
Atypical Fentanyl Transdermal Patch Consumption and Fatalities: Case Report and Literature Review
 , , , ,
, , , ,
Abstract
:1. Introduction
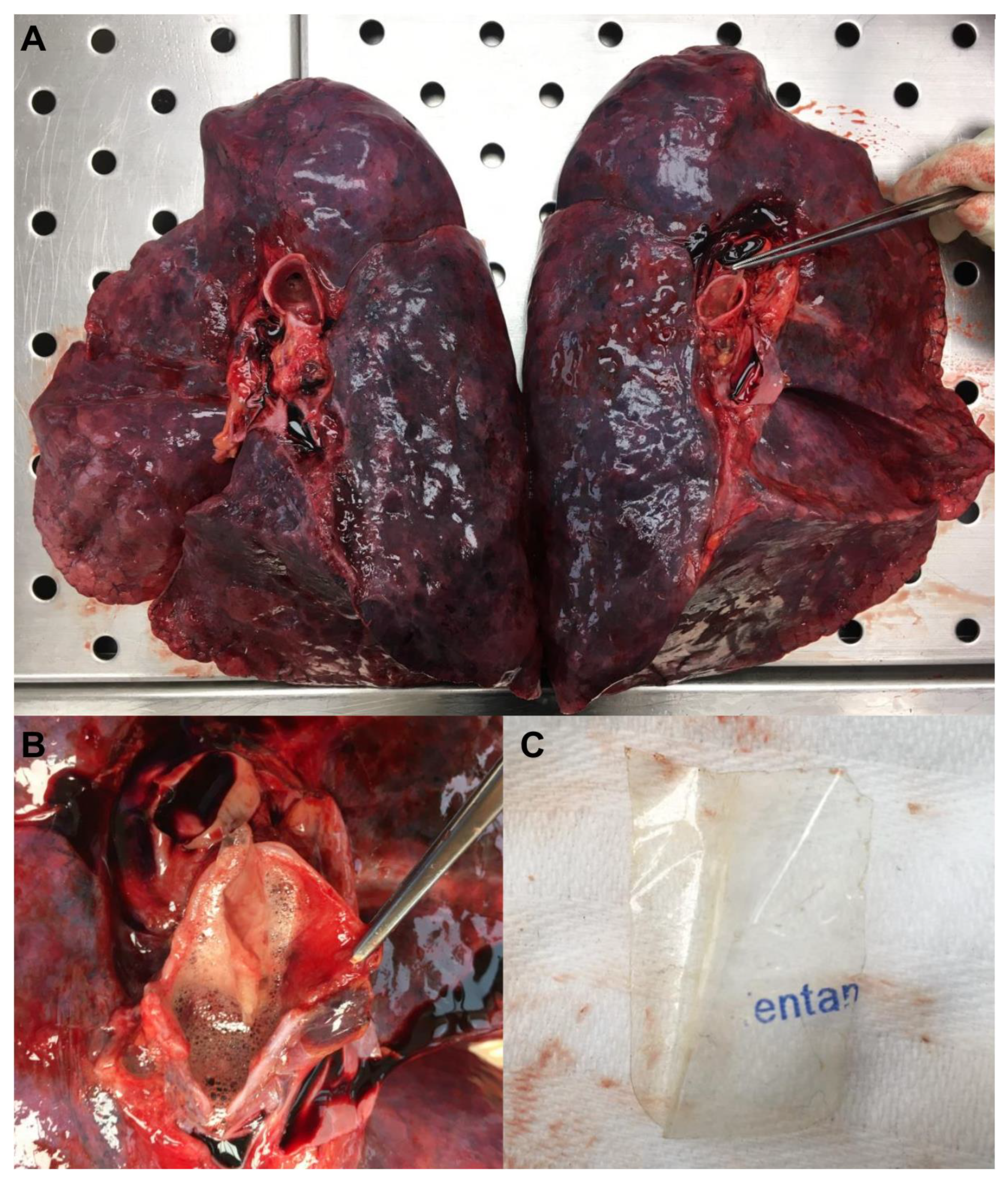
2. Case Report
3. Materials and Methods
3.1. Chemicals and Reagents
3.2. Calibration Curves
3.2.1. Blood Alcohol
3.2.2. Fentanyl
3.3. Sample Pretreatment
3.3.1. Fentanyl, Cocaine, Benzoylecgonine, Morphine, 6-Monoacetylmorphine
3.3.2. Alprazolam
3.3.3. Methadone, EDDP
3.3.4. Blood Alcohol
3.4. GC-MS Conditions
3.4.1. Fentanyl
3.4.2. Cocaine, Benzoylecgonine, Morphine, 6-Monoacethylmorphine, Methadone, EDDP
3.4.3. Alprazolam
3.5. HS-GC-FID Conditions
3.6. Method Validation
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schug, S.A.; Ting, S. Fentanyl Formulations in the Management of Pain: An Update. Drugs 2017, 77, 747–763. [Google Scholar] [CrossRef]
- Peng, P.W.; Sandler, A.N. A review of the use of fentanyl analgesia in the management of acute pain in adults. Anesthesiology 1999, 90, 576–599. [Google Scholar] [CrossRef]
- Kuczyńska, K.; Grzonkowski, P.; Kacprzak, Ł.; Zawilska, J.B. Abuse of fentanyl: An emerging problem to face. Forensic Sci. Int. 2018, 289, 207–214. [Google Scholar] [CrossRef] [PubMed]
- D’Errico, S. Commentary. Fentanyl-related death and the underreporting risk. J. Forensic Leg. Med. 2018, 60, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Phalen, P.; Ray, B.; Watson, D.P.; Huynh, P.; Greene, M.S. Fentanyl related overdose in Indianapolis: Estimating trends using multilevel Bayesian models. Addict. Behav. 2018, 86, 4–10. [Google Scholar] [CrossRef]
- Lavonas, E.J.; Dezfulian, C. Impact of the Opioid Epidemic. Crit. Care Clin. 2020, 36, 753–769. [Google Scholar] [CrossRef] [PubMed]
- Upp, L.A.; Waljee, J.F. The Opioid Epidemic. Clin. Plast. Surg. 2020, 47, 181–190. [Google Scholar] [CrossRef]
- Sinicina, I.; Sachs, H.; Keil, W. Post-mortem review of fentanyl-related overdose deaths among identified drug users in Southern Bavaria, Germany, 2005–2014. Drug Alcohol Depend. 2017, 180, 286–291. [Google Scholar] [CrossRef]
- Spencer, M.R.; Warner, M.; Bastian, B.A.; Trinidad, J.P.; Hedegaard, H. Drug Overdose Deaths Involving Fentanyl, 2011–2016. Natl. Vital Stat. Rep. 2019, 68, 1–19. [Google Scholar]
- Bardwell, G.; Wood, E.; Brar, R. Fentanyl assisted treatment: A possible role in the opioid overdose epidemic? Subst. Abuse Treat. Prev. Policy 2019, 14, 50. [Google Scholar] [CrossRef]
- Han, Y.; Yan, W.; Zheng, Y.; Khan, M.Z.; Yuan, K.; Lu, L. The rising crisis of illicit fentanyl use, overdose, and potential therapeutic strategies. Transl. Psychiatry 2019, 9, 282. [Google Scholar] [CrossRef] [PubMed]
