
Effect of Citrulline and Leucine Intake with Exercises on Body Composition, Physical Activity, and Amino Acid Concentration in Older Women: A Randomized Double-Blind Placebo-Controlled Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Participants
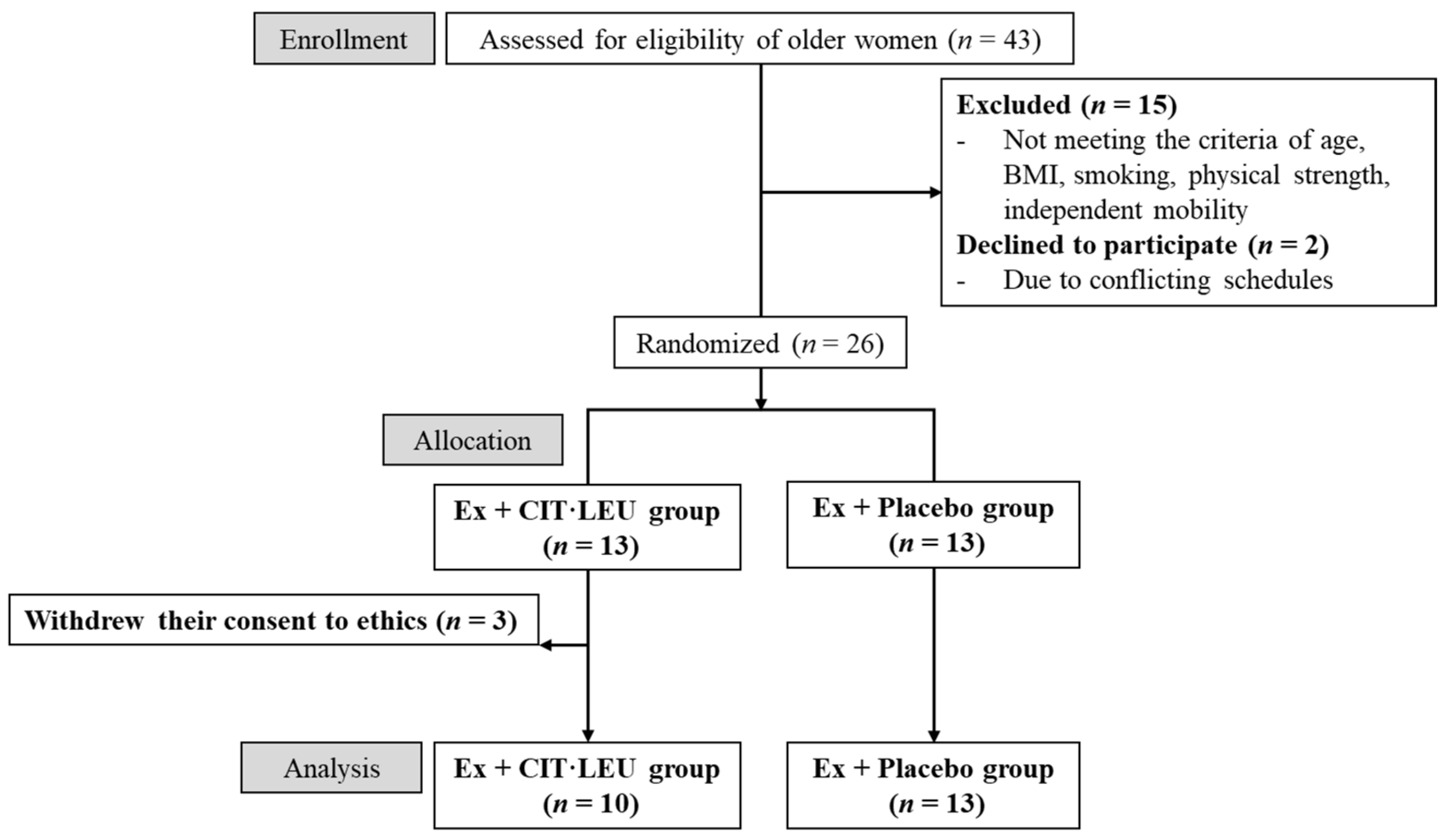
2.2. Study Design
2.3. Characteristics of the Participants
2.4. Body Composition
2.5. Physical Activity
2.6. Amino Acid Concentrations
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Body Compositions
3.3. Physical Activity
3.4. Amino Acid Concentrations in Plasma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baumgartner, R.N.; Stauber, P.M.; McHugh, D.; Koehler, K.M.; Garry, P.J. Cross-sectional age differences in body composition in persons 60 + years of age. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, M307–M316. [Google Scholar] [CrossRef] [PubMed]
- Lexell, J.; Taylor, C.C.; Sjöström, M. What is the cause of the ageing atrophy? Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15- to 83-year-old men. J. Neurol. Sci. 1988, 84, 275–294. [Google Scholar] [CrossRef]
- Strasser, B.; Volaklis, K.; Fuchs, D.; Burtscher, M. Role of dietary protein and muscular fitness on longevity and aging. Aging Dis. 2018, 9, 119. [Google Scholar] [CrossRef] [Green Version]
- Lau, E.M.C.; Lynn, H.S.H.; Woo, J.W.; Kwok, T.C.Y.; Melton III, L.J. Prevalence of and risk factors for sarcopenia in elderly Chinese men and women. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 213–216. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y. Sarcopenia: Prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J. Cachexia Sarcopenia Muscle 2021, 12, 30–38. [Google Scholar] [CrossRef]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [Green Version]
- Atherton, P.J.; Kumar, V.; Selby, A.L.; Rankin, D.; Hildebrandt, W.; Phillips, B.E.; Williams, J.P.; Hiscock, N.; Smith, K. Enriching a protein drink with leucine augments muscle protein synthesis after resistance exercise in young and older men. Clin. Nutr. 2017, 36, 888–895. [Google Scholar] [CrossRef]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of exercise and amino acid supplementation on body composition and physical function in community-dwelling elderly Japanese sarcopenic women: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef]
- Dighe, N.; Anandh, S.; Varadharajulu, G. Effect of Weight Bearing and Neurobic Exercises on Bone Health and Physical Function in Elderly Individuals. Indian J. Public Health Res. Dev. 2020, 11, 261. [Google Scholar] [CrossRef]
