
Subgingival Microbiota Profile in Association with Cigarette Smoking in Young Adults: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
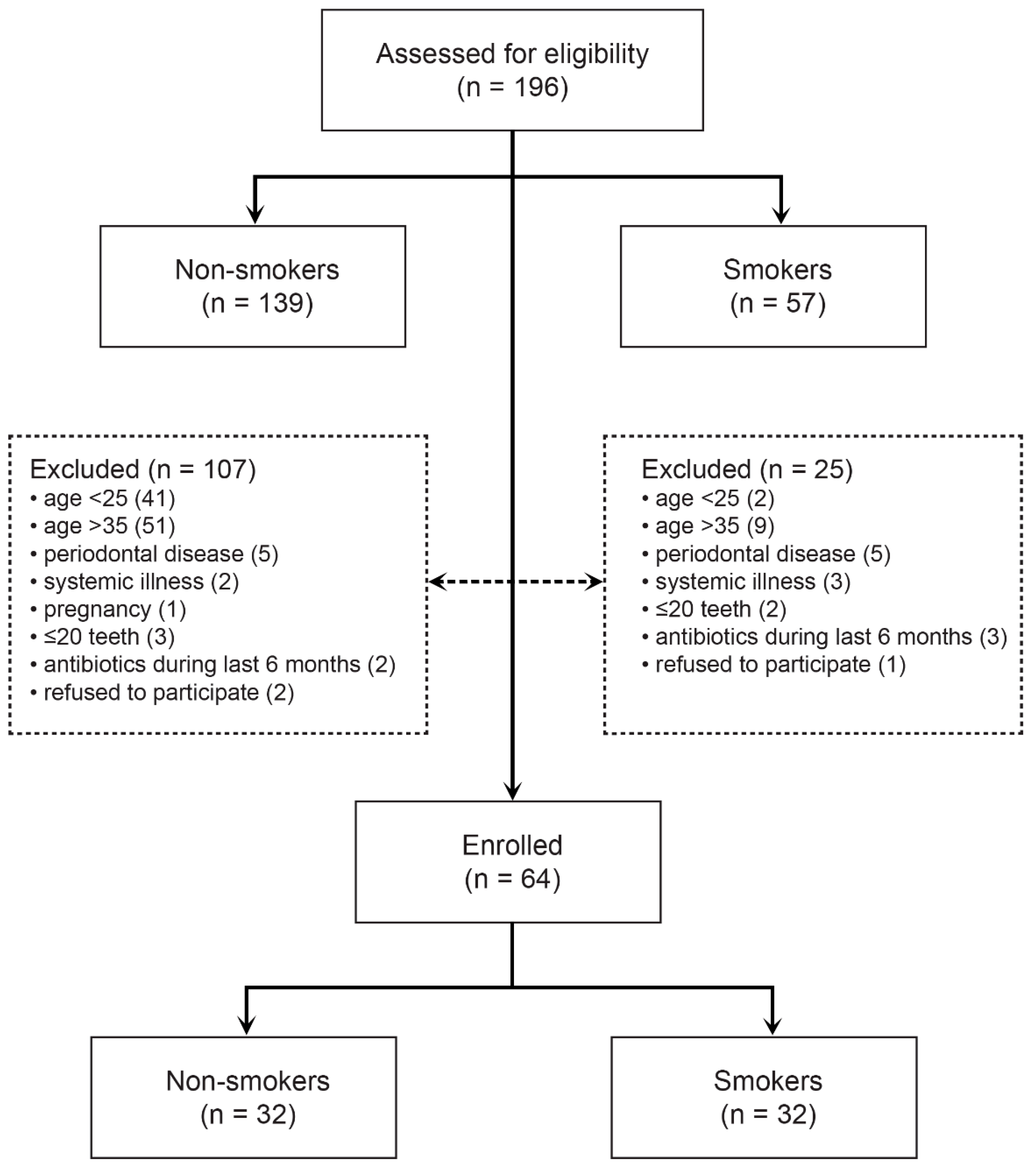
2.2. Subjects
2.3. Sample Size
2.4. Microbiological Sampling and Analyses
2.5. Clinical Examination
2.6. Statistical Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Apatzidou, D.A.; Riggio, M.P.; Kinane, D.F. Impact of smoking on the clinical, microbiological and immunological parameters of adult patients with periodontitis. J. Clin. Periodontol. 2005, 32, 973–983. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.C.; Piccinin, F.B.; Oppermann, R.V.; Susin, C.; Nonnenmacher, C.I.; Mutters, R.; Marcantonio, R.A. Periodontal status in smokers and never-smokers: Clinical findings and real-time polymerase chain reaction quantification of putative periodontal pathogens. J. Periodontol. 2006, 77, 1483–1490. [Google Scholar] [CrossRef]
- Kanwar, A.; Sah, K.; Grover, N.; Chandra, S.; Singh, R.R. Long-term effect of tobacco on resting whole mouth salivary flow rate and pH: An institutional based comparative study. Eur. J. Gen. Dent. 2013, 2, 296. [Google Scholar] [CrossRef]
- Kenney, E.B.; Kraal, J.H.; Saxe, S.R.; Jones, J. The effect of cigarette smoke on human oral polymorphonuclear leukocytes. J. Periodontal Res. 1977, 12, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. The impact of smoking on oral and nasopharyngeal bacterial flora. J. Dent. Res. 2011, 90, 704–710. [Google Scholar] [CrossRef]
- Macgregor, I.D. Effects of smoking on oral ecology. A review of the literature. Clin. Prev. Dent. 1989, 11, 3–7. [Google Scholar]
- Sopori, M. Effects of cigarette smoke on the immune system. Nat. Rev. Immunol. 2002, 2, 372–377. [Google Scholar] [CrossRef]
- Mason, M.R.; Preshaw, P.M.; Nagaraja, H.N.; Dabdoub, S.M.; Rahman, A.; Kumar, P.S. The subgingival microbiome of clinically healthy current and never smokers. ISME J. 2015, 9, 268–272. [Google Scholar] [CrossRef] [Green Version]
- Karasneh, J.A.; Al Habashneh, R.A.; Marzouka, N.A.S.; Thornhill, M.H. Effect of cigarette smoking on subgingival bacteria in healthy subjects and patients with chronic periodontitis. BMC Oral Health 2017, 17, 64. [Google Scholar] [CrossRef] [Green Version]
- Haffajee, A.D.; Socransky, S.S. Relationship of cigarette smoking to the subgingival microbiota. J. Clin. Periodontol. 2001, 28, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Peters, B.A.; Dominianni, C.; Zhang, Y.; Pei, Z.; Yang, L.; Ma, Y.; Purdue, M.P.; Jacobs, E.J.; Gapstur, S.M.; et al. Cigarette smoking and the oral microbiome in a large study of American adults. ISME J. 2016, 10, 2435–2446. [Google Scholar] [CrossRef]
