1. Introduction
Preparing healthy, diversified and tasteful meals for a balanced diet over a longer period requires time, patience, perseverance, creativity, dedication and cooking skills [
1,
2]. This is especially the case when cooking needs to be carried out for several people with varying preferred food choices, for example, in larger families or with family members adhering to special diets [
3,
4]. Cooking is usually an unpaid task that has been historically assigned to women at the expense of market work and private life [
5,
6,
7].
In contrast to market work which yields a certain wage, the value of cooking is difficult to measure. Cooking plays an important role in the physical and mental well-being of all involved individuals [
8,
9]. Home cooking has also been associated with healthier dietary patterns, and potentially reduces the likelihood of nutrition-related disorders [
10,
11], whereas the frequent consumption of meals prepared away from home has been associated with nutritional deficiencies and an increased risk of all-cause mortality [
12,
13,
14].
Traditionally, women have been more likely to fulfill the role of feeding the family in the United States [
3,
15]. That particular role comprised several time-consuming activities, such as meal planning, food shopping and food preparation [
16,
17]. With movements demanding a more equal treatment of women and men [
18], increasing attention has been paid to the sex gap in unpaid household work and food shopping and cooking duties in particular [
19,
20]. A Canadian analysis suggested that men’s share of cooking has risen substantially, as they now do about 40 percent of all cooking [
21]. Younger generations in particular have apparently moved away from the traditional division of historical roles, and attempt to better balance the work related to cooking and shopping activities [
1,
22]. Notably, some authors also reported opposite findings [
23], and suggested that although younger generations have become much more open-minded about gender roles, those aged 18 to 34 were no more likely than older couples to divide most household chores equitably [
24,
25].
Taillie investigated potential genders gaps with regard to cooking activities, meal preparation and food shopping for meals [
26]. Using data from the American Time Use Study (2003–2016) [
27], this study suggested that home cooking generally increased in the aforementioned time span. College-educated men in particular showed the greatest increase in cooking activities, as their percentage increased from 37.9% in 2003 to 51.9% in 2016. Notably, the proportion of cooking men with less than a high school degree did not change significantly. In women, cooking frequency increased only slightly (from 64.7% to 68.7% for college-educated women). Although cross-sectional, these data suggest that a potential change is taking place, and that historical household role assignments might be subject to transition.
Yet, follow-up data to this investigation are scarce, and other US-based data sources have been rarely investigated with regard to that particular question. To gain deeper insights into the current sex distribution of cooking and food shopping responsibilities in US households, we examined data from the US-based National Health and Nutrition Examination Surveys (NHANES (2017–2020)) [
28].
More specifically, we aimed to investigate the following hypotheses:
- (a)
Sex gaps in cooking duties and food shopping based on traditional role models are still present in the United States but potentially less pronounced.
- (b)
Cooking and food shopping duties are more equally distributed in younger generations, as opposed to older generations.
2. Materials and Methods
2.1. The NHANES
To investigate the aforementioned hypotheses, we used data from the NHANES [
28]. The NHANES is a nationally representative program of studies run by the National Center for Health Statistics (NCHS) designed to assess the health and nutritional status of adults and children in the United States of America. NHANES is an ongoing survey examining a representative sample of about 5000 people per year across the United States. Survey data from the NHANES are frequently used by healthcare professionals to determine the prevalence of major diseases and their risk factors in the United States.
The NHANES has two major components: the interview component and the examination component. The interview component contains demographic, socioeconomic, dietary, and health-related questions. The examination component includes laboratory tests and other medical, dental, and physiological measurements administered by highly trained medical personnel. For additional details, we refer the reader to the NHANES overview brochure summarizing key features of the survey [
29].
For this particular analysis, we used data from various NHANES modules, including demographic data and questionnaire data. All data stem from the NHANES 2017–2020 pre-pandemic cycle [
30]. As of March 2020, the NHANES program has suspended their field operations due to the coronavirus disease 2019 (COVID-19) pandemic. As a result, data collection for the NHANES 2019–2020 cycle was not completed at this point, which implies that the collected data were not nationally representative. Therefore, NHANES combined all data collected from 2019 to March 2020 with data from the NHANES 2017–2018 cycle with the aim of forming a nationally representative sample of NHANES 2017-March 2020 pre-pandemic data.
2.2. Demographic Data
Demographic data included age, sex (male and female), race/ethnicity (Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, Non-Hispanic Asian, and Other Race—including Multiracial), marital status (married/living with partner, widowed/divorced/separated, never married), educational level (less than 9th grade, 9–11th grade, high school graduate/GED or equivalent, some college or AA degree, college graduate or above), and ratio of family income to poverty. For all items, we used the pre-defined NHANES categories without performing particular modifications. Individuals were included regardless of household size, since the NHANES 2017-March 2020 pre-pandemic cycle did not include this variable.
