Laser Treatment of Teeth with Apical Periodontitis: A Randomized Controlled Trial. J. Endod. 2017, 43, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Chiniforush, N.; Pourhajibagher, M.; Shahabi, S.; Kosarieh, E.; Bahador, A. Can antimicrobial photodynamic therapy (aPDT) enhance the endodontic treatment? J. Lasers Med. Sci. 2016, 7, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Macedo, R.G.; Wesselink, P.R.; Zaccheo, F.; Fanali, D.; Van Der Sluis, L.W.M. Reaction rate of NaOCl in contact with bovine dentine: Effect of activation, exposure time, concentration and pH. Int. Endod. J. 2010, 43, 1108–1115. [Google Scholar] [CrossRef]
- Garcia-Diaz, M.; Huang, Y.Y.; Hamblin, M.R. Use of fluorescent probes for ROS to tease apart Type I and Type II photochemical pathways in photodynamic therapy. Methods 2016, 109, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diogo, P.; Faustino, M.F.A.; Neves, G.M.P.M.S.; Palma, P.J.; Baptista, I.P.; Gonçalves, T.; Santos, J.M. An insight into advanced approaches for photosensitizer optimization in endodontics—A critical review. J. Funct. Biomater. 2019, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Nagendrababu, V.; Pulikkotil, S.J.; Jinatongthai, P.; Veettil, S.K.; Teerawattanapong, N.; Gutmann, J.L. Efficacy and Safety of Oral Premedication on Pain after Nonsurgical Root Canal Treatment: A Systematic Review and Network Meta-analysis of Randomized Controlled Trials. J. Endod. 2019, 45, 364–371. [Google Scholar] [CrossRef]
- Comparin, D.; Moreira, E.; Souza, E.; De-Deus, G.; Arias, A.; Silva, E. Postoperative Pain after Endodontic Retreatment Using Rotary or Reciprocating Instruments: A Randomized Clinical Trial. J. Endod. 2017, 43, 1084–1088. [Google Scholar] [CrossRef]
- Shamszadeh, S.; Shirvani, A.; Eghbal, M.J.; Asgary, S. Efficacy of Corticosteroids on Postoperative Endodontic Pain: A Systematic Review and Meta-analysis. J. Endod. 2018, 44, 1057–1065. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, X.L.; Zou, X.L.; Chen, S.Z.; Zou, J.; Wang, Y. Efficacy of low-level laser therapy in pain management after root canal treatment or retreatment: A systematic review. Lasers Med. Sci. 2019, 34, 1305–1316. [Google Scholar] [CrossRef]
- Alí, A.; Olivieri, J.G.; Duran-Sindreu, F.; Abella, F.; Roig, M.; García-Font, M. Influence of preoperative pain intensity on postoperative pain after root canal treatment: A prospective clinical study. J. Dent. 2016, 45, 39–42. [Google Scholar] [CrossRef]
- Chow, R.T.; Armati, P.J.; Laakso, E.L.; Bjordal, J.M.; Baxter, G.D. Inhibitory effects of laser irradiation on peripheral mammalian nerves and relevance to analgesic effects: A systematic review. Photomed. Laser Surg. 2011, 29, 365–381. [Google Scholar] [CrossRef] [PubMed]
- Vahdatinia, F.; Gholami, L.; Karkehabadi, H.; Fekrazad, R. Photobiomodulation in Endodontic, Restorative, and Prosthetic Dentistry: A Review of the Literature. Photobiomodulation, Photomed. Laser Surg. 2019, 37, 869–886. [Google Scholar] [CrossRef] [PubMed]
- Chow, R.T.; Armati, P.J. Photobiomodulation: Implications for anesthesia and pain relief. Photomed. Laser Surg. 2016, 34, 599–609. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22. [Google Scholar] [CrossRef] [Green Version]
