
Effects of Dietary Plant-Derived Low-Ratio Linoleic Acid/Alpha-Linolenic Acid on Blood Lipid Profiles: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
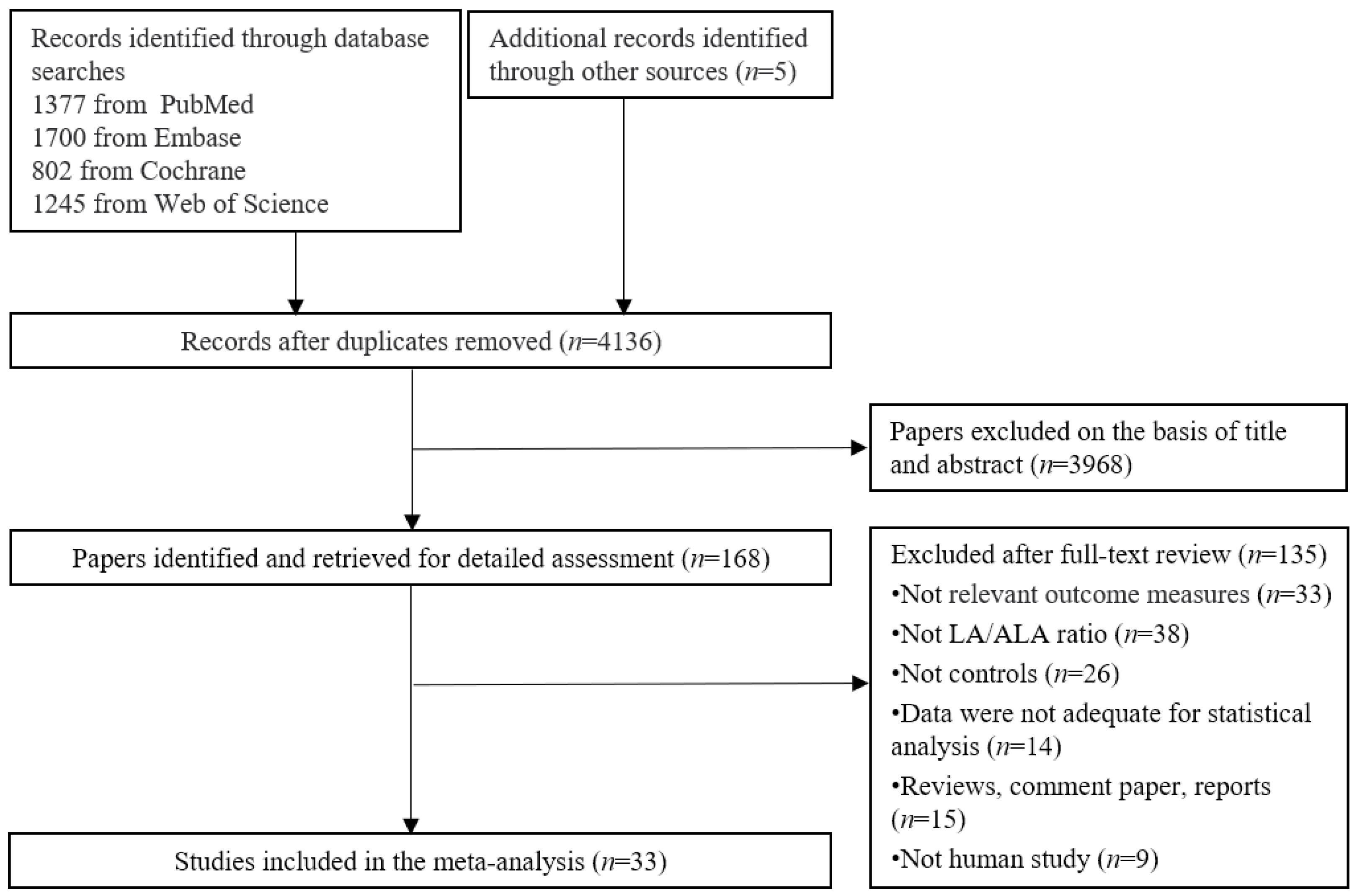
2.1. Search Strategy and Selection Studies
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Description of Studies
3.2. Quality Assessment
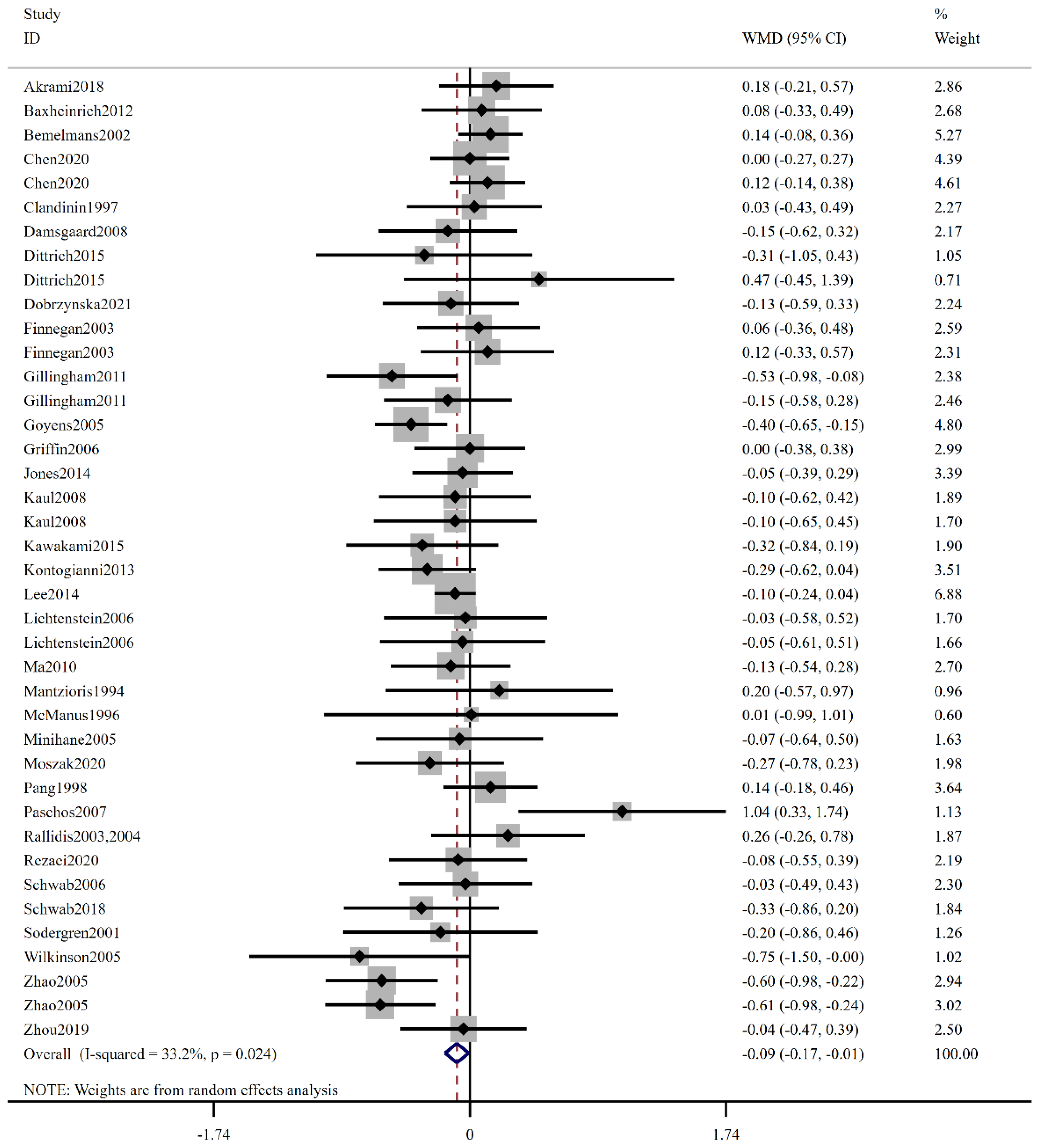
3.3. Effect of Low-Ratio Linoleic Acid/Alpha-Linolenic Acid on Blood Lipid Profiles
3.4. Publication Bias and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LA | Linoleic acid |
| ALA | Alpha-linolenic acid |
| RCTs | Randomized controlled trials |
| WMD | Weighted mean difference |
| CI | Confidence interval |
| TG | Triglycerides |
| TC | Total cholesterol |
| HDL-C | High-density lipoprotein cholesterol |
| LDL-C | Low-density lipoprotein cholesterol |
| CVD | Cardiovascular disease |
| PUFA | Polyunsaturated fatty acid |
| EPA | Eicosapentaenoic acid |
| DHA | Docosahexaenoic acid |
| CLA | Conjugated linoleic acid |
| BMI | Body mass index |
| SD | Standard deviations |
| MCFA | Medium-chain fatty acids |
| PPAR | Peroxisome proliferator-activated receptors |
| NF-κB | Nuclear factor-kappa B |
References
- Daar, A.S.; Singer, P.A.; Persad, D.L.; Pramming, S.K.; Matthews, D.R.; Beaglehole, R.; Bernstein, A.; Borysiewicz, L.K.; Colagiuri, S.; Ganguly, N.; et al. Grand challenges in chronic non-communicable diseases. Nature 2007, 450, 494–496. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Cardiovascular Diseases (CVDs). 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 14 July 2023).
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, L.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update A Report from the American Heart Association. Circulation 2017, 135, E146–E603. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendia, L.E.; Pirro, M.; Gotto, A.M., Jr.; Banach, M.; Atkin, S.L.; Majeed, M.; Sahebkar, A. Lipid-modifying activity of curcuminoids: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2019, 59, 1178–1187. [Google Scholar] [CrossRef]
- Perez-Martinez, P.; Garcia-Rios, A.; Delgado-Lista, J.; Perez-Jimenez, F.; Lopez-Miranda, J. Mediterranean Diet Rich in Olive Oil and Obesity, Metabolic Syndrome and Diabetes Mellitus. Curr. Pharm. Des. 2011, 17, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.H.Y.; Micha, R.; Mozaffarian, D. Dietary fats and cardiometabolic disease: Mechanisms and effects on risk factors and outcomes. Nat. Rev. Cardiol. 2019, 16, 581–601. [Google Scholar] [CrossRef]
- Rimm, E.B.; Appel, L.J.; Chiuve, S.E.; Djousse, L.; Engler, M.B.; Kris-Etherton, P.M.; Mozaffarian, D.; Siscovick, D.S.; Lichtenstein, A.H.; Council Lifestyle Cardiometab, H.; et al. Seafood Long-Chain n-3 Polyunsaturated Fatty Acids and Cardiovascular Disease: A Science Advisory from the American Heart Association. Circulation 2018, 138, E35–E47. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef]
- Brenna, J.T.; Salem, N., Jr.; Sinclair, A.J.; Cunnane, S.C.; ISSFAL. alpha-Linolenic acid supplementation and conversion to n-3 long-chain polyunsaturated fatty acids in humans. Prostaglandins Leukot. Essent. Fat. Acids 2009, 80, 85–91. [Google Scholar] [CrossRef]
- Li, N.; Jia, M.; Deng, Q.; Wang, Z.; Huang, F.; Hou, H.; Xu, T. Effect of low-ratio n-6/n-3 PUFA on blood lipid level: A meta-analysis. Horm.-Int. J. Endocrinol. Metab. 2020, 20, 697–706. [Google Scholar] [CrossRef]
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.; Summerbell, C.D.; Worthington, H.V.; Song, F.; et al. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2020, 3, 17. [Google Scholar] [CrossRef]
- Yue, H.; Qiu, B.; Jia, M.; Liu, W.; Guo, X.-F.; Li, N.; Xu, Z.-X.; Du, F.-L.; Xu, T.; Li, D. Effects of alpha-linolenic acid intake on blood lipid profiles:a systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 61, 2894–2910. [Google Scholar] [CrossRef]
