
Carbamazepine Overdose after Psychiatric Conditions: A Case Study for Postmortem Analysis in Human Bone

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Preparation of Standard Solutions
2.3. Samples
2.4. Preparation of the Samples and Extraction Procedure
2.5. Gas Chromatography–Mass Spectrometry (GC-MS) Analysis
2.6. Validation Procedure
2.7. Expression of Analyte Levels
3. Results
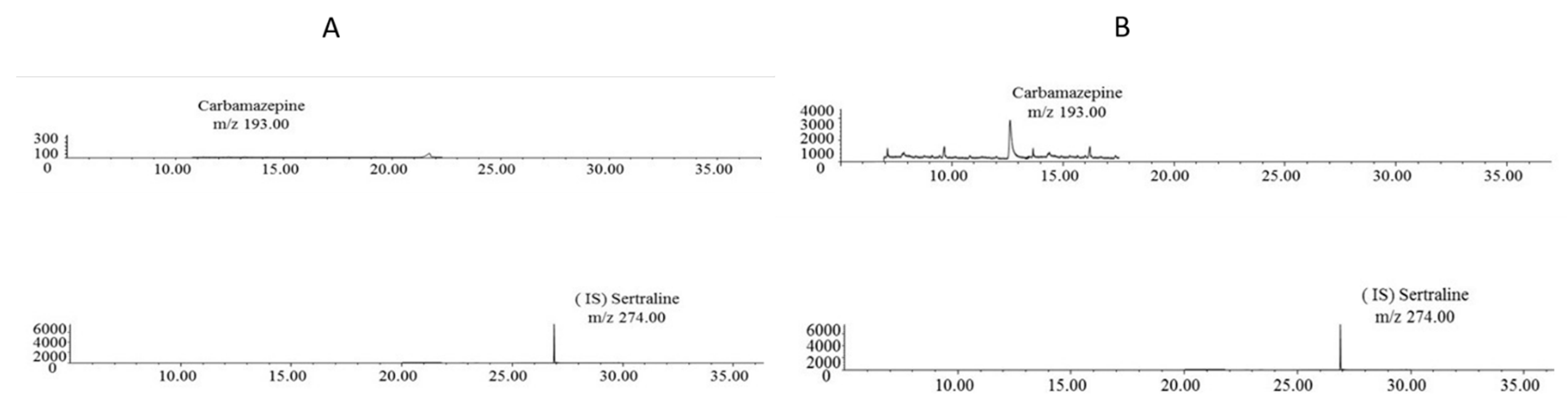
3.1. GC-MS
3.2. Validation Results
3.3. Application to Real Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bridwell, R.E.; Brown, S.; Clerkin, S.; Birdsong, S.; Long, B. Neurologic toxicity of carbamazepine in treatment of trigeminal neuralgia: A case report. Am. J. Emerg. Med. 2022, 55, 231.e3–231.e5. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Cruz, N.; Garcia-Campayo, J.; De Arce, R.; Crespo, J.M.; Vallès, V.; Pérez-Blanco, J.; Roca, E.; Olivares, J.M.; Moríñigo, A.; et al. A double-blind, randomized, placebo-controlled prophylaxis trial of oxcarbazepine as adjunctive treatment to lithium in the long-term treatment of bipolar I and II disorder. Int. J. Neuropsychopharmacol. 2008, 11, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Tondo, L. El tratamiento a largo plazo del trastorno bipolar. Psicodebate 2014, 14, 83–100. [Google Scholar] [CrossRef][Green Version]
- Gummin, D.D.; Mowry, J.B.; Beuhler, M.C.; Spyker, D.A.; Bronstein, A.C.; Rivers, L.J.; Pham, N.P.T.; Weber, J. 2020 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 38th Annual Report. Clin. Toxicol. 2021, 59, 1282–1501. [Google Scholar] [CrossRef]
- Grunze, A.; Amann, B.L.; Grunze, H. Efficacy of Carbamazepine and Its Derivatives in the Treatment of Bipolar Disorder. Medicina 2021, 57, 433. [Google Scholar] [CrossRef]
- Hirsch, A.; Wanounou, M.; Perlman, A.; Hirsh-Raccah, B.; Muszkat, M. The effect of multidrug exposure on neurological manifestations in carbamazepine intoxication: A nested case-control study. BMC Pharmacol. Toxicol. 2020, 21, 47. [Google Scholar] [CrossRef]
- Ghannoum, M.; Yates, C.; Galvao, T.F.; Sowinski, K.M.; Vo, T.H.V.; Coogan, A.; Gosselin, S.; Lavergne, V.; Nolin, T.D.; Hoffman, R.S.; et al. Extracorporeal treatment for carbamazepine poisoning: Systematic review and recommendations from the EXTRIP workgroup. Clin. Toxicol. 2014, 52, 993–1004. [Google Scholar] [CrossRef]
- Tanaka, E. Toxicological Interactions Between Alcohol and Benzodiazepines. J. Toxicol. Clin. Toxicol. 2002, 40, 69–75. [Google Scholar] [CrossRef]
- Hoegberg, L.C.G.; Shepherd, G.; Wood, D.M.; Johnson, J.; Hoffman, R.S.; Caravati, E.M.; Chan, W.L.; Smith, S.W.; Olson, K.R.; Gosselin, S. Systematic review on the use of activated charcoal for gastrointestinal decontamination following acute oral overdose. Clin. Toxicol. 2021, 59, 1196–1227. [Google Scholar] [CrossRef]
- Anand, L.S.; Anand, J.S. Self-poisoning before and during the initial year of the COVID-19 pandemic in northern Poland. Int. J. Occup. Med. Environ. 2022, 35, 1–9. [Google Scholar]
