
Nutrition Knowledge Varies by Food Group and Nutrient Among Adults


 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Recruitment
2.2. Survey Development
2.3. Food Group and Nutrient Knowledge Matrix
2.4. Data Analysis and Transformations
3. Results
3.1. National Sample Characteristics
3.2. Nutrition-Disease Knowledge Questions
3.3. Demographics, Health Conditions, Desired Benefits from Food
3.4. Predictors of the Nutrition-Disease Knowledge Score
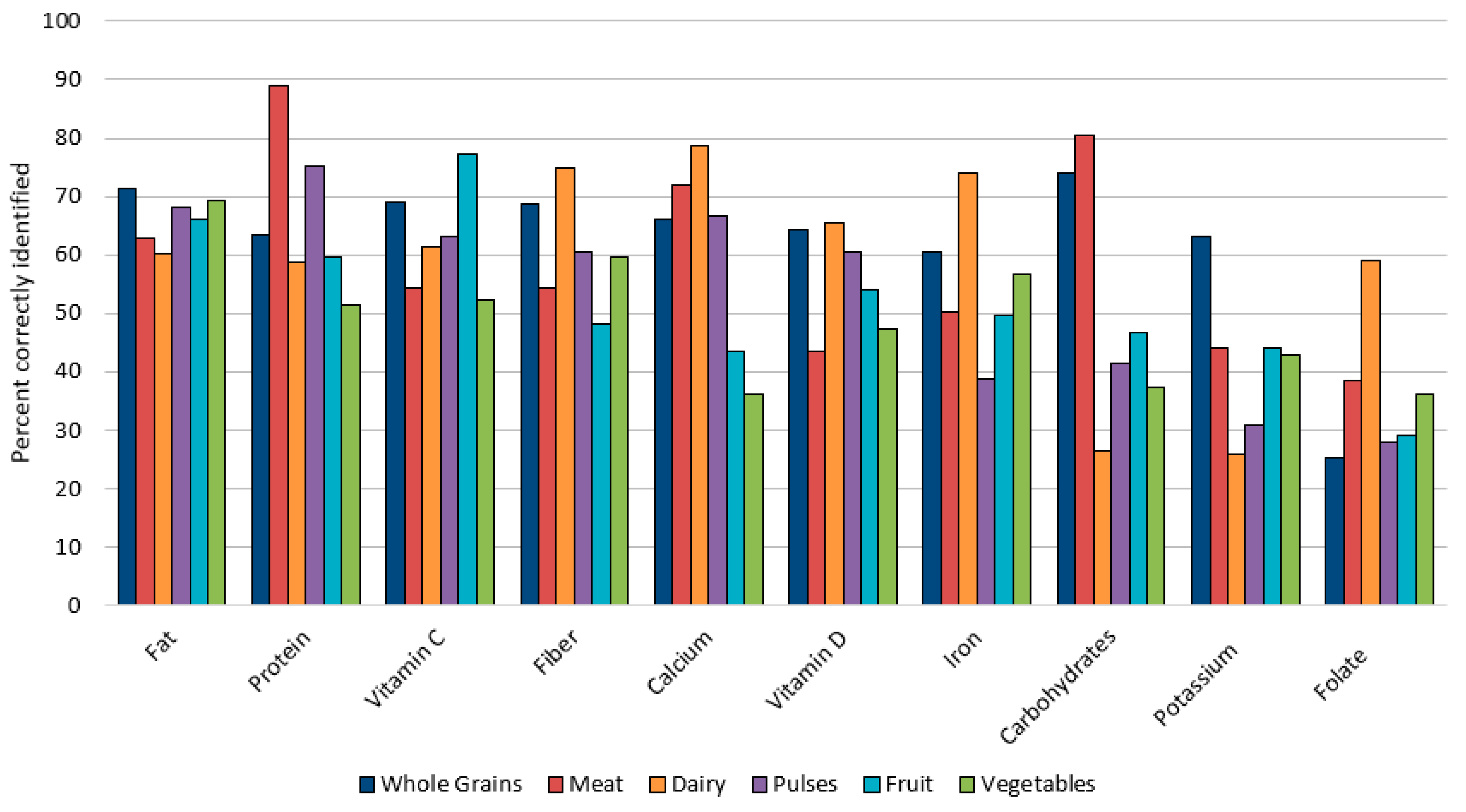
3.5. Food Group Nutrition Knowledge and Nutrient Source Awareness
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United States Department of Agriculture. Dietary Guidelines for Americans 2020–2025. USDA. 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf (accessed on 12 October 2023).
