
Polish Consumers’ Understanding of Different Front-of-Package Food Labels: A Randomized Experiment

 , ,
, ,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participant Recruitment
2.2. Intervention
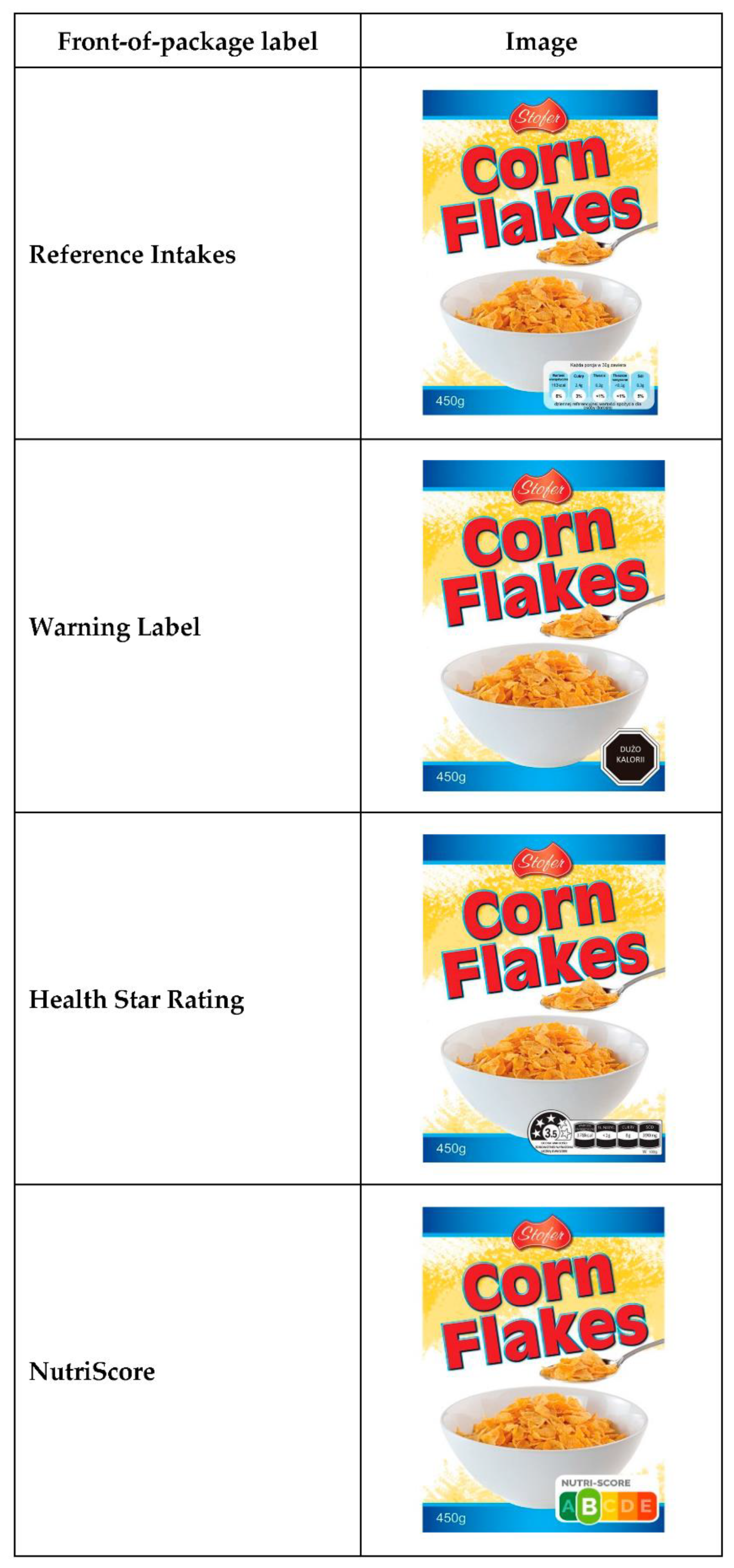
2.3. Description of the FoPL Tested in the Trial
2.4. Statistical Analysis
3. Results
3.1. Sample Description
3.2. Effect of FoPL Condition on Product Rankings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jarosz, M.; Rychlik, E.; Sekuła, W. Dietary changes, tobacco smoking and life expectancy in Poland in the years 1950–2012. Pol. J. Hum. Nutr. Metab. 2016, 43, 152–170. [Google Scholar]
- Olszanecka-Glinianowicz, M.; Chudek, J. The level of health education in the Polish population. Ann. Agric. Environ. Med. 2013, 20, 559–565. [Google Scholar] [PubMed]
- OECD/European Observatory on Health Systems and Policies. Poland: Country Health Profile 2019, State of Health in the EU; OECD Publishing: Paris, France; European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- Rychlik, E.; Jarosz, M.; Wolnicka, K.; Taraszewska, A.; Jaczewska-Schuetz, J.; Stoś, K.; Kłys, W. The problem of overweight and obesity in Poland. Pol. J. Hum. Nutr. Metab. 2019, 46, 338–349. [Google Scholar]
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics; European Heart Network: Brussels, Belgium, 2017. [Google Scholar]
- Kelly, B.; Jewell, J. What Is the Evidence on the Policy Specifications, Development Processes and Effectiveness of Existing Front-of-Pack Food Labelling Policies in the WHO European Region? Health Evidence Network (HEN) Synthesis Report 61; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- World Cancer Research Fund International. Building Momentum: Lessons on Implementing a Robust Front-of-Pack Food Label; WCRF International: London, UK, 2019. [Google Scholar]
- European Commission. Report from the Commission to the European Parliament and the Council Regarding the Use of Additional Forms of Expression and Presentation of the Nutrition Declaration; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Kanter, R.; Vanderlee, L.; Vandevijvere, S. Front-of-package nutrition labelling policy: Global progress and future directions. Public Health Nutr. 2018, 21, 1399–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.; Brown, M.K.; Tan, M.; MacGregor, G.A.; Webster, J.; Campbell, N.R.C.; Trieu, K.; Ni Mhurchu, C.; Cobb, L.K.; He, F.J. Impact of color-coded and warning nutrition labelling schemes: A systematic review and network meta-analysis. PLoS Med. 2021, 18, e1003765. [Google Scholar] [CrossRef] [PubMed]
- Roodenburg, A.J.; Popkin, B.M.; Seidell, J.C. Development of international criteria for a front of package food labelling system: The International Choices Programme. Eur. J. Clin. Nutr. 2011, 65, 1190–1200. [Google Scholar] [CrossRef]
- Ministry of Health Welfare and Sport, Government of the Netherlands. Toespraak van Staatssecretaris Blokhuis bij Persbriefing over het Voedselkeuzelogo [Speech by State Secretary Blokhuis at Press Briefing on the Food Choice Logo]; Government of the Netherlands: The Hague, The Netherlands, 2019.
