
Attitudes towards Freshly Made and Readily Prepared Texture-Modified Foods among Speech-Language Therapists, Dietitians, and Community-Dwelling Older Adults


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. TMF Samples
2.4. Data Collection
2.4.1. Questionnaires with Sensory Ratings
2.4.2. Focus Groups
2.5. Data Analysis
3. Results
3.1. Participant Characteristics
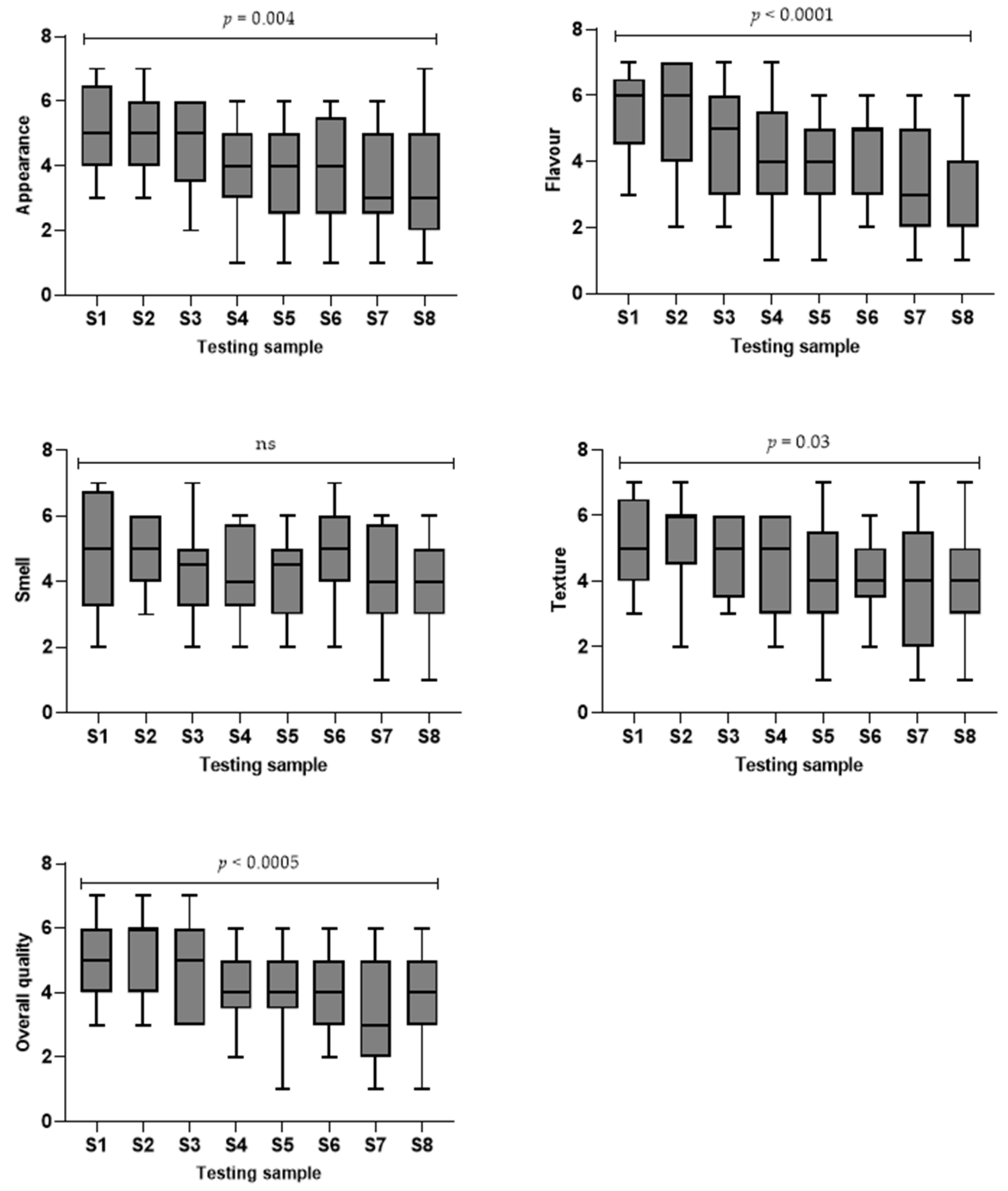
3.2. Palatability of TMFs
3.2.1. Appearance Is the First Impression
- “I personally felt like the colour was all right because it still looks like meat. I feel like people wouldn’t want artificial colouring.” (Speech-language therapist).