- Ahmed, H.; Larsen, M.; Hansen, M.; Andersen, C. The role of QT-prolonging medications in a forensic autopsy study from Western Denmark. Forensic Sci. Int. 2021, 325, 110889. [Google Scholar] [CrossRef] [PubMed]
- Caplan, Y.H.; Goldberger, B.A. Alternative Specimens for Workplace Drug Testing. J. Anal. Toxicol. 2001, 25, 396–399. [Google Scholar] [CrossRef] [PubMed]
- McGrath, K.K.; Jenkins, A.J. Detection of Drugs of Forensic Importance in Postmortem Bone. Am. J. Forensic Med. Pathol. 2009, 30, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Watterson, J.H.; Botman, J.E. Detection of Acute Diazepam Exposure in Bone and Marrow: Influence of Tissue Type and the Dose-Death Interval on Sensitivity of Detection by ELISA with Liquid Chromatography Tandem Mass Spectrometry Confirmation. J. Forensic Sci. 2009, 54, 708–714. [Google Scholar] [CrossRef]
- McIntyre, I.M.; King, C.V.; Boratto, M.; Drummer, O.H. Postmortem drug analyses in bone and bone marrow. Ther. Drug Monit. 2000, 22, 79–83. [Google Scholar] [CrossRef]
- Fernández, P.; Aldonza, M.; Bouzas, A.; Lema, M.; Bermejo, A.M.; Tabernero, M.J. GC-FID determination of cocaine and its metabolites in human bile and vitreous humor. J. Appl. Toxicol. 2006, 26, 253–257. [Google Scholar] [CrossRef]
- Lin, D.-L.; Chen, C.-Y.; Shaw, K.-P.; Havier, R.; Lin, R.-L. Distribution of Codeine, Morphine, and 6-Acetylmorphine in Vitreous Humor. J. Anal. Toxicol. 1997, 21, 258–261. [Google Scholar] [CrossRef][Green Version]
- Politi, L.; Groppi, A.; Polettini, A.; Montagna, M.T. A rapid screening procedure for drugs and poisons in gastric contents by direct injection-HPLC analysis. Forensic Sci. Int. 2004, 141, 115–120. [Google Scholar] [CrossRef]
- Fernandez-Lopez, L.; Pellegrini, M.; Rotolo, M.C.; Maldonado, A.L.; Falcon, M.; Mancini, R. Development and validation of a method for analysing of duloxetine, venlafaxine and amitriptyline in human bone. Forensic Sci. Int. 2019, 299, 154–160. [Google Scholar] [CrossRef]
- Raikos, N.; Tsoukali, H.; Njau, S. Determination of opiates in postmortem bone and bone marrow. Forensic Sci. Int. 2001, 123, 140–141. [Google Scholar] [CrossRef]
- Wiebe, T.R.; Watterson, J.H. Analysis of tramadol and O-desmethyltramadol in decomposed skeletal tissues following acute and repeated tramadol exposure by gas chromatography mass spectrometry. Forensic Sci. Int. 2014, 242, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Wille, S.M.R.; Coucke, W.; De Baere, T.; Peters, F.T. Update of Standard Practices for New Method Validation in Forensic Tox-icology. Curr. Pharm. Des. 2017, 23, 5442–5454. [Google Scholar] [PubMed]
- Peters, F.T.; Wissenbach, D.K.; Busardò, F.P.; Marchei, E.; Pichini, S. Method Development in Forensic Toxicology. Curr. Pharm. Des. 2017, 23, 5455–5467. [Google Scholar] [CrossRef] [PubMed]
- Matuszewski, B.K.; Constanzer, M.L.; Chavez-Eng, C.M. Strategies for the Assessment of Matrix Effect in Quantitative Bioanalytical Methods Based on HPLC−MS/MS. Anal. Chem. 2003, 75, 3019–3030. [Google Scholar] [CrossRef]