- Drewnowski, A. Defining nutrient density: Development and validation of the nutrient rich foods index. J. Am. Coll. Nutr. 2009, 28, 421S–426S. [Google Scholar] [CrossRef] [PubMed]
- Petroni, M.L.; Brodosi, L.; Marchignoli, F.; Sasdelli, A.S.; Caraceni, P.; Marchesini, G.; Ravaioli, F. Nutrition in Patients with Type 2 Diabetes: Present Knowledge and Remaining Challenges. Nutrients 2021, 13, 2748. [Google Scholar] [CrossRef]
- Polzonetti, V.; Pucciarelli, S.; Vincenzetti, S.; Polidori, P. Dietary intake of vitamin D from dairy products reduces the risk of osteoporosis. Nutrients 2020, 12, 1743. [Google Scholar] [CrossRef]
- Casas, R.; Castro-Barquero, S.; Estruch, R.; Sacanella, E. Nutrition and Cardiovascular Health. Int. J. Mol. Sci. 2018, 19, 3988. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.M.; Cordero, A.M.; Pfeiffer, C.M.; Hausman, D.B.; Tsang, B.L.; De-Regil, L.M.; Rosenthal, J.; Razzaghi, H.; Wong, E.C.; Weakland, A.P.; et al. Global folate status in women of reproductive age: A systematic review with emphasis on methodological issues. Ann. N. Y. Acad. Sci. 2018, 1431, 35–57. [Google Scholar] [CrossRef]
- Leonard, A.J.; Chalmers, K.A.; Collins, C.E.; Patterson, A.J. The effect of nutrition knowledge and dietary iron intake on iron status in young women. Appetite 2014, 81, 225–231. [Google Scholar] [CrossRef]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between nutrition knowledge and dietary intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef]
- Koch, F.; Hoffmann, I.; Claupein, E. Types of Nutrition Knowledge, Their Socio-Demographic Determinants and Their Association with Food Consumption: Results of the NEMONIT Study. Front. Nutr. 2021, 8, 630014. [Google Scholar] [CrossRef]
- Glick, A.A.; Winham, D.M.; Heer, M.M.; Shelley, M.C.; Hutchins, A.M. Health belief model predicts likelihood of eating nutrient-rich foods among US adults. Nutrients 2024, 16, 2335. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, X. How much of racial/ethnic disparities in dietary intakes, exercise, and weight status can be explained by nutrition- and health-related psychosocial factors and socioeconomic status among US adults? J. Am. Diet. Assoc. 2011, 111, 1904–1911. [Google Scholar] [CrossRef]
- VanKim, N.A.; Erickson, D.J.; Laska, M.N. Food shopping profiles and their association with dietary patterns: A latent class analysis. J. Acad. Nutr. Diet. 2015, 115, 1109–1116. [Google Scholar] [CrossRef]
- Dissen, A.R.; Policastro, P.; Quick, V.; Byrd-Bredbenner, C. Interrelationships Among Nutrition Knowledge, Attitudes, Behaviors and Body Satisfaction. Health Educ. 2011, 111, 283–295. [Google Scholar] [CrossRef]
- Ruxton, C.H.; Ruani, M.A.; Evans, C.E. Promoting and disseminating consistent and effective nutrition messages: Challenges and opportunities. Proc. Nutr. Soc. 2023, 82, 394–405. [Google Scholar] [CrossRef]
- Sapp, S.G.; Weng, C.Y. Examination of the health-belief model to predict the dietary quality and body mass of adults. Int. J. Consum. Stud. 2007, 31, 189–194. [Google Scholar] [CrossRef]
- Winham, D.M.; Jones, K.M. Knowledge of young African American adults about heart disease: A cross-sectional survey. BMC Public Health 2011, 11, 248. [Google Scholar] [CrossRef] [PubMed]
- Cerullo, G.; Negro, M.; Parimbelli, M.; Pecoraro, M.; Perna, S.; Liguori, G.; Rondanelli, M.; Cena, H.; D’Antona, G. The long history of vitamin C: From prevention of the common cold to potential aid in the treatment of COVID-19. Front. Immunol. 2020, 11, 574029. [Google Scholar] [CrossRef]
- Lin, C.T.J.; Yen, S.T. Knowledge of dietary fats among US consumers. J. Am. Diet. Assoc. 2010, 110, 613–618. [Google Scholar] [CrossRef]
- Quagliani, D.; Felt-Gunderson, P. Closing America’s Fiber Intake Gap. Am. J. Lifestyle Med. 2016, 11, 80–85. [Google Scholar] [CrossRef]
- Collins, C.B.; Winham, D.M.; Hutchins, A.M. Dietary intakes, attitudes toward carbohydrates of postmenopausal women following low carbohydrate diets. Can. J. Diet. Pract. Res. 2009, 70, 44–47. [Google Scholar] [CrossRef]
- Palmer, S.M.; Knoblauch, S.T.; Winham, D.M.; Hiller, M.B.; Shelley, M.C. Putting knowledge into practice: Low-income women talk about food choice decisions. Int. J. Environ. Res. Public Health 2020, 17, 5092. [Google Scholar] [CrossRef] [PubMed]
- Greszki, R.; Meyer, M.; Schoen, H. Exploring the effects of removing “too fast” responses and respondents from web surveys. Public Opin. Q. 2015, 79, 471–503. [Google Scholar] [CrossRef]
- Lin, C.T.; Zhang, Y.; Carlton, E.; Lo, S. 2014 FDA Health and Diet Survey Center for Food Safety and Applied Nutrition Food and Drug Administration. 2016. Available online: https://downloads.regulations.gov/FDA-2004-N-0258-0161/content.pdf (accessed on 20 October 2023).
- Green, S.H.; Glanz, K. Development of the Perceived Nutrition Environment Measures survey. Am. J. Prev. Med. 2015, 49, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.S.; Kaiser, L.L. Development of a Tool to Assess Psychosocial Indicators of Fruit and Vegetable Intake for 2 Federal Programs. J. Nutr. Educ. Behav. 2005, 37, 170–184. [Google Scholar] [CrossRef]
- Lando, A.; Verrill, L.; Wu, F. FSANS FDA’s Food Safety and Nutrition Survey 2019 Survey. 2021. Available online: https://www.fda.gov/media/146532/download?attachment (accessed on 4 March 2024).
- International Food Information Council Foundation (IFIC). 2023 Food and Health Survey. Available online: https://foodinsight.org/2023-food-and-health-survey/ (accessed on 4 March 2024).
