Impact of Pre-Processed Chickpea Flour Incorporation into “Mankoushe” on Appetite Hormones and Scores


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Test Meals
2.3. Experimental Protocol
2.4. Collection and Preparation of Blood Samples
2.5. Biochemical Analysis
2.6. Subjective Appetite Rating and Food Intake
2.7. Statistical Analysis
3. Results and Discussion
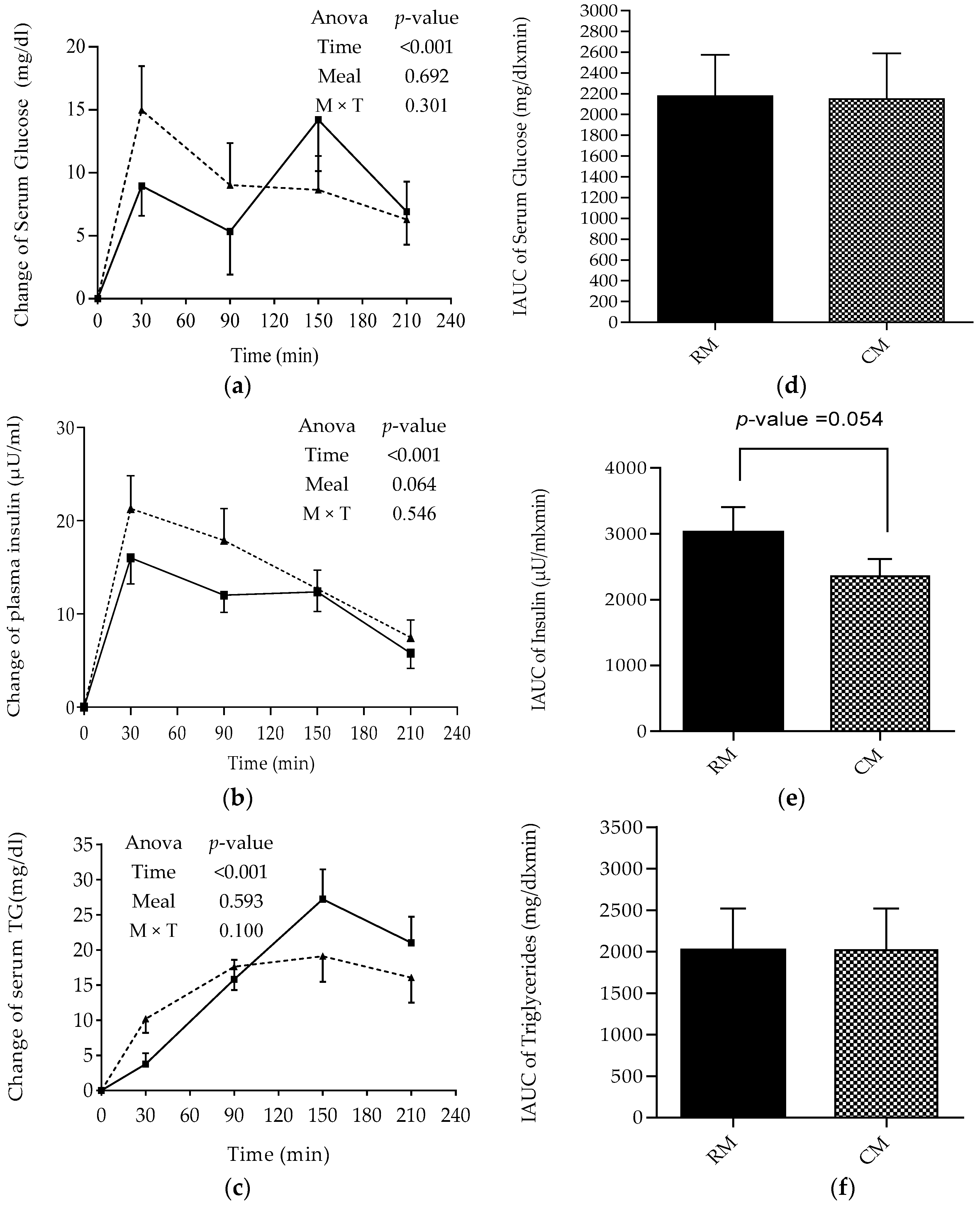
3.1. Postprandial Changes in Glucose, Insulin, and TG
3.2. Postprandial Changes in Appetite Hormones
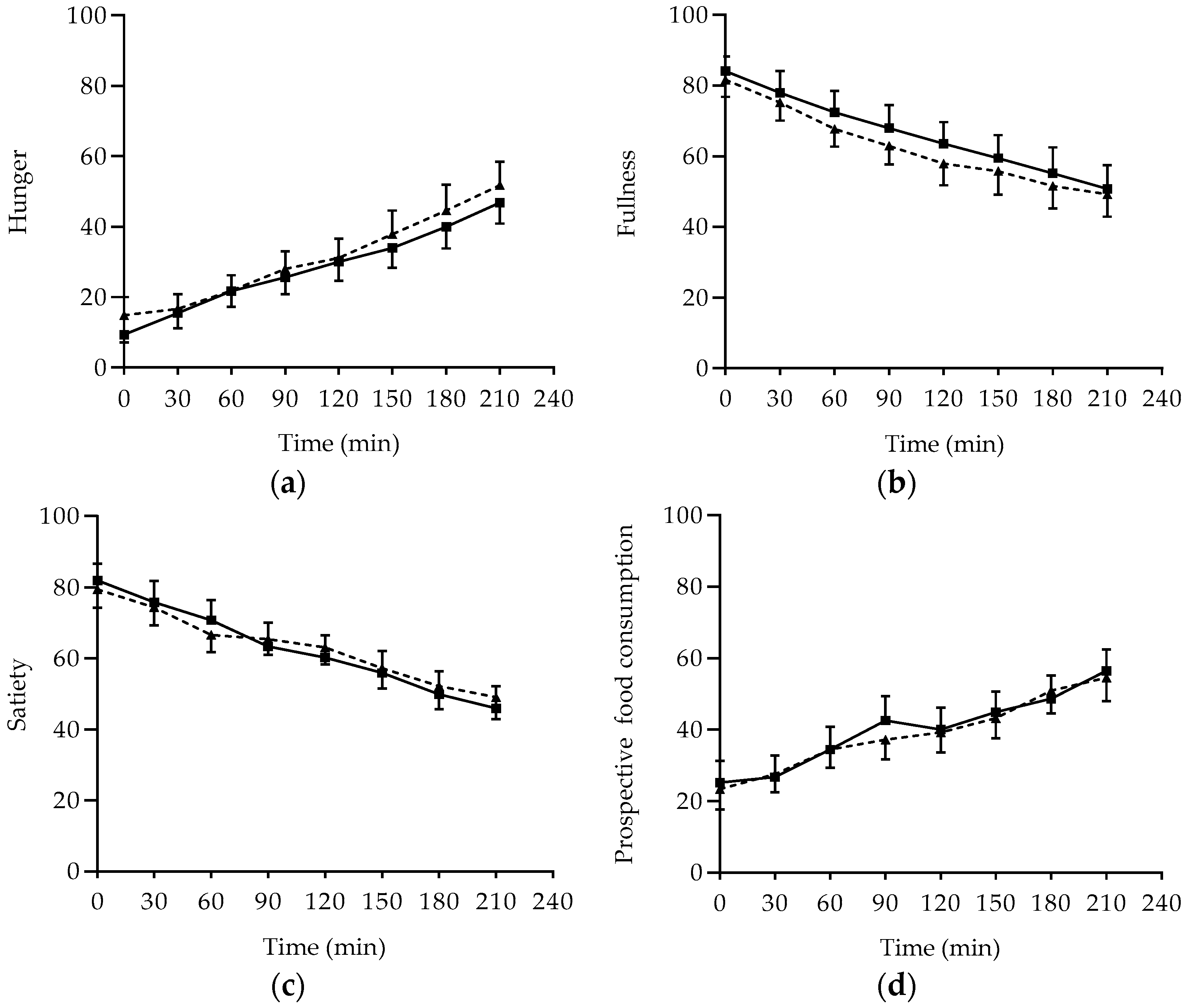
3.3. Subjective Appetite Rating and Food Intake
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nguyen, D.M.; El-Serag, H.B. The epidemiology of obesity. Gastroenterol. Clin. North Am. 2010, 39, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lim, H. The Global Childhood Obesity Epidemic and the Association between Socio-Economic Status and Childhood Obesity; Taylor & Francis: New York, NY, USA, 2012. [Google Scholar]
- WHO Overweight and Obesity. Available online: http://www.who.int/gho/ncd/risk_factors/overweight/en/ (accessed on 21 March 2018).