2.3. Meal Planning/Preparing/Shopping Data
Included questionnaire data stem from the Diet Behavior and Nutrition (DBQ) questionnaire [
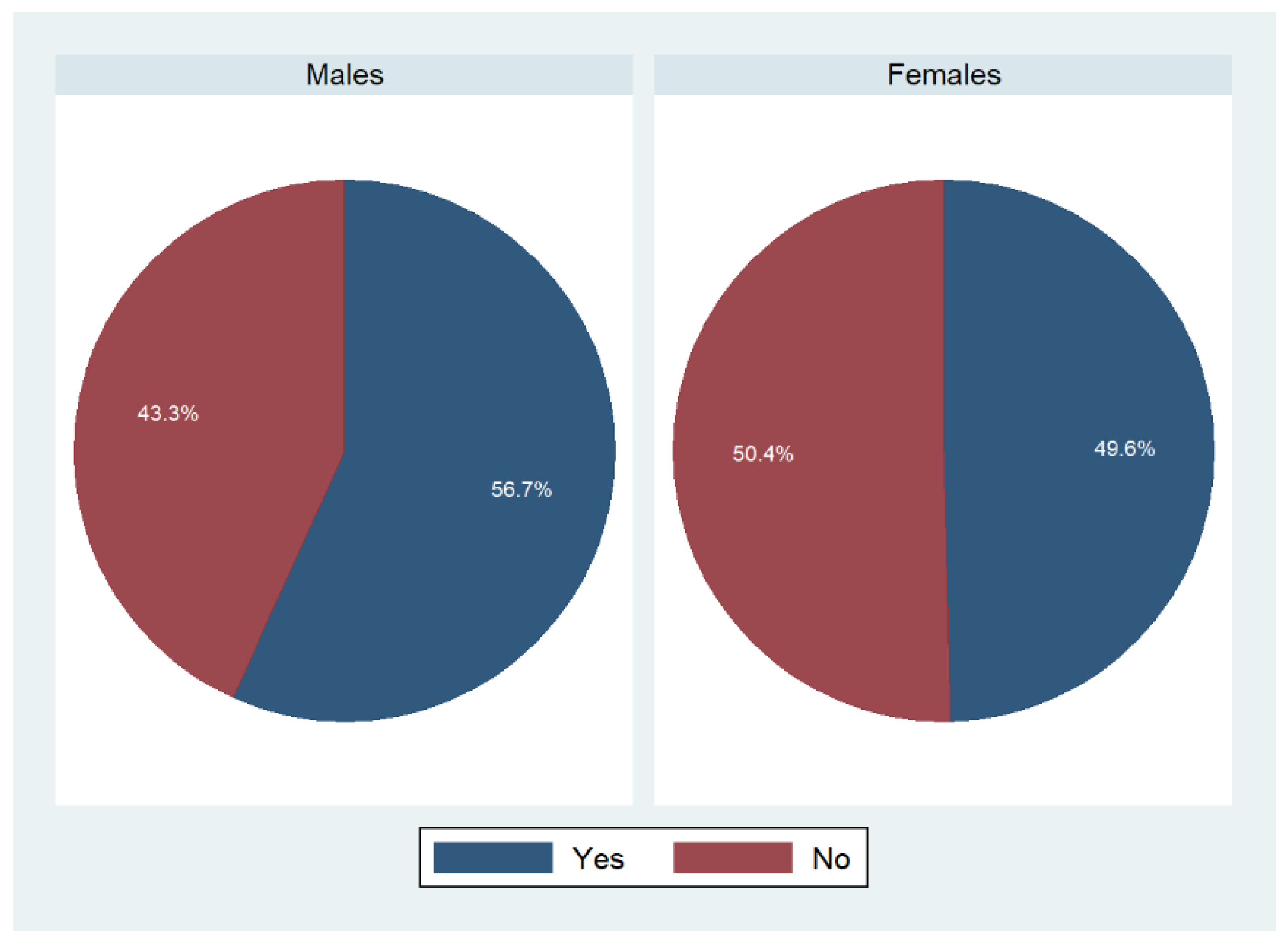
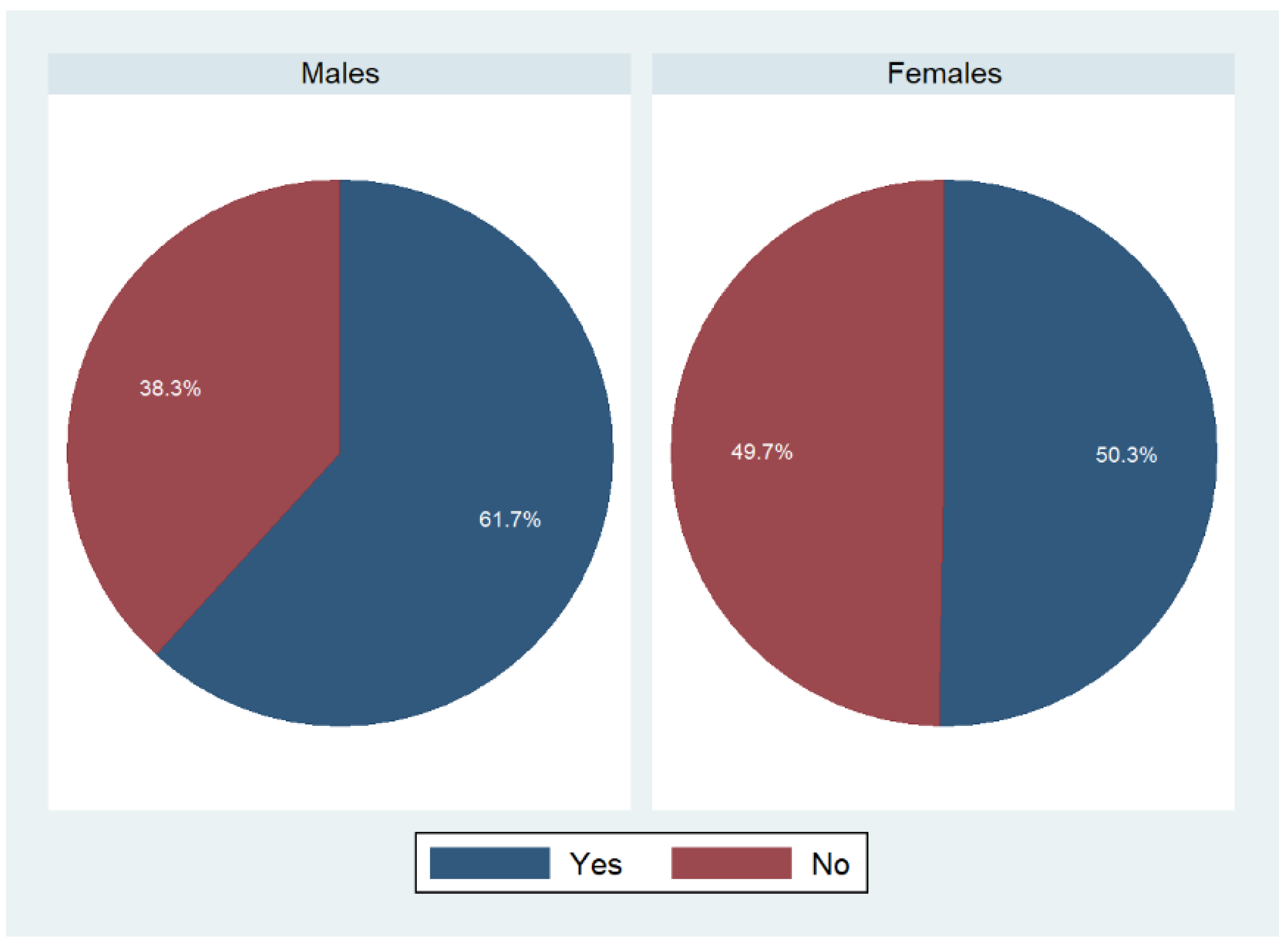
31]. The DBQ contained personal interview data on various dietary behavior and nutrition-related topics. This module included information on participants’ meal planner/shopper/preparer status at home. Questions included: “Are you the person who does most of the planning or preparing of meals in your family?” and “Are you the person who does most of the shopping for food in your family?”. Answer categories included “yes”, “no”, and “don’t know”. Only participants who gave a definite answer (yes/no) were considered in the final analysis.
The module also inquired whether participants shared planning or preparing of meals and shopping duties with someone else. The same answer categories applied here. Data from the DBQ formed the cornerstone of our analysis. Additional information may be obtained from the DBQ module description [
31].
2.4. Statistics
Stata version 14 (StataCorp., College Stadion, TX, USA) was used for the statistical analysis. Appropriate sample weights provided by the NHANES were used to account for the complex, multistage, probability sampling design of the NHANES. All continuous variables were described with their mean and corresponding standard error in parentheses. Categorical variables were described as weighted proportions with their corresponding standard error.