- Ayotte, N.W.; Stetts, D.M.; Keenan, G.; Greenway, E.H. Electromyographical analysis of selected lower extremity muscles during 5 unilateral weight-bearing exercises. J. Orthop. Sports Phys. Ther. 2007, 37, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, R.; Okura, T. A novel exercise for improving lower-extremity functional fitness in the elderly. Aging Clin. Exp. Res. 2006, 18, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Fisseha, B.; Janakiraman, B.; Yitayeh, A.; Ravichandran, H. Effect of square stepping exercise for older adults to prevent fall and injury related to fall: Systematic review and meta-analysis of current evidences. J. Exerc. Rehabil. 2017, 13, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sowers, S. A Primer on Branched Chain Amino Acids; Huntington College of Health Sciences: Knoxville, TN, USA, 2009. [Google Scholar]
- Baum, J.I.; O’Connor, J.C.; Seyler, J.E.; Anthony, T.G.; Freund, G.G.; Layman, D.K. Leucine reduces the duration of insulin-induced PI 3-kinase activity in rat skeletal muscle. Am. J. Physiol. Metab. 2005, 288, E86–E91. [Google Scholar] [CrossRef] [Green Version]
- Grimble, G.K. Adverse gastrointestinal effects of arginine and related amino acids. J. Nutr. 2007, 137, 1693S–1701S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curis, E.; Nicolis, I.; Moinard, C.; Osowska, S.; Zerrouk, N.; Bénazeth, S.; Cynober, L. Almost all about citrulline in mammals. Amino Acids 2005, 29, 177. [Google Scholar] [CrossRef]
- Witte, M.B.; Barbul, A. Arginine physiology and its implication for wound healing. Wound Repair Regen. 2003, 11, 419–423. [Google Scholar] [CrossRef]
- Osowska, S.; Duchemann, T.; Walrand, S.; Paillard, A.; Boirie, Y.; Cynober, L.; Moinard, C. Citrulline modulates muscle protein metabolism in old malnourished rats. Am. J. Physiol. Metab. 2006, 291, E582–E586. [Google Scholar] [CrossRef] [Green Version]
- Le Plénier, S.; Walrand, S.; Noirt, R.; Cynober, L.; Moinard, C. Effects of leucine and citrulline versus non-essential amino acids on muscle protein synthesis in fasted rat: A common activation pathway? Amino Acids 2012, 43, 1171–1178. [Google Scholar] [CrossRef]
- Sasazuki, S.; Inoue, M.; Tsuji, I.; Sugawara, Y.; Tamakoshi, A.; Matsuo, K.; Wakai, K.; Nagata, C.; Tanaka, K.; Mizoue, T. Body mass index and mortality from all causes and major causes in Japanese: Results of a pooled analysis of 7 large-scale cohort studies. J. Epidemiol. 2011, 21, 417–430. [Google Scholar] [CrossRef] [Green Version]
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef]