- Grunert, K.G.; Fernández-Celemín, L.; Wills, J.M.; Bonsmann, S.S.G.; Nureeva, L. Use and understanding of nutrition information on food labels in six European countries. Z. Gesundh. Wiss. 2010, 18, 261–277. [Google Scholar] [CrossRef] [Green Version]
- Egnell, M.; Talati, Z.; Hercberg, S.; Pettigrew, S.; Julia, C. Objective understanding of front-of-package nutrition labels: An international comparative experimental study across 12 countries. Nutrients 2018, 10, 1542. [Google Scholar] [CrossRef] [Green Version]
- Egnell, M.; Talati, Z.; Galan, P.; Andreeva, V.A.; Vandevijvere, S.; Gombaud, M.; Dréano-Trécant, L.; Hercberg, S.; Pettigrew, S.; Julia, C. Objective understanding of the NutriScore front-of-pack label by European consumers and its effect on food choices: An online experimental study. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 146. [Google Scholar] [CrossRef]
- United Nations University, World Institute for Development Economics Research (UNU-WIDER). World Income Inequality Database, Version WIID-4; UNU-WIDER: Helsinki, Finland, 2018. [Google Scholar]
- Packer, J.; Russell, S.; Ridout, D.; Hope, S.; Conolly, A.; Jessop, C.; Robinson, O.; Stoffel, S.; Viner, R.; Croker, H. Assessing the effectiveness of front of pack labels: Findings from an online randomised-controlled experiment in a representative British sample. Nutrients 2021, 13, 900. [Google Scholar] [CrossRef]
- Rahkovsky, I.; Lin, B.H.; Lin, C.T.J.; Lee, J.Y. Effects of the Guiding Stars Program on purchases of ready-to-eat cereals with different nutritional attributes. Food Policy 2013, 43, 100–107. [Google Scholar] [CrossRef]
- Potvin Kent, M.; Pauze, E. The frequency and healthfulness of food and beverages advertised on adolescents’ preferred Web sites in Canada. J. Adolesc. Health 2018, 63, 102–107. [Google Scholar] [CrossRef]
- Powell, L.M.; Wada, R.; Khan, T.; Emery, S.L. Food and beverage television advertising exposure and youth consumption, body mass index and adiposity outcomes. Can. J. Econ. 2017, 50, 345–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talati, Z.; Egnell, M.; Hercberg, S.; Julia, C.; Pettigrew, S. Food choice under five front-of-package nutrition label conditions: An experimental study across 12 countries. Am. J. Public Health 2019, 109, 1770–1775. [Google Scholar] [CrossRef] [PubMed]
- Rayner, M.; Scarborough, P.; Boxer, A.; Stockley, L. Nutrient Profiles: Development of Final Model; Final Report; British Heart Foundation Health Promotion Research Group, Department of Public Health, University of Oxford: Oxford, UK, 2005. [Google Scholar]
- Ministère des Solidarités et de la Santé. Étiquetage Nutritionnel: Signature de L’arrêté Recommandant L’utilisation de NutriScore. [Food Labeling: Signing of the Decree Recommending the Use of NutriScore]; Ministère des Solidarités et de la Santé: Paris, France, 2017.