- Manetti, F.; Scopetti, M.; Santurro, A.; Consoloni, L.; D’Errico, S. Widespread septic embolization in injection drug use mitro-aortic infective endocarditis as a remote cause of death. Int. J. Legal Med. 2020, 134, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Juhascik, M.P.; Jenkins, A.J. Comparison of liquid/liquid and solid-phase extraction for alkaline drugs. J. Chromatogr. Sci. 2009, 47, 553–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, D.A.; Clark, G.D.; Haver, V.M.; Garbin, J.A.; Saxon, A.J. Analysis of urinary benzodiazepines using solid-phase extraction and gas chromatography-mass spectrometry. J. Anal. Toxicol. 1994, 18, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Stout, P.R.; Horn, C.K.; Klette, K.L. Solid-phase extraction and GC-MS analysis of THC-COOH method optimized for a high-throughput forensic drug-testing laboratory. J. Anal. Toxicol. 2001, 25, 550–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polettini, A.; Groppi, A.; Vignali, C.; Montagna, M. Fully-automated systematic toxicological analysis of drugs, poisons, and metabolites in whole blood, urine, and plasma by gas chromatography-full scan mass spectrometry. J. Chromatogr. B Biomed. Sci. Appl. 1998, 713, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Alexandridou, A.; Mouskeftara, T.; Raikos, N.; Gika, H.G. GC-MS analysis of underivatised new psychoactive substances in whole blood and urine. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2020, 1156, 122308. [Google Scholar] [CrossRef]
- Abusada, G.M.; Abukhalaf, I.K.; Alford, D.D.; Vinzon-Bautista, I.; Pramanik, A.K.; Ansari, N.A.; Manno, J.E.; Manno, B.R. Solid-phase extraction and GC/MS quantitation of cocaine, ecgonine methyl ester, benzoylecgonine, and cocaethylene from meconium, whole blood, and plasma. J. Anal. Toxicol. 1993, 17, 353–358. [Google Scholar] [CrossRef]
- Weinmann, W.; Renz, M.; Vogt, S.; Pollak, S. Automated solid-phase extraction and two-step derivatisation for simultaneous analysis of basic illicit drugs in serum by GC/MS. Int. J. Legal Med. 2000, 113, 229–235. [Google Scholar] [CrossRef]
- Meatherall, R. GC-MS quantitation of codeine, morphine, 6-acetylmorphine, hydrocodone, hydromorphone, oxycodone, and oxymorphone in blood. J. Anal. Toxicol. 2005, 29, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Armbruster, D.A.; Tillman, M.D.; Hubbs, L.M. Limit of detection (LQD)/limit of quantitation (LOQ): Comparison of the empirical and the statistical methods exemplified with GC-MS assays of abused drugs. Clin. Chem. 1994, 40, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- GIFT—Group of Italian Forensic Toxicologists. Linee Guida per i Laboratori Di Analisi Di Sostanze D’abuso Con Finalità Tossicologico-Forensi e Medico-Legali—2010. Available online: https://www.gtfi.it/wp-content/uploads/2015/07/LG2010.pdf (accessed on 7 March 2022).
- Palmer, R.B. Fentanyl in postmortem forensic toxicology. Clin. Toxicol. 2010, 48, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Geile, J.; Maas, A.; Kraemer, M.; Doberentz, E.; Madea, B. Fatal misuse of transdermal fentanyl patches. Forensic Sci. Int. 2019, 302, 109858. [Google Scholar] [CrossRef] [PubMed]