- Jayasekara, H.; English, D.R.; Room, R.; MacInnis, R.J. Alcohol consumption over time and risk of death: A systematic review and meta-analysis. Am. J. Epidemiol. 2014, 179, 1049–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagiwara, A.; Ito, N.; Sawai, K.; Kazuma, K. Validity and reliability of the Physical Activity Scale for the Elderly (PASE) in Japanese elderly people. Geriatr. Gerontol. Int. 2008, 8, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Peake, R.W.A.; Law, T.; Hoover, P.N.; Gaewsky, L.; Shkreta, A.; Kellogg, M.D. Improved separation and analysis of plasma amino acids by modification of the MassTrakTM AAA Solution Ultraperformance® liquid chromatography method. Clin. Chim. Acta 2013, 423, 75–82. [Google Scholar] [CrossRef]
- Cohen, J. Quantitative methods in psychology: A power primer. Psychol. Bull. 1992, 112, 1155–1159. [Google Scholar] [CrossRef]
- Hughes, V.A.; Frontera, W.R.; Wood, M.; Evans, W.J.; Dallal, G.E.; Roubenoff, R.; Singh, M.A.F. Longitudinal muscle strength changes in older adults: Influence of muscle mass, physical activity, and health. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, B209–B217. [Google Scholar] [CrossRef]
- Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; Newman, A.B.; et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [CrossRef]
- Liao, C.-D.; Chen, H.-C.; Huang, S.-W.; Liou, T.-H. The role of muscle mass gain following protein supplementation plus exercise therapy in older adults with sarcopenia and frailty risks: A systematic review and meta-regression analysis of randomized trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, T.; Sairenchi, T.; Iso, H.; Irie, F.; Tanaka, K.; Fukasawa, N.; Ota, H.; Muto, T. Age- and Gender-specific BMI in Terms of the Lowest Mortality in Japanese General Population. Obesity 2008, 16, 2348–2355. [Google Scholar] [CrossRef] [PubMed]
- Elhakeem, A.; Hannam, K.; Deere, K.C.; Hartley, A.; Clark, E.M.; Moss, C.; Edwards, M.H.; Dennison, E.; Gaysin, T.; Kuh, D. Physical activity producing low, but not medium or higher, vertical impacts is inversely related to BMI in older adults: Findings from a multicohort study. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 643–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramontano, A.; Veronese, N.; Sergi, G.; Manzato, E.; Rodriguez-Hurtado, D.; Maggi, S.; Trevisan, C.; De Zaiacomo, F.; Giantin, V. Prevalence of sarcopenia and associated factors in the healthy older adults of the Peruvian Andes. Arch. Gerontol. Geriatr. 2017, 68, 49–54. [Google Scholar] [CrossRef]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef]