- Takic, M.; Pokimica, B.; Petrovic-Oggiano, G.; Popovic, T. Effects of Dietary alpha-Linolenic Acid Treatment and the Efficiency of Its Conversion to Eicosapentaenoic and Docosahexaenoic Acids in Obesity and Related Diseases. Molecules 2022, 27, 4471. [Google Scholar] [CrossRef]
- Gillingham, L.G.; Gustafson, J.A.; Han, S.-Y.; Jassal, D.S.; Jones, P.J.H. High-oleic rapeseed (canola) and flaxseed oils modulate serum lipids and inflammatory biomarkers in hypercholesterolaemic subjects. Br. J. Nutr. 2011, 105, 417–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillingham, L.G.; Robinson, K.S.; Jones, P.J. Effect of high-oleic canola and flaxseed oils on energy expenditure and body composition in hypercholesterolemic subjects. Metab. Clin. Exp. 2012, 61, 1598–1605. [Google Scholar] [CrossRef]
- Nelson, T.L.; Stevens, J.R.; Hickey, M.S. Inflammatory markers are not altered by an eight week dietary alpha-linolenic acid intervention in healthy abdominally obese adult males and females. Cytokine 2007, 38, 101–106. [Google Scholar] [CrossRef] [PubMed]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Grp, P.-D. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies The PRISMA-DTA Statement. JAMA-J. Am. Med. Assoc. 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.T.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, 10. [Google Scholar] [CrossRef] [Green Version]
- Clandinin, M.T.; Foxwell, A.; Goh, Y.K.; Layne, K.; Jumpsen, J.A. Omega-3 fatty acid intake results in a relationship between the fatty acid composition of LDL cholesterol ester and LDL cholesterol content in humans. Biochim. Biophys. Acta. 1997, 1346, 247–252. [Google Scholar] [CrossRef]
- Damsgaard, C.T.; Frøkiær, H.; Andersen, A.D.; Lauritzen, L. Fish oil in combination with high or low intakes of linoleic acid lowers plasma triacylglycerols but does not affect other cardiovascular risk markers in healthy men. J. Nutr. 2008, 138, 1061–1066. [Google Scholar] [CrossRef] [Green Version]
- Goyens, P.L.L.; Mensink, R.P. The dietary α-linolenic acid to linoleic acid ratio does not affect the serum lipoprotein profile in humans. J. Nutr. 2005, 135, 2799–2804. [Google Scholar] [CrossRef] [Green Version]
- Griffin, M.D.; Sanders, T.A.; Davies, I.G.; Morgan, L.M.; Millward, D.J.; Lewis, F.; Slaughter, S.; Cooper, J.A.; Miller, G.J.; Griffin, B.A. Effects of altering the ratio of dietary n-6 to n-3 fatty acids on insulin sensitivity, lipoprotein size, and postprandial lipemia in men and postmenopausal women aged 45-70 y: The OPTILIP Study. Am. J. Clin. Nutr. 2006, 84, 1290–1298. [Google Scholar] [CrossRef] [Green Version]
- Kaul, N.; Kreml, R.; Austria, J.A.; Richard, M.N.; Edel, A.L.; Dibrov, E.; Hirono, S.; Zettler, M.E.; Pierce, G.N. A comparison of fish oil, flaxseed oil and hempseed oil supplementation on selected parameters of cardiovascular health in healthy volunteers. J. Am. Coll. Nutr. 2008, 27, 51–58. [Google Scholar] [CrossRef]
- Kawakami, Y.; Yamanaka-Okumura, H.; Naniwa-Kuroki, Y.; Sakuma, M.; Taketani, Y.; Takeda, E. Flaxseed oil intake reduces serum small dense low-density lipoprotein concentrations in Japanese men: A randomized, double blind, crossover study. Nutr. J. 2015, 14, 39. [Google Scholar] [CrossRef] [Green Version]
- Kontogianni, M.D.; Vlassopoulos, A.; Gatzieva, A.; Farmaki, A.E.; Katsiougiannis, S.; Panagiotakos, D.B.; Kalogeropoulos, N.; Skopouli, F.N. Flaxseed oil does not affect inflammatory markers and lipid profile compared to olive oil, in young, healthy, normal weight adults. Metab. Clin. Exp. 2013, 62, 686–693. [Google Scholar] [CrossRef]
- Mantzioris, E.; James, M.J.; Gibson, R.A.; Cleland, L.G. Dietary substitution with an α-linolenic acid-rich vegetable oil increases eicosapentaenoic acid concentrations in tissues. Am. J. Clin. Nutr. 1994, 59, 1304–1309. [Google Scholar] [CrossRef] [PubMed]