- Parker, S. Laser-tissue interaction and photobiomodulation Chapter 3.14. In Lasers in Dentistry-Current Concepts, 1st ed.; Coluzzi, D., Parker, S., Eds.; Springer: Cham, Switzerland, 2017; p. 51. ISBN 978-3-319-51944-9. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement (Reprinted from Annals of Internal Medicine). PLOS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Savović, J.; Page, M.; Elbers, R.; Sterne, J. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; John Wiley & Sons: Chichester, UK, 2019; pp. 205–228. [Google Scholar] [CrossRef]
- Genc Sen, O.; Kaya, M. Effect of root canal disinfection with a diode laser on postoperative pain after endodontic retreatment. Photobiomodulation Photomed. Laser Surg. 2019, 37, 85–90. [Google Scholar] [CrossRef]
- Dagher, J.; El Feghali, R.; Parker, S.; Benedicenti, S.; Zogheib, C. Postoperative Quality of Life Following Conventional Endodontic Intracanal Irrigation Compared with Laser-Activated Irrigation: A Randomized Clinical Study. Photobiomodulation Photomed. Laser Surg. 2019, 37, 248–253. [Google Scholar] [CrossRef]
- Morsy, D.A.; Negm, M.; Diab, A.; Ahmed, G. Postoperative pain and antibacterial effect of 980 nm diode laser versus conventional endodontic treatment in necrotic teeth with chronic periapical lesions: A randomized control trial. F1000 Res. 2018, 7. [Google Scholar] [CrossRef]
- Yoo, Y.J.; Shon, W.J.; Baek, S.H.; Kang, M.K.; Kim, H.C.; Lee, W. Effect of 1440-nanometer neodymium:Yttrium-aluminum-garnet laser irradiation on pain and neuropeptide reduction: A randomized prospective clinical trial. J. Endod. 2014, 40, 28–32. [Google Scholar] [CrossRef]
- Coelho, M.S.; Vilas-Boas, L.; Tawil, P.Z. The effects of photodynamic therapy on postoperative pain in teeth with necrotic pulps. Photodiagnosis Photodyn. Ther. 2019, 27, 396–401. [Google Scholar] [CrossRef]
- de Miranda, R.G.; Colombo, A.P.V. Clinical and microbiological effectiveness of photodynamic therapy on primary endodontic infections: A 6-month randomized clinical trial. Clin. Oral Investig. 2018, 22, 1751–1761. [Google Scholar] [CrossRef] [PubMed]
- Pourhajibagher, M.; Ghorbanzadeh, R.; Parker, S.; Chiniforush, N.; Bahador, A. The evaluation of cultivable microbiota profile in patients with secondary endodontic infection before and after photo-activated disinfection. Photodiagnosis Photodyn. Ther. 2017, 18, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Jurič, I.B.; Plečko, V.; Pandurić, D.G.; Anić, I. The antimicrobial effectiveness of photodynamic therapy used as an addition to the conventional endodontic re-treatment: A clinical study. Photodiagnosis Photodyn. Ther. 2014, 11, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Garcez, A.S.; Nuñez, S.C.; Hamblin, M.R.; Suzuki, H.; Ribeiro, M.S. Photodynamic therapy associated with conventional endodontic treatment in patients with antibiotic-resistant microflora: A preliminary report. J. Endod. 2010, 36, 1463–1466. [Google Scholar] [CrossRef] [PubMed]
- Nunes, E.C.; Herkrath, F.J.; Suzuki, E.H.; Gualberto Júnior, E.C.; Marques, A.A.F.; Sponchiado Júnior, E.C. Comparison of the effect of photobiomodulation therapy and Ibuprofen on postoperative pain after endodontic treatment: Randomized, controlled, clinical study. Lasers Med. Sci. 2019, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Lopes Barros, L.; Herkrath, F.J. Effect of photobiomodulation therapy on postoperative pain after endodontic treatment: A randomized, controlled, clinical study. Clin. Oral Investig. 2019, 23, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Doğanay Yildiz, E.; Arslan, H.; Köseoğlu, S.; Arabaci, T.; Yildiz, D.A.; Savran, L. The effect of photobiomodulation on total amount of substance P in gingival crevicular fluid: Placebo-controlled randomized clinical trial. Lasers Med. Sci. 2019, 34, 517–523. [Google Scholar] [CrossRef]
