
The Healthy Food Environment Policy Index in Poland: Implementation Gaps and Actions for Improvement

 , , , , , and
, , , , , and
Abstract
1. Introduction
- To depict the overall strength of healthy food environment policies in Poland and to identify basic implementation gaps in terms of policies and infrastructure support.
- To identify and prioritise healthy food environment policies in Poland, taking into account their importance, achievability and equity.
2. Materials and Methods
2.1. Study Procedure
2.1.1. Step 1: Reviewing the Tool and Its Indicators
2.1.2. Step 2: The Catalogue of International Best Practices
2.1.3. Step 3: National Evidence Document
2.1.4. Step 4: Online Rating Survey
2.1.5. Step 5: Identification and Prioritisation of Actions to Improve the Food Environment
2.2. Data Analysis
3. Results
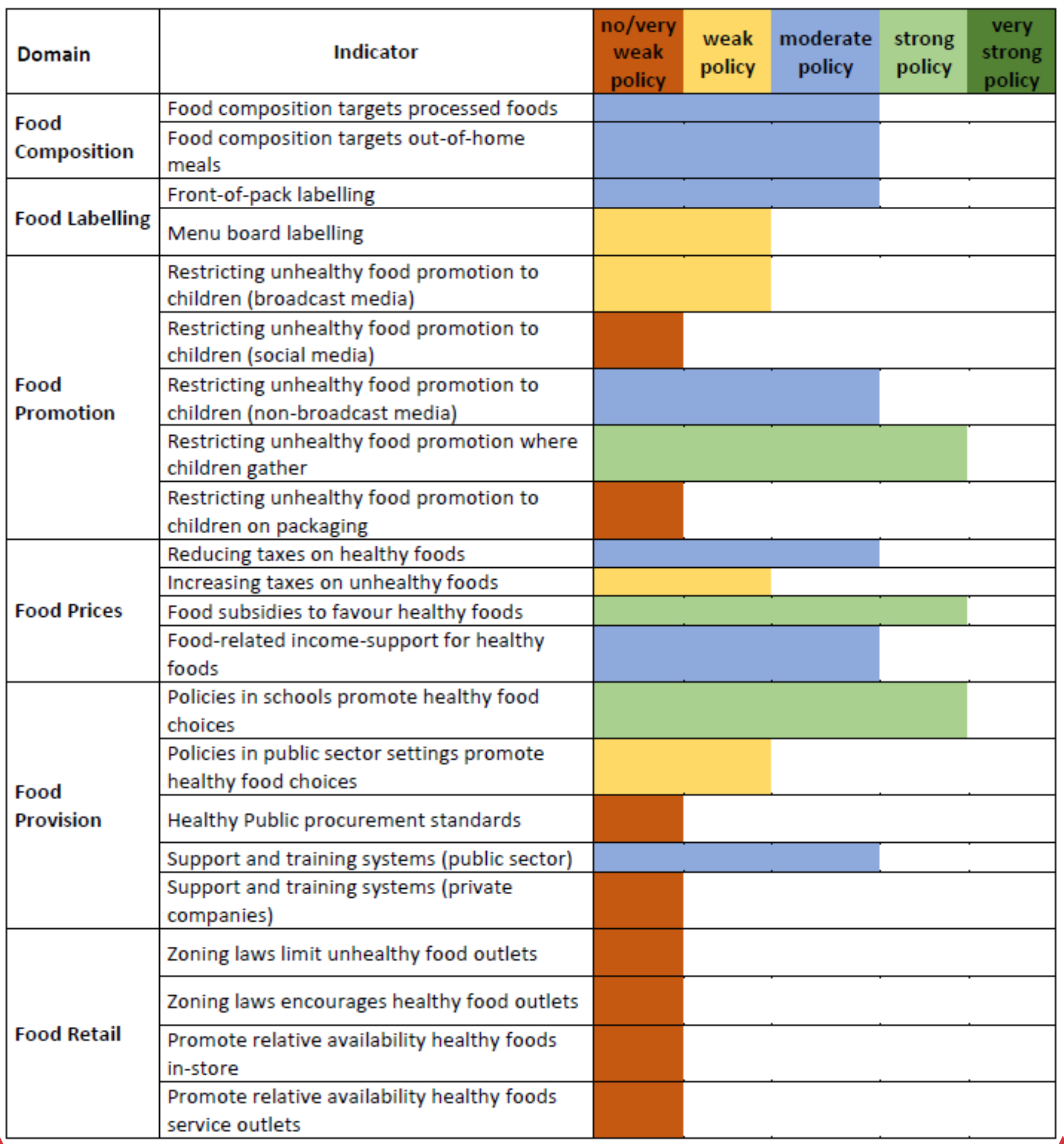
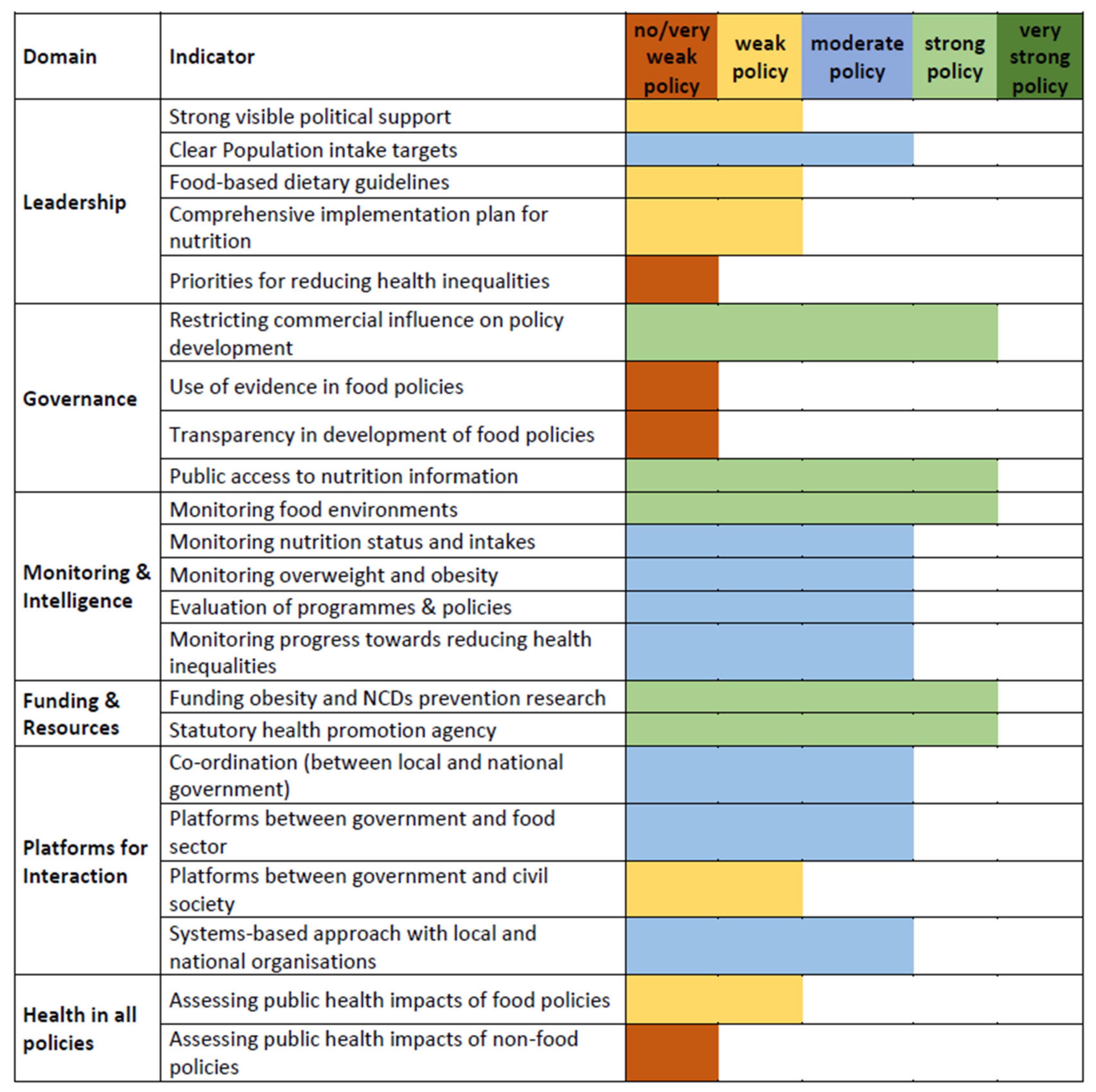
3.1. Evaluation of the Extent of Implementation of Healthy Food Environment Policies in Poland
3.1.1. Overall Assessment of the Policy- and Infrastructure-Related Domains
3.1.2. Assessment of the Impact on Socio-Economic Inequalities
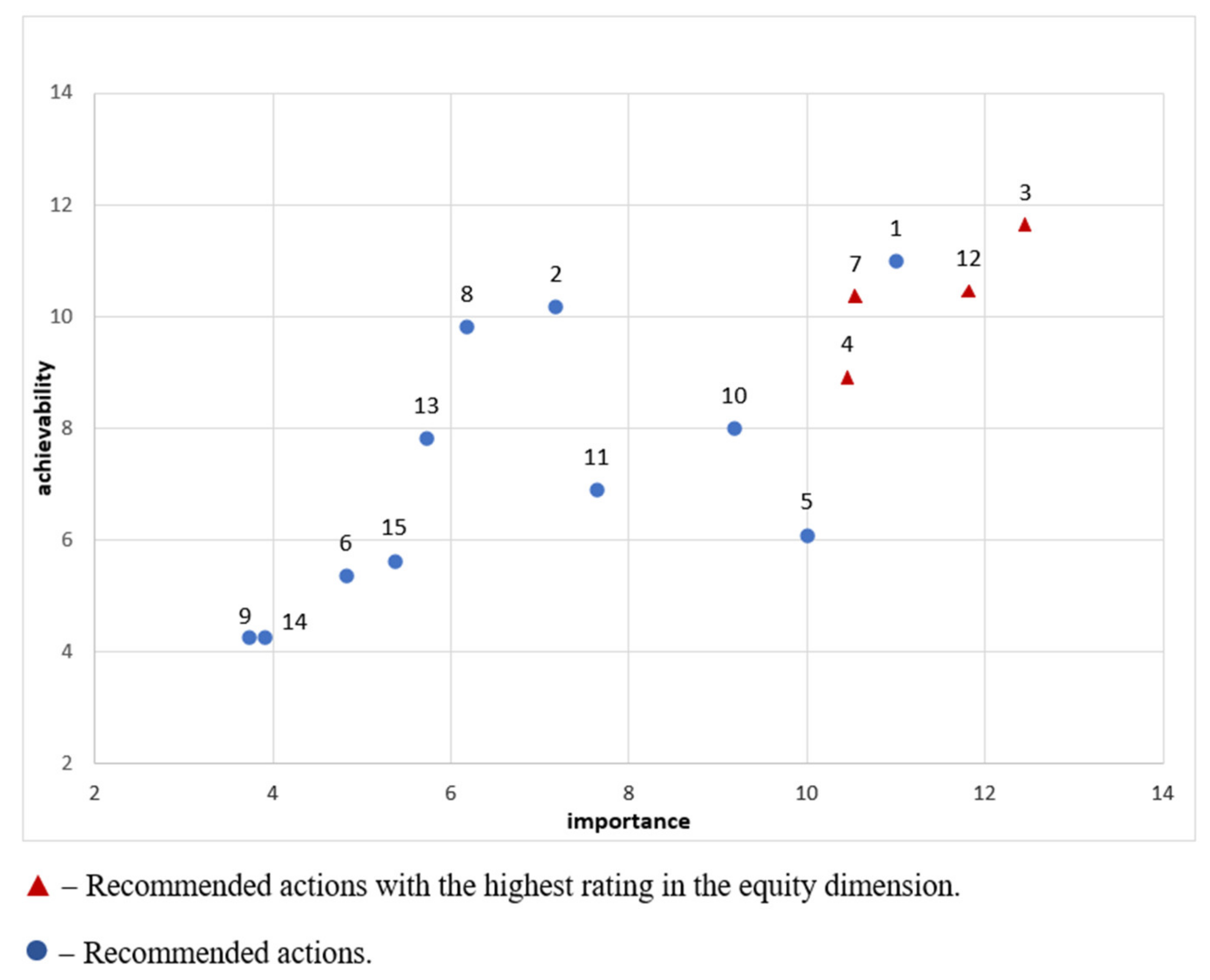
3.2. Identification and Prioritisation of Actions to Improve Poland’s Healthy Food Environment
3.2.1. Policy Actions
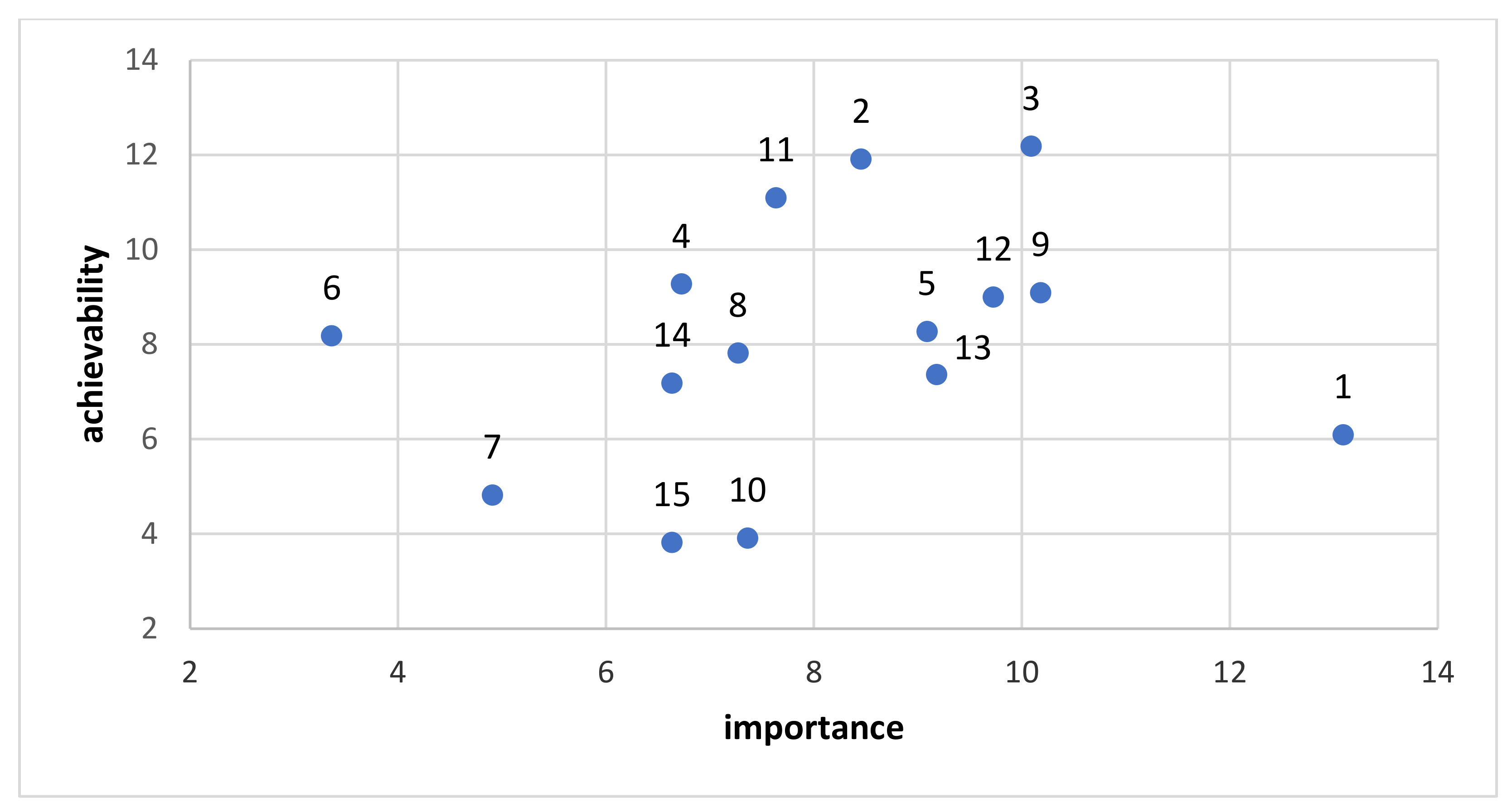
3.2.2. Infrastructure Support Actions
4. Discussion
5. Conclusions
- The healthy food environment in Poland has been assessed as being very weak or weak in most cases of the indicators related to policies, with only three indicators being assessed as strong policies. The largest gaps were identified in the food retail domain, along with individual indicators related to other domains, namely, restricting unhealthy food promotion to children on social media, restricting unhealthy food promotion to children on packaging, healthy public procurement standards and support and training systems in private companies. Infrastructure was assessed as being slightly better, with more indicators being assessed as moderate policies and four indicators being assessed as strong policies. The main gaps identified here are the political support related to priorities for reducing health inequalities, the use of evidence in food policies, transparency in the development of food policies and assessing the public health impact of non-food policies.