- Schulz, M.; Schmoldt, A. Therapeutic and toxic blood concentrations of more than 800 drugs and other xenobiotics. Pharmazie 2003, 58, 447–474. [Google Scholar]
- Ösby, U.; Brandt, L.; Correia, N.; Ekbom, A.; Sparén, P. Excess Mortality in Bipolar and Unipolar Disorder in Sweden. Arch. Gen. Psychiatry 2001, 58, 844–850. [Google Scholar] [CrossRef]
- Fazel, S.; Gulati, G.; Linsell, L.; Geddes, J.R.; Grann, M. Schizophrenia and violence: Systematic review and me-ta-analysis. PLoS Med. 2009, 6, e1000120. [Google Scholar] [CrossRef]
- Baillargeon, J.; Binswanger, I.A.; Penn, J.V.; Williams, B.A.; Murray, O.J. Psychiatric Disorders and Repeat Incarcerations: The Revolving Prison Door. Am. J. Psychiatry 2009, 166, 103–109. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Indication | Pharmacokinetic | Blood Levels |
|---|---|---|
| Main indication: epilepsy Other indications: trigeminal neuralgia neuropathic pain psychiatric conditions (depression, bipolar disorder, manic episodes) | Distribution: 70–80% protein binding Reaches breast milk and crosses placental barrier. Metabolism: hepatic Elimination: 70% renal, 30% hepatic t1/2 36 h | Terapeutic: 4–12 μg/mL Toxic: >12 μg/mL Severe toxicity: 40 μg/mL (in combination with antidepressants or alcohol: 30 μg/mL) |
| Substance | RT (min) | Characteristic Mass Fragments (m/z) |
|---|---|---|
| Carbamazepine | 12.9 | 193–165–139 |
| Sertraline (IS) | 26.8 | 159–262–274–304 |
| Analyte | Intra-Assay Precision (RSD) | Intra-Assay Accuracy (ABS%Error) | Inter-Assay Precision (RSD) | Inter-Assay Accuracy (ABS%Error) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| * QCL | ** QCM | *** QCH | QCL | QCM | QCH | QCL | QCM | QCH | QCL | QCM | QCH | |
| Carbamazepine | 1.4 | 2.3 | 0.4 | 13.6 | 3.3 | 1.9 | 1.3 | 1.4 | 0.9 | 6.9 | 0.2 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-López, L.; Mancini, R.; Rotolo, M.-C.; Navarro-Zaragoza, J.; Hernández del Rincón, J.-P.; Falcón, M. Carbamazepine Overdose after Psychiatric Conditions: A Case Study for Postmortem Analysis in Human Bone. Toxics 2022, 10, 322. https://doi.org/10.3390/toxics10060322
Fernández-López L, Mancini R, Rotolo M-C, Navarro-Zaragoza J, Hernández del Rincón J-P, Falcón M. Carbamazepine Overdose after Psychiatric Conditions: A Case Study for Postmortem Analysis in Human Bone. Toxics. 2022; 10(6):322. https://doi.org/10.3390/toxics10060322
Chicago/Turabian StyleFernández-López, Lucia, Rosanna Mancini, Maria-Concetta Rotolo, Javier Navarro-Zaragoza, Juan-Pedro Hernández del Rincón, and Maria Falcón. 2022. "Carbamazepine Overdose after Psychiatric Conditions: A Case Study for Postmortem Analysis in Human Bone" Toxics 10, no. 6: 322. https://doi.org/10.3390/toxics10060322
APA StyleFernández-López, L., Mancini, R., Rotolo, M.-C., Navarro-Zaragoza, J., Hernández del Rincón, J.-P., & Falcón, M. (2022). Carbamazepine Overdose after Psychiatric Conditions: A Case Study for Postmortem Analysis in Human Bone. Toxics, 10(6), 322. https://doi.org/10.3390/toxics10060322