- Arslan, H.; Köseoğlu, S.; Doğanay Yildiz, E.; Arabaci, T.; Savran, L.; Yildiz, D.A.; Veyisoğlu, G. Effect of intracanal diode laser application and low-level laser therapy on CGRP change. Braz. Oral Res. 2018, 32, e125. [Google Scholar] [CrossRef] [Green Version]
- Nabi, S.; Amin, K.; Masoodi, A.; Farooq, R.; Purra, A.R.; Ahangar, F.A. Effect of preoperative ibuprofen in controlling post endodontic pain with and without low-level laser therapy in single visit endodontics: A randomized clinical study. Indian J. Dent. Res. 2018, 29, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Doğanay Yildiz, E.; Arslan, H. Effect of Low-level Laser Therapy on Postoperative Pain in Molars with Symptomatic Apical Periodontitis: A Randomized Placebo-controlled Clinical Trial. J. Endod. 2018, 44, 1610–1615. [Google Scholar] [CrossRef] [PubMed]
- Arslan, H.; Doğanay, E.; Karataş, E.; Ünlü, M.A.; Ahmed, H.M.A. Effect of Low-level Laser Therapy on Postoperative Pain after Root Canal Retreatment: A Preliminary Placebo-controlled, Triple-blind, Randomized Clinical Trial. J. Endod. 2017, 43, 1765–1769. [Google Scholar] [CrossRef] [PubMed]
- Asnaashari, M.; Ashraf, H.; Daghayeghi, A.H.; Mojahedi, S.M.; Azari-Marhabi, S. Management of post endodontic retreatment pain with low level laser therapy. J. Lasers Med. Sci. 2017, 8, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Kreisler, M.; Kohnen, W.; Beck, M.; Al Haj, H.; Christoffers, A.; Götz, H.; Duschner, H.; Jansen, B. Efficacy of NaOCl/H2O2 Irrigation and GaAlAs Laser in Decontamination of Root Canals In Vitro. Lasers Surg. Med. 2003, 32, 189–196. [Google Scholar] [CrossRef]
- Sarda, R.A.; Shetty, R.M.; Tamrakar, A.; Shetty, S.Y. Antimicrobial efficacy of photodynamic therapy, diode laser, and sodium hypochlorite and their combinations on endodontic pathogens. Photodiagnosis Photodyn. Ther. 2019, 28, 265–272. [Google Scholar] [CrossRef]
- Sohrabi, K.; Sooratgar, A.; Zolfagharnasab, K.; Kharazifard, M.J.; Afkhami, F. Antibacterial activity of diode laser and sodium hypochlorite in enterococcus faecalis-contaminated root canals. Iran. Endod. J. 2016, 11, 8–12. [Google Scholar] [CrossRef]
- Rechenberg, D.K.; Galicia, J.C.; Peters, O.A. Biological markers for pulpal inflammation: A systematic review. PLoS ONE 2016, 11, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Cronshaw, M.; Parker, S.; Arany, P. Feeling the Heat: Evolutionary and Microbial Basis for the Analgesic Mechanisms of Photobiomodulation Therapy. Photobiomodulation Photomed. Laser Surg. 2019, 37, 517–526. [Google Scholar] [CrossRef]
- Wainwright, M.; Maisch, T.; Nonell, S.; Plaetzer, K.; Almeida, A.; Tegos, G.P.; Hamblin, M.R. Photoantimicrobials-are we afraid of the light? Lancet Infect. Dis. 2017, 17, e49–e55. [Google Scholar] [CrossRef]


{kind=link}
| Citation | Type of Study/Number of Samples | Test/Control Groups | Aim/ Approach | Laser/ Protocol | Follow-up | Outcome |