- Minihane, A.M.; Brady, L.M.; Lovegrove, S.S.; Lesauvage, S.V.; Williams, C.M.; Lovegrove, J.A. Lack of effect of dietary n-6: N-3 PUFA ratio on plasma lipids and markers of insulin responses in Indian Asians living in the UK. Eur. J. Nutr. 2005, 44, 26–32. [Google Scholar] [CrossRef]
- Pang, D.; Allman-Farinelli, M.A.; Wong, T.; Barnes, R.; Kingham, K.M. Replacement of linoleic acid with α-linolenic acid does not alter blood lipids in normolipidaemic men. Br. J. Nutr. 1998, 80, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Schwab, U.S.; Callaway, J.C.; Erkkilä, A.T.; Gynther, J.; Uusitupa, M.I.; Järvinen, T. Effects of hempseed and flaxseed oils on the profile of serum lipids, serum total and lipoprotein lipid concentrations and haemostatic factors. Eur. J. Nutr. 2006, 45, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, P.; Leach, C.; Ah-Sing, E.E.; Hussain, N.; Miller, G.J.; Millward, D.J.; Griffin, B.A. Influence of alpha-linolenic acid and fish-oil on markers of cardiovascular risk in subjects with an atherogenic lipoprotein phenotype. Atherosclerosis 2005, 181, 115–124. [Google Scholar] [CrossRef]
- Chen, C.G.; Wang, P.; Zhang, Z.Q.; Ye, Y.B.; Zhuo, S.Y.; Zhou, Q.; Chen, Y.M.; Su, Y.X.; Zhang, B. Effects of plant oils with different fatty acid composition on cardiovascular risk factors in moderately hypercholesteremic Chinese adults: A randomized, double-blinded, parallel-designed trial. Food Funct. 2020, 11, 7164–7174. [Google Scholar] [CrossRef] [PubMed]
- Dittrich, M.; Jahreis, G.; Bothor, K.; Drechsel, C.; Kiehntopf, M.; Blüher, M.; Dawczynski, C. Benefits of foods supplemented with vegetable oils rich in α-linolenic, stearidonic or docosahexaenoic acid in hypertriglyceridemic subjects: A double-blind, randomized, controlled trail. Eur. J. Nutr. 2015, 54, 881–893. [Google Scholar] [CrossRef] [PubMed]
- Dobrzyńska, M.A.; Przysławski, J. The effect of camelina oil (α-linolenic acid) and canola oil (oleic acid) on lipid profile, blood pressure, and anthropometric parameters in postmenopausal women. Arch. Med. Sci. AMS 2021, 17, 1566–1574. [Google Scholar] [CrossRef]
- Finnegan, Y.E.; Minihane, A.M.; Leigh-Firbank, E.C.; Kew, K.; Meijer, G.W.; Muggli, R.; Calder, P.C.; Williams, C.M. Plant- and marine-derived n-3 polyunsaturated fatty acids have differential effects on fasting and postprandial blood lipid concentrations and on the susceptibility of LDL to oxidative modification in moderately hyperlipidemic subjects. Am. J. Clin. Nutr. 2003, 77, 783–795. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, A.H.; Matthan, N.R.; Jalbert, S.M.; Resteghini, N.A.; Schaefer, E.J.; Ausman, L.M. Novel soybean oils with different fatty acid profiles alter cardiovascular disease risk factors in moderately hyperlipidemic subjects. Am. J. Clin. Nutr. 2006, 84, 497–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paschos, G.K.; Zampelas, A.; Panagiotakos, D.B.; Katsiougiannis, S.; Griffin, B.A.; Votteas, V.; Skopouli, F.N. Effects of flaxseed oil supplementation on plasma adiponectin levels in dyslipidemic men. Eur. J. Nutr. 2007, 46, 315–320. [Google Scholar] [CrossRef]
- Rallidis, L.S.; Paschos, G.; Liakos, G.K.; Velissaridou, A.H.; Anastasiadis, G.; Zampelas, A. Dietary α-linolenic acid decreases C-reactive protein, serum amyloid A and interleukin-6 in dyslipidaemic patients. Atherosclerosis 2003, 167, 237–242. [Google Scholar] [CrossRef]
- Sodergren, E.; Gustafsson, I.B.; Basu, S.; Nourooz-Zadeh, J.; Nalsen, C.; Turpeinen, A.; Berglund, L.; Vessby, B. A diet containing rapeseed oil-based fats does not increase lipid peroxidation in humans when compared to a diet rich in saturated fatty acids. Eur. J. Clin. Nutr. 2001, 55, 922–931. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Etherton, T.D.; Martin, K.R.; West, S.G.; Gillies, P.J.; Kris-Etherton, P.M. Dietary α-linolenic acid reduces inflammatory and lipid cardiovascular risk factors in hypercholesterolemic men and women. J. Nutr. 2004, 134, 2991–2997. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Q.; Zhang, Z.; Wang, P.; Zhang, B.; Chen, C.; Zhang, C.; Su, Y. EPA plus DHA, but not ALA, Improved Lipids and Inflammation Status in Hypercholesterolemic Adults: A Randomized, Double-Blind, Placebo-Controlled Trial. Mol. Nutr. Food Res. 2019, 63. [Google Scholar] [CrossRef]