- “If you can see what is in it, you kind of know what to expect. I don’t know if it is just my mind, (I feel) like all the orange ones taste the same, and then all the other colour ones taste the same.” (Dietitian).
3.2.2. Richer Meat Taste Is Preferred
- “I think taste that is quite a personal thing because you can have a couple of carbs and a veg on your plate, and this is only part of your meal.” (Speech-language therapist).
- “I think (hydrolysed puree) seven tastes meatier to me compared to (commercially packaged puree) eight. (Commercially packaged puree) eight is creamier.” (Dietitian).
3.2.3. Optimal Texture and Consistency Are Difficult to Achieve
- “I thought waterier was nicer. This one (commercially packaged Minced & Moist) was a bit dry. I mean it is probably moister than it looked, which is why I did call it meeting standard.” (Speech-language therapist).
- “I didn’t find six (freshly made puree) that acceptable as a smooth puree. I do find it quite gritty and for my head and neck patients who may have quite a lot of swelling and when they’ve reconstructed. Say somebody’s tongue doesn’t move the same as your tongue does and things get lost down the side of the mouth, so that sort of grittiness that people have commented on quite a lot not with the puree food.” (Dietitian).
- “I didn’t like the first one (freshly made Soft & Bite-sized chicken). I found it was a bit too chewy and tough. But the second one (sous-vide Soft & Bite-sized chicken), those smaller chicken pieces, were divine.” (Older adult).
- “The (sous-vide Soft & Bite-sized) two is closer (to the standard), but still need to really focus on the chewing and put some force into it. I just wonder if beef and lamb are virtually impossible to make Soft & Bite-Sized as the meat product.” (Speech-language therapist).
3.3. Perceived Challenges for the Currently Available TMFs
3.3.1. Freshly Made TMFs
- “In terms of caregiver, I don’t think there is enough training for caregivers to prepare the same consistency (TMFs).” (Speech-language therapist).
- “We have two soft diets. We have got soft mechanical and soft dysphagic, so sometimes there can be confusion around which one is most appropriate. It is really important to differentiate like what do you consider soft does.” (Dietitian).
- “From the foodservice perspective, I am just thinking about whenever I have been in there. It is almost like the foodservice staff will identify which sort of food options are in the standard menu that would qualify as Soft & Bite-Sized.” (Dietitian).
3.3.2. Readily Prepared TMFs
- “It depends on their age. I mean, obviously that we do get a lot of young patients around 30–50 s that are perfectly capable of preparing food, and then we get a lot of older patients who may not necessarily be that comfortable with doing that or don’t have the energy to do that. So, we can give them advice for home cooking and talk about food fortification of modified textured foods. We quite often point them towards the commercially packaged ones.” (Dietitian).
- “There is not much variety, so I think it will be good to have some varieties with different things and when it is ready-made as well.” (Speech-language therapist).
- “Because I know the hospital uses the products from the commercially packaged company. I think there is a difference between somebody using those products and warming them up themselves at home and then being done on an industrial scale and delivered to the patients. They are not necessarily arriving at the patient’s bedside in the most appropriate way.” (Dietitian).