|---|---|---|---|---|---|---|
| Genc Sen et al. (2019) [28] | Parallel-group RCT/73 patients/single-rooted teeth retreatment | Laser + Conventional tx (37 patients)/ Conventional tx with placebo laser device (36 patients) 17% EDTA, and 2% NaOCl was used for the final irrigation in both groups. | Post-OP pain evaluation NRS 0–10 Percussion 0–2 | 940 nm 1 W 200 μm Tip starting from working length Speed of movement 2 mm/sec irradiation in circular motion 4 times each canal with 20 s intervals Canal DRY/ 1 session: day 0 | 3 days | Laser + RC tx group showed significant difference in VAS score (lower) after 24 h p = 0.036 and 72 h p = 0.016 Number of analgesic pills over 3 days significantly lower in laser group p = 0.008 Laser group Percussion on 4th day p = 0.008 |
| Dagher et al (2019) [29] | Parallel-group RCT/56 patients/premolars and molars | PIPS Protocol + Conventional tx (25 patients)/ Conventional tx (31 patients) Both groups immediate obturation | Post-OP pain evaluation VAS daily Percussion day 7 | 2940 nm 20 mJ 50 μsec 15 Hz 0.3 W 600 μm radial stripped tip EDTA/ distilled water/NaOCl/distilled water 30 sec stationary irradiation in pulp chamber 30 s resting 4 cycles for NaOCl/ 1 session: day 0 | Daily for 7 days | VAS: No difference between groups at any time Percussion: No difference between groups Pain in mastication: No difference between groups |
| Morsy et al. (2018) [30] | Parallel-group RCT/56 patients/maxillary central incisors with apical periodontitis | Laser + Conventional tx (28 patients)/ Conventional tx + placebo laser device (28 patients) Microbiological samples: 1.initial 2.after mechanical preparation 3.after laser day 0 (only Laser group) 4. day 7 (before irradiation) 5. day 7 (after irradiation for LG) before obturation 17% EDTA, and 2.5% NaOCl was used and Saline for the final irrigation | Pain (NRS) Micro-biology | 980 nm 1.2 W gated mode 200 μm 1 mm from apex Speed of movement 2 mm/sec irradiation in helicoidal motion touching the canal walls 5 s each canal with 10-sec intervals 4 repetitions /2 sessions: day 0, day 7 | 7 days | Pain NRS: Laser group significantly better 6–12–24 h p < 0.001 48 h p = 0.002 7d p = 0.044 Bacteria: Laser group significantly better Both aerobic and anaerobic in all sampling times |
| Yoo et al. (2013) [31] | Parallel-group RCT/40 patients/teeth with persistent symptomatic apical periodontitis retreatment | Laser + Conventional tx (20 patients)/ Conventional tx (placebo laser) (20 patients) Root canal exudate to quantify the associated levels of substance P, calcitonin gene-related peptide (CGRP), and matrix metalloproteinase (MMP)-8 by immunoassay Both groups: copious 3.5% NaOCl was used as irrigation and filled with Ca(OH)2 | Pain (VAS) Percussion (VAS) Reduction of pain-related neuropeptides and inflammatory cytokine levels in root canal exudates | 1440 nm 0.2 W pulsed mode 1 Hz 200 mJ 300 μm tip apical 3 mm stationary (to prevent touching the walls) for 10 sec Canal DRY /1 session: day 0 | 3 days | Laser irradiation was significantly more effective in reducing pain on percussion (p = 0.003) and in decreasing substanceP (p = 0.002) CGRP (p = 0.049) and MMP-8 (p = 0.002) VAS-percussion was positively correlated with substanceP, CGRP, and MMP-8 levels. VAS-spontaneous pain was positively correlated with substanceP and MMP-8 levels. SubstanceP levels correlated directly with CGRP levels |