- Jones, A.M.; Lamp, C.; Neelon, M.; Nicholson, Y.; Schneider, C.; Swanson, P.W.; Zidenberg-Cherr, S. Reliability and validity of nutrition knowledge questionnaire for adults. J. Nutr. Educ. Behav. 2015, 47, 69–74. [Google Scholar] [CrossRef]
- Food Labeling, 21 CFR §101. 2024. Available online: https://www.ecfr.gov/current/title-21/chapter-I/subchapter-B/part-101 (accessed on 20 October 2023).
- Carb Choices. Centers for Disease Control. Available online: https://www.cdc.gov/diabetes/healthy-eating/carbohydrate-lists-starchy-foods.html (accessed on 24 September 2023).
- United States Department of Agriculture, Food Data Central. Available online: https://fdc.nal.usda.gov/ (accessed on 20 October 2023).
- United States Department of Health & Human Services. National Institutes of Health. Office of Dietary Supplements. Dietary Supplement Fact Sheets. Available online: https://ods.od.nih.gov/factsheets/list-all/ (accessed on 20 October 2023).
- IBM. GLM Model. SPSS Statistics. 30 September 2024. Available online: https://www.ibm.com/docs/en/spss-statistics/saas?topic=analysis-glm-model (accessed on 21 January 2025).
- Laerd Statistics. Ordinal Logistic Regression Using SPSS Statistics. Statistical Tutorials and Software Guides. 2015. Available online: https://statistics.laerd.com/ (accessed on 10 October 2024).
- Winham, D.M.; Hutchins, A.M.; Thompson, S.V.; Dougherty, M.K. Arizona registered dietitians show gaps in knowledge of bean health benefits. Nutrients 2018, 10, 52. [Google Scholar] [CrossRef]
- US Census Bureau. Quick Facts. Population Estimates 1 July 2023. Available online: http://www.census.gov/quickfacts/fact/table/US/PST045222 (accessed on 12 November 2023).
- Kaiser Family Foundation. State Health Facts. Available online: https://www.kff.org/other/state-indicator/distribution-by-age/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed on 29 June 2024).
- Food and Nutrition Service. US Department of Agriculture. Available online: http://www.fns.usda.gov/cn/school-nutrition-standards-updates/whole-grains (accessed on 24 November 2024).
- Abderbwih, E.; Mahanani, M.R.; Deckert, A.; Antia, K.; Agbaria, N.; Dambach, P.; Kohler, S.; Horstick, O.; Winkler, V.; Wendt, A.S. The Impact of School-Based Nutrition Interventions on Parents and Other Family Members: A Systematic Literature Review. Nutrients 2022, 14, 2399. [Google Scholar] [CrossRef] [PubMed]
- Albertson, A.M.; Reicks, M.; Joshi, N.; Gugger, C.K. Whole grain consumption trends and associations with body weight measures in the United States: Results from the cross sectional National Health and Nutrition Examination Survey 2001–2012. Nutr. J. 2016, 15, 8. [Google Scholar] [CrossRef]
- Schupp, A.R.; Downer, R.; Gillespie, J.M.; Reed, D. Consumer Knowledge of Selected Nutrient Content of Nine Fresh Meat Cuts. J. Agribus. 1999, 17, 161–168. [Google Scholar] [CrossRef]
- Kennedy, J.; Alexander, P.; Taillie, L.S.; Jaacks, L.M. Estimated effects of reductions in processed meat consumption and unprocessed red meat consumption on occurrences of type 2 diabetes, cardiovascular disease, colorectal cancer, and mortality in the USA: A microsimulation study. Lancet Planet. Health 2024, 8, e441–e451. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Or, B.; Tsoi, M.F.; Cheung, C.L.; Cheung, B.M. Prevalence of metabolic syndrome in the United States National Health and Nutrition Examination Survey 2011–2018. Postgrad. Med. J. 2023, 99, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, X.; Wang, Z.; Bancks, M.P.; Carnethon, M.R.; Greenland, P.; Feng, Y.Q.; Wang, H.; Zhong, V.W. Trends in prevalence of diabetes and control of risk factors in diabetes among US adults, 1999–2018. Jama 2021, 326, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Han, C.Y.; Chan, C.G.B.; Lim, S.L.; Zheng, X.; Woon, Z.W.; Chan, Y.T.; Bhaskaran, K.; Tan, K.F.; Mangaikarasu, K.; Chong, M.F.-F. Diabetes-related nutrition knowledge and dietary adherence in patients with type 2 diabetes mellitus: A mixed-methods exploratory study. Proc. Singapore Healthc. 2020, 29, 81–90. [Google Scholar] [CrossRef]
- Breen, C.; Ryan, M.; Gibney, M.J.; O’Shea, D. Diabetes-related nutrition knowledge and dietary intake among adults with type 2 diabetes. Br. J. Nutr. 2015, 114, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Rebello, C.J.; Greenway, F.L.; Finley, J.W. Whole grains and pulses: A comparison of the nutritional and health benefits. J. Agric. Food Chem. 2014, 62, 7029–7049. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.M.; Moss, K.O.; Mitchell, J.; Still, C.; Hawkins, J.; Tang, E.; Wright, K.D. Challenges to dietary hypertension self-management as described by a sample of African American older adults. Worldviews Evid.-Based Nurs. 2022, 19, 64–72. [Google Scholar] [CrossRef]
- Bowman, S.A. Dietary Data Brief No. 46. Impact of Fruit and Vegetable Intakes on Food and Nutrient Intakes of Adults: What We Eat in America, NHANES 2017–2018. 2022 Oct. In FSRG Dietary Data Briefs [Internet]; United States Department of Agriculture (USDA): Beltsville, MD, USA, 2010. Available online: https://www.ncbi.nlm.nih.gov/books/NBK588577/ (accessed on 10 February 2025).