3.4. Key Differences in Opinions between Stakeholder Groups
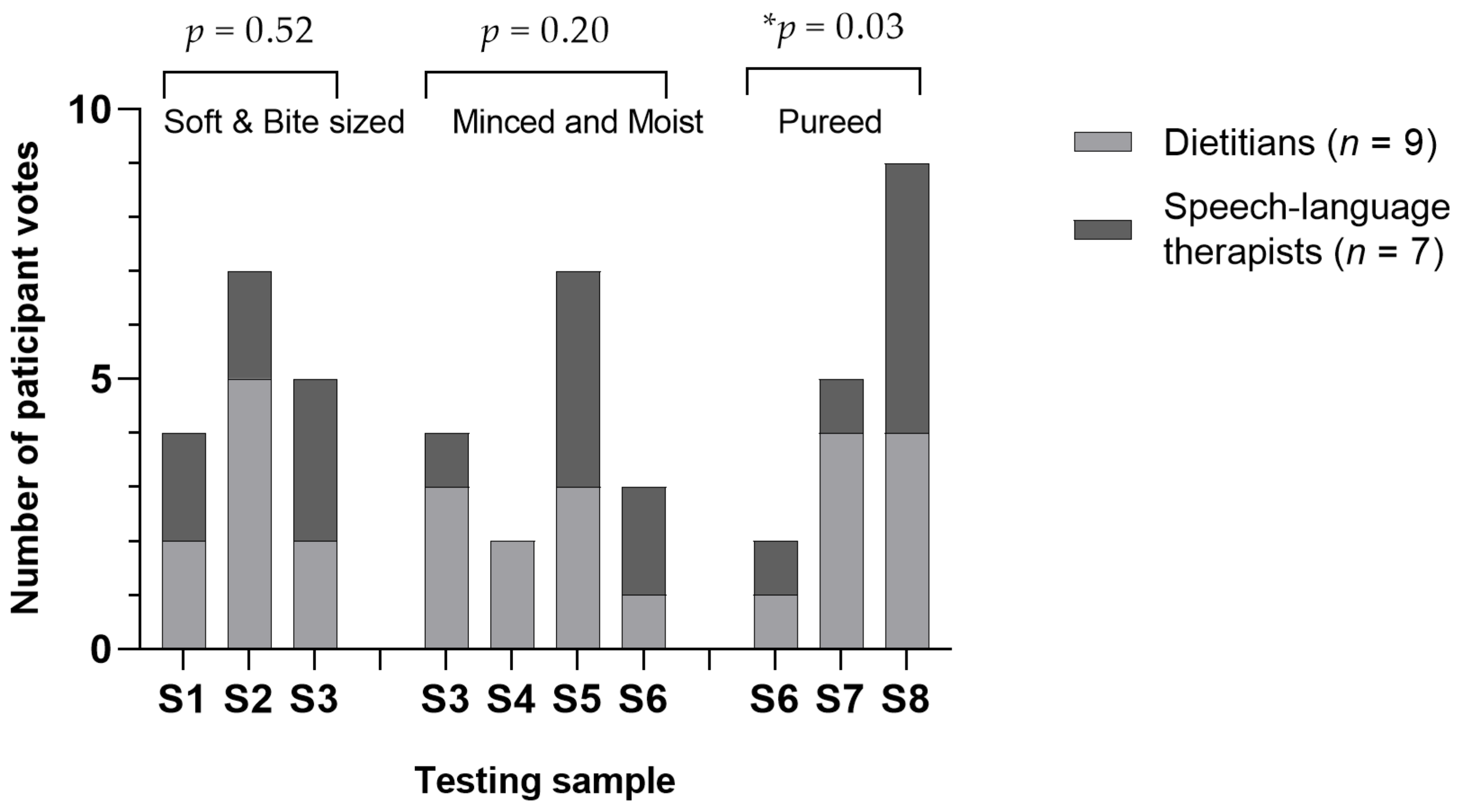
3.4.1. Different Choices in Preferred TMFs
- “I feel like five (commercially packaged minced & moist) and eight (commercially packaged puree) was what I expected like texture-modified food to taste like, just quite tasteless and like not very pleasant. The last one (commercially packaged puree) tastes like pumpkin, but I was surprised by the other ones because it was better than I expected.” (Older adult).
3.4.2. Different Focus of TMF between Dietitians and Speech-Language Therapists
- “I feel flavour and taste (are the most important things) because I think texture makes sense logically, but I feel like you can’t really have one without the other. With flavour, like when I go to see patients in the hospital, the main reason people weren’t eating enough when they were on texture-modified foods was because they just didn’t like the taste. They just found it was disgusting and no texture, appearance, smell or anything could overcome that. So, I feel like flavour is really important because no matter how the texture is if they are not going to eat it.” (Dietitian).
- “I guess our job as a speech-language therapist is always about that safety, so from a speech therapist’s point of view, we care about lumps because they are safety risks for choking.” (Speech-language therapist).
- “I would definitely go for the one with higher meat content.” (Older adult).