- Zhu, L.-Y.; Chan, R.; Kwok, T.; Cheng, K.C.-C.; Ha, A.; Woo, J. Effects of exercise and nutrition supplementation in community-dwelling older Chinese people with sarcopenia: A randomized controlled trial. Age Ageing 2019, 48, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Gwin, J.A.; Church, D.D.; Wolfe, R.R.; Ferrando, A.A.; Pasiakos, S.M. Muscle protein synthesis and whole-body protein turnover responses to ingesting essential amino acids, intact protein, and protein-containing mixed meals with considerations for energy deficit. Nutrients 2020, 12, 2457. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, N.A.; McKinley-Barnard, S.K.; Blahnik, Z.J. Effect of Bang® Pre-Workout Master Blaster® combined with four weeks of resistance training on lean body mass, maximal strength, mircoRNA expression, and serum IGF-1 in men: A randomized, double-blind, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2019, 16, 54. [Google Scholar] [CrossRef] [Green Version]
- Churchward-Venne, T.A.; Cotie, L.M.; MacDonald, M.J.; Mitchell, C.J.; Prior, T.; Baker, S.K.; Phillips, S.M. Citrulline does not enhance blood flow, microvascular circulation, or myofibrillar protein synthesis in elderly men at rest or following exercise. Am. J. Physiol. Metab. 2014, 307, E71–E83. [Google Scholar] [CrossRef] [Green Version]
- Thibault, R.; Flet, L.; Vavasseur, F.; Lemerle, M.; Ferchaud-Roucher, V.; Picot, D.; Darmaun, D. Oral citrulline does not affect whole body protein metabolism in healthy human volunteers: Results of a prospective, randomized, double-blind, cross-over study. Clin. Nutr. 2011, 30, 807–811. [Google Scholar] [CrossRef]
- Allerton, T.D.; Proctor, D.N.; Stephens, J.M.; Dugas, T.R.; Spielmann, G.; Irving, B.A. l-Citrulline supplementation: Impact on cardiometabolic health. Nutrients 2018, 10, 921. [Google Scholar] [CrossRef] [Green Version]
- Food and Agriculture Organization of the United Nations; United Nations University. Protein and Amino Acid Requirements in Human Nutrition; World Health Organization: Geneva, Switzerland; Volume 935, ISBN 9241209356.
- Tessari, P.; Kiwanuka, E.; Zanetti, M.; Barazzoni, R. Postprandial body protein synthesis and amino acid catabolism measured with leucine and phenylalanine-tyrosine tracers. Am. J. Physiol. Metab. 2003, 284, E1037–E1042. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Ex + CIT·LEU (n = 10) | Ex + Placebo (n = 13) | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Unit | Mean | ± | SD | Mean | ± | SD | p-Value |
| Age | (year) | 69.5 | ± | 3.7 | 71.2 | ± | 5.8 | 0.69 |
| Height | (cm) | 151.1 | ± | 4.0 | 155.4 | ± | 5.1 | 0.09 |
| Body weight | (kg) | 42.4 | ± | 2.4 | 45.7 | ± | 3.5 | 0.03 |
| BMI | (kg/m2) | 18.6 | ± | 1.5 | 18.9 | ± | 1.1 | 0.56 |