- Boström, L.; Bergström, J.; Dahlén, G.; Linder, L.E. Smoking and subgingival microflora in periodontal disease. J. Clin. Periodontol. 2001, 28, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Kamma, J.J.; Nakou, M.; Baehni, P.C. Clinical and microbiological characteristics of smokers with early onset periodontitis. J. Periodontal Res. 1999, 34, 25–33. [Google Scholar] [CrossRef]
- Van Winkelhoff, A.J.; Bosch-Tijhof, C.J.; Winkel, E.G.; van der Reijden, W.A. Smoking affects the subgingival microflora in periodontitis. J. Periodontol. 2001, 72, 666–671. [Google Scholar] [CrossRef]
- Kumar, P.S.; Matthews, C.R.; Joshi, V.; de Jager, M.; Aspiras, M. Tobacco Smoking Affects Bacterial Acquisition and Colonization in Oral Biofilms. Infect. Immun. 2011, 79, 4730–4738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, G.; Phillips, S.; Gail, M.H.; Goedert, J.J.; Humphrys, M.S.; Ravel, J.; Ren, Y.; Caporaso, N.E. The effect of cigarette smoking on the oral and nasal microbiota. Microbiome 2017, 5, 3. [Google Scholar] [CrossRef] [Green Version]
- Gomes, S.C.; Nonnenmacher, C.; Susin, C.; Oppermann, R.V.; Mutters, R.; Marcantonio, R.A.C. The effect of a supragingival plaque-control regimen on the subgingival microbiota in smokers and never-smokers: Evaluation by real-time polymerase chain reaction. J. Periodontol. 2008, 79, 2297–2304. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Zhou, X.; Cheng, L.; Li, M. The Impact of Smoking on Subgingival Microflora: From Periodontal Health to Disease. Front. Microbiol. 2020, 11, 66. [Google Scholar] [CrossRef]
- Coretti, L.; Cuomo, M.; Florio, E.; Palumbo, D.; Keller, S.; Pero, R.; Chiariotti, L.; Lembo, F.; Cafiero, C. Subgingival dysbiosis in smoker and non-smoker patients with chronic periodontitis. Mol. Med. Rep. 2017, 15, 2007–2014. [Google Scholar] [CrossRef] [Green Version]
- Delima, S.L.; McBride, R.K.; Preshaw, P.M.; Heasman, P.A.; Kumar, P.S. Response of Subgingival Bacteria to Smoking Cessation. J. Clin. Microbiol. 2010, 48, 2344–2349. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Heikkinen, A.M.; Pitkäniemi, J.; Kari, K.; Pajukanta, R.; Elonheimo, O.; Koskenvuo, M.; Meurman, J.H. Effect of teenage smoking on the prevalence of periodontal bacteria. Clin. Oral Investig. 2012, 16, 571–580. [Google Scholar] [CrossRef]
- Garcia, L.S. (Ed.) Clinical Microbiology Procedures Handbook, 3rd ed.; American Society of Microbiology: Washington, DC, USA, 2010. [Google Scholar]
- Freiwald, A.; Sauer, S. Phylogenetic classification and identification of bacteria by mass spectrometry. Nat. Protoc. 2009, 4, 732–742. [Google Scholar] [CrossRef] [PubMed]