- Taking into account the combined dimensions of importance, achievability and equity for policies and importance and achievability for infrastructure, the most prioritised actions identified to be implemented to improve the Polish health food environment are the implementation of a clear and simple labelling system for food products, including information on salt/sugar/trans fats, and the implementation of a system of training on healthy eating rules targeting people responsible for feeding children. These constitute the basic recommendations regarding food policy actions to be implemented by the public authorities in Poland.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pineda, E.; Sanchez-Romero, L.M.; Brown, M.; Jaccard, A.; Jewell, J.; Galea, G.; Webber, L.; Breda, J. Forecasting Future Trends in Obesity across Europe: The Value of Improving Surveillance. Obes. Facts 2018, 11, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Główny Urząd Statystyczny Stan Zdrowia Ludności Polski w 2014 Roku. Available online: https://stat.gov.pl/obszary-tematyczne/zdrowie/zdrowie/stan-zdrowia-ludnosci-polski-w-2014-r-,6,6.html (accessed on 18 February 2021).
- NFZ Cukier, Otyłość-Konsekwencje. Przegląd Literatury, Szacunki dla Polski. Available online: https://www.gov.pl/attachment/2b2ff239-3745-442a-b8bc-d12a69f25645 (accessed on 11 March 2021).
- Towpik, I.; Walicka, M.; Marcinkowska, K.; Lisicka, I.; Raczyńska, M.; Wierzba, W.; Strojek, K.; Ryś, P.; Wajda-Cuszlag, M.; Franek, E. Epidemiology of diabetes in Poland in 2014–2017. Clin. Diabetol. 2020, 9, 279–285. [Google Scholar] [CrossRef]
- Pająk, A.; Szafraniec, K.; Polak, M.; Polakowska, M.; Kozela, M.; Piotrowski, W.; Kwaśniewska, M.; Podolecka, E.; Kozakiewicz, K.; Tykarski, A.; et al. Changes in the prevalence, treatment, and control of hypercholesterolemia and other dyslipidemias over 10 years in Poland: The WOBASZ study. Pol. Arch. Med. Wewn. 2016, 126, 642–652. [Google Scholar] [CrossRef] [PubMed][Green Version]
- NFZ Nadciśnienie Tętnicze. 2019. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultaktualnosci/370/7352/1/nadcisnienie-tetnicze-raport-nfz-2019-small.pdf (accessed on 15 February 2021).
- NCD-RisC. Available online: https://ncdrisc.org/country-profile.html (accessed on 3 April 2021).
- Didkowska, J.; Wojciechowska, U.; Michałek, I.; Olasek, P.; Ciuba, A. Cancer in Poland in 2018; Center of Oncology-Maria Skłodowska-Curie Institute: Warsaw, Poland, 2020; Available online: http://onkologia.org.pl/wp-content/uploads/Nowotwory_2018.pdf (accessed on 3 April 2021).
- Godlewski, D.; Adamczak, M.; Wojtyś, P. Experiences of cancer patients in Poland throughout diagnosis and treatment. Eur. J. Cancer Care 2016, 26, e12436. [Google Scholar] [CrossRef]
- Gruchelski, M.; Niemczyk, J. Konieczność zmian w polskiej polityce żywnościowej. Postępy Tech. Przetwórstwa Spożywczego 2008, 2, 98–103. [Google Scholar]
- Jarosz, M.; Rychlik, E.; Stoś, K.; Charzewska, J. Normy Żywienia dla Populacji Polski i ich Zastosowanie. Available online: https://www.pzh.gov.pl/normy-zywienia-2020/ (accessed on 5 March 2021).
- Global Nutrition Report. Available online: https://globalnutritionreport.org/resources/nutrition-profiles/europe/eastern-europe/poland/ (accessed on 11 April 2021).
- Uchwała Nr 140 Rady Ministrów z dnia 15 października 2018 r. w Sprawie Ustanowienia Wieloletniego Rządowego Programu Posiłek w Szkole i w Domu na Lata 2019–2023 Program Posiłek w Szkole i w Domu na Lata 2019–2023 (M.P. 2018 poz. 1007). Available online: https://monitorpolski.gov.pl/M2018000100701.pdf (accessed on 26 February 2022).