| Systolic blood pressure | (mmHg) | 119.1 | ± | 12.2 | 132.5 | ± | 13.3 | 0.01 |
| Diastolic blood pressure | (mmHg) | 68.0 | ± | 7.0 | 72.9 | ± | 10.4 | 0.17 |
| Heart rate | (bpm) | 75.8 | ± | 5.8 | 79.8 | ± | 11.0 | 0.17 |
| Intake rate of amino acid supplementation | (%) | 96.5 | ± | 5.0 | 96.9 | ± | 5.0 | 0.69 |
| Participation rate of exercise classes | (%) | 96.1 | ± | 5.3 | 91.5 | ± | 9.2 | 0.23 |
| Hand grip strength | (kg) | 21.0 | ± | 4.4 | 22.7 | ± | 3.0 | 0.66 |
| 5-m habitual walk | (sec) | 4.1 | ± | 0.4 | 4.1 | ± | 1.0 | 0.39 |
| Appendicular lean mass index | (kg/m2) | 5.0 | ± | 0.4 | 5.2 | ± | 0.5 | 0.54 |
| Ex + CIT·LEU (n = 10) | Ex + Placebo (n = 13) | Main Effect of Time p-Value (Pre-Mid-Post) | Interaction p-Value (Groups × Times) | Post Hoc Analysis with Bonferroni Correction | † Main Effect of Time p-Value (Pre-Mid-Post) | † Interaction p-Value (Groups × Times) | † Post Hoc Analysis with Bonferroni Correction | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Unit | Time | Mean | ± | SD | Mean | ± | SD | ||||||
| Height | (cm) | Pre | 151.1 | ± | 4.0 | 155.4 | ± | 5.1 | 0.01 | 0.78 | ||||
| Mid | 150.9 | ± | 3.8 | 155.1 | ± | 5.1 | ||||||||
| Post | 151.1 | ± | 3.9 | 155.4 | ± | 5.2 | ||||||||
| Effect size | 0 | 0 | ||||||||||||
| Body weight | (kg) | Pre | 42.4 | ± | 2.4 | 45.7 | ± | 3.5 | 0.05 | 0.03 | Ex + CIT·LEU: Pre, Mid< Post | |||
| Mid | 42.8 | ± | 3.1 | 45.7 | ± | 3.6 | ||||||||
| Post | 43.4 | ± | 3.2 | 45.6 | ± | 3.6 | ||||||||
| Effect size | 0.4 | 0 | ||||||||||||
| BMI | (kg/m2) | Pre | 18.6 | ± | 1.5 | 18.9 | ± | 1.1 | 0.04 | 0.01 | Ex + CIT·LEU: Pre, Mid < Post | |||
| Mid | 18.9 | ± | 1.7 | 19.0 | ± | 1.0 | ||||||||
| Post | 19.1 | ± | 1.6 | 18.9 | ± | 1.1 | ||||||||
| Effect size | 0.3 | 0 | ||||||||||||
| Variables | Unit | Time | Ex + CIT·LEU (n = 10) | Ex + Placebo (n = 13) | Main Effect of Time p-Value (Pre-Post) | Interaction p-Value (Groups × Times) | Post Hoc Analysis with Bonferroni Correction | † Main Effect of Time p-Value (Pre-Post) | † Interaction p-Value (Groups × Times) | † Post Hoc Analysis with Bonferroni Correction | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Mean | ± | SD | |||||||||
| Body fat | (%) | Pre | 25.6 | ± | 6.5 | 27.7 | ± | 4.3 | 0.28 | 0.23 | 0.84 | 0.53 | ||
| Post | 26.3 | ± | 6.5 | 27.7 | ± | 4.0 | ||||||||
| Effect size | 0.1 | 0 | ||||||||||||
| Bone area | (cm2) | Pre | 1500.2 | ± | 125.2 | 1617.5 | ± | 131.8 | 0.89 | 0.12 | 0.26 | 0.17 | ||
| Post | 1508.5 | ± | 120.1 | 1609.8 | ± | 131.2 | ||||||||
| Effect size | 0.1 | 0.1 | ||||||||||||