- Haigh, J.; Degun, A.; Eydmann, M.; Millar, M.; Wilks, M. Improved performance of bacterium and yeast identification by a commercial matrix-assisted laser desorption ionization-time of flight mass spectrometry system in the clinical microbiology laboratory. J. Clin. Microbiol. 2011, 49, 3441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The Plaque Control Record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Tang, G.; Samaranayake, L.P.; Yip, H.-K.; Chu, F.C.S.; Tsang, P.C.S.; Cheung, B.P.K. Direct detection of Actinomyces spp. from infected root canals in a Chinese population: A study using PCR-based, oligonucleotide-DNA hybridization technique. J. Dent. 2003, 31, 559–568. [Google Scholar] [CrossRef] [Green Version]
- Hamada, S.; Amano, A.; Kimura, S.; Nakagawa, I.; Kawabata, S.; Morisaki, I. The importance of fimbriae in the virulence and ecology of some oral bacteria. Oral Microbiol. Immunol. 1998, 13, 129–138. [Google Scholar] [CrossRef]
- Egland, P.G.; Dû, L.D.; Kolenbrander, P.E. Identification of Independent Streptococcus gordonii SspA and SspB Functions in Coaggregation with Actinomyces naeslundii. Infect. Immun. 2001, 69, 7512–7516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Teles, R.; Sakellari, D.; Teles, F.; Konstantinidis, A.; Kent, R.; Socransky, S.; Haffajee, A. Relationships among gingival crevicular fluid biomarkers, clinical parameters of periodontal disease, and the subgingival microbiota. J. Periodontol. 2010, 81, 89–98. [Google Scholar] [CrossRef]
- Faveri, M.; Figueiredo, L.C.; Duarte, P.M.; Mestnik, M.J.; Mayer, M.P.A.; Feres, M. Microbiological profile of untreated subjects with localized aggressive periodontitis. J. Clin. Periodontol. 2009, 36, 739–749. [Google Scholar] [CrossRef]
- Vielkind, P.; Jentsch, H.; Eschrich, K.; Rodloff, A.C.; Stingu, C.-S. Prevalence of Actinomyces spp. in patients with chronic periodontitis. Int. J. Med. Microbiol. 2015, 305, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Ximénez-Fyvie, L.A.; Haffajee, A.D.; Socransky, S.S. Comparison of the microbiota of supra-and subgingival plaque in health and periodontitis. J. Clin. Periodontol. 2000, 27, 648–657. [Google Scholar] [CrossRef]
- Shchipkova, A.Y.; Nagaraja, H.N.; Kumar, P.S. Subgingival Microbial Profiles of Smokers with Periodontitis. J. Dent. Res. 2010, 89, 1247–1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, A.; Maiden, M.F.J.; Macuch, P.J.; Murray, L.L.; Kent, R.L. Microbiota of health, gingivitis, and initial periodontitis. J. Clin. Periodontol. 1998, 25, 85–98. [Google Scholar] [CrossRef]
- Mager, D.L.; Haffajee, A.D.; Socransky, S.S. Effects of periodontitis and smoking on the microbiota of oral mucous membranes and saliva in systemically healthy subjects. J. Clin. Periodontol. 2003, 30, 1031–1037. [Google Scholar] [CrossRef]