- Rozporządzenie Ministra Zdrowia z dnia 26 lipca 2016 roku w Sprawie Grup Środków Spożywczych Przeznaczonych do Sprzedaży Dzieciom w Jednostkach Systemu Oświaty Oraz Wymagań, Jakie Muszą Spełnić Środki Spożywcze Stosowane w Ramach Żywienia Zbiorowego Dzieci i Młodzieży w Tych Jednostkach (Dz.U. z 2016 r. poz. 1154). Available online: https://dziennikustaw.gov.pl/D2016000115401.pdf (accessed on 7 February 2021).
- Euro WHO. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/country-work/poland (accessed on 11 March 2021).
- Hébert, J.R.; Hurley, T.G.; Steck, S.E.; Miller, D.R.; Tabung, F.K.; Peterson, K.E.; Kushi, L.H.; Frongillo, E.A. Considering the value of dietary assessment data in informing nutrition-related health policy. Adv. Nutr. 2014, 5, 447–455. [Google Scholar] [CrossRef]
- Swinburn, B.; Vandevijvere, S.; Kraak, V.; Sacks, G.; Snowdon, W.; Hawkes, C.; Barquera, S.; Friel, S.; Kelly, B.; Kumanyika, S.; et al. Monitoring public sector policies and actions. Obes. Rev. 2013, 14, 24–37. [Google Scholar] [CrossRef]
- Swinburn, B.; Sacks, G.; Vandevijvere, S.; Kumanyika, S.; Lobstein, T.; Neal, B.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; et al. Informas overview. Obes. Rev. 2013, 14, 1–12. [Google Scholar] [CrossRef]
- Vandevijvere, S.; Swinburn, B. Towards global benchmarking of food environments and policies to reduce obesity and diet-related non-communicable diseases: Design and methods for nation-wide surveys. BMJ Open 2014, 4, e005339. [Google Scholar] [CrossRef]
- Ustawa z Dnia 25 sierpnia 2006 r. o Bezpieczeństwie Żywności i Żywienia (Dz. U. z 2017 r. poz. 149). Available online: https://dziennikustaw.gov.pl/D2017000014901.pdf (accessed on 12 December 2021).
- Ustawa z dnia 21 Grudnia 2000 r. o Jakości Handlowej artykułów Rolno-Spożywczych (Dz. U. z 2017 r. poz. 2212). Available online: https://dziennikustaw.gov.pl/D2017000221201.pdf (accessed on 12 December 2021).
- Rozporządzenie Ministra Rolnictwa i Rozwoju Wsi z dnia 23 grudnia 2014 r. w Sprawie Znakowania Poszczególnych Rodzajów Środków Spożywczych (Dz. U. z 2015 r. poz. 29, z późn. zm.). Available online: https://dziennikustaw.gov.pl/D2015000002901.pdf (accessed on 5 January 2022).
- Ustawa z Dnia 21grudnia 2000r.o Jakości Handlowej Artykułów Rolno-Spożywczych (Dz. U. 2001 Nr 5 poz. 44 z późn. zm.). Available online: https://dziennikustaw.gov.pl/D2001005004401.pdf (accessed on 12 December 2021).
- Rozporządzenia Ministra Rolnictwa i Rozwoju Wsi z dnia 29 lipca 2015 r. w Sprawie Stawek Dotacji Przedmiotowych dla Różnych Podmiotów Wykonujących Zadania na rzecz Rolnictwa (Dz. U. poz. 1170, z 2016 r. poz. 1614 oraz z 2017 r. poz. 1470). Available online: https://dziennikustaw.gov.pl/D2016000161401.pdf (accessed on 5 January 2022).
- Ministerstwo Zdrowia Zarządzenie nr 2 Dyrektora Generalnego Ministerstwa Zdrowia z dnia 12 lutego 2015 r. w Sprawie Sposobu Postępowania Pracowników Ministerstwa Zdrowia wobec Działań Podejmowanych Przez Podmioty Wykonujące Zawodową Działalność Lobbingową Oraz Podmioty Wykonujące bez Wpisu do Rejestru Czynności z Zakresu Zawodowej Działalności Lobbingowej. Available online: https://www.gov.pl/attachment/2d42560d-d229-4e32-bb31-9bbb720714c8 (accessed on 22 November 2020).
- Ustawa o Dostępie do Informacji Publicznej z 6 Września 2001 (Dz.U. 2001 nr 112 poz. 1198). Available online: https://dziennikustaw.gov.pl/D2001112119801.pdf (accessed on 18 March 2022).
- Ustawą z dnia 11 Maja 2001 r. o Warunkach Zdrowotnych Żywności i Żywienia (Dz.U. 2001 nr 63 poz. 634). Available online: https://dziennikustaw.gov.pl/D2001063063401.pdf (accessed on 18 March 2022).
- Rozporządzenie Ministra Edukacji Narodowej z Dnia 24 Sierpnia 2018 r. Zmieniające Rozporządzenie w Sprawie Szczegółowego Sposobu Realizacji w Szkołach Środków Towarzyszących o Charakterze edukacyjnym, Które Służą Prawidłowej Realizacji Programu dla Szkół Oraz Upowszechniają Wśród Dzieci Zdrowe Nawyki Żywieniowe (Dz. U. z 2018 r., poz. 1670). Available online: https://dziennikustaw.gov.pl/DU/rok/2017/pozycja/1670 (accessed on 18 March 2022).