| Bone mineral density | (g/cm2) | Pre | 0.99 | ± | 0.13 | 0.98 | ± | 0.09 | 0.01 | 0.49 | 0.38 | 0.88 | ||
| Post | 0.99 | ± | 0.12 | 0.97 | ± | 0.09 | ||||||||
| Effect size | 0.1 | 0.1 | ||||||||||||
| Bone mass | (g) | Pre | 1498.1 | ± | 277.3 | 1594.5 | ± | 264.2 | 0.02 | 0.11 | 0.76 | 0.36 | ||
| Post | 1494.4 | ± | 264.0 | 1565.8 | ± | 253.2 | ||||||||
| Effect size | 0 | 0.1 | ||||||||||||
| Fat mass | (kg) | Pre | 10.7 | ± | 3.3 | 12.3 | ± | 2.5 | 0.30 | 0.09 | 0.97 | 0.22 | ||
| Post | 11.2 | ± | 3.5 | 12.3 | ± | 2.3 | ||||||||
| Effect size | 0.1 | 0 | ||||||||||||
| Lean mass | (kg) | Pre | 29.1 | ± | 1.3 | 30.4 | ± | 2.2 | 0.79 | 0.30 | 0.12 | 0.04 | N.S | |
| Post | 29.4 | ± | 1.3 | 30.3 | ± | 2.4 | ||||||||
| Effect size | 0.2 | 0 | ||||||||||||
| Body mass | (kg) | Pre | 41.3 | ± | 2.6 | 44.3 | ± | 3.4 | 0.41 | 0.06 | 0.92 | 0.02 | Ex + CIT·LEU: Pre < Post | |
| Post | 42.1 | ± | 3.2 | 44.1 | ± | 3.5 | ||||||||
| Effect size | 0.3 | 0.1 | ||||||||||||
| Variables | Unit | Time | Ex + CIT·LEU (n = 10) | Ex + Placebo (n = 13) | Main Effect of Time p-Value (Pre-Mid-Post) | Interaction p-Value (Groups × Times) | Post Hoc Analysis with Bonferroni Correction | † Main Effect of Time p-Value Pre-Mid-Post) | † Interaction p-Value (Groups × Times) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Mean | ± | SD | ||||||||
| Leisure time PA | (score) | Pre | 14.9 | ± | 13.2 | 13.3 | ± | 9.0 | <0.01 | 0.81 | <0.01 | 0.84 | |
| Mid | 38.1 | ± | 27.1 | 33.6 | ± | 15.5 | |||||||
| Post | 32.3 | ± | 17.0 | 28.1 | ± | 12.3 | |||||||
| Effect size | 1.1 | 1.4 | |||||||||||
| Household PA | (score) | Pre | 52.0 | ± | 14.6 | 87.5 | ± | 35.6 | 0.02 | 0.04 | Ex + CIT·LEU: Pre < Mid, Post | <0.01 | 0.25 |
| Mid | 77.4 | ± | 24.2 | 82.5 | ± | 27.6 | |||||||
| Post | 80.7 | ± | 20.5 | 93.4 | ± | 23.6 | |||||||
| Effect size | 1.6 | 0.2 | |||||||||||
| Occupational PA | (score) | Pre | 9.3 | ± | 18.8 | 6.6 | ± | 20.0 | 0.44 | 0.92 | 0.76 | 0.75 | |
| Mid | 9.3 | ± | 17.9 | 6.5 | ± | 19.9 | |||||||
| Post | 8.1 | ± | 17.9 | 4.8 | ± | 13.6 | |||||||
| Effect size | 0.1 | 0.1 | |||||||||||
| Total PA | (score) | Pre | 76.2 | ± | 31.8 | 107.4 | ± | 50.0 | <0.01 | 0.04 | Ex + CIT·LEU: Pre < Mid, Post | <0.01 | 0.15 |
| Mid | 124.8 | ± | 46.0 | 122.5 | ± | 35.3 | |||||||
| Post | 121.1 | ± | 29.6 | 126.3 | ± | 32.5 | |||||||
| Effect size | 1.5 | 0.5 | |||||||||||
| Variables | Unit | Time | Ex + CIT·LEU (n = 10) | Ex + Placebo (n = 13) | Main Effect of Time p-Value (Pre - Post) | Interaction p-Value (Groups × Times) | Post Hoc Analysis with Bonferroni Correction | † Main Effect of Time p-Value (Pre - Post) | † Interaction p-Value (Groups × Times) | † Post Hoc Analysis with Bonferroni Correction | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Mean | ± | SD | |||||||||