- Thomas, A.M.; Gleber-Netto, F.O.; Fernandes, G.R.; Amorim, M.; Barbosa, L.F.; Francisco, A.L.N.; de Andrade, A.G.; Setubal, J.C.; Kowalski, L.P.; Nunes, D.N.; et al. Alcohol and tobacco consumption affects bacterial richness in oral cavity mucosa biofilms. BMC Microbiol. 2014, 14, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lie, M.A.; Weijden, G.A.; Timmerman, M.F.; Loos, B.G.; Steenbergen, T.J.M.; Velden, U. Oral microbiota in smokers and non-smokers in natural and experimentally-induced gingivitis. J. Clin. Periodontol. 2005, 25, 677–686. [Google Scholar] [CrossRef]
- Stingu, C.S.; Rodloff, A.C.; Jentsch, H.; Schaumann, R.; Eschrich, K. Rapid identification of oral anaerobic bacteria cultivated from subgingival biofilm by MALDI-TOF-MS. Mol. Oral Microbiol. 2008, 23, 372–376. [Google Scholar] [CrossRef]
- Kreth, J.; Merritt, J.; Shi, W.; Qi, F. Competition and Coexistence between Streptococcus mutans and Streptococcus sanguinis in the Dental Biofilm. J. Bacteriol. 2005, 187, 7193–7203. [Google Scholar] [CrossRef] [Green Version]
- Hillman, J.D.; Socransky, S.S. Bacterial interference in the oral ecology of Actinobacillus actinomycetemcomitans and its relationship to human periodontosis. Arch. Oral Biol. 1982, 27, 75–77. [Google Scholar] [CrossRef]
- Teughels, W.; Kinder Haake, S.; Sliepen, I.; Pauwels, M.; Van Eldere, J.; Cassiman, J.-J.; Quirynen, M. Bacteria Interfere with A. actinomycetemcomitans Colonization. J. Dent. Res. 2007, 86, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.C.; Zhou, C.; Wu, B.; Zhang, Y.H. Investigation on interaction between Streptococcus sanguis and Porphyromonas gingivalis in specific pathogen-free rats. Chin. J. Dent. Res. 2000, 3, 5–9. [Google Scholar]
- Huang, R.; Li, M.; Gregory, R.L. Bacterial interactions in dental biofilm. Virulence 2011, 2, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Hammond, B.F.; Lillard, S.E.; Stevens, R.H. A bacteriocin of Actinobacillus actinomycetemcomitans. Infect. Immun. 1987, 55, 686–691. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.-H.; Lee, J.-H.; Lee, J.-Y. Subgingival microbiome in smokers and non-smokers in Korean chronic periodontitis patients. Mol. Oral Microbiol. 2015, 30, 227–241. [Google Scholar] [CrossRef]
- Bizzarro, S.; Loos, B.G.; Laine, M.L.; Crielaard, W.; Zaura, E. Subgingival microbiome in smokers and non-smokers in periodontitis: An exploratory study using traditional targeted techniques and a next-generation sequencing. J. Clin. Periodontol. 2013, 40, 483–492. [Google Scholar] [CrossRef]
- Signat, B.; Roques, C.; Poulet, P.; Duffaut, D. Fusobacterium nucleatum in periodontal health and disease. Curr. Issues Mol. Biol. 2011, 13, 25–36. [Google Scholar]


{kind=link}
| Non-Smokers (n = 32) | Smokers (n = 32) | |||
|---|---|---|---|---|
| Gender | ||||
| women | 15 | (46.9) | 13 | (40.6) |
| men | 17 | (53.1) | 19 | (59.4) |
| Age (years), median (IQR) | 31 | (26–34) | 30 | (27–32) |
| Dental exams at least once a year | 20 | (62.5) | 21 | (65.6) |
| Periodontal indices | ||||