- Kuhlman, J.J., Jr.; McCaulley, R.; Valouch, T.J.; Behonick, G.S. Fentanyl use, misuse, and abuse: A summary of 23 postmortem cases. J. Anal. Toxicol. 2003, 27, 499–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liappas, I.A.; Dimopoulos, N.P.; Mellos, E.; Gitsa, O.E.; Liappas, A.I.; Rabavilas, A.D. Oral transmucosal abuse of transdermal fentanyl. J. Psychopharmacol. 2004, 18, 277–280. [Google Scholar] [CrossRef]
- Thomas, S.; Winecker, R.; Pestaner, J.P. Unusual fentanyl patch administration. Am. J. Forensic Med. Pathol. 2008, 29, 162–163. [Google Scholar] [CrossRef]
- Woodall, K.L.; Martin, T.L.; McLellan, B.A. Oral abuse of fentanyl patches (Duragesic): Seven case reports. J. Forensic Sci. 2008, 53, 222–225. [Google Scholar] [CrossRef]
- Zhang, Q.; Murawsky, M.; LaCount, T.D.; Hao, J.; Ghosh, P.; Raney, S.G.; Kasting, G.B.; Li, S.K. Evaluation of Heat Effects on Fentanyl Transdermal Delivery Systems Using In Vitro Permeation and In Vitro Release Methods. J. Pharm. Sci. 2020, 109, 3095–3104. [Google Scholar] [CrossRef]
- Prodduturi, S.; Sadrieh, N.; Wokovich, A.M.; Doub, W.H.; Westenberger, B.J.; Buhse, L. Transdermal delivery of fentanyl from matrix and reservoir systems: Effect of heat and compromised skin. J. Pharm. Sci. 2010, 99, 2357–2366. [Google Scholar] [CrossRef]
- Coon, T.P.; Miller, M.; Kaylor, D.; Jones-Spangle, K. Rectal insertion of fentanyl patches: A new route of toxicity. Ann. Emerg. Med. 2005, 46, 473. [Google Scholar] [CrossRef]
- Krinsky, C.S.; Lathrop, S.L.; Crossey, M.; Baker, G.; Zumwalt, R. A toxicology-based review of fentanyl-related deaths in New Mexico (1986-2007). Am. J. Forensic Med. Pathol. 2011, 32(4), 347–351. [Google Scholar] [CrossRef] [PubMed]
- Schauer, C.K.; Shand, J.A.; Reynolds, T.M. The Fentanyl Patch Boil-Up—A Novel Method of Opioid Abuse. Basic Clin. Pharmacol. Toxicol. 2015, 117, 358–359. [Google Scholar] [CrossRef] [PubMed]
- Kacela, M.; Wojcieszak, J.; Zawilska, J.B. Use of fentanyl, butyrfentanyl and furanylfentanyl as discussed on Polish online forums devoted to ‘designer drugs’. Używanie fentanylu, butyrylofentanylu i furanylofentanylu w opinii użytkowników polskich forów internetowych poświęconych „dopalaczom”. Psychiatr. Pol. 2022, 56, 355–372. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, K.A.; Tharratt, R.S. Inhalation abuse of fentanyl patch. J. Toxicol. Clin. Toxicol. 1994, 32, 75–78. [Google Scholar] [CrossRef]
- Barrueto, F., Jr.; Howland, M.A.; Hoffman, R.S.; Nelson, L.S. The fentanyl tea bag. Vet. Hum. Toxicol. 2004, 46, 30–31. [Google Scholar]
- Carson, H.J.; Knight, L.D.; Dudley, M.H.; Garg, U. A fatality involving an unusual route of fentanyl delivery: Chewing and aspirating the transdermal patch. Leg. Med. 2010, 12, 157–159. [Google Scholar] [CrossRef]
- Rahman, S.; Trussell, A.; Pearson, S.A.; Buckley, N.A.; Karanges, E.A.; Cairns, R.; Litchfield, M.; Todd, A.; Gisev, N. Trends in transdermal fentanyl utilisation and fatal fentanyl overdose across Australia (2003–2015). Drug Alcohol Rev. 2022, 41, 435–443. [Google Scholar] [CrossRef]