- Segula, D. Complications of obesity in adults: A short review of the literature. Malawi Med. J. 2014, 26, 20–24. [Google Scholar] [PubMed]
- Marinangeli, C.P.; Jones, P.J. Pulse grain consumption and obesity: Effects on energy expenditure, substrate oxidation, body composition, fat deposition and satiety. Br. J. Nutr. 2012, 108, S46–S51. [Google Scholar] [CrossRef] [PubMed]
- Tosh, S.M.; Yada, S. Dietary fibres in pulse seeds and fractions: Characterization, functional attributes, and applications. Food Res. Int. 2010, 43, 450–460. [Google Scholar] [CrossRef]
- Singh, B.; Singh, J.P.; Shevkani, K.; Singh, N.; Kaur, A. Bioactive constituents in pulses and their health benefits. J. Food Sci. Technol. 2017, 54, 858–870. [Google Scholar] [CrossRef] [PubMed]
- Trinidad, T.P.; Mallillin, A.C.; Loyola, A.S.; Sagum, R.S.; Encabo, R.R. The potential health benefits of legumes as a good source of dietary fibre. Br. J. Nutr. 2010, 103, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Leterme, P. Recommendations by health organizations for pulse consumption. Br. J. Nutr. 2002, 88, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Noorfarahzilah, M.; Lee, J.S.; Sharifudin, M.S.; Mohd Fadzelly, A.B.; Hasmadi, M. Applications of composite flour in development of food products. Int. Food Res. J. 2014, 21, 2061–2074. [Google Scholar]
- Mohammed, I.; Ahmed, A.R.; Senge, B. Dough rheology and bread quality of wheat–chickpea flour blends. Ind. Crops Prod. 2012, 36, 196–202. [Google Scholar] [CrossRef]
- Rachwa-Rosiak, D.; Nebesny, E.; Budryn, G. Chickpeas—Composition, nutritional value, health benefits, application to bread and snacks: A review. Crit. Rev. Food Sci. Nutr. 2015, 55, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Zafar, T.A.; Al-Hassawi, F.; Al-Khulaifi, F.; Al-Rayyes, G.; Waslien, C.; Huffman, F.G. Organoleptic and glycemic properties of chickpea-wheat composite breads. J. Food Sci. Technol. 2015, 52, 2256–2263. [Google Scholar] [CrossRef] [PubMed]
- Fares, C.; Menga, V. Effects of toasting on the carbohydrate profile and antioxidant properties of chickpea (Cicer arietinum L.) flour added to durum wheat pasta. Food Chem. 2012, 131, 1140–1148. [Google Scholar] [CrossRef]
- Gómez, M.; Oliete, B.; Rosell, C.M.; Pando, V.; Fernández, E. Studies on cake quality made of wheat–chickpea flour blends. LWT-Food Sci. Technol. 2008, 41, 1701–1709. [Google Scholar] [CrossRef] [Green Version]
- Yadav, R.B.; Yadav, B.S.; Dhull, N. Effect of incorporation of plantain and chickpea flours on the quality characteristics of biscuits. J. Food Sci. Technol. 2012, 49, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Thongram, S.; Tanwar, B.; Chauhan, A.; Kumar, V. Physicochemical and organoleptic properties of cookies incorporated with legume flours. Cog. Food Agric. 2016, 2, 1172389. [Google Scholar] [CrossRef]
- Johnson, S.K.; Thomas, S.J.; Hall, R.S. Palatability and glucose, insulin and satiety responses of chickpea flour and extruded chickpea flour bread eaten as part of a breakfast. Eur. J. Clin. Nutr. 2005, 59, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Roland, W.S.; Pouvreau, L.; Curran, J.; Velde, F.; Kok, P.M. Flavor aspects of pulse ingredients. Cereal Chem. 2017, 94, 58–65. [Google Scholar] [CrossRef]
- Oghbaei, M.; Prakash, J. Effect of primary processing of cereals and legumes on its nutritional quality: A comprehensive review. Cog. Food Agric. 2016, 2, 1136015. [Google Scholar] [CrossRef]
- Alajaji, S.A.; El-Adawy, T.A. Nutritional composition of chickpea (Cicer arietinum L.) as affected by microwave cooking and other traditional cooking methods. J. Food Compos. Anal. 2006, 19, 806–812. [Google Scholar] [CrossRef]
- Usda Database—Google Search. Available online: https://www.google.com.lb/search (accessed on 3 March 2018).