4. Discussion
4.1. Palatability of TMFs
4.2. Nutritional Content of TMFs
4.3. Differences between Stakeholders
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cichero, J.A.Y.; Steele, C.; Duivestein, J.; Clavé, P.; Chen, J.; Kayashita, J.; Dantas, R.; Lecko, C.; Speyer, R.; Lam, P.; et al. The Need for International Terminology and Definitions for Texture-Modified Foods and Thickened Liquids Used in Dysphagia Management: Foundations of a Global Initiative. Curr. Phys. Med. Rehabil. Rep. 2013, 1, 280–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFabrizio, M.E.; Rajappa, A. Contemporary Approaches to Dysphagia Management. J. Nurse Pract. 2010, 6, 622–630. [Google Scholar] [CrossRef]
- Wham, C.; Fraser, E.; Buhs-Catterall, J.; Watkin, R.; Gammon, C.; Allen, J. Malnutrition risk of older people across district health board community, hospital and residential care settings in New Zealand. Australas. J. Ageing 2017, 36, 205–211. [Google Scholar] [CrossRef]
- Rothenberg, E.; Wendin, K. Texture modification of food for elderly people. In Modifying Food Texture; Chen, J., Rosenthal, A., Eds.; Elsevier: Amsterdam, The Netherlands, 2015; Volume 2, pp. 163–185. ISBN 9781782423522. [Google Scholar]
- Engh, M.C.N.; Speyer, R. Management of Dysphagia in Nursing Homes: A National Survey. Dysphagia 2022, 37, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Cichero, J.A.Y. Adjustment of Food Textural Properties for Elderly Patients. J. Texture Stud. 2016, 47, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Garcia, J.M.; Chambers, E. Managing Dysphagia Through Diet Modifications. AJN Am. J. Nurs. 2010, 110, 26–33. [Google Scholar] [CrossRef]
- Martineau, C. International Dysphagia Diet Standardisation Initiative: IDDSI Framework. Available online: http://iddsi.org/framework/ (accessed on 29 May 2021).
- Aguilera, J.M.; Park, D.J. Texture-modified foods for the elderly: Status, technology and opportunities. Trends Food Sci. Technol. 2016, 57, 156–164. [Google Scholar] [CrossRef]
- Wu, X.S.; Miles, A.; Braakhuis, A. An Evaluation of Texture-Modified Diets Compliant with the International Dysphagia Diet Standardization Initiative in Aged-Care Facilities Using the Consolidated Framework for Implementation Research. Dysphagia 2022. [Google Scholar] [CrossRef]
- Ahmad, N.B. Beef hydorlysis by Zyactinase Enzymes. Ph.D. Thesis, Massey University, Palmerston North, New Zealand, 2016. [Google Scholar]
- Lee, K.M.; Song, J.-A. Factors influencing the degree of eating ability among people with dementia. J. Clin. Nurs. 2015, 24, 1707–1717. [Google Scholar] [CrossRef]
- Cardello, A.V.; Bell, R.; Kramer, F.M. Attitudes of consumers toward military and other institutional foods. Food Qual. Prefer. 1996, 7, 7–20. [Google Scholar] [CrossRef]
- Cassens, D.; Johnson, E.; Keelan, S. Enhancing taste, texture, appearance, and presentation of pureed food improved resident quality of life and weight status. Nutr. Rev. 1996, 54, S51–S54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, C.J.; Milan, A.M.; Mitchell, S.M.; Zeng, N.; Ramzan, F.; Sharma, P.; Knowles, S.O.; Roy, N.C.; Sjödin, A.; Wagner, K.-H.; et al. The effects of dietary protein intake on appendicular lean mass and muscle function in elderly men: A 10-wk randomized controlled trial. Am. J. Clin. Nutr. 2017, 106, 1375–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Food and Nutrition Guidelines for Healthy Older People A Background Paper; Minstry of Health: Wellingon, New Zealand, 2013.