- Björkman, S.; Stanski, D.R.; Verotta, D.; Harashima, H. Comparative tissue concentration profiles of fentanyl and alfentanil in humans predicted from tissue/blood partition data obtained in rats. Anesthesiology 1990, 72, 865–873. [Google Scholar] [CrossRef]
- Guitton, J.; Buronfosse, T.; Désage, M.; Lepape, A.; Brazier, J.L.; Beaune, P. Possible involvement of multiple cytochrome P450S in fentanyl and sufentanil metabolism as opposed to alfentanil. Biochem. Pharmacol. 1997, 53, 1613–1619. [Google Scholar] [CrossRef]
- Nelson, L.; Schwaner, R. Transdermal fentanyl: Pharmacology and toxicology. J. Med. Toxicol. 2009, 5, 230–241. [Google Scholar] [CrossRef] [Green Version]
- Tharp, A.M.; Winecker, R.E.; Winston, D.C. Fatal intravenous fentanyl abuse: Four cases involving extraction of fentanyl from transdermal patches. Am. J. Forensic Med. Pathol. 2004, 25, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Jumbelic, M.I. Deaths with transdermal fentanyl patches. Am. J. Forensic Med. Pathol. 2010, 31, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.L.; Woodall, K.L.; McLellan, B.A. Fentanyl-related deaths in Ontario, Canada: Toxicological findings and circumstances of death in 112 cases (2002–2004). J. Anal. Toxicol. 2006, 30, 603–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, J.G.; Baker, A.M.; Bracey, A.H.; Seningen, J.; Kloss, J.S.; Strobl, A.Q.; Apple, F.S. Fentanyl concentrations in 23 postmortem cases from the hennepin county medical examiner’s office. J. Forensic Sci. 2007, 52, 978–981. [Google Scholar] [CrossRef]
- Andresen, H.; Gullans, A.; Veselinovic, M.; Anders, S.; Schmoldt, A.; Iwersen-Bergmann, S.; Mueller, A. Fentanyl: Toxic or therapeutic? Postmortem and antemortem blood concentrations after transdermal fentanyl application. J. Anal. Toxicol. 2012, 36, 182–194. [Google Scholar] [CrossRef]
- Moore, P.W.; Palmer, R.B.; Donovan, J.W. Fatal fentanyl patch misuse in a hospitalized patient with a postmortem increase in fentanyl blood concentration. J. Forensic Sci. 2015, 60, 243–246. [Google Scholar] [CrossRef]
- Hill, R.; Santhakumar, R.; Dewey, W.; Kelly, E.; Henderson, G. Fentanyl depression of respiration: Comparison with heroin and morphine. Br. J. Pharmacol. 2020, 177, 254–266. [Google Scholar] [CrossRef]
- Kinshella, M.W.; Gauthier, T.; Lysyshyn, M. Rigidity, dyskinesia and other atypical overdose presentations observed at a supervised injection site, Vancouver, Canada. Harm Reduct. J. 2018, 15, 64. [Google Scholar] [CrossRef] [Green Version]
- Burns, G.; DeRienz, R.T.; Baker, D.D.; Casavant, M.; Spiller, H.A. Could chest wall rigidity be a factor in rapid death from illicit fentanyl abuse? Clin. Toxicol. 2016, 54, 420–423. [Google Scholar] [CrossRef]
- Pergolizzi, J.V., Jr.; Webster, L.R.; Vortsman, E.; Ann LeQuang, J.; Raffa, R.B. Wooden Chest syndrome: The atypical pharmacology of fentanyl overdose. J. Clin. Pharm. Ther. 2021, 46, 1505–1508. [Google Scholar] [CrossRef] [PubMed]