| approximal plaque index | 0.18 | (0.13–0.22) | 0.15 | (0.10–0.22) |
| bleeding on probing | 0.25 | (0.16–0.30) | 0.23 | (0.08–0.31) |
| periodontal pocket depths (mm) | 2.42 | (2.32–2.49) | 2.50 | (2.26–2.65) |
| gingival retraction (mm) | 0.18 | (0.11–0.26) | 0.14 | (0.03–0.34) |
| clinical attachment level | 2.47 | (2.35–2.55) | 2.56 | (2.30–2.72) |
| Duration of smoking (years), median (IQR) | 12 | (8–15) | ||
| Non-Smokers (n = 32) | Smokers (n = 32) | p | φ | |||
|---|---|---|---|---|---|---|
| Actinobacteria | 15 | (46.9) | 20 | (62.5) | 0.315 | 0.16 |
| Proteobacteria | 10 | (31.3) | 9 | (28.1) | >0.999 | 0.03 |
| Bacteroidetes | 5 | (15.6) | 6 | (18.8) | >0.999 | 0.04 |
| Firmicutes | 28 | (87.5) | 25 | (78.1) | 0.509 | 0.12 |
| Fusobacteria | 6 | (18.8) | 12 | (37.5) | 0.164 | 0.21 |
| Non-Smokers (n = 32) | Smokers (n = 32) | p | φ | |||
|---|---|---|---|---|---|---|
| Veillonella parvula | 8 | (25.0) | 9 | (28.1) | >0.999 | 0.08 |
| Fusobacterium nucleatum | 5 | (15.6) | 8 | (25.0) | 0.536 | 0.12 |
| Actinomyces odontolyticus | 1 | (3.1) | 8 | (25.0) | 0.026 | 0.32 |
| Actinomyces oris | 12 | (37.5) | 7 | (21.9) | 0.274 | 0.17 |
| Parvimonas micra | 4 | (12.5) | 5 | (15.6) | >0.999 | 0.00 |
| Fusobacterium canifelinum | 1 | (3.1) | 4 | (12.5) | 0.355 | 0.18 |
| Capnocytophaga granulosa | 2 | (6.3) | 3 | (9.4) | >0.999 | 0.06 |
| Veillonella atypica | 2 | (6.3) | 3 | (9.4) | >0.999 | 0.06 |
| Capnocytophaga gingivalis | 1 | (3.1) | 3 | (9.4) | 0.613 | 0.13 |
| Gemella morbillorum | 5 | (15.6) | 2 | (6.3) | 0.672 | 0.11 |
| Propionibacterium acnes | 2 | (6.3) | 2 | (6.3) | ||
| Gemella haemolysans | 1 | (3.1) | 2 | (6.3) | ||
| Veillonella dispar | 1 | (3.1) | 2 | (6.3) | ||
| Prevotella intermedia | 3 | (9.4) | 1 | (3.1) | 0.613 | 0.13 |
| Capnocytophaga ochracea | 2 | (6.3) | 1 | (3.1) | ||
| Actinomyces meyeri | 1 | (3.1) | 1 | (3.1) | ||
| Fusobacterium periodonticum | 1 | (3.1) | 1 | (3.1) | ||
| Prevotella nigrescens | 1 | (3.1) | 1 | (3.1) | ||
| Prevotella spp | 1 | (3.1) | 1 | (3.1) | ||
| Atopobium parvulum | 1 | (3.1) | ||||
| Campylobacter showae | 1 | (3.1) | ||||
| Capnocytophaga sputigena | 1 | (3.1) | ||||
| Eubacterium brachy | 1 | (3.1) | ||||
| Fusobacterium naviforme | 1 | (3.1) | ||||
| Gemella bergeri | 1 | (3.1) | ||||
| Lactobacillus salivarius | 1 | (3.1) | ||||
| Leptotrichia wadei | 1 | (3.1) | ||||
| Prevotella buccae | 1 | (3.1) | ||||
| Prevotella loescheii | 1 | (3.1) | ||||
| Prevotella dentalis | 2 | (6.3) | ||||
| Prevotella melaninogenica | 2 | (6.3) | ||||
| Aggregatibacter aphrophilus | 1 | (3.1) | ||||
| Campylobacter concisus | 1 | (3.1) | ||||
| Leptotrichia trevisanii | 1 | (3.1) | ||||
| Prevotella denticola | 1 | (3.1) | ||||
| Veillonella rogosae | 1 | (3.1) | ||||
| No bacteria | 9 | (28.1) | 10 | (31.3) | ||