- Flint, A.; Raben, A.; Blundell, J.E.; Astrup, A. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 38–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Anton, C.; Rico, M.C.; Sanchez-Rodriguez, E.; Ruiz-Lopez, M.D.; Gil, A.; Mesa, M.D. Glycemic responses, appetite ratings and gastrointestinal hormone responses of most common breads consumed in Spain. A randomized control trial in healthy humans. Nutrients 2015, 7, 4033–4053. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, J.-A.; Gasteyger, C.; Raben, A.; Meier, D.H.; Astrup, A.; Sjödin, A. The effect of tesofensine on appetite sensations. Obesity 2012, 20, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Augustin, L.S.; Chiavaroli, L.; Campbell, J.; Ezatagha, A.; Jenkins, A.L.; Esfahani, A.; Kendall, C.W. Post-prandial glucose and insulin responses of hummus alone or combined with a carbohydrate food: A dose–response study. Nutr. J. 2016, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Mahan, L.K.; Raymond, J.L. Krause’s Food & the Nutrition Care Process-e-Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2016. [Google Scholar]
- DiNicolantonio, J.J.; Bhutani, J.; OKeefe, J.H.; Crofts, C. Postprandial Insulin Assay as the Earliest Biomarker for Diagnosing Pre-Diabetes, Type 2 Diabetes and Increased Cardiovascular Risk. Open Heart 2017, 4, e000656. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Kendall, C.W.; Augustin, L.S.; Franceschi, S.; Hamidi, M.; Marchie, A.; Jenkins, A.L.; Axelsen, M. Glycemic index: Overview of implications in health and disease. Am. J. Clin. Nutr. 2002, 76, 266S–273S. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.S.; Chen, W. Chickpea Breeding and Management; CABI: Wallingford, UK, 2007. [Google Scholar]
- El-Adawy, T.A. Nutritional composition and antinutritional factors of chickpeas (Cicer arietinum L.) undergoing different cooking methods and germination. Plant Foods Hum. Nutr. (Former. Qual. Plant.) 2002, 57, 83–97. [Google Scholar] [CrossRef]
- Guillon, F.; Champ, M.-J. Carbohydrate fractions of legumes: Uses in human nutrition and potential for health. Br. J. Nutr. 2002, 88, 293–306. [Google Scholar] [CrossRef] [PubMed]
- McCrory, M.A.; Hamaker, B.R.; Lovejoy, J.C.; Eichelsdoerfer, P.E. Pulse consumption, satiety, and weight management. Adv. Nutr. Int. Rev. J. 2010, 1, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Havemeier, S.; Erickson, J.; Slavin, J. Dietary guidance for pulses: The challenge and opportunity to be part of both the vegetable and protein food groups. Ann. N. Y. Acad. Sci. 2017, 1392, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Kolovou, G.D.; Mikhailidis, D.P.; Kovar, J.; Lairon, D.; Nordestgaard, B.G.; Ooi, T.C.; Perez-Martinez, P.; Bilianou, H.; Anagnostopoulou, K.; Panotopoulos, G. Assessment and clinical relevance of non-fasting and postprandial triglycerides: An expert panel statement. Curr. Vasc. Pharmacol. 