| Citation | Type of Study/Number of Samples | Test/Control Groups | Aim/ Approach | Laser + PS Used aPDT Protocol | Follow-up | Outcome |
|---|---|---|---|---|---|---|
| Coelho et al. (2019) [32] | Parallel-group RCT/60 patients/single-rooted teeth with fully developed apices, no probing and no mobility Rubber dam used | aPDT + Conventional rc tx (30 patients)/ Conventional rc tx (30 patients) Both groups received MB for 2 mins | Pain (VAS) | 660 nm + MB (0.5 mg/mL) 2 mins incubation time 100 mW 180 s irradiation tip at working length in vertical motion 18 J 600 J/cm2 1 session: day 0 | 7 days | aPDT + RC tx group showed significant difference in VAS score (lower) after 24 h and 72 h After 7 days no pain and no flare-up in both groups |
| de Miranda et al. (2018) [33] | Parallel-group RCT/16 patients/mandibular molars with apical periodontitis Rubber dam used | aPDT + Conventional rc tx (16 molars)/Conventional rc tx (16 molars) Both groups Ca(OH)2 for 7 days before obturation | Clinical symptoms (VAS) Periapical Index (PAI) Micro-biology | 660 nm + MB (25 mg/mL) 5 mins incubation time 100 mW 300 s irradiation in vertical motion 300 μm tip 1 session: day 0 | 6 months | Clinically (VAS) no significant difference Microbiology no significant difference Radiographically significant better healing in aPDT group |
| Pourhajibagher et al. (2017) [34] | Repeated measures/14 patients with secondary-persistent endodontic infections (retreatments) Rubber dam used | Conventional endo re-treatment + aPDT Sampling before+after aPDT | Micro-biology | 635 nm + TBO (0.025 mg/mL) 5 mins incubation time 220 mW 30 s irradiation 1 mm from WL 750 μm diffusor tip 1 session: day 0 | Microbiological samples before/ after | Significant difference p < 0.05 in total bacteria count of secondary endodontic infection in aPDT group |
| Juric et al. (2014) [35] | Repeated measures/ 21 periapical periodontitis endo retreatment (endo ≥ 2 years) apical bone lesion 3 × 3 mm microbiological samples: 1. after access of canal 2. after endo re-treatment 3. after aPDT Rubber dam used | Conventional endo re-treatment + aPDT Sampling before+after aPDT | Micro-biology | 660 + MB (10 mg/mL) 2 min incubation Wash with distilled water and dry 100 mW 60 s irradiation 450 μm diffusor tip 1 session: day 0 |
microbiological samples: 1. after access of canal 2. after endo re-treatment 3. after aPDT | chemomechanical preparation + aPDT vs. chemomechanical preparation alone significant difference in bacteria: gram positive (p = 0.02) gram negative (p = 0.005) facultative anaerobes (p = 0.013) obligate anaerobes (p = 0.007) |
| Garcez et al. (2010) [36] | Repeated measures/30 teeth of 21 patients periapical periodontitis, endo retreatment previously with antibiotic resistance apical bone lesion microbiological samples: 1. after access of canal 2. after endo re-treatment 3. after aPDT Rubber dam used | Conventional endo re-treatment + aPDT Sampling before+after aPDT Placing Ca(OH)2 for 7 days and then second aPDT session without sampling | Micro-biology | 660 nm + polyethylenimine chlorin(e6) (3.6 mg/mL) 2 min incubation wash with distilled water and dry 40 mW 240 s irradiation 9.6 J 200 μm tip spiral movement 1 session: day 0 |