- Julia, C.; Touvier, M.; Méjean, C.; Ducrot, P.; Péneau, S.; Hercberg, S.; Kesse-Guyot, E. Development and validation of an individual dietary index based on the British Food Standard Agency nutrient profiling system in a French context. J. Nutr. 2014, 144, 2009–2017. [Google Scholar] [CrossRef] [Green Version]
- FoodDrinkEurope. Reference Intakes. A FoodDrinkEurope Initiative; FoodDrinkEurope: Brussels, Belgium, 2014. [Google Scholar]
- Malam, S.; Clegg, S.; Kirwan, S.; McGinigal, S.; BMRB Social Research. Comprehension and Use of UK Nutrition Signpost Labelling Schemes. A Report for the FSA; Food Standards Agency: London, UK, 2009. [Google Scholar]
- Department of Health, Food Standards Agency. Guide to Creating a Front of Pack (FoP) Nutrition Label for Pre-Packed Products Sold through Retail Outlets; Department of Health: London, UK, 2016.
- Reyes, M.; Garmendia, M.L.; Olivares, S.; Aqueveque, C.; Zacarías, I.; Corvalán, C. Development of the Chilean front-of-package food warning label. BMC Public Health 2019, 19, 906. [Google Scholar] [CrossRef] [Green Version]
- Andreeva, V.A.; Egnell, M.; Handjieva-Darlenska, T.; Talati, Z.; Touvier, M.; Galan, P.; Hercberg, S.; Pettigrew, S.; Julia, C. Bulgarian consumers’ objective understanding of front-of-package nutrition labels: A comparative, randomized study. Arch. Public Health 2020, 78, 35. [Google Scholar] [CrossRef] [PubMed]
- Aschemann-Witzel, J.; Grunert, K.G.; van Trijp, H.C.; Bialkova, S.; Raats, M.; Hodgkins, C.; Wąsowicz, G.; Koenigstorfer, J. Effects of nutrition label format and product assortment on the healthfulness of food choice. Appetite 2013, 71, 63–74. [Google Scholar] [CrossRef]
- Raats, M.; Hieke, S.; Jola, C.; Hodgkins, C.; Kennedy, J.; Wills, J. Reference amounts utilised in front of package nutrition labelling; impact on product healthfulness evaluations. Eur. J. Clin. Nutr. 2015, 69, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Feunekes, G.I.; Gortemaker, I.A.; Willems, A.A.; Lion, R.; Kommer, M.V.D. Front-of-pack nutrition labelling: Testing effectiveness of different nutrition labelling formats front-of-pack in four European countries. Appetite 2008, 50, 57–70. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, Y.; Gu, Y.; Wang, S.; Chen, H. Red for “Stop”: “Traffic-Light” nutrition labels decrease unhealthy food choices by increasing activity and connectivity in the frontal lobe. Nutrients 2020, 12, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasiljevic, M.; Pechey, R.; Marteau, T.M. Making food labels social: The impact of colour of nutritional labels and injunctive norms on perceptions and choice of snack foods. Appetite 2015, 91, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health. Conducting research in 2017 and 2018 on the development and introduction of a friendly food labelling system by a simple message regarding the content of individual nutrients in food using knowledge of solutions developed so far. In Report Summary: National Health Programme NZP Task 315; Ministry of Health: Warsaw, Poland, 2020. Available online: https://www.gov.pl/web/zdrowie (accessed on 9 November 2021).