2011, 9, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Nestel, P.; Cehun, M.; Chronopoulos, A. Effects of long-term consumption and single meals of chickpeas on plasma glucose, insulin, and triacylglycerol concentrations. Am. J. Clin. Nutr. 2004, 79, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Marić, G.; Gazibara, T.; Zaletel, I.; Labudović Borović, M.; Tomanović, N.; Ćirić, M.; Puškaš, N. The role of gut hormones in appetite regulation. Acta Physiol. Hung. 2014, 101, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Koliaki, C.; Kokkinos, A.; Tentolouris, N.; Katsilambros, N. The effect of ingested macronutrients on postprandial ghrelin response: A critical review of existing literature data. Int. J. Pept. 2010, 2010. [Google Scholar] [CrossRef] [PubMed]
- Saad, M.F.; Bernaba, B.; Hwu, C.-M.; Jinagouda, S.; Fahmi, S.; Kogosov, E.; Boyadjian, R. Insulin regulates plasma ghrelin concentration. J. Clin. Endocrinol. Metab. 2002, 87, 3997–4000. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E. Barley-and Legume Products Beneficially Affect Metabolic Responses and Appetite Regulation; Department of Food Technology, Engineering and Nutrition, Lund University: Lund, Sweden, 2014. [Google Scholar]
- Miller, G.D. Appetite Regulation: Hormones, Peptides, and Neurotransmitters and Their Role in Obesity. Am. J. Lifestyle Med. 2017. [Google Scholar] [CrossRef]
- Zafar, T.A.; Kabir, Y. Chickpeas suppress postprandial blood glucose concentration, and appetite and reduce energy intake at the next meal. J. Food Sci. Technol. 2017, 54, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.; Green, H. Dietary fibre and satiety. Nutr. Bull. 2007, 32, 32–42. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ingredients | Weight (g) | Regular Mankoushe (kcal) | Chickpea Mankoushe (kcal) |
|---|---|---|---|
| Dough | 160 | 394.38 | 399.31 |
| Topping | 13 | 44.15 | 44.15 |
| Oil | 28 | 240 | 240 |
| Total | 201 | 678.53 | 683.46 |
| Parameter | Mean ± SEM | Range |
|---|---|---|
| Age (year) | 22.90 ± 3.00 | 21.0–34.0 |
| Weight (kg) | 58.18 ± 6.78 | 47.1–75.5 |
| BMI (kg/m2) | 22.70 ± 2.65 | 19.7–29.0 |
| LBM (kg) | 42.90 ± 3.36 | 36.1–50.5 |
| Body Fat (%) | 25.92 ± 3.58 | 20.1–33.1 |
| Blood Glucose (mg/dL) | 88.12 ± 8.16 | 73–103 |
| Insulin (μU/mL) | 4.49 ± 1.68 | 1.91–9.12 |
| TG (mg/dL) | 55.46 ± 17.29 | 24–100 |
| GLP-1 (pM) | 26.29 ± 10.21 | 13.73–47.08 |
| Ghrelin (pg/mL) | 527.28 ± 213.65 | 253.83–1131.5 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dandachy, S.; Mawlawi, H.; Chedid, M.; El-Mallah, C.; Obeid, O. Impact of Pre-Processed Chickpea Flour Incorporation into “Mankoushe” on Appetite Hormones and Scores. Foods 2018, 7, 173. https://doi.org/10.3390/foods7100173
Dandachy S, Mawlawi H, Chedid M, El-Mallah C, Obeid O. Impact of Pre-Processed Chickpea Flour Incorporation into “Mankoushe” on Appetite Hormones and Scores. Foods. 2018; 7(10):173. https://doi.org/10.3390/foods7100173
Chicago/Turabian StyleDandachy, Sahar, Hiba Mawlawi, Marwan Chedid, Carla El-Mallah, and Omar Obeid. 2018. "Impact of Pre-Processed Chickpea Flour Incorporation into “Mankoushe” on Appetite Hormones and Scores" Foods 7, no. 10: 173. https://doi.org/10.3390/foods7100173
APA StyleDandachy, S., Mawlawi, H., Chedid, M., El-Mallah, C., & Obeid, O. (2018). Impact of Pre-Processed Chickpea Flour Incorporation into “Mankoushe” on Appetite Hormones and Scores. Foods, 7(10), 173. https://doi.org/10.3390/foods7100173