To allow for statistically valid population inferences from sample data, we computed standard errors using established survey data procedures (including Taylor series linearization) that took into account the complex nature of the sample design. Reliability of the presented weighted proportions was assessed based on the current reporting standards for proportions by the NCHS [
32].
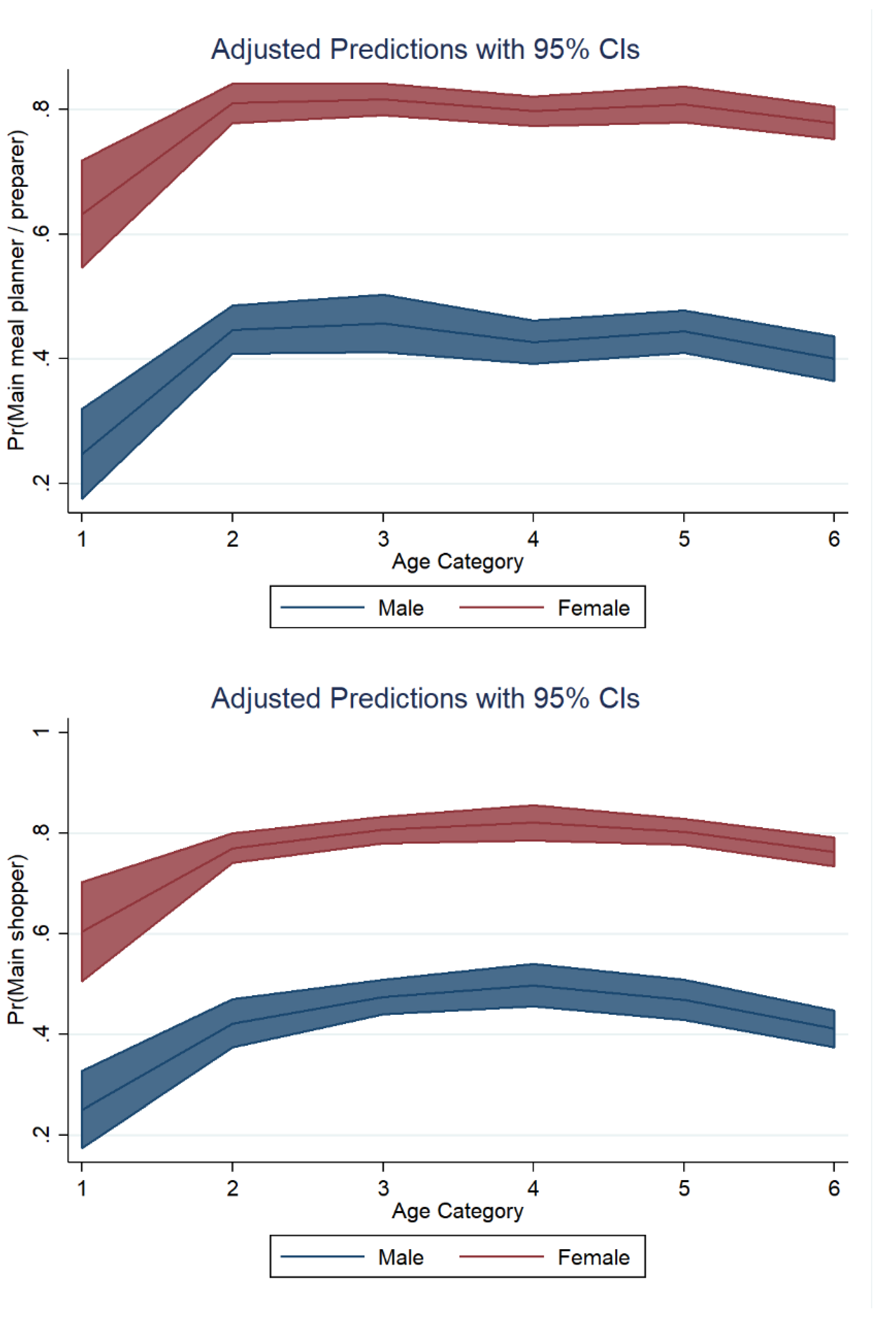
For categorical variables, we used STATA’s design-adjusted Rao–Scott test (a design-adjusted version of the Pearson chi-square test) to explore potential associations between sex and main meal planner/food shopper/food preparer status. In weighted subanalyses, we also stratified results by race/ethnicity and age category.
Furthermore, we ran multivariate logistic regression models to investigate potential associations between sex and main meal planner/food shopper/preparer status after adjusting for covariates. Covariates included age, ethnicity, marital status, education level, and ratio of family income to poverty. Potential covariates were chosen based on initial exploratory bivariate analyses and based on previous publications in the field. All tests were two-sided and statistical significance was determined at α = 0.05.