microbiological samples: 1. after access of canal 2. after endo re-treatment 3. after aPDT | The combination of endodontic therapy and aPDT killed all 9 multi-drug resistant bacterial species found in root canal infections no statistical analysis |
| Citation [ref] | Type of Study/Number of Samples | Test/Control Groups | Aim/ Approach | Laser/ Protocol | Follow-up | Outcome |
|---|---|---|---|---|---|---|
| Nunes et al. (2019) [37] | Parallel-group RCT/70 patients/mandibular molars with pulpitis | conventional rc tx + PBM (35 patients)/conventional rc tx + ibuprofen 600mg after 12 + 24h (35 patients) | Pain (VRS+NRS) | 808 nm 100 mW CW Spot size 0.0283 cm2 2 points buccal 2 points lingual corresponding to the apex of each root Contact with mucosa 25 s per point 2.5 J per point 90 J/cm2 per point Power meter 1 session: day 0 | 72 h | VRS: 6 h p < 0.001 12 h p = 0.005 24 h p = 0.001 72 h p = 0.317 (ns) NRS: 6 h p = 0.001 12 h p = 0.002 24 h p < 0.001 72 h p = 0.317 (ns) |
| Lopes et al. (2019) [38] | Parallel-group RCT/60 patients/mandibular molars with pulpitis | conventional rc tx + PBM (30 patients)/conventional rc tx (30 patients) | Pain (VRS + NRS) Possible reason of pain (regression analysis) | 808 nm 100 mW CW Spot size 0.0283 cm2 2 points buccal 2 points lingual corresponding to the apex of each root Contact with mucosa 25 s per point 2.5 J per point 90 J/cm2 per point 1 session: day 0 | 24 h | VRS: 6 h p = 0.123 12 h p = 0.127 24 h p = 0.013 NRS: 6 h p = 0.123 12 h p = 0.127 24 h p = 0.015 pain intensity associated with extrusion of root canal filling material-regression analysis |
| Doganay et al. (2019) [39] | Parallel-group RCT/26 patients/mandibular molars with symptomatic apical periodontitis | conventional rc tx + PBM (13 patients)/conventional rc tx + placebo (13 patients) | Pain (VAS) Substance P in gingival crevicular fluid (GCF) Immune-assay ELISA | 970 nm 0.5 W 10 Hz Pulse width duty cycle 50% Tip-to-tissue 10 mm Apex area circular movement 200 μm tip Spot size 1.1569 cm2 60 s per tooth 2.86 W/cm2 1 session: day 0 | 7 days | Substance P Placebo group p = 0.553 PBM group significantly higher p = 0.005 VAS-percussion pain was significantly lower in PBM group Day 1 p = 0.006 Day 3 p = 0.019 Day 5 p = 0.011 Day 7 p = 0.046 |
| Arslan et al. (2018) [40] | Parallel-group RCT/39 patients/mandibular molars with symptomatic apical periodontitis | conventional rc tx + PBM (13 patients)/conventional rc tx + intracanal laser (13 patients)/conventional rc tx + placebo (13 patients) GCF sample collected always also in contralateral tooth | Pain VAS-percussion (Pearson’s correlation) calcitonin gene-related peptide (CGRP) in the gingival crevicular fluid (GCF) GCF sample collected always also in contralateral tooth as control | 970 nm Intracanal: 2 W, 200 μm tip WL-1 mm up-and-down motion under continuous irrigation with distilled water Irradiation time 60 s PBM: 0.5 W 10 Hz Tip-to-tissue 10 mm Apex area 200 μm tip 30 s per mesial and distal root 2.86 W/cm2 1 session: day 0 | VAS day 0 and 7 CGRP Day 0 and 7 | CGRP: Placebo group significantly higher for experimental than control teeth Intracanal and PBM groups no significant difference between experimental and control teeth VAS: Pain on percussion positively correlated to total amount of CGRP |