- KOWR Program dla Szkół. Available online: https://www.kowr.gov.pl/program-dla-szkol/program-dla-szkol (accessed on 3 May 2021).
- Holecki, T.; Sobczyk, K.; Syrkiewicz-Świtała, M. Wykorzystanie narzędzi social media marketingu przez polskie organizacje pozarządowe w komunikacji z otoczeniem na rzecz promocji zdrowia. Zesz. Nauk. Uniw. Szczecińskiego Probl. Zarządzania Finans. Mark. 2015, 41, 177–186. [Google Scholar] [CrossRef]
- Maksymiuk, R.A.; Jasielska, A. Polaryzacja społecznych efektów reklam komercyjnych—Analiza Mechanizmów Działania na Przykładzie Nastoletnich Odbiorców. Available online: https://repozytorium.amu.edu.pl/bitstream/10593/13624/1/SE%2033_2014_Renata_Anna_Maksymiuk_Aleksandra_Jasielska.pdf (accessed on 18 February 2021).
- Pyżalski, J. Agresja elektroniczna dzieci i młodzieży–różne wymiary zjawiska. Dziecko krzywdzone. Teoria Badania Praktyka 2009, 8, 12–26. [Google Scholar]
- Ankiel, M.; Grzybowska-Brzezińska, M. Wartość informacyjna opakowań jako determinanta zakupu żywności. Mark. Instytucji Nauk. Badaw. 2020, 2, 31–44. [Google Scholar]
- Pawlak-Lemańska, K.; Mruk-Tomczak, D. Ocena postrzegania informacji na etykietach deserków jabłkowych dla dzieci. Handel Wewnętrzny 2018, 2, 343–356. [Google Scholar]
- Regulation (EU) No 609/2013 of the European Parliament and of the Council of 12 June 2013 on Food Intended for Infants and Young Children, Food for Special Medical Purposes, and Total Diet Replacement for Weight Control and Repealing Council Directive 92/52/EEC, Commission Directives 96/8/EC, 1999/21/EC, 2006/125/EC and 2006/141/EC, Directive 2009/39/EC of the European Parliament and of the Council and Commission Regulations (EC) No 41/2009 and (EC) No 953/2009 Text with EEA relevance. Off. J. Eur. Union 2013, 35–56. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32013R0609 (accessed on 23 February 2022).
- von Philipsborn, P.; Geffert, K.; Klinger, C.; Hebestreit, A.; Stratil, J.; Rehfuess, E.A.; PEN Consortium. Nutrition policies in Germany: A systematic assessment with the Food Environment Policy Index. Public Health Nutr. 2022, 25, 1691–1700. [Google Scholar] [CrossRef]
- Djojosoeparto, S.K.; Kamphuis, C.B.M.; Vandevijvere, S.; Poelman, M.P. How can National Government Policies Improve Food Environments in the Netherlands? Int. J. Public Health 2022, 7, 1604115. [Google Scholar] [CrossRef]
- Mackay, S.; Gerritsen, S.; Sing, F.; Vandevijvere, S.; Swinburn, B. Implementing healthy food environment policies in New Zealand: Nine years of inaction. Health Res. Policy Syst. 2022, 15, 8. [Google Scholar] [CrossRef]
- Vanderlee, L.; Goorang, S.; Karbasy, K.; Vandevijvere, S.; L’Abbé, M.R. Policies to Create Healthier Food Environments in Canada: Experts’ Evaluation and Prioritized Actions Using the Healthy Food Environment Policy Index (Food-EPI). Int. J. Environ. Res. Public Health 2019, 14, 4473. [Google Scholar] [CrossRef]
- Reformat, B.; Reformat, P. Działania Sieci Handlowych w Kierunku Rozwoju Zdrowych Nawyków Żywieniowych Polskich Konsumentów, np. Oferty Produktów Bio i Eco. Studia Ekon. 2018, 354, 17–26. [Google Scholar]
- Goryńska-Goldmann, E. Ewolucja rozwoju żywności lokalnej w kontekście idei zrównoważonej konsumpcji. J. Tour. Reg. Dev. 2019, 12, 43–57. [Google Scholar]
- Ustawa z dnia 16 Listopada 2016 r. o Zmianie Niektórych Ustaw w Celu Ułatwienia Sprzedaży Żywności Przez rolników (Dz.U. 2016 poz. 1961.). Available online: https://dziennikustaw.gov.pl/D2016000196101.pdf (accessed on 23 February 2022).
- CBOS, Akademia Leona Koźmińskiego. Jak i gdzie kupujemy żywność? Komunikat z badań CBOS, BS/94/2013. Available online: https://www.kozminski.edu.pl/fileadmin/wspolne_elementy/Dokumenty/Raporty_ALK-CBOS/K094_13_zakupy_zywnosci.pdf (accessed on 5 February 2021).