4. Discussion
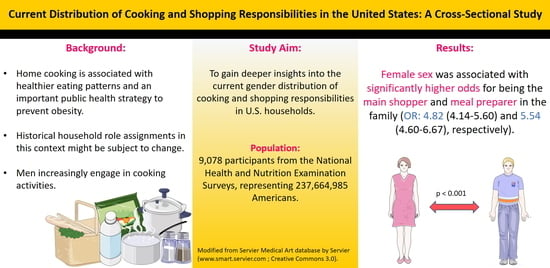
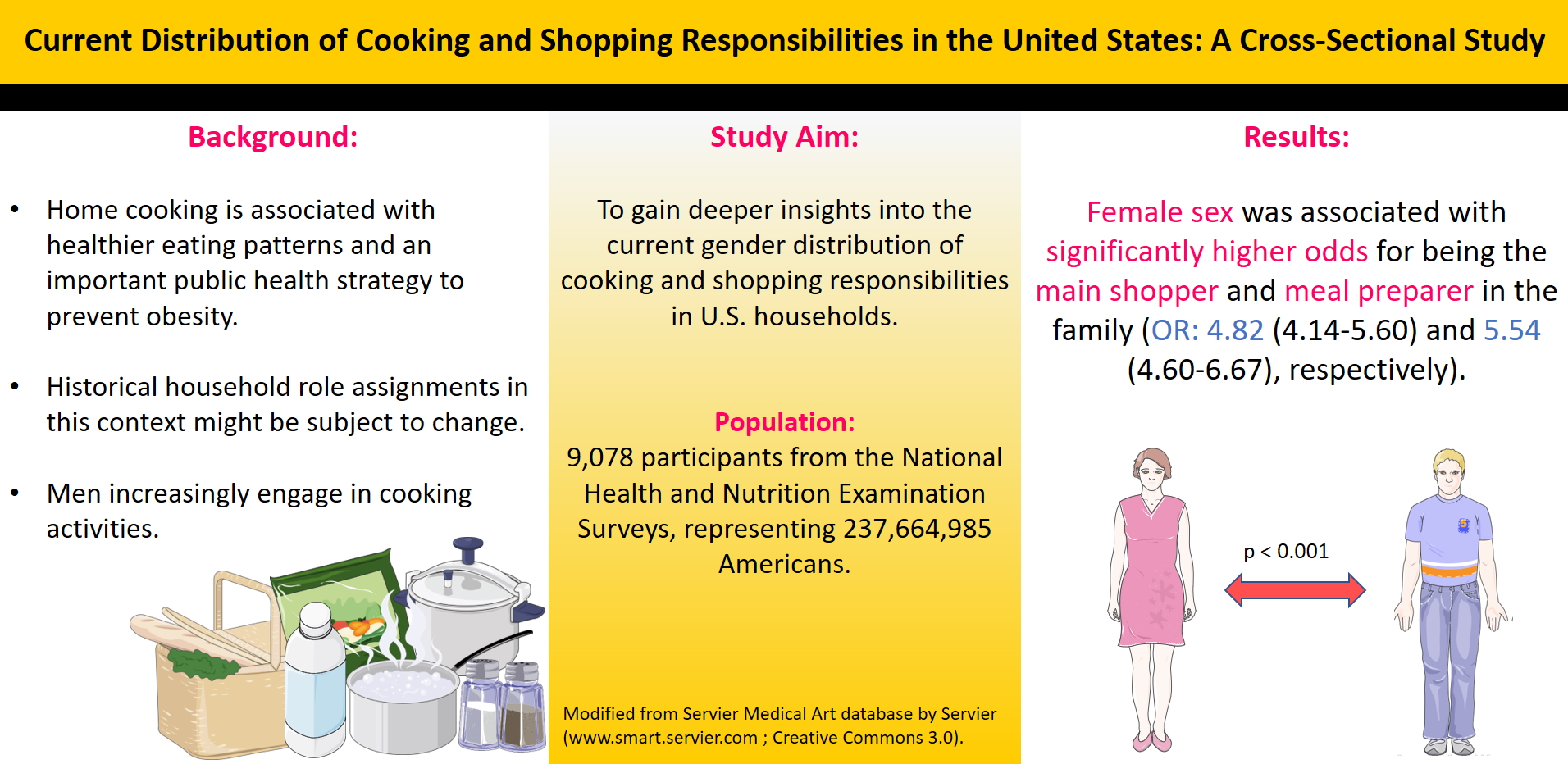
The present study sought to gain deeper insights into the current sex distribution of cooking and food shopping responsibilities in the United States.