| Nabi et al. (2018) [41] | Parallel-group RCT/120 patients/ teeth with pulpitis | conventional rc tx + PBM (30 patients)/ conventional rc tx + 400 ibuprofen 1 h before tx (30 patients)/ conventional rc tx + 400 ibuprofen 1 h before tx + PBM (30 patients)/ conventional rc tx (30 patients) | Pain Heft and Parker pain rating scale | 905 nm 50 Hz 3 min irradiation buccal and lingual perpendicular to apex | 48 h | 24 h: PBM-only group vs. ibuprofen p = 0.04 (PBM less pain) PBM-only group vs. PBM+ibuprofen p = 0.455 (ns) PBM-only vs. no medication p = 0.004 (PBM less pain) 48h: PBM-only group vs. ibuprofen p = 0.046 (PBM less pain) PBM-only group vs. PBM+ibuprofen p = 0.808 (ns) PBM-only vs. no medication p = 0.002 (PBM less pain) |
| Doganay et al. (2018) [42] | Parallel-group RCT/42 patients mandibular molars with symptomatic apical periodontitis | conventional rc tx + PBM (14 patients)/ conventional rc tx + placebo (14 patients)/ Conventional only rc tx (14 patients) | Pain (VAS) Percussion-pain (VAS) | 970 nm 0.5 W 10 Hz Tip-to-tissue 10 mm Apex area 8 mm tip 30 s per mesial and distal root 2.86 W/cm2/ 1 session: day 0 | 7 days | PBM-group lower pain p < 0.05 in day 1 and 3 Percussion at day 7 no significant difference |
| Arslan et al. (2017) [43] | Parallel-group RCT/36 patients mandibular molars with periapical lesion | conventional rc tx + PBM (18 patients)/ conventional rc tx (18 patients) | Pain (VAS) and number of analgesics Percussion | 970 nm 0.5 W 10 Hz Tip-to-tissue 10 mm Apex area 8 mm tip 30 s per mesial and distal root 2.86 W/cm2/ 1 session: day 0 | 7 days | PBM-group lower pain p < 0.05 in first four days Number of analgesics taken significantly lower Percussion day 7 no significant difference |
| Asnaashari et al. (2017) [44] | Parallel-group RCT/61 patients Retreatment of maxillar and mandibular molars | conventional rc tx + PBM (41 patients)/ conventional rc tx (20 patients) | 808 nm 100 mW 70 J/cm2 80 s 600 μm tip Buccal and lingual apical area/ 1 session: day 0 | VAS and analgesic consumption not statistically significant at any time |
| Citation [ref] | Randomization | Sample Size Calculation and Required Number Included | Allocation Ratio of 1:1 | Baseline Situation Similar | Blinding | Parameters of Laser Use Described Appropriately and Calculations Correct | Power Meter Used | Numerical Results Available (Statistics) | Outcome Data Complete | Correct Inter-pretation of Data | Total Score/10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Endo + ConvLas | |||||||||||
| Genc Sen et al. (2019) [28] | yes | yes | yes | yes | yes | yes | no | yes | yes | yes | 9 |
| Dagher et al. (2019) [29] | yes | no | no | yes | yes | yes | no | yes | yes | yes | 7 |
| Morsy et al. (2018) [30] | yes | yes | yes | yes | yes | no | no | yes | yes | yes | 9 |
| Yoo et al. (2013) [31] | yes | yes | yes | yes | yes | no | no | yes | yes | yes | 9 |
| Endo + aPDT | |||||||||||
| Coelho et al. (2019) [32] | yes | yes | yes | yes | yes | yes | no | yes | yes | yes | 9 |
| de Miranda et al. (2018) [33] | yes | yes | yes | yes | yes | yes | no | yes | yes | yes | 9 |
| Pourhajibagher et al. (2017) [34] | yes | no | yes | yes | yes | yes | no | yes | yes | yes | 8 |
| Juric et al (2014) [35] | yes | no | yes | yes | yes | yes | no | yes | yes | yes | 8 |
| Garcez et al. (2010) [36] | yes | no | yes | yes | yes | yes | no | no | yes | yes | 7 |
| Endo + PBM | |||||||||||