- Yamaguchi, M.; Nomura, M.; Arai, Y.; Vandevijvere, S.; Swinburn, B.; Nishi, N. An assessment of implementation gaps and priority recommendations on food environment policies: The Healthy Food Environment Policy Index in Japan. Public Health Nutr. 2022, 25, 1720–1732. [Google Scholar] [CrossRef]
- McFadden, A.; Green, J.M.; Williams, V.; Mcleish, J. Can food vouchers improve nutrition and reduce health inequalities in low-income mothers and young children: A multi-method evaluation of the experiences of beneficiaries and practitioners of the Healthy Start programme in England. BMC Public Health 2014, 14, 148. [Google Scholar] [CrossRef]
- NIZP-PZH. Ograniczanie Społecznych Nierówności w Zdrowiu. 2017. Available online: http://bazawiedzy.pzh.gov.pl/nierownosci-w-zdrowiu (accessed on 5 September 2021).
- Rządowe Centrum Legislacji. 2015. Available online: http://legislacja.rcl.gov.pl/docs//2/12279566/12326791/12326792/dokument199002.pdf (accessed on 28 June 2021).
- Ministerstwo Finansów. Matryca Stawek VAT. 2020. Available online: https://www.podatki.gov.pl/vat/abc-vat/matryca-stawek-vat/ (accessed on 13 February 2020).
- Gröfke, N.; Duplat, V.; Wickert, C.; Tjemkes, B. A Multi-Stakeholder Perspective on Food Labelling for Environmental Sustainability: Attitudes, Perceived Barriers, and Solution Approaches towards the ‘Traffic Light Index’. Sustainability 2021, 13, 933. [Google Scholar] [CrossRef]
- Kaliszewska, M. Dyskurs medialny o odżywaniu się uczniów w szkole i skutkach rozporządzenia Ministra Zdrowia. Wprowadzenie do badań, cz.1. J. Res. Rev. Q. 2016, 1, 19–35. [Google Scholar]
- Opinion of the European Economic and Social Committee on ‘Civil Society’s Contribution to the Development of a Comprehensive Food Policy in the EU’ (Own-Initiative Opinion) OJ C 129. Available online: https://op.europa.eu/en/publication-detail/-/publication/d51efa40-3d13-11e8-b5fe-01aa75ed71a1/language-en (accessed on 1 March 2022).
- Mylona, K.; Ulberth, F.; Maragkoudakis, P.; Bock, A.-K.; Caldeira, S.; Wollgast, J. Delivering on EU Food Safety and Nutrition in 2050—Future Challenges and Policy Preparedness; EUR27957 EN; Publications Office of the European Union: Luxembourg, 2016; ISBN 978-92-79-58916-4. [Google Scholar] [CrossRef]
- Day, R.E.; Sahota, P.; Christian, M.S. Effective implementation of primary school-based healthy lifestyle programmes: A qualitative study of views of school staff. BMC Public Health 2019, 19, 1239. [Google Scholar] [CrossRef]
- Bragg, M.A.; Miller, A.N.; Elizee, J.; Dighe, S.; Elbel, B.D. Popular music celebrity endorsements in food and nonalcoholic beverage marketing. Pediatrics 2016, 138, e20153977. [Google Scholar] [CrossRef]
- Sun, Y.; You, W.; Almeida, F.; Estabrooks, P.; Davy, B. The Effectiveness and Cost of Lifestyle Interventions Including Nutrition Education for Diabetes Prevention: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2017, 117, 404–421.e36. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rank | Action | Domain/Indicator in the Food-EPI That the Respective Action Refers to | Average Score (Importance, Achievability, Equity Scores Combined, Weighting Included) |
|---|---|---|---|
| 1 | Action 3. Introduce a clear and simple labelling system for food products, including information on salt/sugar/trans fats. | 2/1 | 4.0 |
| 2 | Action 12. Prepare the launching of information campaigns that are thoroughly prepared from the sociological and psychological point of view, preceding the introduction of food policy regulations. | All | 3.69 |
| 3 | Action 1. Modify the Ordinance of the Minister of Health on groups of foodstuffs intended for sale to children and adolescents in education system units and the requirements to be met by foodstuffs used as part of mass nutrition for children and adolescents in these units in a way that specifies requirements that are consistent with nutritional requirements and recommendations. | 5/1 | 3.57 |
| 4 | Action 7. Modify school curricula by adding a subject or at least a compulsory thematic block on “nutritional education”. | 5/2 5/4 | 3.53 |
| 5 | Action 5. Change the VAT matrix in a way that unequivocally promotes low-processed foods and healthy food choices. | 4/1 | 3.21 |
| 6 | Action 4. Introduce warnings on food products and/or during advertisements for products that are not recommended in the daily diet (e.g., sweets, energy/sweetened drinks) in line with regulations regarding drugs or tobacco product packaging. Regulate the media market in the field of unhealthy food advertisements, including the application of consistent regulations to the entire media market, including the internet. | 2/1 3/1 3/2 | 3.14 |
| 7 | Action 2. Regulate the rules for eating meals in schools with regard to the time and place of eating a meal (reserve enough time for and the regularity of eating meals). | 5/1 | 3.03 |
| 8 | Action 10. Introduce regulations limiting the exposure of unhealthy food in commercial establishments, especially in regard to exposing such food to the eyes of children and/or prohibiting displaying such food in the vicinity of cash desks. | 6/1 | 2.98 |
| 9 | Action 8. Introduce a requirement to label menu items in restaurants, taking into account the nutritional and energy value of the dishes served. | 2/2 | 2.70 |
| 10 | Action 13. Introduce food fortification (e.g., with folic acid) to eliminate the most common shortages. | 1/1 | 2.44 |