- Lee, T.C.; Ivester, P.; Hester, A.G.; Sergeant, S.; Case, L.D.; Morgan, T.; Kouba, E.O.; Chilton, F.H. The impact of polyunsaturated fatty acid-based dietary supplements on disease biomarkers in a metabolic syndrome/diabetes population. Lipids Health Dis. 2014, 13, 196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Njike, V.Y.; Millet, J.; Dutta, S.; Doughty, K.; Treu, J.A.; Katz, D.L. Effects of walnut consumption on endothelial function in type 2 diabetic subjects: A randomized controlled crossover trial. Diabetes Care 2010, 33, 227–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McManus, R.M.; Jumpson, J.; Finegood, D.T.; Clandinin, M.T.; Ryan, E.A. A comparison of the effects of n-3 fatty acids from linseed oil and fish oil in well-controlled type II diabetes. Diabetes Care 1996, 19, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Schwab, U.S.; Lankinen, M.A.; de Mello, V.D.; Manninen, S.M.; Kurl, S.; Pulkki, K.J.; Laaksonen, D.E.; Erkkila, A.T. Camelina sativa oil, but not fatty fish or lean fish, improves serum lipid profile in subjects with impaired glucose metabolism—a randomized controlled trial. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef]
- Jones, P.J.; Senanayake, V.K.; Pu, S.; Jenkins, D.J.; Connelly, P.W.; Lamarche, B.; Couture, P.; Charest, A.; Baril-Gravel, L.; West, S.G.; et al. DHA-enriched high-oleic acid canola oil improves lipid profile and lowers predicted cardiovascular disease risk in the canola oil multicenter randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 88–97. [Google Scholar] [CrossRef] [Green Version]
- Moszak, M.; Zawada, A.; Juchacz, A.; Grzymislawski, M.; Bogdanski, P. Comparison of the effect of rapeseed oil or amaranth seed oil supplementation on weight loss, body composition, and changes in the metabolic profile of obese patients following 3-week body mass reduction program: A randomized clinical trial. Lipids Health Dis. 2020, 19, 143. [Google Scholar] [CrossRef]
- Akrami, A.; Nikaein, F.; Babajafari, S.; Faghih, S.; Yarmohammadi, H. Comparison of the effects of flaxseed oil and sunflower seed oil consumption on serum glucose, lipid profile, blood pressure, and lipid peroxidation in patients with metabolic syndrome. J. Clin. Lipidol. 2018, 12, 70–77. [Google Scholar] [CrossRef]
- Baxheinrich, A.; Stratmann, B.; Lee-Barkey, Y.H.; Tschoepe, D.; Wahrburg, U. Effects of a rapeseed oil-enriched hypoenergetic diet with a high content of α-linolenic acid on body weight and cardiovascular risk profile in patients with the metabolic syndrome. Br. J. Nutr. 2012, 108, 682–691. [Google Scholar] [CrossRef] [Green Version]
- Bemelmans, W.J.; Broer, J.; Feskens, E.J.; Smit, A.J.; Muskiet, F.A.; Lefrandt, J.D.; Bom, V.J.; May, J.F.; Meyboom-de Jong, B. Effect of an increased intake of alpha-linolenic acid and group nutritional education on cardiovascular risk factors: The Mediterranean Alpha-linolenic Enriched Groningen Dietary Intervention (MARGARIN) study. Am. J. Clin. Nutr. 2002, 75, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, S.; Reza Sasani, M.; Akhlaghi, M.; Kohanmoo, A. Flaxseed oil in the context of a weight loss programme ameliorates fatty liver grade in patients with non-alcoholic fatty liver disease: A randomised double-blind controlled trial. Br. J. Nutr. 2020, 123, 994–1002. [Google Scholar] [CrossRef]