- Rounsefell, K.; Gibson, S.; McLean, S.; Blair, M.; Molenaar, A.; Brennan, L.; Truby, H.; McCaffrey, T.A. Social media, body image and food choices in healthy young adults: A mixed methods systematic review. Nutr. Diet. 2020, 77, 19–40. [Google Scholar] [CrossRef]
- Kowall, B.; Rathmann, W.; Stang, A.; Bongaerts, B.; Kuss, O.; Herder, C.; Roden, M.; Quante, A.; Holle, R.; Huth, C.; et al. Perceived risk of diabetes seriously underestimates actual diabetes risk: The KORA FF4 study. PLoS ONE 2017, 12, e0171152. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; O’Neill, S.M.; Rothrock, N.; Gramling, R.; Sen, A.; Acheson, L.S.; Rubinstein, W.S.; Nease, D.E., Jr.; Ruffin, I.V.M.T. Comparison of risk perceptions and beliefs across common chronic diseases. Prev. Med. 2009, 48, 197–202. [Google Scholar] [CrossRef]
- Siopis, G.; Colagiuri, S.; Allman-Farinelli, M. People with type 2 diabetes report dietitians, social support, and health literacy facilitate their dietary change. J. Nutr. Educ. Behav. 2021, 53, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Rofail, D.; Colligs, A.; Abetz, L.; Lindemann, M.; Maguire, L. Factors contributing to the success of folic acid public health campaigns. J. Public Health 2012, 34, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Improving Folic Acid Intake. Folic Acid. Published 17 May 2024. Available online: https://www.cdc.gov/folic-acid/health-equity/index.html (accessed on 24 November 2024).
- Sicinska, E.; Kubiak, K.; Madej, D.; Granda, D.; Kaluza, J. Main sources and predictive factors of folate intake in female university students. Nutrition 2024, 120, 112359. [Google Scholar] [CrossRef]
- Feyisa, J.W.; Siu, J.Y.M.; Bai, X. Effectiveness of Health Education Interventions in Enhancing Iron-Folic Acid Supplement Utilization Among Pregnant Women: Systematic Review and Meta-analysis. Nutr. Rev. 2024, nuae196. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, M.E.; Zhang, Z.; Carriquiry, A.L.; Gunn, J.P.; Kuklina, E.V.; Saydah, S.H.; Yang, Q.; Moshfegh, A.J. Sodium and potassium intakes among US adults: NHANES 2003–2008. Am. J. Clin. Nutr. 2012, 96, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Curtis, C.J.; Niederman, S.A.; Kansagra, S.M. Availability of potassium on the Nutrition Facts panel of US packaged foods. JAMA Intern. Med. 2013, 173, 828–829. [Google Scholar] [CrossRef]
- Johnson, S.A.; Kirkpatrick, C.F.; Miller, N.H.; Carson, J.A.S.; Handu, D.; Moloney, L. Saturated fat intake and the prevention and management of cardiovascular disease in adults: An Academy of Nutrition and Dietetics evidence-based nutrition practice guideline. J. Acad. Nutr. Diet. 2023, 123, 1808–1830. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, C.R.; Rose, D.J. US Consumer Identification of the Health Benefits of Dietary Fiber and Consideration of Fiber When Making Food Choices. Nutrients 2022, 14, 2341. [Google Scholar] [CrossRef]
- Heer, M.M.; Winham, D.M. Food behaviors, health, and bean nutrition awareness among low-income men: A pilot study. Int. J. Environ. Res. Public Health 2020, 17, 1039. [Google Scholar] [CrossRef] [PubMed]
- Winham, D.M. Culturally tailored foods and cardiovascular disease prevention. Am. J. Lifestyle Med. 2009, 3 (Suppl. S1), 64S–68S. [Google Scholar] [CrossRef]
- McLeod, M.R.; Chionis, L.; Gregg, B.; Gianchandani, R.; Wolfson, J.A. Knowledge and attitudes of lower Michigan primary care physicians towards dietary interventions: A cross-sectional survey. Prev. Med. Rep. 2022, 27, 101793. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.I.; Doerr, L.; Dworatzek, P.D.N. University Students Intend to Eat Better but Lack Coping Self-Efficacy and Knowledge of Dietary Recommendations. J. Nutr. Educ. Behav. 2016, 48, 12–19.e1. [Google Scholar] [CrossRef] [PubMed]