| Non-Smokers (n = 32) | Smokers (n = 32) | p | φ | |||
|---|---|---|---|---|---|---|
| Streptococcus oralis | 18 | (56.3) | 13 | (40.6) | 0.317 | 0.16 |
| Streptococcus mitis | 9 | (28.1) | 14 | (43.8) | >0.999 | 0.07 |
| Streptococcus salivarius | 3 | (9.4) | 8 | (25.0) | 0.184 | 0.21 |
| Streptococcus sanguinis | 13 | (40.6) | 6 | (18.8) | 0.049 | 0.24 |
| Rothia mucilaginosa | 3 | (9.4) | 6 | (18.8) | 0.474 | 0.14 |
| Streptococcus intermedius | 3 | (9.4) | 6 | (18.8) | 0.474 | 0.14 |
| Streptococcus parasanguinis | 5 | (15.6) | 5 | (15.6) | >0.999 | 0.00 |
| Streptococcus gordonii | 2 | (6.3) | 5 | (15.6) | 0.426 | 0.15 |
| Rothia dentocariosa | 3 | (9.4) | 4 | (12.5) | >0.999 | 0.05 |
| Staphylococcus epidermidis | 3 | (9.4) | 4 | (12.5) | >0.999 | 0.16 |
| Neisseria flavens | 2 | (6.3) | 3 | (9.4) | >0.999 | 0.06 |
| Staphylococcus hominis | 3 | (9.4) | 0.238 | 0.22 | ||
| Streptococcus pneumoniae | 6 | (18.8) | 2 | (6.3) | 0.257 | 0.19 |
| Haemophilus parainfluenze | 5 | (15.6) | 2 | (6.3) | 0.426 | 0.15 |
| Neisseria mucosa | 1 | (3.1) | 2 | (6.3) | ||
| Neisseria bacilliformis | 2 | (6.3) | ||||
| Streptococcus anginosus | 2 | (6.3) | ||||
| Rothia aeria | 1 | (3.1) | 1 | (3.1) | ||
| Streptococcus cristatus | 1 | (3.1) | 1 | (3.1) | ||
| Aggregatibacter aphrophilus | 1 | (3.1) | ||||
| Streptococcus vestibularis | 1 | (3.1) | ||||
| Staphylococcus capitis | 2 | (6.3) | ||||
| Campylobacter showae | 1 | (3.1) | ||||
| Enterococcus faecalis | 1 | (3.1) | ||||
| Neisseria elongata | 1 | (3.1) | ||||
| Neisseria macacae | 1 | (3.1) | ||||
| Staphylococcus aureus | 1 | (3.1) | ||||
| Staphylococcus lugdunensis | 1 | (3.1) | ||||
| Streptococcus cristatus | 1 | (3.1) | ||||
| Streptococcus mutans | 1 | (3.1) | ||||
| No bacteria | 4 | (12.5) | 6 | (18.8) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bašić, K.; Peroš, K.; Bošnjak, Z.; Šutej, I. Subgingival Microbiota Profile in Association with Cigarette Smoking in Young Adults: A Cross-Sectional Study. Dent. J. 2021, 9, 150. https://doi.org/10.3390/dj9120150
Bašić K, Peroš K, Bošnjak Z, Šutej I. Subgingival Microbiota Profile in Association with Cigarette Smoking in Young Adults: A Cross-Sectional Study. Dentistry Journal. 2021; 9(12):150. https://doi.org/10.3390/dj9120150
Chicago/Turabian StyleBašić, Krešimir, Kristina Peroš, Zrinka Bošnjak, and Ivana Šutej. 2021. "Subgingival Microbiota Profile in Association with Cigarette Smoking in Young Adults: A Cross-Sectional Study" Dentistry Journal 9, no. 12: 150. https://doi.org/10.3390/dj9120150
APA StyleBašić, K., Peroš, K., Bošnjak, Z., & Šutej, I. (2021). Subgingival Microbiota Profile in Association with Cigarette Smoking in Young Adults: A Cross-Sectional Study. Dentistry Journal, 9(12), 150. https://doi.org/10.3390/dj9120150