- Helland, I.B.; Saugstad, O.D.; Saarem, K.; Van Houwelingen, A.C.; Nylander, G.; Drevon, C.A. Supplementation of n-3 fatty acids during pregnancy and lactation reduces maternal plasma lipid levels and provides DHA to the infants. J. Matern.-Fetal Neonatal Med. 2006, 19, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Egert, S.; Kannenberg, F.; Somoza, V.; Erbersdobler, H.F.; Wahrburg, U. Dietary α-linolenic acid, EPA, and DHA have differential effects on LDL fatty acid composition but similar effects on serum lipid profiles in normolipidemic humans. J. Nutr. 2009, 139, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.H.; Wang, J.; Zhang, R.X.; Zhang, Y.H.; Xu, Q.; Zhang, J.Y.; Zhang, Y.; Zheng, Z.X.; Yu, X.M.; Jing, H.J.; et al. A good response to oil with medium- and long-chain fatty acids in body fat and blood lipid profiles of male hypertriglyceridemic subjects. Asia Pac. J. Clin. Nutr. 2009, 18, 351–358. [Google Scholar]
- Umesha, S.S.; Naidu, K.A. Vegetable oil blends with alpha-linolenic acid rich Garden cress oil modulate lipid metabolism in experimental rats. Food Chem. 2012, 135, 2845–2851. [Google Scholar] [CrossRef]
- Skoczynska, A.H.; Gluza, E.; Wojakowska, A.; Turczyn, B.; Skoczynska, M. Linseed oil increases HDL3 cholesterol and decreases blood pressure in patients diagnosed with mild hypercholesterolaemia. Kardiol. Pol. 2018, 76, 1242–1250. [Google Scholar] [CrossRef] [Green Version]
- Nelson, T.L.; Stevens, J.R.; Hickey, M.S. Adiponectin levels are reduced, independent of polymorphisms in the adiponectin gene, after supplementation with alpha-linolenic acid among healthy adults. Metab. Clin. Exp. 2007, 56, 1209–1215. [Google Scholar] [CrossRef]
- Avelino, A.P.; Oliveira, G.M.; Ferreira, C.C.; Luiz, R.R.; Rosa, G. Additive effect of linseed oil supplementation on the lipid profiles of older adults. Clin. Interv. Aging 2015, 10, 1679–1685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harper, C.R.; Edwards, M.C.; Jacobson, T.A. Flaxseed oil supplementation does not affect plasma lipoprotein concentration or particle size in human subjects. J. Nutr. 2006, 136, 2844–2848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieters, D.J.; Mensink, R.P. Effects of stearidonic acid on serum triacylglycerol concentrations in overweight and obese subjects: A randomized controlled trial. Eur. J. Clin. Nutr. 2015, 69, 121–126. [Google Scholar] [CrossRef]
- Morise, A.; Serougne, C.; Gripois, D.; Blouquit, M.F.; Lutton, C.; Hermier, D. Effects of dietary alpha linolenic acid on cholesterol metabolism in male and female hamsters of the LPN strain. J. Nutr. Biochem. 2004, 15, 51–61. [Google Scholar] [CrossRef]
- Vijaimohan, K.; Jainu, M.; Sabitha, K.E.; Subramaniyam, S.; Anandhan, C.; Shyamala Devi, C.S. Beneficial effects of alpha linolenic acid rich flaxseed oil on growth performance and hepatic cholesterol metabolism in high fat diet fed rats. Life Sci. 2006, 79, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Fukumitsu, S.; Villareal, M.O.; Onaga, S.; Aida, K.; Han, J.; Isoda, H. alpha-Linolenic acid suppresses cholesterol and triacylglycerol biosynthesis pathway by suppressing SREBP-2, SREBP-1a and -1c expression. Cytotechnology 2013, 65, 899–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borniquel, S.; Jansson, E.A.; Cole, M.P.; Freeman, B.A.; Lundberg, J.O. Nitrated oleic acid up-regulates PPARgamma and attenuates experimental inflammatory bowel disease. Free Radic. Biol. Med. 2010, 48, 499–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, K.A.; Walker, C.L.; Xu, Z.; Whitley, P.; Pavlina, T.M.; Hise, M.; Zaloga, G.P.; Siddiqui, R.A. Oleic acid inhibits stearic acid-induced inhibition of cell growth and pro-inflammatory responses in human aortic endothelial cells. J. Lipid Res. 2010, 51, 3470–3480. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Zhang, H.; Jin, Q.; Wang, X. Effects of dietary linoleic acid on blood lipid profiles: A systematic review and meta-analysis of 40 randomized controlled trials. Foods 2023, 12, 2129. [Google Scholar] [CrossRef]