- Alhuthali, H.M.; Alzahrani, H.A.; Ataya, E.F.; Almehmadi, M.; Alsaiari, A.A.; Alrehaili, A.A.; Bakhuraysah, M.M.; Alsaeedi, F.A.; Alsalmi, O.; Altalhi, W.; et al. Enhancing knowledge and practices toward Vitamin D deficiency through implementing awareness programs among medical science female students. Eur. J. Inflamm. 2023, 21, 1721727X231223365. [Google Scholar] [CrossRef]

{kind=link}
| Variables Included in All Food Group and Nutrient General Linear Models | |
| Continuous | Age, nutrition-disease knowledge score, years of education, self-reported health status, self-reported dietary quality |
| Binomial | Gender, children in household, race, nutrition-related disease condition, marital status, vitamin use, main shopper, main food preparer |
| Food Group and Nutrient Additional Variables: | |
| Pulses | Increasing fiber, folate, protein, seeking diabetes management and cardiovascular disease (CVD) benefits |
| Whole Grains | Increasing fiber and seeking digestive health benefits |
| Fruit | Increasing fiber, folate, vitamin C, potassium, decreasing sugar and carbohydrates |
| Vegetables | Increasing, fiber, folate, vitamin C, potassium, and iron |
| Dairy | Increasing vitamin D, calcium, and seeking bone health benefits |
| Meat | Increasing protein and decreasing saturated fat and cholesterol |
| Carbohydrates | Weight loss management, diabetes management, limiting carbohydrates, and limiting sugar |
| Fat | Weight loss management, diabetes management, limiting carbohydrates, limiting cholesterol, limiting saturated fat, and increasing protein |
| Protein | Weight loss management, diabetes management, limiting cholesterol, limiting saturated fat, and limiting calories |
| Fiber | Weight loss management, diabetes management, increasing fiber, seeking CVD benefits, and digestive benefits |
| Iron | Increasing iron and seeking energy benefits |
| Calcium | Increasing calcium and seeking bone health benefits |
| Vitamin C | Increasing vitamin C |
| Folate | Increasing folate |
| Vitamin D | Increasing vitamin D and seeking bone health benefits |
| Potassium | Increasing potassium and seeking bone health benefits |
| Total (n = 930) | Nutrition-Disease knowledge Score 0–3 (47.5%; 442) | Nutrition-Disease Knowledge Score 4–7 (52.5%; 488) | p | |
|---|---|---|---|---|
 % %  | ||||
| Eating less salt protects against heart disease Yes—Correct No Not sure | 79.1 8.2 12.7 | 64.9 a 13.8 a 21.3 a | 92.0 b 3.1 b 4.9 b | <0.001 |
| Eating more fiber protects against heart disease Yes—Correct No Not sure | 63.7 8.7 27.6 | 43.7 a 14.7 a 41.6 a | 81.8 b 3.3 b 15.0 b | <0.001 |
| Eating more meat protects against heart disease No—Correct Yes Not sure | 60.6 19.2 20.1 | 33.7 a 32.6 a 33.7 a | 85.0 b 7.2 b 7.8 b | <0.001 |
| Item in foods that raises blood cholesterol level Saturated fats—Correct Cholesterol in the diet Polyunsaturated fats Antioxidants Not sure | 46.2 24.6 14.8 4.8 9.5 | 21.3 a 34.8 a 18.8 a 8.4 a 16.7 a | 68.9 b 15.4 b 11.3 b 1.6 b 2.9 b | <0.001 |
| Not eating fruits/vegetables can cause disease True—Correct False | 43.9 56.1 | 23.5 a 76.5 a | 62.3 b 37.7 b | <0.001 |
| Nutrient that helps prevent neural tube defects Folic acid or folate—Correct Iron Vitamin A Vitamin D Not sure | 37.3 9.1 9.1 8.7 35.7 | 16.3 a 13.3 a 15.1 a 13.8 a 41.5 a | 56.4 b 5.5 b 3.7 b 4.1 b 30.3 b | <0.001 |
| Item that has the most calories 1 g of fat—Correct 1 g of sugar 1 g of protein 1 g of fiber Not sure | 29.0 38.3 8.9 4.8 18.9 | 14.0 a 39.4 a 14.3 a 8.6 a 23.8 a | 42.6 b 37.3 a 4.1 b 1.4 b 14.5 b | <0.001 |
| Summary score ( ± SD) | 3.61 ± 1.6 | 2.19 ± 0.9 | 4.90 ± 0.9 | <0.001 |
| Total (n = 930) | Nutrition-Disease Knowledge Score 0–3 (47.5%; 442) | Nutrition-Disease Knowledge Score 4–7 (52.5%; 488) | p | |
|---|---|---|---|---|
 mean ± standard deviation mean ± standard deviation  | ||||
| Age in years | 45.1 ± 14.4 | 41.8 ± 13.6 | 48.1 ± 14.4 | <0.001 |
| Total household size | 3.1 ± 1.4 | 3.4 ± 1.3 | 2.9 ± 1.3 | 0.001 |