| Arginine | (nmol/mL) | Pre | 69.3 | ± | 14.2 | 65.2 | ± | 16.0 | <0.01 | 0.68 | <0.01 | 0.37 | ||
| Post | 92.5 | ± | 18.3 | 85.1 | ± | 13.9 | ||||||||
| Effect size | 1.4 | 1.3 | ||||||||||||
| Citrulline | (nmol/mL) | Pre | 32.4 | ± | 6.8 | 34.5 | ± | 6.9 | <0.01 | 0.07 | 0.03 | 0.11 | ||
| Post | 37.1 | ± | 7.6 | 36.0 | ± | 6.2 | ||||||||
| Effect size | 0.7 | 0.2 | ||||||||||||
| Leucine | (nmol/mL) | Pre | 104.0 | ± | 23.5 | 105.7 | ± | 17.8 | 0.05 | 0.12 | <0.01 | 0.07 | ||
| Post | 113.5 | ± | 19.0 | 107.3 | ± | 13.1 | ||||||||
| Effect size | 0.5 | 0.1 | ||||||||||||
| Valine | (nmol/mL) | Pre | 195.7 | ± | 35.8 | 197.8 | ± | 31.1 | <0.01 | 0.79 | 0.03 | 0.82 | ||
| Post | 219.1 | ± | 35.6 | 218.2 | ± | 33.0 | ||||||||
| Effect size | 0.7 | 0.6 | ||||||||||||
| Isoleucine | (nmol/mL) | Pre | 49.2 | ± | 11.2 | 52.6 | ± | 9.3 | <0.01 | 0.25 | 0.01 | 0.37 | ||
| Post | 56.4 | ± | 11.7 | 56.3 | ± | 8.3 | ||||||||
| Effect size | 0.6 | 0.4 | ||||||||||||
| Threonine | (nmol/mL) | Pre | 114.7 | ± | 14.8 | 110.4 | ± | 19.9 | <0.01 | 0.52 | 0.28 | 0.58 | ||
| Post | 125.3 | ± | 20.2 | 126.3 | ± | 27.3 | ||||||||
| Effect size | 0.6 | 0.7 | ||||||||||||
| Serine | (nmol/mL) | Pre | 125.2 | ± | 14.0 | 116.0 | ± | 14.0 | 0.08 | 0.23 | 0.30 | 0.33 | ||
| Post | 126.4 | ± | 20.7 | 124.2 | ± | 16.1 | ||||||||
| Effect size | 0.1 | 0.5 | ||||||||||||
| Asparagine | (nmol/mL) | Pre | 59.8 | ± | 7.8 | 59.8 | ± | 8.9 | 0.06 | 0.36 | 0.27 | 0.36 | ||
| Post | 59.0 | ± | 10.6 | 57.1 | ± | 10.1 | ||||||||
| Effect size | 0.1 | 0.3 | ||||||||||||
| Glutamic acid | (nmol/mL) | Pre | 34.3 | ± | 7.1 | 35.4 | ± | 5.3 | <0.01 | 0.31 | 0.80 | 0.35 | ||
| Post | 41.6 | ± | 10.1 | 48.1 | ± | 17.2 | ||||||||
| Effect size | 0.8 | 1.0 | ||||||||||||
| Glutamine | (nmol/mL) | Pre | 636.6 | ± | 58.9 | 632.7 | ± | 75.4 | <0.01 | 0.81 | <0.01 | 0.83 | ||
| Post | 690.5 | ± | 74.1 | 679.3 | ± | 56.2 | ||||||||
| Effect size | 0.8 | 0.7 | ||||||||||||
| Glycine | (nmol/mL) | Pre | 230.5 | ± | 43.7 | 241.6 | ± | 59.1 | <0.01 | 0.08 | 0.54 | 0.10 | ||
| Post | 259.8 | ± | 58.6 | 303.2 | ± | 77.3 | ||||||||
| Effect size | 0.6 | 0.9 | ||||||||||||
| Alanine | (nmol/mL) | Pre | 313.7 | ± | 43.1 | 319.6 | ± | 75.1 | <0.01 | 0.84 | 0.15 | 0.87 | ||
| Post | 364.0 | ± | 83.1 | 364.7 | ± | 75.3 | ||||||||
| Effect size | 0.8 | 0.6 | ||||||||||||
| Cystine | (nmol/mL) | Pre | 50.1 | ± | 8.1 | 48.4 | ± | 7.2 | <0.01 | 0.13 | <0.01 | 0.15 | ||