- Naghshi, S.; Aune, D.; Beyene, J.; Mobarak, S.; Asadi, M.; Sadeghi, O. Dietary intake and biomarkers of alpha linolenic acid and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of cohort studies. BMJ-Br. Med. J. 2021, 375. [Google Scholar] [CrossRef]
- Barre, D.E. The role of consumption of alpha-linolenic, eicosapentaenoic and docosahexaenoic acids in human metabolic syndrome and type 2 diabetes—A mini-review. J. Oleo Sci. 2007, 56, 319–325. [Google Scholar] [CrossRef] [Green Version]
- Sala-Vila, A.; Cofan, M.; Nunez, I.; Gilabert, R.; Junyent, M.; Ros, E. Carotid and femoral plaque burden is inversely associated with the alpha-linolenic acid proportion of serum phospholipids in Spanish subjects with primary dyslipidemia. Atherosclerosis 2011, 214, 209–214. [Google Scholar] [CrossRef]
- Alves-Bezerra, M.; Cohen, D.E. Triglyceride Metabolism in the Liver. Compr. Physiol. 2018, 8, 1–22. [Google Scholar] [CrossRef]
- Boren, J.; Taskinen, M.-R.; Bjornson, E.; Packard, C.J. Metabolism of triglyceride-rich lipoproteins in health and dyslipidaemia. Nat. Rev. Cardiol. 2022, 19, 577–592. [Google Scholar] [CrossRef]
- Haghikia, A.; Zimmermann, F.; Schumann, P.; Jasina, A.; Roessler, J.; Schmidt, D.; Heinze, P.; Kaisler, J.; Nageswaran, V.; Aigner, A.; et al. Propionate attenuates atherosclerosis by immune-dependent regulation of intestinal cholesterol metabolism. Eur. Heart J. 2022, 43, 518–533. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes: From molecules to man. Biochem. Soc. Trans. 2017, 45, 1105–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Participants Information | Age | BMI | Smoking | No. | M/F | Duration | Design | Low LA/ALA | High LA/ALA |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Akrami 2018 [48] | Iran | Metabolic syndrome | 48.6 | NR | Non-smoker | 52 | 33/19 | 7 W | P | 0.14 | 19.1 |
| Baxheinrich 2012 [49] | Germany | Metabolic syndrome | 51.3 | 34.3 | Non-smoker | 81 | 26/55 | 24 W | P | 3.12 | 10.89 |
| Bemelmans 2002 [50] | Netherlands | Cardiovascular | 54.1 | 29.8 | Mixed | 163 | 79/84 | 104 W | P | 4.7 | 29.1 |
| Chen 2020 [32] | China | Dyslipidaemia | 54.5 | 23.2 | Mixed | 243 | 92/151 | 48 W | P | 7.1 | 30 |
| 7.1 | 20 | ||||||||||
| Clandinin 1997 [20] | Canada | Healthy | 30.9 | Non-smoker | 26 | NR | 12 W | CO | 0.25 | 14.45 | |
| Damsgaard 2008 [21] | Denmark | Healthy | 25 | 23.2 | Mixed | 33 | 33/0 | 8 W | P | 4.7 | 7.72 |
| Dittrich 2015 [33] | Germany | Dyslipidaemia | 56 | 28.2 | NR | 49 | 17/32 | 10 W | CO | 0.42 | 71.43 |
| 0.74 | 71.43 | ||||||||||
| Dobrzynska 2021 [34] | Poland | Dyslipidaemia | 56.0 | 26.7 | Mixed | 60 | 0/60 | 6 W | P | 0.48 | 1.38 |
| Finnegan 2003 [35] | UK | Dyslipidaemia | 53.7 | 26.1 | Non-smoker | 60 | 35/25 | 24 W | P | 3.6 | 15.5 |
| 54.5 | 26.2 | 59 | 35/24 | 1.4 | 15.5 | ||||||
| Gillingham 2011 [15] | Canada | Dyslipidaemia | 47.5 | 28.6 | Non-smoker | 39 | 14/25 | 4 W | CO | 0.66 | 11.8 |
| 0.66 | 6 | ||||||||||
| Goyens 2005 [22] | Netherlands | Healthy | 49.6 | 24.1 | Mixed | 36 | 14/22 | 6 W | P | 7 | 19 |
| Griffin 2006 [23] | UK | Healthy | 59 | 26.3 | Mixed | 97 | 62/35 | 24 W | P | 4.64 | 14 |
| Jones 2014 [46] | Canada | Overweight or obese | 46.5 | 29.8 | Non-smoker | 130 | 60/70 | 4 W | CO | 1.17 | 231 |
| Kaul 2008 [24] | Canada | Healthy | 33.8 | 24.3 | Non-smoker | 44 | 17/27 | 12 W | P | 0.29 | 45.8 |
| 3.22 | 45.8 | ||||||||||
| Kawakami 2015 [25] | Japan | Healthy | 44.5 | 25.1 | Mixed | 15 | 15/0 | 12 W | CO | 1.34 | 9.8 |
| Kontogianni 2013 [26] | Greece | Healthy | 26 | 21.9 | NR | 37 | 8/29 | 6 W | CO | 1.4 | 8.3 |
| Lee 2014 [42] | USA | T2DM | 58.6 | 34.5 | Non-smoker | 43 | 18/25 | 8 W | P | 0.95 | 66 |
| Lichtenstein 2006 [36] | USA | Dyslipidaemia | 64 | 25.7 | Non-smoker | 14 | 14/0 | 7 W | CO | 8.7 | 18.3 |
| 61 | 26.7 | 16 | 0/16 | 8.7 | 18.3 | ||||||
| Ma 2010 [43] | USA | T2DM | 58.1 | 32.5 | Non-smoker | 24 | 10/14 | 8 W | P | 4.48 | 7.75 |