 % %  | ||||
| Gender Men Women | 48.7 51.3 | 54.5 a 45.5 a | 43.4 b 56.6 b | <0.001 |
| Marital Status Single/Divorced/Widowed Married/Living w/partner | 28.6 70.4 | 29.6 70.4 | 27.7 72.3 | 1 n.s. |
| Children in household No children One child+ in household | 49.2 50.8 | 41.4 a 58.6 a | 56.4 b 43.6 b | <0.001 |
| Race/Ethnicity Other White | 23.2 76.8 | 25.8 74.2 | 20.9 79.1 | n.s. |
| Years of Education 9–12th grade and/or GED Some college, no degree Associates degree, Tech school Bachelor’s degree Masters, Doctoral, Professional degree | 14.5 13.7 13.8 32.5 25.5 | 17.0 12.2 12.4 32.8 25.6 | 12.3 15.2 15.0 32.2 25.4 | n.s. |
| Self-reported health Poor–Fair Good Very good Excellent | 17.1 42.7 28.9 11.3 | 15.6 a 41.2 a 26.9 a 16.3 a | 18.4 a 44.1 a 30.7 a 6.8 b | <0.001 |
| Self-reported diet quality Poor–Fair Good Very good Excellent | 21.1 42.2 26.1 10.6 | 19.5 a 39.1 a 25.3 a 16.1 a | 22.5 a 44.9 a 26.8 a 5.7 b | <0.001 |
| Vitamin and/or supplement use No Yes | 23.5 76.5 | 23.1 76.9 | 24.0 76.0 | n.s. |
| Main food shopper No Yes | 25.7 74.3 | 26.5 73.5 | 25.0 75.0 | n.s. |
| Main food preparer No Yes | 42.8 57.2 | 43.4 56.6 | 42.2 57.8 | n.s. |
| Total | Nutrition-Disease Knowledge 0–3 (47.5%; 442) | Nutrition-Disease Knowledge 4–7 (52.5%; 488) | p | |
|---|---|---|---|---|
 % %  | ||||
| Binomial nutrition-related disease presence No Yes | 44.4 55.6 | 45.5 54.5 | 43.4 56.6 | 1 n.s. |
| Nutrition-related disease conditions High blood pressure High cholesterol Diabetes Gastrointestinal disorder Heart disease | 29.8 25.4 17.7 14.7 6.5 | 28.3 25.3 19.7 10.2 a 7.9 | 31.1 25.4 16.0 18.9 b 5.1 | n.s. n.s. n.s. <0.001 n.s. |
| Health benefits wanted from foods Weight loss or management Digestive or gut health Heart/cardiovascular health Bone health Diabetes or blood sugar management None of these | 49.4 49.9 40.3 35.3 24.7 9.8 | 45.9 a 41.2 a 33.3 a 36.0 21.9 12.7 a | 52.5 b 57.8 b 46.7 b 34.6 27.3 7.2 b | 0.049 <0.001 <0.001 n.s. n.s. 0.006 |
| Trying to limit or eat less nutrients Sugar Carbohydrates Sodium Saturated fat Calories Cholesterol No, not limiting any nutrients | 54.9 37.2 36.5 32.2 34.1 31.9 13.8 | 45.9 a 37.3 33.7 28.3 a 34.6 33.9 14.3 | 63.1 b 37.1 38.9 35.7 b 33.6 30.1 13.3 | <0.001 n.s. n.s. 0.017 n.s. n.s. n.s. |
| Trying to eat more nutrients Protein Fiber Vitamin D Vitamin C Calcium Iron Potassium Folate No, not increasing any nutrients | 45.5 40.8 42.5 39.2 29.7 25.9 19.7 13.0 16.9 | 38.5 a 31.9 a 43.7 42.8 a 30.5 27.8 19.5 12.0 18.7 | 51.8 b 48.8 b 41.4 36.1 b 28.9 24.2 19.9 13.9 15.2 | <0.001 <0.001 n.s. 0.037 n.s. n.s. n.s. n.s. n.s. |
| Variable | Beta (p-Value) | Partial Eta Squared | Observed Power |
|---|---|---|---|
| Age | 0.023 (<0.001) | 0.045 | >0.999 |
| Education | 0.162 (<0.001) | 0.020 | 0.991 |
| Seeking cardiovascular disease benefits | 0.490 (<0.001) | 0.022 | 0.996 |
| Increasing fiber | 0.494 (<0.001) | 0.023 | 0.997 |
| Limiting cholesterol | −0.364 (0.001) | 0.011 | 0.904 |
| Self-reported health status | −0.181 (0.001) | 0.011 | 0.893 |
| Gender (woman) | 0.249 (0.014) | 0.006 | 0.689 |
| Whole Grains | Meat | Dairy | Pulses | Fruit | Vegetables | Nutrient-Source Score | |
|---|---|---|---|---|---|---|---|
| ± SD | |||||||
| FAT | 3.98 ± 1.51 | ||||||
| Nutrient source | No | Yes | Yes | No | No | No | |
| % Correct | 71.3 | 62.7 | 60.2 | 68.1 | 66.0 | 69.2 | |
| % Not sure | 7.7 | 3.1 | 2.7 | 9.1 | 22.7 | 19.4 | |
| PROTEIN | 3.97 ± 1.42 | ||||||
| Nutrient source | No | Yes | Yes | Yes | No | No | |
| % Correct | 63.5 | 88.9 | 58.8 | 75.1 | 59.6 | 51.4 | |
| % Not sure | 7.7 | 3.1 | 2.7 | 9.1 | 22.7 | 19.4 | |
| VITAMIN C | 3.78 ± 1.57 | ||||||
| Nutrient source | No | No | No | No | Yes | Yes | |
| % Correct | 68.9 | 54.4 | 61.5 | 63.2 | 77.3 | 52.4 | |
| % Not sure | 16.2 | 29.8 | 16.0 | 20.3 | 7.2 | 12.2 | |
| FIBER | 3.66 ± 1.70 | ||||||