- Green, T.C.; Gilbert, M. Counterfeit Medications and Fentanyl. JAMA Intern. Med. 2016, 176, 1555–1557. [Google Scholar] [CrossRef] [PubMed]
- Fairbairn, N.; Coffin, P.O.; Walley, A.Y. Naloxone for heroin, prescription opioid, and illicitly made fentanyl overdoses: Challenges and innovations responding to a dynamic epidemic. Int. J. Drug Policy 2017, 46, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Peterson, A.B.; Gladden, R.M.; Delcher, C.; Spies, E.; Garcia-Williams, A.; Wang, Y.; Halpin, J.; Zibbell, J.; McCarty, C.L.; DeFiore-Hyrmer, J.; et al. Increases in Fentanyl-Related Overdose Deaths—Florida and Ohio, 2013–2015. MMWR Morb. Mortal. Wkly Rep. 2016, 65, 844–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobeck, E.N.; Schoo, S.M.; Ingram, S.L.; Morgan, M.M. Lack of Antinociceptive Cross-Tolerance with Co-Administration of Morphine and Fentanyl into the Periaqueductal Gray of Male Sprague-Dawley Rats. J. Pain 2019, 20, 1040–1047. [Google Scholar] [CrossRef] [Green Version]
- Cheema, E.; McGuinness, K.; Hadi, M.A.; Paudyal, V.; Elnaem, M.H.; Alhifany, A.A.; Elrggal, M.W.; Al Hamid, A. Causes, Nature and Toxicology of Fentanyl-Associated Deaths: A Systematic Review of Deaths Reported in Peer-Reviewed Literature. J. Pain Res. 2020, 13, 3281–3294. [Google Scholar] [CrossRef]
- Manetti, F.; Chericoni, S.; Marrocco, A.; Scopetti, M.; Padovano, M.; Santurro, A.; Frati, P.; Gabbrielli, M.; Fineschi, V. Cannabis and Driving: Developing Guidelines for Safety Policies. Curr. Pharm. Biotechnol. 2022. ahead of print. [Google Scholar] [CrossRef]
- Scopetti, M.; Morena, D.; Manetti, F.; Santurro, A.; Fazio, N.D.; D’Errico, S.; Padovano, M.; Frati, P.; Fineschi, V. Cannabinoids and brain damage: A systematic review on a frequently overlooked issue. Curr. Pharm. Biotechnol. 2022. ahead of print. [Google Scholar] [CrossRef]
- Padovano, M.; Aromatario, M.; D’Errico, S.; Concato, M.; Manetti, F.; David, M.C.; Scopetti, M.; Frati, P.; Fineschi, V. Sodium Nitrite Intoxication and Death: Summarizing Evidence to Facilitate Diagnosis. Int. J. Environ. Res. Public Health 2022, 19, 13996. [Google Scholar] [CrossRef]
- Tadrous, M.; Greaves, S.; Martins, D.; Nadeem, K.; Singh, S.; Mamdani, M.M.; Juurlink, D.N.; Gomes, T. Evaluation of the fentanyl patch-for-patch program in Ontario, Canada. Int. J. Drug Policy 2019, 66, 82–86. [Google Scholar] [CrossRef]
- Guliyev, C.; Tuna, Z.O.; Ögel, K. Fentanyl use disorder characterized by unprescribed use of transdermal patches: A case report. J. Addict. Dis. 2002, 40, 285–290. [Google Scholar] [CrossRef]
- La Russa, R.; Catalano, C.; Di Sanzo, M.; Scopetti, M.; Gatto, V.; Santurro, A.; Viola, R.V.; Panebianco, V.; Frati, P.; Fineschi, V. Postmortem computed tomography angiography (PMCTA) and traditional autopsy in cases of sudden cardiac death due to coronary artery disease: A systematic review and meta-analysis. Radiol. Med. 2019, 124, 109–117. [Google Scholar] [CrossRef]