- Zanini, M.; Bagnasco, A.; Catania, G.; Aleo, G.; Sartini, M.; Cristina, M.L.; Ripamonti, S.; Monacelli, F.; Odetti, P.; Sasso, L. A Dedicated Nutritional Care Program (NUTRICARE) to reduce malnutrition in institutionalised dysphagic older people: A quasi-experimental study. J. Clin. Nurs. 2017, 26, 4446–4455. [Google Scholar] [CrossRef] [PubMed]
- Keller, H.; Chambers, L.; Niezgoda, H.; Duizer, L. Issues associated with the use of modified texture foods. J. Nutr. Health Aging 2012, 16, 195–200. [Google Scholar] [CrossRef]
- Wu, X.S.; Miles, A.; Braakhuis, A. Nutritional Intake and Meal Composition of Patients Consuming Texture Modified Diets and Thickened Fluids: A Systematic Review and Meta-Analysis. Healthcare 2020, 8, 579. [Google Scholar] [CrossRef]
- Miles, A.; Dennison, K.; Oad, M.A.; Shasha, L.; Royal, M. Consumer Satisfaction of Texture Modified Meals Served in Residential Aged-Care Facilities. Int. J. Food Sci. Nutr. Res. 2019, 1, 1–10. [Google Scholar] [CrossRef]
- Baijens, L.W.J.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.; Leners, J.C.; Masiero, S.; Mateos del Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders – European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [Green Version]
- Ettinger, L.; Keller, H.H.; Duizer, L.M. A comparison of liking of pureed food between two groups of older adults. J. Nutr. Gerontol. Geriatr. 2014, 33, 198–209. [Google Scholar] [CrossRef]
- Pelletier, C.A.; Lawless, H.T. Measuring taste acceptance in neurologically impaired adults. Food Qual. Prefer. 2003, 14, 595–602. [Google Scholar] [CrossRef]
- Rothenberg, E.; Ekman, S.; Bülow, M.; Möller, K.; Svantesson, J.; Wendin, K. Texture-modified meat and carrot products for elderly people with dysphagia: Preference in relation to health and oral status. Scand. J. Food Nutr. 2007, 51, 141–147. [Google Scholar] [CrossRef]
- Krueger, R.A. Focus Groups: A Practical Guide for Applied Research, 4th ed.; Casey, M.A., Mary, A.W., Eds.; SAGE: Los Angeles, CA, USA, 2009. [Google Scholar]
- O’Cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Hannan-Jones, M.; Capra, S. Developing a valid meal assessment tool for hospital patients. Appetite 2017, 108, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Okkels, S.L.; Saxosen, M.; Bügel, S.; Olsen, A.; Klausen, T.W.; Beck, A.M. Acceptance of texture-modified in-between-meals among old adults with dysphagia. Clin. Nutr. ESPEN 2018, 25, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Onwuegbuzie, A.J.; Dickinson, W.B.; Leech, N.L.; Zoran, A.G. A Qualitative Framework for Collecting and Analyzing Data in Focus Group Research. Int. J. Qual. Methods 2009, 8, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Wallace, S. Observing method: Recognizing the significant of belief, discipline, position and documentation in observational studies. In Qualitative Research in Health Care; Holloway, I., Ed.; Open University Press: Maidenhead, UK, 2005; pp. 71–84. [Google Scholar]
- Grønkjær, M.; Curtis, T.; De Crespigny, C.; Delmar, C. Analysing group interaction in focus group research: Impact on content and the role of the moderator. Qual. Stud. 1970, 2, 16–30. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research (3rd ed.): Techniques and Procedures for Developing Grounded Theory, 3rd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Holloway, I.; Todres, L. The status of method: Flexibility, consistency and coherence. In Qualitative Research in Health Care; Holloway, I., Ed.; Open University Press: Maidenhead, UK, 2005; pp. 90–103. [Google Scholar]