| Nutrient source | Yes | No | No | Yes | Yes | Yes | |
| % Correct | 68.6 | 54.3 | 74.8 | 60.5 | 48.1 | 59.6 | |
| % Not sure | 16.2 | 29.8 | 16.0 | 20.3 | 7.2 | 12.2 | |
| CALCIUM | 3.63 ± 1.46 | ||||||
| Nutrient source | No | No | Yes | No | No | No | |
| % Correct | 66.2 | 71.9 | 78.8 | 66.6 | 43.5 | 36.1 | |
| % Not sure | 7.7 | 3.1 | 2.7 | 9.1 | 22.7 | 19.4 | |
| VITAMIN D | 3.35 ± 1.61 | ||||||
| Nutrient source | No | No | Yes | No | No | No | |
| % Correct | 64.4 | 43.5 | 65.4 | 60.6 | 53.9 | 47.3 | |
| % Not sure | 16.2 | 29.8 | 16.0 | 20.3 | 7.2 | 12.2 | |
| IRON | 3.30 ± 1.25 | ||||||
| Nutrient source | No | Yes | No | Yes | No | Yes | |
| % Correct | 60.6 | 50.3 | 74.0 | 38.8 | 49.7 | 56.6 | |
| % Not sure | 7.7 | 3.1 | 2.7 | 9.1 | 22.7 | 19.4 | |
| CARBOHYDRATES | 3.06 ± 1.58 | ||||||
| Nutrient source | Yes | No | Yes | Yes | Yes | Yes | |
| % Correct | 73.9 | 80.3 | 26.5 | 41.4 | 46.7 | 37.3 | |
| % Not sure | 7.7 | 3.1 | 2.7 | 9.1 | 22.7 | 19.4 | |
| POTASSIUM | 2.50 ± 1.38 | ||||||
| Nutrient source | No | No | Yes | Yes | Yes | Yes | |
| % Correct | 63.0 | 44.0 | 25.8 | 30.8 | 44.1 | 42.9 | |
| % Not sure | 16.2 | 29.8 | 16.0 | 20.3 | 7.2 | 12.2 | |
| FOLATE | 2.16 ± 1.37 | ||||||
| Nutrient source | Yes | No | No | Yes | Yes | Yes | |
| % Correct | 25.2 | 38.6 | 58.9 | 27.8 | 29.1 | 36.1 | |
| % Not sure | 16.2 | 29.8 | 16.0 | 20.3 | 7.2 | 12.2 | |
| FOOD GROUP SCORE ± SD | 6.26 ± 2.51 | 5.89 ± 2.26 | 5.85 ± 2.15 | 5.33 ± 2.30 | 5.15 ± 2.51 | 4.89 ± 2.30 |
| Nutrient Knowledge Score | Beta (p Value) | Partial Eta Squared | Observed Power | Adjusted R2 |
|---|---|---|---|---|
| PULSES | 0.194 | |||
| Nutrition-Disease Knowledge | 0.479 (<0.001) | 0.119 | >0.999 | |
| Increasing Fiber | 0.575 (<0.001) | 0.016 | 0.974 | |
| Nutrition-Related Condition | 0.415 (0.003) | 0.010 | 0.852 | |
| Gender | 0.388 (0.005) | 0.008 | 0.796 | |
| Main Meal Preparer | 0.344 (0.014) | 0.007 | 0.691 | |
| Increasing Protein | 0.309 (0.031) | 0.005 | 0.580 | |
| VEGETABLES | ||||
| Nutrition-Disease Knowledge | 0.452 (<0.001) | 0.104 | >0.999 | 0.162 |
| Education | 0.235 (<0.001) | 0.023 | 0.997 | |
| Increasing Fiber | 0.505 (0.001) | 0.013 | 0.932 | |
| Increasing Potassium | 0.447 (0.012) | 0.007 | 0.713 | |
| FRUIT | ||||
| Nutrition-Disease Knowledge | 0.490 (<0.001) | 0.099 | >0.999 | 0.145 |
| Education | 0.154 (0.006) | 0.008 | 0.789 | |
| Trying to limit sugar | 0.387 (0.015) | 0.006 | 0.686 | |
| Trying to increase fiber | 0.388 (0.016) | 0.006 | 0.673 | |
| Main meal preparer | 0.325 (0.0360 | 0.005 | 0.557 | |
| DAIRY | ||||
| Nutrition-Disease Knowledge | 0.432 (<0.001) | 0.110 | >0.999 | 0.140 |
| Seeking Bone Health Benefits | 0.519 (<0.001) | 0.015 | 0.960 | |
| Race/Ethnicity | 0.579 (<0.001) | 0.015 | 0.961 | |
| Self-Reported Diet Quality | 0.149 (0.034) | 0.005 | 0.563 | |
| WHOLE GRAINS | ||||
| Nutrition-Disease Knowledge | 0.440 (<0.001) | 0.081 | >0.999 | 0.102 |
| Has Children in the Household | 0.387 (0.015) | 0.006 | 0.681 | |
| Nutrition-Related Disease | 0.373 (0.018) | 0.006 | 0.654 | |
| Self-reported health status | −0.197 (0.023) | 0.006 | 0.624 | |
| MEAT | ||||
| Nutrition-Disease Knowledge | 0.392 (<0.001) | 0.075 | >0.999 | 0.077 |
| Age | −0.014 (0.005) | 0.008 | 0.796 | |
| Marital status | 0.392 (0.013) | 0.007 | 0.698 |
| Food Group Macronutrient Knowledge Score | Beta (p Value) | Partial Eta Squared | Observed Power | Adjusted R2 |
|---|---|---|---|---|
| FIBER | 0.271 | |||
| Nutrition-disease knowledge | 0.410 (<0.001) | 0.158 | >0.999 | |
| Digestive benefits | 0.359 (<0.001) | 0.014 | 0.948 | |
| Age | 0.011 (0.002) | 0.011 | 0.882 | |
| Increasing fiber | 0.326 (0.001) | 0.011 | 0.892 | |
| Interested in weight loss | 0.271 (0.005) | 0.008 | 0.794 | |
| Children in the household | −0.255 (0.012) | 0.007 | 0.713 | |
| CARBOHYDRATES | 0.230 | |||