Our data suggest that the majority of shopping and cooking duties are still performed by women. More than 80% of women aged 25 years or older responded affirmatively to the statement that they were the person who did most of the planning or preparing of meals in the family. The percentage of males responding affirmatively to this statement was substantially lower. A comparable picture was found with regard to shopping duties. In our employed logistic regression models, female sex was associated with significantly higher odds of being the main food shopper and meal preparer in the family (OR: 4.82 (4.14–5.60) and 5.54 (4.60–6.67), respectively).
Home cooking has been identified as a potent strategy to improve dietary intake and to prevent obesity [
10,
33]. Home cooking has also been associated with numerous social, cultural and emotional benefits, and gives families control over their food supplies [
33,
34]. Despite these benefits, home cooking frequency has demonstrably declined in the second half of the twentieth century [
35]. One study demonstrated that total time spent on cooking in the United States declined by more than 30% from 1965 to 1995 [
35].
One of the most frequent cited reasons for this development is the dual burden in women (e.g., balancing household work and job duties), who have traditionally been the predominant food shoppers and preparers in families [
16,
36]. Although cooking may be joyful at times, it is also filled with time pressures and requires preparation and planning. In a world where many households often depend on every adult family member working, sometimes even in multiple jobs and assignments with non-standard and unpredictable hours, it is immensely difficult to balance paid work and unpaid work at home [
37].
A global analysis by Wolfson et al. revealed that cooking frequency varies considerably around the globe [
38]. Their analysis suggested that women (median frequency 5 meals/week) generally cook more than men (median frequency 0 meals/week). On the other hand, there is also some evidence that the traditional kitchen roles begin to shift and that men take an increasing role in food preparation [
21,
35]. Using data from the NHANES (2017–2020), we therefore investigated the current distribution of cooking and shopping responsibilities among men in women in the United States.
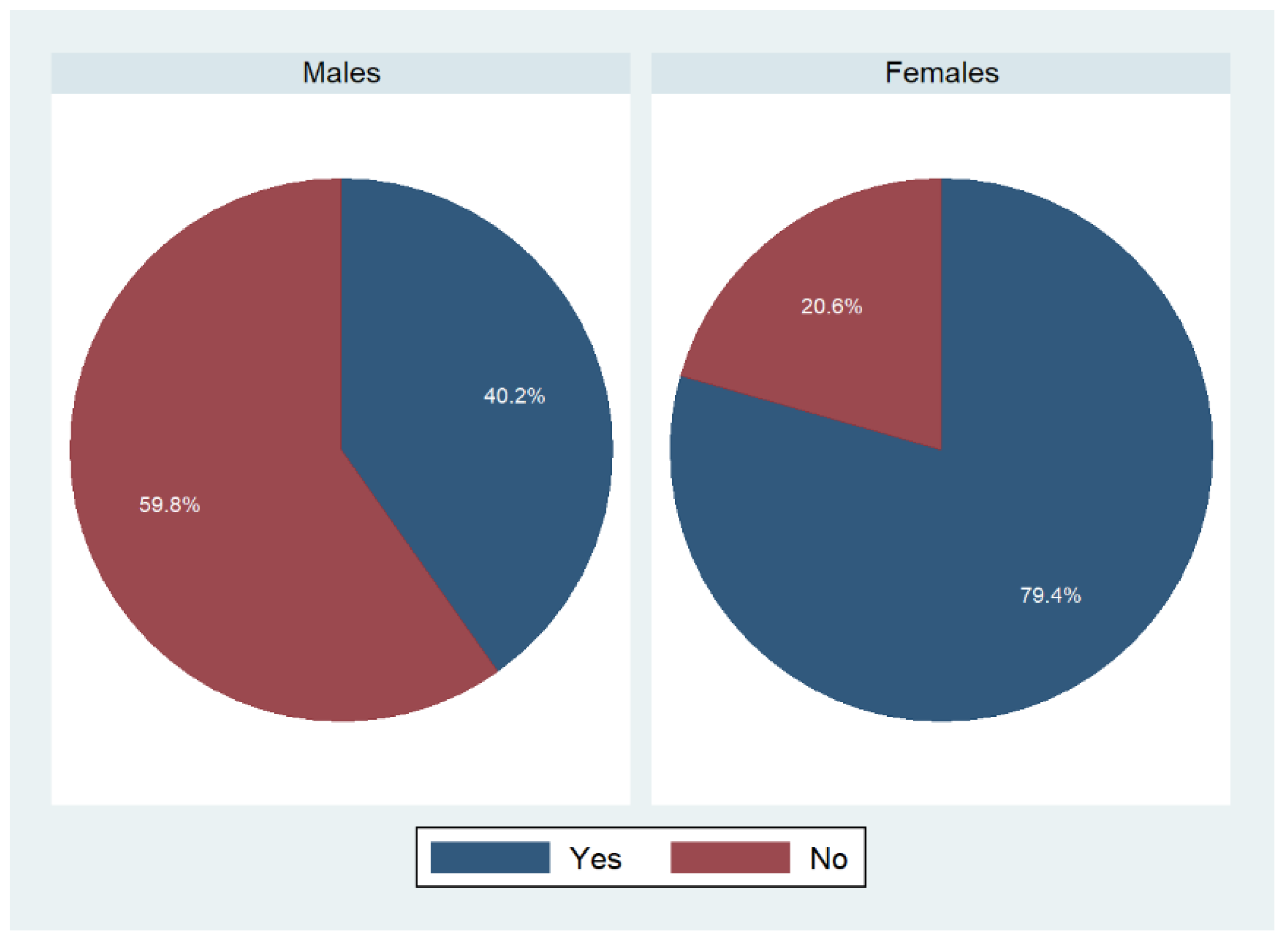
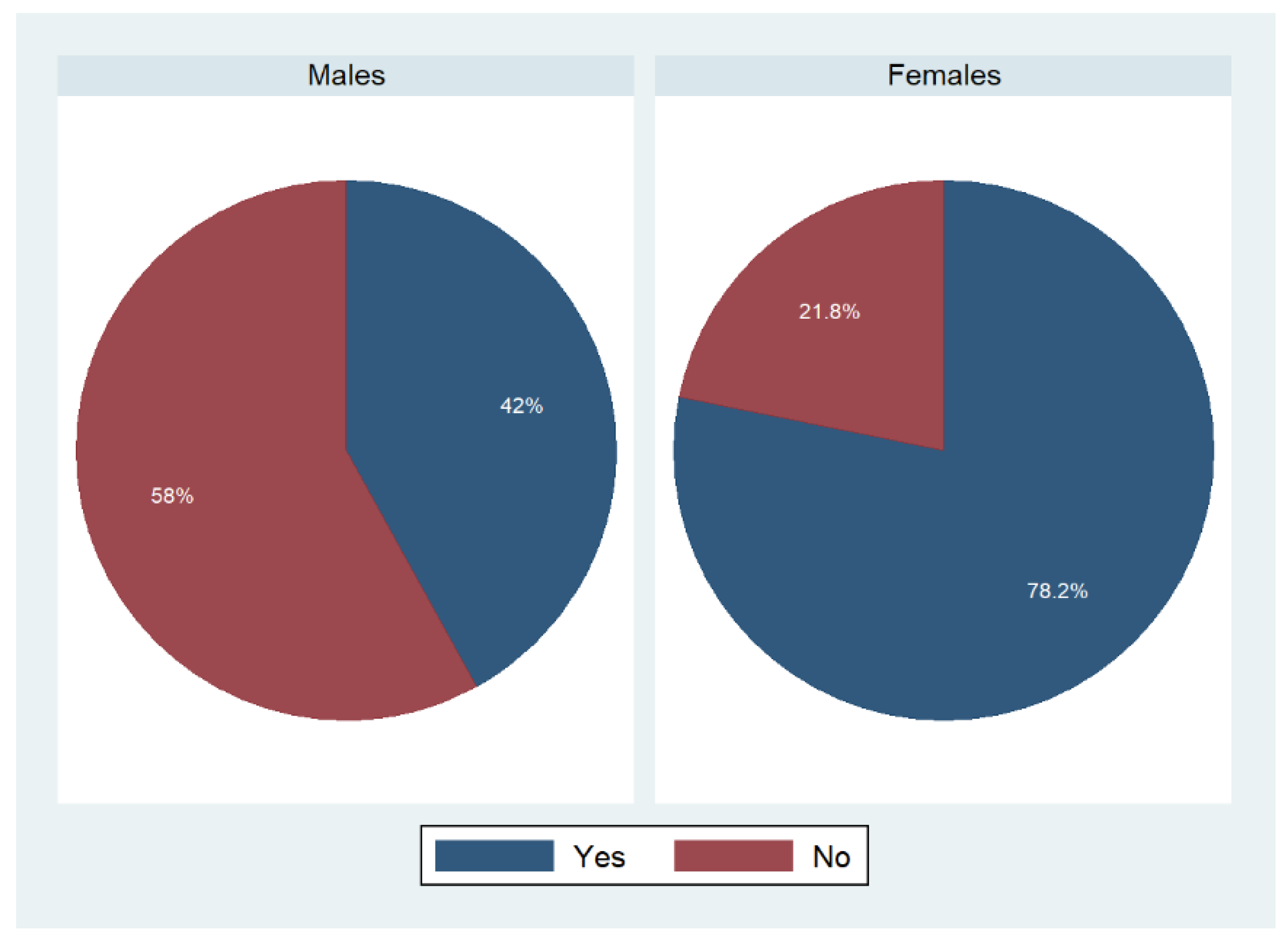
Overall, our results suggest that women are substantially more engaged in food shopping and cooking. Approximately 4/5 of women ≥25 years responded affirmatively to the statement that they were the person who did most of the planning or preparing of meals in family. In contrast, the percentage of males responding affirmatively to this statement was substantially lower (
Table 2). A comparable picture was found with regard to shopping duties.