| Nunes et al. (2019) [37] | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | 10 |
| Lopes et al. (2019) [38] | yes | yes | yes | yes | yes | yes | no | yes | yes | yes | 9 |
| Doganay et al. (2019) [39] | yes | no | yes | yes | yes | no | no | yes | yes | yes | 7 |
| Arslan et al. (2018) [40] | yes | no | yes | yes | yes | yes | no | yes | yes | yes | 8 |
| Nabi et al. (2018) [41] | yes | no | yes | yes | no | no | no | yes | yes | yes | 6 |
| Doganay et al. (2018) [42] | yes | no | yes | yes | yes | yes | no | yes | yes | yes | 8 |
| Arslan et al. (2017) [43] | yes | yes | yes | yes | yes | yes | no | yes | yes | yes | 9 |
| Asnaashari et al. (2017) [44] | yes | yes | no | yes | no | no | no | yes | yes | yes | 6 |
| Conventional | 1 Study [28] | 1 Study [29] |
|---|---|---|
| Wavelength (nm) | 940 | 2940 |
| Power (W) | 1 | 0.3 |
| Energy per pulse (mJ) | CW | 20 |
| Pulse duration (μs) | CW | 50 |
| Frequency (Hz) | CW | 15 |
| Tip (μm) | 200 | 600 |
| Tip localization | Working length | Pulp chamber |
| Speed of movement (mm/s) | 2 | 0 |
| Kind of motion | Circular | None |
| Irradiation time (s) | Depending on root canal length | 30 |
| Time-intervals (s) | 20 | 30 |
| Repetition of irradiation cycles | 4 | 4 |
| Wet or Dry canal | Dry | EDTA/water/ NaOCl/water |
| Number of sessions | 1 | 1 |
| aPDT | 1 Study [36] | 1 Study [34] | 3 Studies [32,33,35] | ||
|---|---|---|---|---|---|
| Combination PS + Laser Wavelength | PEI-ce6 + 660 nm | TBO + 635 nm | MB + 660 nm | ||
| PS-concentration (mg/mL) | 3.6 | 0.025 | 0.5 | 25 | 10 |
| Incubation time (min) | 2 | 5 | 2 | 5 | 2 |
| Power (mW) | 40 | 220 | 100 | 100 | 100 |
| Irradiation time (s) | 240 | 30 | 180 | 300 | 60 |
| Tip (μm) | 200 | 750 | 200 | 300 | 450 diffusor |
| Number of sessions | 1 | 1 | 1 | 1 | 1 |
| PBM | 2 Studies [37,38] | 1 Study [40] | 2 Studies [42,43] |
|---|---|---|---|
| Wavelength (nm) | 808 | 970 | 970 |
| Power (W) | 0.1 | 0.5 | 0.5 |
| Energy per pulse (mJ) | CW | 25 | 25 |
| Pulse duration (ms) | CW | 50 | 50 |
| Frequency (Hz) | CW | 10 | 10 |
| Tip (μm) | 1900 | 200 | 8000 |
| Tip-to-tissue distance (mm) | 0 | 10 | 10 |
| Speed of movement (mm/s) | 0 | 0 | 0 |
| Irradiation time (s) | 25 per point | 30 per root | 30 per root |
| Fluence (J/cm2) | 90 per point | 43.1 per root | 6.1 per root |
| Number of sessions | 1 | 1 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anagnostaki, E.; Mylona, V.; Parker, S.; Lynch, E.; Grootveld, M. Systematic Review on the Role of Lasers in Endodontic Therapy: Valuable Adjunct Treatment? Dent. J. 2020, 8, 63. https://doi.org/10.3390/dj8030063
Anagnostaki E, Mylona V, Parker S, Lynch E, Grootveld M. Systematic Review on the Role of Lasers in Endodontic Therapy: Valuable Adjunct Treatment? Dentistry Journal. 2020; 8(3):63. https://doi.org/10.3390/dj8030063
Chicago/Turabian StyleAnagnostaki, Eugenia, Valina Mylona, Steven Parker, Edward Lynch, and Martin Grootveld. 2020. "Systematic Review on the Role of Lasers in Endodontic Therapy: Valuable Adjunct Treatment?" Dentistry Journal 8, no. 3: 63. https://doi.org/10.3390/dj8030063
APA StyleAnagnostaki, E., Mylona, V., Parker, S., Lynch, E., & Grootveld, M. (2020). Systematic Review on the Role of Lasers in Endodontic Therapy: Valuable Adjunct Treatment? Dentistry Journal, 8(3), 63. https://doi.org/10.3390/dj8030063