| Mantzioris 1994 [27] | Australia | Healthy | 35.3 | 25.4 | NR | 30 | 30/0 | 4 W | P | 0.62 | 19.5 |
| McManus 1996 [44] | Canada | T2DM | 61.8 | 27.8 | NR | 11 | 8/3 | 12 W | CO | 0.25 | 14.45 |
| Minihane 2005 [28] | India | Healthy | 48 | 26 | Non-smoker | 29 | NR | 6 W | P | 9 | 16 |
| Moszak 2020 [47] | Poland | Overweight or obese | 48.7 | 39.6 | Non-smoker | 52 | 20/32 | 3 W | P | 1.88 | 41.5 |
| Pang 1998 [29] | Australia | Healthy | 24.5 | 22.4 | NR | 29 | 29/0 | 6 W | P | 0.89 | 67 |
| Paschos 2007 [37] | Greece | Dyslipidaemia | 52 | 28 | Non-smoker | 35 | 35/0 | 12 W | P | 0.26 | 148 |
| Rallidis 2003 [38] | Greece | Dyslipidaemia | 51 | 28.4 | Mixed | 76 | 76/0 | 12 W | P | 1.3 | 13.2 |
| Rezaei 2020 [51] | Iran | Non-alcoholic fatty liver | 43.2 | 29.9 | Mixed | 68 | 33/35 | 12 W | P | 0.36 | 228.2 |
| Schwab 2006 [30] | USA | Healthy | 45 | 24.5 | NR | 14 | 8/6 | 4 W | CO | 0.245 | 2.45 |
| Schwab 2018 [45] | Finland | T2DM | 58.9 | 29.2 | NR | 79 | 40/39 | 12 W | P | 1.1 | 4.3 |
| Sodergren 2001 [39] | Sweden | Dyslipidaemia | 50 | 24.5 | Mixed | 19 | 13/6 | 4 W | CO | 3 | 10 |
| Wilkinson 2005 [31] | UK | Healthy | 49 | 28.3 | Non-smoker | 38 | NR | 12 W | P | 0.5 | 27.9 |
| Zhao 2005 [40] | USA | Dyslipidaemia | 49.8 | 28.1 | Non-smoker | 23 | 20/3 | 6 W | CO | 1.5 | 9 |
| 3.5 | 9 | ||||||||||
| Zhou 2019 [41] | China | Dyslipidaemia | 52.7 | 26 | Mixed | 75 | 39/36 | 12 W | P | 2.05 | 16.04 |
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessments | Incomplete Outcome Data | Selective Outcome Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Akrami 2018 | L | U | U | U | L | L | L |
| Baxheinrich 2012 | U | U | U | U | L | L | L |
| Bemelmans 2002 | L | L | L | U | L | U | L |
| Chen 2020 | L | L | L | U | L | U | L |
| Clandinin 1997 | L | U | L | L | L | U | L |
| Damsgaard 2008 | L | L | L | L | L | L | L |
| Dittrich 2015 | U | U | L | U | L | U | L |
| Dobrzynska 2021 | U | L | L | U | L | U | L |
| Finnegan 2003 | L | U | L | U | L | U | L |
| Gillingham 2011 | L | L | H | U | L | L | L |
| Goyens 2005 | U | U | L | U | L | U | L |
| Griffin 2006 | U | U | U | U | U | U | L |
| Jones 2014 | L | U | L | U | L | L | L |
| Kaul 2008 | L | U | L | U | U | U | L |
| Kawakami 2015 | U | U | L | U | L | U | L |
| Kontogianni 2013 | L | L | H | U | L | U | L |
| Lee 2014 | U | U | H | U | L | U | L |
| Lichtenstein 2006 | U | U | U | U | L | U | L |
| Ma 2010 | U | U | L | L | L | L | L |
| Mantzioris 1994 | U | U | U | U | L | U | L |
| McManus 1996 | L | U | L | L | L | U | L |
| Minihane 2005 | U | U | L | U | L | U | L |
| Moszak 2020 | U | U | L | L | L | U | L |
| Pang 1998 | U | U | U | U | U | U | L |
| Paschos 2007 | U | U | H | U | U | U | L |
| Rallidis 2003 | U | U | U | U | U | U | L |
| Rezaei 2020 | L | L | L | U | L | L | L |
| Schwab 2006 | U | U | L | U | U | U | L |
| Schwab 2018 | L | U | U | L | L | U | L |
| Sodergren 2001 | U | U | U | U | U | U | L |
| Wilkinson 2005 | U | U | H | U | U | U | L |
| Zhao 2005 | L | U | U | L | L | U | L |
| Zhou 2019 | U | U | L | U | L | L | L |
| TG | TC | HDL | LDL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subgroup | N | WMD (95% CI) | I2 % | N | WMD (95% CI) | I2 % | N | WMD (95% CI) | I2 % | N | WMD (95% CI) | I2 % |
| Low-ratio LA/ALA | ||||||||||||
| ≤1 | 16 | −0.04 (−0.13, 0.05) | 0.00 | 16 | −0.03 (−0.19, 0.13) | 32.6 | 16 | −0.01 (−0.05, 0.02) | 0.0 | 15 | 0.01 (−0.11, 0.12) | 0.0 |
| 1–5 | 18 | −0.04 (−0.10, 0.02) | 1.2 | 18 | −0.12 (−0.23, −0.01) | 34.6 | 18 | 0.00 (−0.03, 0.02) | 0.0 | 18 | −0.10 (−0.18, −0.02) | 8.3 |
| ≥5 | 6 | 0.05 (−0.21, 0.30) | 46.7 | 6 | −0.08 (−0.28, 0.11) | 45.4 | 6 | 0.04 (−0.02, 0.11) | 0.0 | 6 | −0.11 (−0.25, 0.04) | 5.4 |
| Region | ||||||||||||
| North America | 13 | −0.06 (−0.14, 0.02) | 0.0 | 13 | −0.21 (−0.33, −0.07) | 22.7 | 13 | −0.01 (−0.04, 0.02) | 0.0 | 13 | −0.14 (−0.23, −0.05) | 7.7 |