- Dubois, P.; Albuquerque, P.; Allais, O.; Bonnet, C.; Bertail, P.; Combris, P.; Lahlou, S.; Rigal, N.; Ruffieux, B.; Chandon, P. Effects of front-of-pack labels on the nutritional quality of supermarket food purchases: Evidence from a large-scale randomized controlled trial. J. Acad. Mark. Sci. 2020, 49, 119–138. [Google Scholar] [CrossRef] [Green Version]
- Bix, L.; Sundar, R.P.; Bello, N.M.; Peltier, C.; Weatherspoon, L.J.; Becker, M.W. To see or not to see: Do front of pack nutrition labels affect attention to overall nutrition information? PLoS ONE 2015, 10, e0139732. [Google Scholar]
- Gregori, D.; Ballali, S.; Vögele, C.; Gafare, C.E.; Stefanini, G.; Widhalm, K. Evaluating food front-of-pack labelling: A pan-European survey on consumers’ attitudes toward food labelling. Int. J. Food Sci. Nutr. 2014, 65, 177–186. [Google Scholar] [CrossRef]
- Waśkiewicz, A.; Szcześniewska, D.; Szostak-Węgierek, D.; Kwaśniewska, M.; Pająk, A.; Stepaniak, U.; Kozakiewicz, K.; Tykarski, A.; Zdrojewski, T.; Zujko, M.; et al. Are dietary habits of the Polish population consistent with the recommendations for prevention of cardiovascular disease?—WOBASZ II project. Kardiol. Pol. 2016, 74, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Bonsmann, S.S.G.; Marandola, G.; Ciriolo, E.; van Bavel, R.; Wollgast, J. Front-of-Pack Nutrition Labelling Schemes: A Comprehensive Review; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- Vyth, E.L.; Steenhuis, I.; Mallant, S.F.; Mol, Z.L.; Brug, J.; Temminghoff, M.; Feunekes, G.I.; Jansen, L.; Verhagen, H.; Seidell, J.C. A front-of-pack nutrition logo: A quantitative and qualitative process evaluation in the Netherlands. J. Health Commun. 2009, 14, 631–645. [Google Scholar] [CrossRef]
- Bryla, P. Who reads food labels? Selected predictors of consumer interest in front-of-package and back-of-package labels during and after the purchase. Nutrients 2020, 12, 2605. [Google Scholar] [CrossRef]
- Jezewska-Zychowicz, M.; Plichta, M.; Drywien, M.E.; Hamulka, J. Food neophobia among adults: Differences in dietary patterns, food choice motives, and food labels reading in Poles. Nutrients 2021, 13, 1590. [Google Scholar] [CrossRef]
- Talati, Z.; Egnell, M.; Hercberg, S.; Julia, C.; Pettigrew, S. Consumers’ perceptions of five front-of-package nutrition labels: An experimental study across 12 countries. Nutrients 2019, 11, 1934. [Google Scholar] [CrossRef] [Green Version]
- Vargas-Meza, J.; Jáuregui, A.; Contreras-Manzano, A.; Nieto, C.; Barquera, S. Acceptability and understanding of front-of-pack nutritional labels: An experimental study in Mexican consumers. BMC Public Health 2019, 19, 1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soderlund, F.; Eyles, H.; Mhurchu, C.N. Stars versus warnings: Comparison of the Australasian Health Star Rating nutrition labelling system with Chilean Warning labels. Aust. N. Z. J. Public Health 2020, 44, 28–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa, T.; Fierro, C.; Reyes, M.; Dillman Carpentier, F.R.; Taillie, L.S.; Corvalan, C. Responses to the Chilean law of food labeling and advertising: Exploring knowledge, perceptions and behaviors of mothers of young children. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Nutrition Labelling; European Commission: Brussels, Belgium, 2020. [Google Scholar]