- Gatto, V.; Scopetti, M.; La Russa, R.; Santurro, A.; Cipolloni, L.; Viola, R.V.; Di Sanzo, M.; Frati, P.; Fineschi, V. Advanced Loss Eventuality Assessment and Technical Estimates: An Integrated Approach for Management of Healthcare-Associated Infections. Curr. Pharm. Biotechnol. 2019, 20, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Busardò, F.P.; Frati, P.; Santurro, A.; Zaami, S.; Fineschi, V. Errors and malpractice lawsuits in radiology: What the radiologist needs to know. Radiol. Med. 2015, 120, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Santurro, A.; Vullo, A.M.; Borro, M.; Gentile, G.; La Russa, R.; Simmaco, M.; Frati, P.; Fineschi, V. Personalized Medicine Applied to Forensic Sciences: New Advances and Perspectives for a Tailored Forensic Approach. Curr. Pharm. Biotechnol. 2017, 18, 263–273. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Compound | LOD | LOQ |
|---|---|---|
| Methadone | 5 ng/mL | 15 ng/mL |
| EDDP | 5 ng/mL | 15 ng/mL |
| Morphine | 5 ng/mL | 15 ng/mL |
| 6-MAM | 5 ng/mL | 15 ng/mL |
| Fentanyl | 1.5 ng/mL | 2.5 ng/mL |
| Alprazolam | 3 ng/mL | 10 ng/mL |
| Cocaine | 5 ng/mL | 15 ng/mL |
| BEG | 10 ng/mL | 30 ng/mL |
| Ethyl alcohol | 0.05 g/L | 0.1 g/L |
| Compound | Femoral Blood | Urine |
|---|---|---|
| Methadone | <LOD | 195 ng/mL |
| EDDP | <LOD | 285 ng/mL |
| Total morphine | 133 ng/mL | 5553 ng/mL |
| Free morphine | <LOD | 995 ng/mL |
| 6-MAM | <LOD | 182 ng/mL |
| Fentanyl | 50 ng/mL | 73 ng/mL |
| Alprazolam | <LOD | 96 ng/mL |
| Cocaine | <LOD | 994 ng/mL |
| BEG | 91 ng/mL | 4967 ng/mL |
| Ethyl alcohol | 0.22 g/l | - |
| Extraction/Consumption Method | Characteristics |
|---|---|
| Application of a patch on cutaneous surface |
|
| Chewing or ingestion of a patch—Application of a patch to buccal or rectal mucosa |
|
| Needle extraction of fentanyl from a patch |
|
| Extraction by simmering in hot water |
|
| Extraction using other solvents |
|
| Patch smoking or “vaporization” |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manetti, F.; David, M.C.; Gariglio, S.; Consalvo, F.; Padovano, M.; Scopetti, M.; Grande, A.; Santurro, A. Atypical Fentanyl Transdermal Patch Consumption and Fatalities: Case Report and Literature Review. Toxics 2023, 11, 46. https://doi.org/10.3390/toxics11010046
Manetti F, David MC, Gariglio S, Consalvo F, Padovano M, Scopetti M, Grande A, Santurro A. Atypical Fentanyl Transdermal Patch Consumption and Fatalities: Case Report and Literature Review. Toxics. 2023; 11(1):46. https://doi.org/10.3390/toxics11010046
Chicago/Turabian StyleManetti, Federico, Maria Chiara David, Sara Gariglio, Francesca Consalvo, Martina Padovano, Matteo Scopetti, Antonio Grande, and Alessandro Santurro. 2023. "Atypical Fentanyl Transdermal Patch Consumption and Fatalities: Case Report and Literature Review" Toxics 11, no. 1: 46. https://doi.org/10.3390/toxics11010046