| Post | 52.4 | ± | 4.6 | 55.4 | ± | 8.5 | ||||||||
| Effect size | 0.3 | 0.9 | ||||||||||||
| Methionine | (nmol/mL) | Pre | 22.8 | ± | 2.2 | 23.1 | ± | 3.2 | <0.01 | 0.24 | 0.11 | 0.27 | ||
| Post | 26.8 | ± | 3.5 | 25.7 | ± | 3.5 | ||||||||
| Effect size | 1.4 | 0.8 | ||||||||||||
| Tyrosine | (nmol/mL) | Pre | 57.0 | ± | 11.5 | 59.6 | ± | 12.5 | <0.01 | 0.02 | Ex + CIT·LEU, Ex + Placebo: Pre < Post | 0.01 | 0.03 | Ex + CIT·LEU, Ex + Placebo: Pre < Post |
| Post | 70.5 | ± | 12.6 | 65.6 | ± | 11.3 | ||||||||
| Effect size | 1.1 | 0.5 | ||||||||||||
| Phenylalanine | (nmol/mL) | Pre | 58.2 | ± | 7.6 | 58.9 | ± | 6.2 | 0.43 | 0.04 | Ex + CIT·LEU: Pre < Post | 0.02 | 0.03 | Ex + CIT·LEU: Pre < Post |
| Post | 62.2 | ± | 7.5 | 57.6 | ± | 5.8 | ||||||||
| Effect size | 0.5 | 0.2 | ||||||||||||
| Histidine | (nmol/mL) | Pre | 85.0 | ± | 7.2 | 83.7 | ± | 7.7 | <0.01 | 0.19 | 0.37 | 0.18 | ||
| Post | 91.6 | ± | 11.0 | 87.1 | ± | 6.3 | ||||||||
| Effect size | 0.7 | 0.5 | ||||||||||||
| Lysine | (nmol/mL) | Pre | 199.5 | ± | 12.6 | 188.0 | ± | 18.7 | <0.01 | 0.25 | 0.08 | 0.47 | ||
| Post | 210.2 | ± | 18.0 | 208.4 | ± | 24.6 | ||||||||
| Effect size | 0.7 | 0.9 | ||||||||||||
| Tryptophan | (nmol/mL) | Pre | 45.8 | ± | 7.7 | 46.5 | ± | 6.1 | 0.11 | 0.13 | <0.01 | 0.06 | ||
| Post | 50.1 | ± | 3.8 | 46.8 | ± | 5.6 | ||||||||
| Effect size | 0.7 | 0.1 | ||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Isoda, H.; Okura, T. Effect of Citrulline and Leucine Intake with Exercises on Body Composition, Physical Activity, and Amino Acid Concentration in Older Women: A Randomized Double-Blind Placebo-Controlled Study. Foods 2021, 10, 3117. https://doi.org/10.3390/foods10123117
Kim M, Isoda H, Okura T. Effect of Citrulline and Leucine Intake with Exercises on Body Composition, Physical Activity, and Amino Acid Concentration in Older Women: A Randomized Double-Blind Placebo-Controlled Study. Foods. 2021; 10(12):3117. https://doi.org/10.3390/foods10123117
Chicago/Turabian StyleKim, Mijin, Hiroko Isoda, and Tomohiro Okura. 2021. "Effect of Citrulline and Leucine Intake with Exercises on Body Composition, Physical Activity, and Amino Acid Concentration in Older Women: A Randomized Double-Blind Placebo-Controlled Study" Foods 10, no. 12: 3117. https://doi.org/10.3390/foods10123117
APA StyleKim, M., Isoda, H., & Okura, T. (2021). Effect of Citrulline and Leucine Intake with Exercises on Body Composition, Physical Activity, and Amino Acid Concentration in Older Women: A Randomized Double-Blind Placebo-Controlled Study. Foods, 10(12), 3117. https://doi.org/10.3390/foods10123117