- Keller, H.; Duizer, L.M. What do consumers think of pureed food? Making the most of the indistinguishable food. J. Nutr. Gerontol. Geriatr. 2014, 33, 139–159. [Google Scholar] [CrossRef]
- Ilhamto, N.; Anciado, K.; Keller, H.H.; Duizer, L.M. In-House Pureed Food Production in Long-Term Care: Perspectives of Dietary Staff and Implications for Improvement. J. Nutr. Gerontol. Geriatr. 2014, 33, 210–228. [Google Scholar] [CrossRef]
- Costa, A.; Carrión, S.; Puig-Pey, M.; Juárez, F.; Clavé, P. Triple adaptation of the mediterranean diet: Design of a meal plan for older people with oropharyngeal dysphagia based on home cooking. Nutrients 2019, 11, 425. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.S.; Miles, A.; Braakhuis, A.J. The Effectiveness of International Dysphagia Diet Standardization Initiative—Tailored Interventions on Staff Knowledge and Texture-Modified Diet Compliance in Aged Care Facilities: A Pre-Post Study. Curr. Dev. Nutr. 2022, 6, nzac021. [Google Scholar] [CrossRef]
- Anciado, K.; Ilhamto, N.; Keller, H.; Duizer, L. Purchasing commercially prepared pureed foods: Nutrition managers’ perspectives. J. Foodserv. Manag. Educ. 2012, 6, 9–16. [Google Scholar]
- Stahlman, L.B.; Garcia, J.M.; Hakel, M.; Chambers IV, E. Comparison ratings of pureed versus molded fruits: Preliminary results. Dysphagia 2000, 15, 2–5. [Google Scholar] [CrossRef]
- Baugreet, S.; Kerry, J.P.; Botineştean, C.; Allen, P.; Hamill, R.M. Development of novel fortified beef patties with added functional protein ingredients for the elderly. Meat Sci. 2016, 122, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Massoulard, A.; Bonnabau, H.; Gindre-Poulvelarie, L.; Baptistev, A.; Preux, P.M.; Villemonteix, C.; Javerliat, V.; Fraysse, J.L.; Desport, J.C. Analysis of the food consumption of 87 elderly nursing home residents, depending on food texture. J. Nutr. Health Aging 2011, 15, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Sungsinchai, S.; Niamnuy, C.; Wattanapan, P.; Charoenchaitrakool, M.; Devahastin, S. Texture Modification Technologies and Their Opportunities for the Production of Dysphagia Foods: A Review. Compr. Rev. Food Sci. Food Saf. 2019, 18, 1898–1912. [Google Scholar] [CrossRef] [Green Version]
- Giura, L.; Urtasun, L.; Belarra, A.; Ansorena, D.; Astiasarán, I. Exploring tools for designing dysphagia-friendly foods: A review. Foods 2021, 10, 1334. [Google Scholar] [CrossRef]
- Nakamura, T.; Amano, N. Proposal for preventing malnutrition in individuals on a texture-modified diet. Nutr. Health 2019, 25, 241–243. [Google Scholar] [CrossRef]
- Heiss, C.J.; Goldberg, L.; Dzarnoski, M. Registered dietitians and speech-language pathologists: An important partnership in Dysphagia management. J. Am. Diet. Assoc. 2010, 110, 1290–1293. [Google Scholar] [CrossRef]
- Brody, R.A.; Touger-Decker, R.; VonHagen, S.; O’Sullivan Maillet, J. Role of registered dietitians in dysphagia screening. J. Am. Diet. Assoc. 2000, 100, 1029–1034. [Google Scholar] [CrossRef]
- Macqueen, C.E.; Taubert, S.; Cotter, D.; Stevens, S.; Frost, G.S. Which commercial thickening agent do patients prefer? Dysphagia 2003, 18, 46–52. [Google Scholar] [CrossRef]
- Schiffman, S.S.; Graham, B.G. Taste and smell perception affect appetite and immunity in the elderly. Eur. J. Clin. Nutr. 2000, 54 (Suppl. 3), S54–S63. [Google Scholar] [CrossRef] [PubMed]