| Nutrition-disease knowledge | 0.352 (<0.001) | 0.140 | >0.999 | |
| Education | 0.139 (<0.001) | 0.018 | 0.984 | |
| Interested in weight loss | 0.385 (<0.001) | 0.018 | 0.983 | |
| Race | 0.437 (<0.001) | 0.017 | 0.980 | |
| Children in the household | −0.352 (<0.001) | 0.015 | 0.966 | |
| Eating fewer carbohydrates | 0.261 (0.008) | 0.008 | 0.759 | |
| PROTEIN | 0.155 | |||
| Nutrition-disease knowledge | 0.274 (<0.001) | 0.095 | >0.999 | |
| Age | −0.12 (<0.001) | 0.014 | 0.951 | |
| Trying to increase protein | 0.342 (<0.001) | 0.016 | 0.970 | |
| Children in the household | −0.318 (0.001) | 0.011 | 0.895 | |
| Education | 0.101 (0.002) | 0.010 | 0.876 | |
| Limiting cholesterol | −0.221 (0.020) | 0.006 | 0.641 | |
| Marital status (married) | 0.233 (0.026) | 0.005 | 0.603 | |
| Interested in weight loss | 0.174 (0.046) | 0.004 | 0.514 | |
| FAT | 0.106 | |||
| Nutrition-disease knowledge | 0.263 (<0.001) | 0.079 | >0.999 | |
| Education | 0.088 (0.014) | 0.006 | 0.689 | |
| Nutrition-related disease | −0.226 (0.018) | 0.006 | 0.661 | |
| Children in the household | −0.189 (0.049) | 0.004 | 0.505 | |
| Self-reported health status | −0.104 (0.053) | 0.004 | 0.490 | |
| Interested in weight loss | 0.153 (0.105) | 0.003 | 0.368 |
| Food Group Micronutrient Knowledge Score | Beta (p Value) | Partial Eta Squared | Observed Power | Adjusted R2 |
|---|---|---|---|---|
| VITAMIN C | 0.183 | |||
| Nutrition-disease knowledge | 0.399 (<0.001) | 0.171 | >0.999 | |
| Gender | 0.249 (<0.001) | 0.008 | 0.754 | |
| FOLATE | 0.121 | |||
| Nutrition-disease knowledge | 0.207 (<0.001) | 0.063 | >0.999 | |
| Self-reported Diet Quality | 0.174 (<0.001) | 0.015 | 0.966 | |
| Trying to increase Folate | 0.508 (<0.001) | 0.017 | 0.977 | |
| Children in the Household | 0.260 (0.001) | 0.010 | 0.847 | |
| Nutrition Related Condition | 0.229 (0.002) | 0.008 | 0.759 | |
| Main Meal Preparer | 0.200 (0.020) | 0.006 | 0.631 | |
| POTASSIUM | 0.105 | |||
| Nutrition-disease knowledge | 0.219 (<0.001) | 0.067 | >0.999 | |
| Increasing Potassium | 0.417 (<0.001) | 0.016 | 0.968 | |
| Seeking Bone Health Benefits | 0.267 (0.003) | 0.009 | 0.833 | |
| Education | 0.082 (0.010) | 0.007 | 0.734 | |
| Children in the Household | 0.189 (0.030) | 0.005 | 0.581 | |
| IRON | 0.081 | |||
| Nutrition-disease knowledge | 0.178 (<0.001) | 0.053 | >0.999 | |
| Seeking Energy Benefits | 0.226 (0.005) | 0.009 | 0.804 | |
| Education | 0.061 (0.035) | 0.005 | 0.560 | |
| Main Meal Preparer | 0.154 (0.054) | 0.004 | 0.486 | |
| Race (White) | 0.181 (0.055) | 0.004 | 0.458 | |
| VITAMIN D | 0.077 | |||
| Nutrition-disease knowledge | 0.265 (<0.001) | 0.072 | >0.999 | |
| Self-reported Diet Quality | −0.115 (0.031) | 0.005 | 0.577 | |
| CALCIUM | 0.047 | |||
| Nutrition-disease knowledge | 0.123 (<0.001) | 0.018 | 0.985 | |
| Increasing Calcium | −0.384 (<0.001) | 0.015 | 0.959 | |
| Children in the Household | 0.343 (<0.001) | 0.013 | 0.931 | |
| Age | −0.008 (0.021) | 0.006 | 0.636 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glick, A.A.; Winham, D.M.; Heer, M.M.; Hutchins, A.M.; Shelley, M.C. Nutrition Knowledge Varies by Food Group and Nutrient Among Adults. Foods 2025, 14, 606. https://doi.org/10.3390/foods14040606
Glick AA, Winham DM, Heer MM, Hutchins AM, Shelley MC. Nutrition Knowledge Varies by Food Group and Nutrient Among Adults. Foods. 2025; 14(4):606. https://doi.org/10.3390/foods14040606
Chicago/Turabian StyleGlick, Abigail A., Donna M. Winham, Michelle M. Heer, Andrea M. Hutchins, and Mack C. Shelley. 2025. "Nutrition Knowledge Varies by Food Group and Nutrient Among Adults" Foods 14, no. 4: 606. https://doi.org/10.3390/foods14040606
APA StyleGlick, A. A., Winham, D. M., Heer, M. M., Hutchins, A. M., & Shelley, M. C. (2025). Nutrition Knowledge Varies by Food Group and Nutrient Among Adults. Foods, 14(4), 606. https://doi.org/10.3390/foods14040606