Our data are thus essentially in line with prior studies from the United States, suggesting an unequal sex distribution in cooking and shopping duties [
26,
39,
40]. Notably, a comparison between the respective studies is difficult and should be performed with great caution in light of the different data sources (e.g., data stem from the American Time Use Study and older NHANES cycles with different variables). Flagg et al., for example, analyzed 2007–2008 NHANES data and demonstrated that women were more likely to report being mainly responsible for both meal preparation/planning and shopping [
39]. According to their analysis, women were also less likely to report having no responsibility for those tasks (in comparison to men). Our results support the ongoing gender gap with regard to cooking and shopping duties that appears to be existent in younger generations, as well. However, the reservation must be made that a 1:1 comparison between studies may not be possible due to differences in the variables’ structures and the employed regression models.
The herein presented data might be useful for policy makers, healthcare professionals, social workers and other authorities. Developing a clear understanding of who engages in food preparation at home and why is of paramount importance to allow for the tailoring of healthy eating and home cooking interventions [
41]. Home cooking interventions demonstrated clear benefits [
42,
43], yet their practical implementation is often a challenge. In a modern world where human and financial resources for healthcare interventions are often scarce, our data might be of value to point out groups that could benefit in particular from such interventions.
Strengths and Limitations
The present analysis draws upon a number of strengths but also has various weaknesses that warrant further discussion. A major strength is the large and nationally representative dataset from the NHANES. The sample comprised almost 9100 individuals, which may be extrapolated to represent 237,664,985 US Americans. Data from the NHANES is often used in epidemiological research, and the NHANES is a trusted longitudinal study and one of the largest of its kind. It is a reliable source designed to assess health and health behavior in US adults. Additional strengths of our manuscript include the various subanalyses (stratified analyses by gender and race/ethnicity) as well as the regression models that include a variety of confounders. Thus, we believe that our data allow for new and important insights into current food shopping and cooking duties distribution in the United States.
On the other hand, the reservation must be made that we present cross-sectional data, and no causal inference can be drawn from this type of dataset. Unlike Taillie [
26], we did not perform a trend analysis and instead provided a rather descriptive picture limited to a relatively short time frame (2017–2020). While we present relatively new data, we also acknowledge that our analyses are built on data that stems from pre-COVID-19 times. Changes in eating, shopping and meal preparation patterns during the pandemic have been reported globally—an important aspect that has to be taken into account [
44,
45,
46,
47].
Moreover, we acknowledge that the analyzed items were mostly self-reported and may thus be subject to bias, such as recall bias or reporting bias. Finally, we acknowledge that our analysis would have benefited from adding additional socioeconomic predictors (e.g., adult employment status) describing our sample. Considering how some of these factors intersect with sex to influence food provisioning behaviors would provide more nuanced insights and possible targets for nutrition interventions and programming. Unfortunately, the addition of some variables would have dramatically reduced the overall sample size, whereas other variables (e.g., the existence of a person to help with household duties) were simply unavailable.
Yet, despite those limitations, we believe that our data allow for important insights into the distribution of meal preparation and shopping duties in the United States. Our data will be of importance for other researchers in the field as they allow for comparisons and trend analyses in said behaviors in the future. Finally, our analysis might be of high translational value for public health authorities and other stakeholders engaged in health promotion. Basic findings from our investigation may be taken into account when tailoring age- and gender-specific health promotion programs designed to promote a healthier lifestyle in Americans.
Our data might be used in future studies as a comparison and to reflect trends, yet future trials should also take the COVID-19 pandemic into account. Post-pandemic studies including a more detailed set of covariates (e.g., the geographical location (rural versus city-side) are required to evolve the understanding of cooking and shopping duties distribution in the United States. A more detailed exploration of the causes and drivers of inequities is also warranted.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}