{kind=link}
{kind=link}
| Full Sample (N = 1159) | Ages 18–30 years (N = 390) | Ages 31–50 years (N = 389) | Ages 51–89 years (N = 380) | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| Randomization group | 0.97 | ||||||||
| Health Star Rating | 232 | (20.0) | 77 | (19.7) | 79 | (20.3) | 76 | (20.0) | |
| Multiple Traffic Lights | 231 | (19.9) | 79 | (20.3) | 71 | (18.2) | 81 | (21.3) | |
| NutriScore | 232 | (20.0) | 80 | (20.5) | 83 | (21.3) | 69 | (18.2) | |
| Reference Intakes | 232 | (20.0) | 76 | (19.5) | 78 | (20.1) | 78 | (20.5) | |
| Warning Label | 232 | (20.0) | 78 | (20.0) | 78 | (20.1) | 76 | (20.0) | |
| Mean age, years (SD) | 40.9 | (15.4) | 24.9 | (3.5) | 38.3 | (5.4) | 60.1 | (6.6) | |
| Sex | <0.0001 | ||||||||
| Male | 579 | (50.0) | 123 | (31.5) | 206 | (53.0) | 250 | (65.8) | |
| Female | 580 | (50.0) | 267 | (68.5) | 183 | (47.0) | 130 | (34.2) | |
| Education | <0.0001 | ||||||||
| Up to high school | 494 | (42.6) | 161 | (41.3) | 148 | (38.1) | 185 | (48.7) | |
| Trade certification | 122 | (10.5) | 16 | (4.1) | 55 | (14.1) | 51 | (13.4) | |
| Undergraduate level | 192 | (16.6) | 105 | (26.9) | 58 | (14.9) | 29 | (7.6) | |
| Graduate level | 351 | (30.3) | 108 | (27.7) | 128 | (32.9) | 115 | (30.3) | |
| Household income | <0.0001 | ||||||||
| Low | 375 | (32.4) | 103 | (26.4) | 170 | (43.7) | 102 | (26.8) | |
| Medium | 397 | (34.2) | 185 | (47.4) | 127 | (32.7) | 85 | (22.4) | |
| High | 387 | (33.4) | 102 | (26.2) | 92 | (23.6) | 193 | (50.8) | |
| Children ≤ 14 years in household | <0.0001 | ||||||||
| No | 648 | (55.9) | 185 | (47.4) | 148 | (38.1) | 315 | (82.9) | |
| Yes | 511 | (44.1) | 205 | (52.6) | 241 | (61.9) | 65 | (17.1) | |
| Grocery shopping responsibility | 0.005 | ||||||||
| No | 35 | (3.0) | 11 | (2.8) | 16 | (4.1) | 8 | (2.1) | |
| Shared | 291 | (25.1) | 84 | (21.5) | 87 | (22.4) | 120 | (31.6) | |
| Yes | 833 | (71.9) | 295 | (75.7) | 286 | (73.5) | 252 | (66.3) | |
| Knowledge about nutrition | 0.02 | ||||||||
| Very limited | 168 | (14.5) | 48 | (12.3) | 68 | (17.5) | 52 | (13.7) | |
| Average level | 852 | (73.5) | 284 | (72.8) | 289 | (74.3) | 279 | (73.4) | |
| High level | 139 | (12.0) | 58 | (14.9) | 32 | (8.2) | 49 | (12.9) | |
| Self-assessed diet quality | 0.68 | ||||||||
| Mostly or very unhealthy | 256 | (22.1) | 81 | (20.8) | 91 | (23.4) | 84 | (22.1) | |
| Mostly or very healthy | 903 | (77.9) | 309 | (79.2) | 298 | (76.6) | 296 | (77.9) | |
| Food Category | Health Star Rating | Multiple Traffic Lights | NutriScore | Warning Label | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | (95% CI) | p | OR | (95% CI) | p | OR | (95% CI) | p | OR | (95% CI) | p | |
| All categories | 1.25 | (0.87–1.81) | 0.23 | 0.96 | (0.66–1.39) | 0.83 | 2.02 | (1.41–2.91) | 0.0001 | 1.61 | (1.12–2.32) | 0.01 |