- Walton, K.; Williams, P.; Tapsell, L. What do stakeholders consider the key issues affecting the quality of foodservice provision for long-stay patients? J. Foodserv. 2006, 17, 212–225. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Beef Bolognese (Beef Goulash for Soft & Bite-Sized Level) | |||
|---|---|---|---|
| Freshly Made | Sous-Vide/Hydrolysed | Commercially Packaged | |
| Beef (%) | 38 | 60–75 | 61 |
| Tomato puree (%) | 30 | 10 | 12 |
| Vegetables (%) | 26 | 2–17 | 10 |
| Others a (%) | 6 | 13 | 17 |
| Butter chicken | |||
| Chicken (%) | 47 | 66 | 31 |
| Cream (%) | 12 | 9 | 19 |
| Tomato puree (%) | 19 | 2 | 14 |
| Onions (%) | 10 | 3 | 36 b |
| Others a (%) | 12 | 20 | |
| Product | Levels | Type | Energy (kJ) | Protein (g) | Fat (g) | Saturated Fat (g) | Carbohydrate (g) | Dietary Fibre (g) | Sodium (g) |
|---|---|---|---|---|---|---|---|---|---|
| Beef Bolognese | Soft & Bite-Sized | Freshly made | 387 | 10.1 | 4.3 | 1.2 | 3 | 0.7 | 742 |
| Sous-vide | 676 | 16.5 | 7.2 | 1.4 | 5.7 | 4.3 | 448 | ||
| Minced & Moist | Freshly made | 396 | 6 | 6.2 | 3 | 2.7 | 0.9 | 678 | |
| Hydrolysed | 498 | 14.2 | 5.6 | 2.4 | 2.5 | 1.4 | 255 | ||
| Commercial | 723 | 17 | 9.4 | 2.9 | 5.7 | 1.1 | 370 | ||
| Pureed | Freshly made | 396 | 6 | 6.2 | 3 | 2.7 | 0.9 | 678 | |
| Hydrolysed | 599 | 17.7 | 7 | 3 | 2 | 1.1 | 423 | ||
| Commercial | 723 | 17 | 9.4 | 2.9 | 5.7 | 1.1 | 370 | ||
| Butter chicken | Soft & Bite-Sized | Freshly made | 400 | 10.6 | 4.4 | 2.5 | 2.9 | 1 | 794 |
| Sous-vide | 375 | 15.5 | 1.7 | 0.6 | 2.7 | 1 | 287 | ||
| Minced & Moist | Freshly made | 400 | 10.6 | 4.4 | 2.5 | 2.9 | 1 | 794 | |
| Hydrolysed | 375 | 15.5 | 1.7 | 0.6 | 2.7 | 0.9 | 288 | ||
| Commercial | 738 | 11.2 | 11.3 | 5.8 | 7.6 | 1.9 | 216 | ||
| Pureed | Freshly made | 400 | 10.6 | 4.4 | 2.5 | 2.9 | 1 | 794 | |
| Hydrolysed | 374 | 15.5 | 1.7 | 0.6 | 2.7 | 0.9 | 288 | ||
| Commercial | 738 | 11.2 | 11.3 | 5.8 | 7.6 | 1.9 | 216 |
| Dietitians (n = 9) | Speech-Language Therapists (n = 7) | Older Adults (n = 5) | Total (n = 21) | |
|---|---|---|---|---|
| Gender (Male/Female) | 0/9 | 0/7 | 1/4 | 1/20 |
| Mean age (years) ± SD | 29 ± 11 | 29 ± 8 | 72 ± 4 | 39 ± 21 |
| Age range (years) | 20–50 | 24–45 | 68–77 | 20–77 |
| Professional area a | ||||
| Hospital | 4 | 1 | Retired | 5 |
| Research | 2 | 1 | 3 | |
| Master students b | 4 | 5 | 9 | |
| Commercial industry | 1 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, X.S.; Miles, A.; Braakhuis, A. Attitudes towards Freshly Made and Readily Prepared Texture-Modified Foods among Speech-Language Therapists, Dietitians, and Community-Dwelling Older Adults. Foods 2022, 11, 2157. https://doi.org/10.3390/foods11142157
Wu XS, Miles A, Braakhuis A. Attitudes towards Freshly Made and Readily Prepared Texture-Modified Foods among Speech-Language Therapists, Dietitians, and Community-Dwelling Older Adults. Foods. 2022; 11(14):2157. https://doi.org/10.3390/foods11142157
Chicago/Turabian StyleWu, Xiaojing Sharon, Anna Miles, and Andrea Braakhuis. 2022. "Attitudes towards Freshly Made and Readily Prepared Texture-Modified Foods among Speech-Language Therapists, Dietitians, and Community-Dwelling Older Adults" Foods 11, no. 14: 2157. https://doi.org/10.3390/foods11142157
APA StyleWu, X. S., Miles, A., & Braakhuis, A. (2022). Attitudes towards Freshly Made and Readily Prepared Texture-Modified Foods among Speech-Language Therapists, Dietitians, and Community-Dwelling Older Adults. Foods, 11(14), 2157. https://doi.org/10.3390/foods11142157