| Europe | 17 | −0.03 (−0.11, 0.05) | 11.8 | 17 | −0.06 (−0.22, 0.09) | 49.2 | 17 | 0.00 (−0.04, 0.03) | 0.0 | 16 | −0.07 (−0.16, 0.03) | 0.0 |
| Asia | 8 | 0.05 (−0.11, 0.20) | 0.0 | 8 | 0.02 (−0.12, 0.15) | 0.0 | 8 | 0.01 (−0.03, 0.05) | 0.0 | 8 | 0.01 (−0.13, 0.14) | 0.0 |
| Oceania | 2 | −0.12 (−0.27, 0.03) | 0.0 | 2 | 0.15 (−0.15, 0.45) | 0.0 | 2 | 0.05 (−0.08, 0.17) | 0.0 | 2 | 0.19 (−0.09, 0.46) | 0.0 |
| Health status | ||||||||||||
| Health | 13 | −0.08 (−0.15, −0.01) | 0.0 | 13 | −0.15 (−0.28, −0.03) | 8.0 | 13 | −0.01 (−0.05, 0.04) | 0.0 | 13 | −0.09 (−0.19, 0.02) | 0.0 |
| Dyslipidaemia | 17 | 0.04 (−0.07, 0.14) | 3.3 | 17 | −0.08 (−0.24, 0.09) | 55.4 | 17 | 0.01 (−0.03, 0.04) | 0.0 | 16 | −0.14 (−0.25, −0.03) | 5.9 |
| T2DM | 4 | −0.07 (−0.18, 0.04) | 0.0 | 4 | −0.12 (−0.24, 0.01) | 0.0 | 4 | 0.01 (−0.03, 0.05) | 0.0 | 4 | −0.13 (−0.24, −0.01) | 0.0 |
| Overweight or obese | 2 | −0.05 (−0.27, 0.16) | 0.0 | 2 | −0.12 (−0.40, 0.16) | 0.0 | 2 | −0.02 (−0.09, 0.04) | 0.0 | 2 | 0.00 (−0.21, 0.20) | 0.0 |
| Other | 4 | 0.00 (−0.19, 0.19) | 0.0 | 4 | 0.11 (−0.05, 0.27) | 0.0 | 4 | −0.01 (−0.05, 0.03) | 0.0 | 4 | 0.11 (−0.03, 0.25) | 0.0 |
| Age | ||||||||||||
| ≤45 | 20 | −0.09 (−0.15, −0.03) | 0.0 | 20 | −0.20 (−0.32, −0.09) | 32.3 | 20 | −0.01 (−0.04, 0.01) | 0.0 | 20 | −0.11 (−0.21, 0.02) | 25.0 |
| >45 | 20 | 0.01 (−0.06, 0.08) | 0.0 | 20 | 0.00 (−0.08, 0.08) | 0.0 | 20 | 0.01 (−0.02, 0.04) | 0.0 | 19 | −0.05 (−0.12, 0.03) | 0.0 |
| BMI | ||||||||||||
| ≤25 | 7 | −0.09 (−0.20, 0.02) | 34.0 | 7 | −0.10 (−0.28, 0.08) | 52.3 | 7 | 0.04 (−0.02, 0.09) | 0.3 | 7 | −0.01 (−0.26, 0.07) | 40.6 |
| 25–30 | 22 | 0.02 (−0.07, 0.10) | 0.0 | 22 | −0.10 (−0.24, 0.04) | 42.1 | 22 | −0.02 (−0.05, 0.02) | 0.0 | 21 | −0.11 (−0.20, −0.02) | 0.0 |
| ≥30 | 8 | 0.08 (−0.18, 0.02) | 0.0 | 8 | −0.12 (−0.23, 0.00) | 0.0 | 8 | 0.01 (−0.03, 0.05) | 5.1 | 8 | −0.11 (−0.21, −0.01) | 0.0 |
| NR | 3 | 0.06 (−0.09, 0.21) | 0.0 | 3 | 0.13 (−0.05, 0.31) | 0.0 | 3 | −0.02 (−0.06, 0.02) | 0.0 | 3 | 0.14 (−0.01, 0.30) | 0.0 |
| Smoking | ||||||||||||
| Non-smoker | 20 | −0.03 (−0.10, 0.04) | 0.0 | 20 | −0.12 (−0.25, 0.01) | 45.9 | 20 | −0.00 (−0.03, 0.02) | 0.0 | 19 | −0.09 (−0.17, −0.02) | 5.6 |
| Mixed | 13 | −0.01 (−0.11, 0.09) | 20.7 | 13 | −0.05 (−0.16, 0.07) | 22.2 | 13 | 0.00 (−0.04, 0.04) | 13.2 | 13 | −0.06 (−0.15, 0.04) | 0.2 |
| NR | 7 | −0.09 (−0.19, 0.01) | 0.0 | 7 | −0.08 (−0.28, 0.13) | 7.5 | 7 | 0.01 (−0.06, 0.08) | 0.0 | 7 | −0.03 (−0.20, 0.15) | 2.3 |
| Duration | ||||||||||||
| <12 W | 22 | −0.09 (−0.15, −0.04) | 0.0 | 22 | −0.18 (−0.28, −0.08) | 26.7 | 22 | 0.00 (−0.02, 0.02) | 0.0 | 22 | −0.13 (−0.21, −0.04) | 21.8 |
| ≥12 W | 18 | 0.06 (−0.02, 0.15) | 0.0 | 18 | 0.03 (−0.07, 0.14) | 9.4 | 18 | 0.00 (−0.03, 0.03) | 0.0 | 17 | 0.02 (−0.08, 0.11) | 0.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; Zhang, H.; Jin, Q.; Wang, X. Effects of Dietary Plant-Derived Low-Ratio Linoleic Acid/Alpha-Linolenic Acid on Blood Lipid Profiles: A Systematic Review and Meta-Analysis. Foods 2023, 12, 3005. https://doi.org/10.3390/foods12163005
Wang Q, Zhang H, Jin Q, Wang X. Effects of Dietary Plant-Derived Low-Ratio Linoleic Acid/Alpha-Linolenic Acid on Blood Lipid Profiles: A Systematic Review and Meta-Analysis. Foods. 2023; 12(16):3005. https://doi.org/10.3390/foods12163005
Chicago/Turabian StyleWang, Qiong, Hui Zhang, Qingzhe Jin, and Xingguo Wang. 2023. "Effects of Dietary Plant-Derived Low-Ratio Linoleic Acid/Alpha-Linolenic Acid on Blood Lipid Profiles: A Systematic Review and Meta-Analysis" Foods 12, no. 16: 3005. https://doi.org/10.3390/foods12163005
APA StyleWang, Q., Zhang, H., Jin, Q., & Wang, X. (2023). Effects of Dietary Plant-Derived Low-Ratio Linoleic Acid/Alpha-Linolenic Acid on Blood Lipid Profiles: A Systematic Review and Meta-Analysis. Foods, 12(16), 3005. https://doi.org/10.3390/foods12163005