| Cereals | 1.62 | (1.01–2.59) | 0.05 | 1.26 | (0.78–2.02) | 0.34 | 1.89 | (1.18–3.02) | 0.008 | 1.51 | (0.94–2.44) | 0.09 |
| Cakes | 1.83 | (1.14–2.93) | 0.01 | 1.38 | (0.86–2.23) | 0.19 | 2.85 | (1.79–4.53) | <0.0001 | 2.39 | (1.49–3.81) | 0.0003 |
| Pizzas | 0.89 | (0.56–1.39) | 0.60 | 0.68 | (0.43–1.07) | 0.09 | 1.59 | (1.02–2.46) | 0.04 | 1.22 | (0.78–1.91) | 0.37 |
| Food Category | Health Star Rating | Multiple Traffic Lights | NutriScore | Warning Label | ||||
|---|---|---|---|---|---|---|---|---|
| OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | |
| Ages 18–30 years | ||||||||
| All categories | 1.51 | (0.79–2.90) | 0.94 | (0.49–1.80) | 3.88 | (2.04–7.36) | 2.12 | (1.11–4.06) |
| Breakfast cereals | 2.91 | (1.27–6.68) | 1.34 | (0.58–3.14) | 3.21 | (1.40–7.33) | 2.11 | (0.90–4.96) |
| Cakes | 2.29 | (0.99–5.28) | 1.26 | (0.54–2.93) | 6.88 | (3.05–15.51) | 5.07 | (2.20–11.66) |
| Pizzas | 0.97 | (0.44–2.14) | 0.70 | (0.32–1.55) | 1.92 | (0.90–4.08) | 0.90 | (0.40–1.99) |
| Ages 31–50 years | ||||||||
| All categories | 1.07 | (0.57–2.01) | 0.95 | (0.49–1.82) | 1.60 | (0.86–2.98) | 1.99 | (1.06–3.73) |
| Breakfast cereals | 1.23 | (0.55–2.76) | 2.29 | (0.57–2.93) | 1.48 | (0.67–3.28) | 1.94 | (0.88–4.30) |
| Cakes | 1.74 | (0.75–4.05) | 1.65 | (0.69–3.97) | 2.00 | (0.87–4.60) | 2.52 | (1.09–5.83) |
| Pizzas | 0.75 | (0.33–1.68) | 0.58 | (0.25–1.32) | 2.02 | (0.95–4.34) | 1.62 | (0.74–3.56) |
| Ages 51–89 years | ||||||||
| All categories | 1.18 | (0.61–2.25) | 1.03 | (0.54–1.94) | 1.31 | (0.68–2.53) | 1.05 | (0.55–2.02) |
| Breakfast cereals | 1.18 | (0.50–2.78) | 1.31 | (0.57–3.04) | 1.57 | (0.66–3.76) | 0.85 | (0.35–2.09) |
| Cakes | 1.75 | (0.76–4.01) | 1.31 | (0.58–2.30) | 1.66 | (0.72–3.85) | 1.38 | (0.59–3.20) |
| Pizzas | 0.77 | (0.35–1.70) | 0.76 | (0.35–1.67) | 0.90 | (0.41–1.97) | 1.06 | (0.48–2.32) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreeva, V.A.; Egnell, M.; Stoś, K.; Przygoda, B.; Talati, Z.; Touvier, M.; Galan, P.; Hercberg, S.; Pettigrew, S.; Julia, C. Polish Consumers’ Understanding of Different Front-of-Package Food Labels: A Randomized Experiment. Foods 2022, 11, 134. https://doi.org/10.3390/foods11010134
Andreeva VA, Egnell M, Stoś K, Przygoda B, Talati Z, Touvier M, Galan P, Hercberg S, Pettigrew S, Julia C. Polish Consumers’ Understanding of Different Front-of-Package Food Labels: A Randomized Experiment. Foods. 2022; 11(1):134. https://doi.org/10.3390/foods11010134
Chicago/Turabian StyleAndreeva, Valentina A., Manon Egnell, Katarzyna Stoś, Beata Przygoda, Zenobia Talati, Mathilde Touvier, Pilar Galan, Serge Hercberg, Simone Pettigrew, and Chantal Julia. 2022. "Polish Consumers’ Understanding of Different Front-of-Package Food Labels: A Randomized Experiment" Foods 11, no. 1: 134. https://doi.org/10.3390/foods11010134
APA StyleAndreeva, V. A., Egnell, M., Stoś, K., Przygoda, B., Talati, Z., Touvier, M., Galan, P., Hercberg, S., Pettigrew, S., & Julia, C. (2022). Polish Consumers’ Understanding of Different Front-of-Package Food Labels: A Randomized Experiment. Foods, 11(1), 134. https://doi.org/10.3390/foods11010134