| 11 | Action 6. Modify the assumptions of the nutritional policy implemented in relation to poor individuals in a way that promotes healthy eating choices (e.g., creating a catalogue of products that cannot be purchased with food vouchers and/or rewarding the purchase of low-processed food). | 4/3 4/4 | 2.39 |
| 12 | Action 11. Implement social impact programmes aimed at building a culture of trust and support for regulations in the field of healthy eating. | All | 2.31 |
| 13 | Action 15. Introduce a system of incentives and discounts for small entrepreneurs for running small vegetable and fruit stores to increase access to low-processed food. | 6/2 | 1.85 |
| 14 | Action 14. Introduce legal requirements regarding public procurements in a way that enforces the use of the quality criterion of purchased food products. | 5/3 | 1.69 |
| 15 | Action 9. Introduce a system of controlling the density of fast-food bars in the public space, e.g., through a licensing system, taking into account the distance from educational establishments. | 6/1 | 1.45 |
| Rank | Action | Domain/Indicator in the Food-EPI That the Respective Action Refers to | Average Score (Importance, Achievability, Equity Scores Combined, Weighting Included) |
|---|---|---|---|
| 1 | Action 3. Introduce a system of trainings on healthy eating rules targeting people responsible for feeding children (including cooks, authorizing officers, parents). | 2/4 | 5.67 |
| 2 | Action 2. Promote the principles of healthy eating using marketing tools, media campaigns and influencers. | 2/2 | 5.21 |
| 3 | Action 1. Introduce reimbursed dietitian services at the level of primary health care and specialist care. | 1/5 2/4 | 5.1 |
| 4 | Action 9. Legally regulate the profession of dietitian. | 2/3 | 4.83 |
| 5 | Action 11. Facilitate the availability of fruit and vegetables in schools and workplaces. | ¼ | 4.7 |
| 6 | Action 12. Introduce dietary supervision of nutrition in educational institutions and child care and caregiving institutions (e.g., require a special administrative position at the municipal/commune level). | 1/2 3/2 | 4.67 |
| 7 | Action 5. Creating leaders—the implementation of educational programmes to disseminate nutritional knowledge among people responsible for the education and upbringing of children and the introduction of an appropriate educational module as part of pedagogical studies. | 1/1 | 4.35 |
| 8 | Action 13. Introduce systemic and transparent rules of collective nutrition in public entities (especially hospitals) in accordance with evidence-based public health. Introduce hospital nutrition education. | 2/2 | 4.25 |
| 9 | Action 4. Create leaders who promote healthy food choices and support public action at various levels, including the micro-level (e.g., school managers). | 1/1 | 4.19 |
| 10 | Action 8. Introduce tax solutions that support employers in promoting healthy food choices in the workplace. | 1/5 | 3.86 |
| 11 | Action 14. Introduce unified requirements regarding the need to conduct evaluations of implemented public health activities. | 3/4 | 3.58 |
| 12 | Action 6. Introduce a public communication system for sanitary inspection alerts regarding food products and dietary supplements (e.g., a system analogous to the alerts of the Government Centre for Security distributed via mobile telephone networks). | 3/1 | 3.2 |
| 13 | Action 10. Implement regularly conducted epidemiological studies and monitoring of the nutritional status of the population as a basis for the implementation of public health actions. | 4/1 2/2 | 2.86 |
| 14 | Action 15. Create a system of information exchange and coordination of activities of entities implementing nutrition policy tasks, health education and health promotion to increase the effectiveness of spending funds and to improve measures targeting the population’s health status, especially its nutritional status. | 5/4 | 2.86 |
| 15 | Action 7. Introduce clear and transparent solutions for food certification to build public confidence in this system. Develop the ability to recognize quality certificates. | 2/1 2/3 | 2.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romaniuk, P.; Kaczmarek, K.; Brukało, K.; Grochowska-Niedworok, E.; Łobczowska, K.; Banik, A.; Luszczynska, A.; Poelman, M.; Harrington, J.M.; Vandevijvere, S.; et al. The Healthy Food Environment Policy Index in Poland: Implementation Gaps and Actions for Improvement. Foods 2022, 11, 1648. https://doi.org/10.3390/foods11111648
Romaniuk P, Kaczmarek K, Brukało K, Grochowska-Niedworok E, Łobczowska K, Banik A, Luszczynska A, Poelman M, Harrington JM, Vandevijvere S, et al. The Healthy Food Environment Policy Index in Poland: Implementation Gaps and Actions for Improvement. Foods. 2022; 11(11):1648. https://doi.org/10.3390/foods11111648
Chicago/Turabian StyleRomaniuk, Piotr, Krzysztof Kaczmarek, Katarzyna Brukało, Elżbieta Grochowska-Niedworok, Karolina Łobczowska, Anna Banik, Aleksandra Luszczynska, Maartje Poelman, Janas M. Harrington, Stefanie Vandevijvere, and et al. 2022. "The Healthy Food Environment Policy Index in Poland: Implementation Gaps and Actions for Improvement" Foods 11, no. 11: 1648. https://doi.org/10.3390/foods11111648
APA StyleRomaniuk, P., Kaczmarek, K., Brukało, K., Grochowska-Niedworok, E., Łobczowska, K., Banik, A., Luszczynska, A., Poelman, M., Harrington, J. M., Vandevijvere, S., & on behalf of the PEN Consortium. (2022). The Healthy Food Environment Policy Index in Poland: Implementation Gaps and Actions for Improvement. Foods, 11(11), 1648. https://doi.org/10.3390/foods11111648