

Modulation of the Cardiovascular Effects of Polycyclic Aromatic Hydrocarbons: Physical Exercise as a Protective Strategy
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Nasal Instillation
2.3. Intervention Protocol
2.4. Exercise Training
2.5. Sampling Extraction
2.6. Serum cytokines
2.7. RT-qPCR
2.8. Western Blotting
2.9. Statistics
3. Results
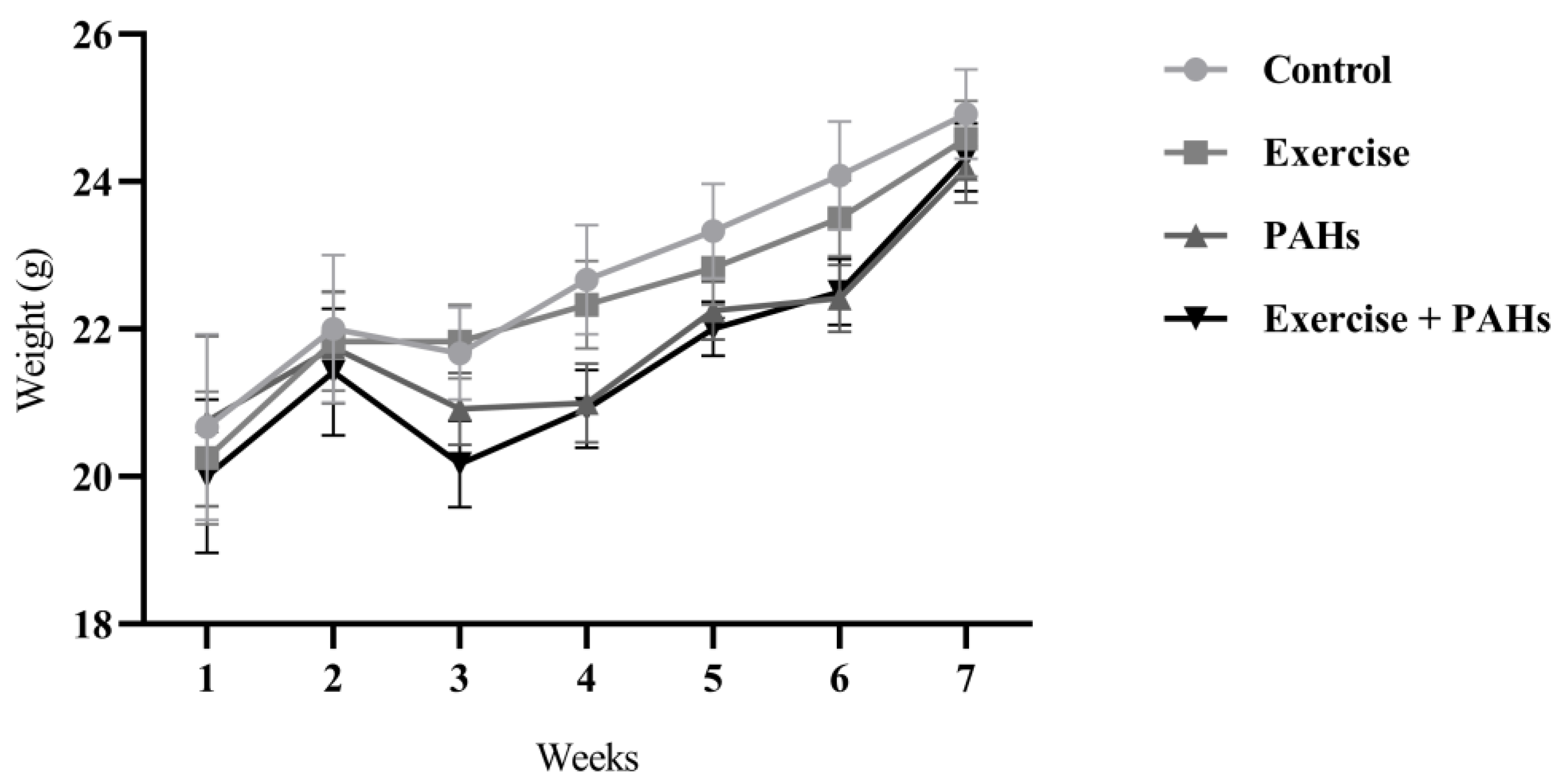
3.1. Animals
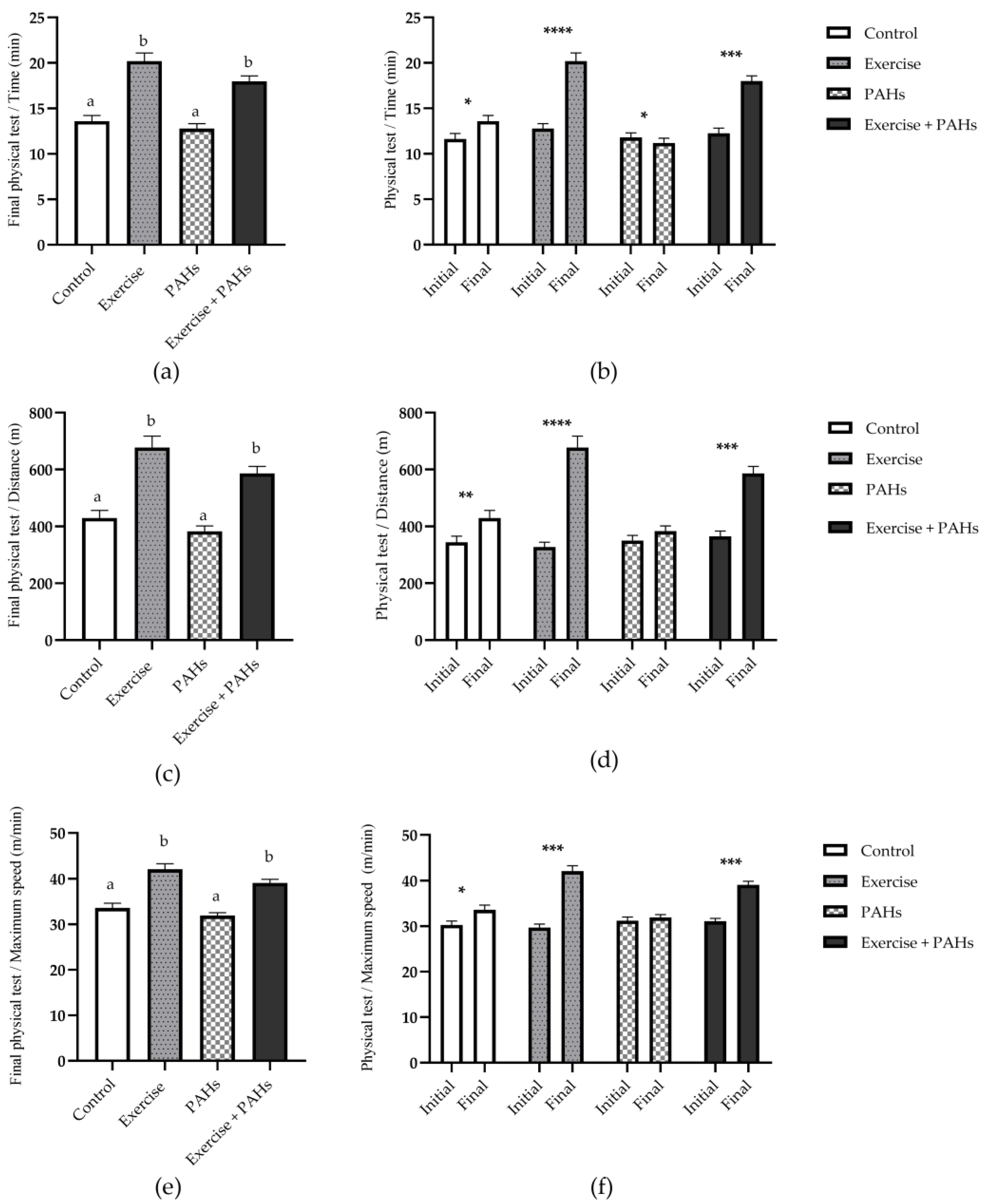
3.2. Training Effects
3.3. Serum Cytokines
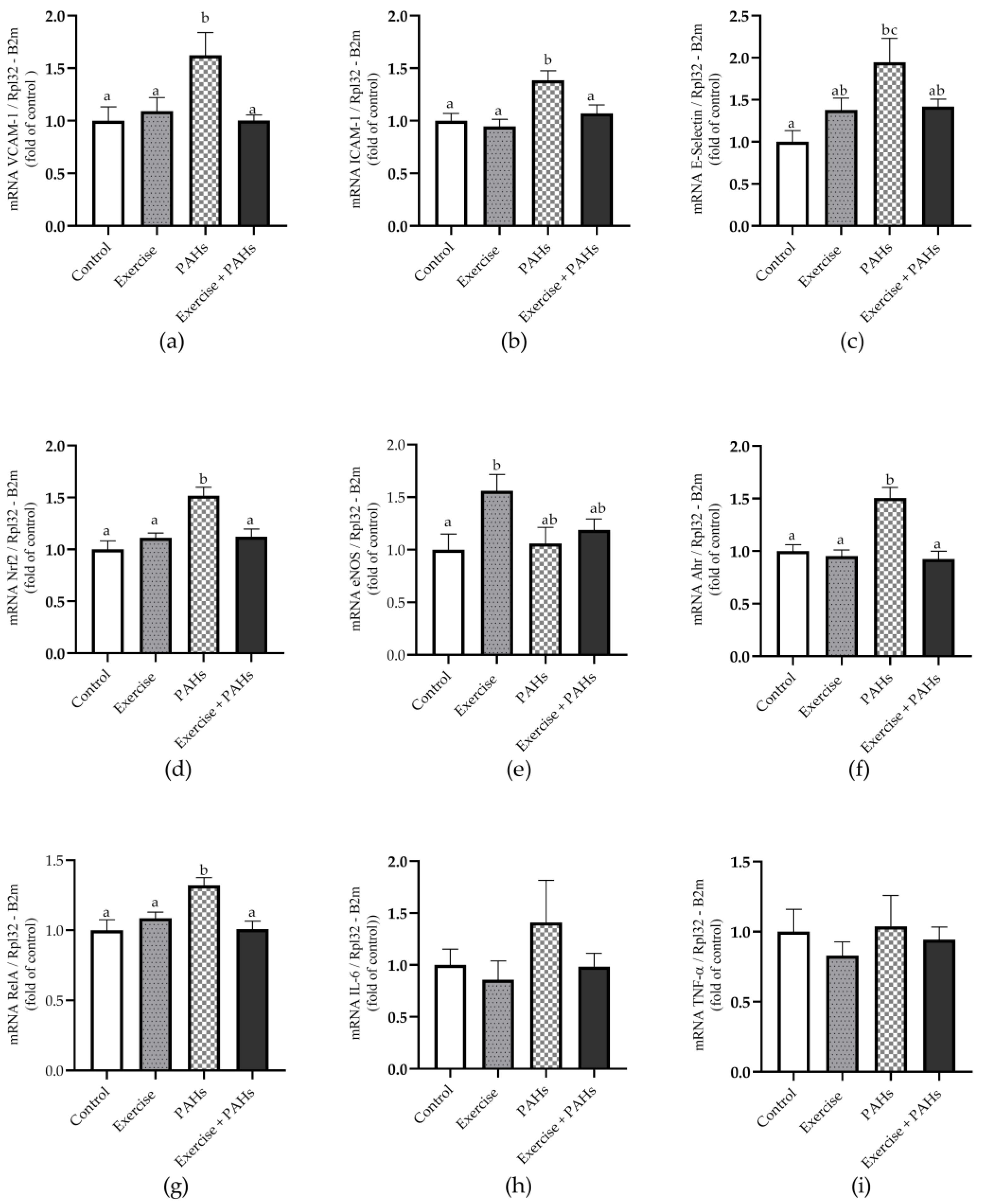
3.4. Gene Expression
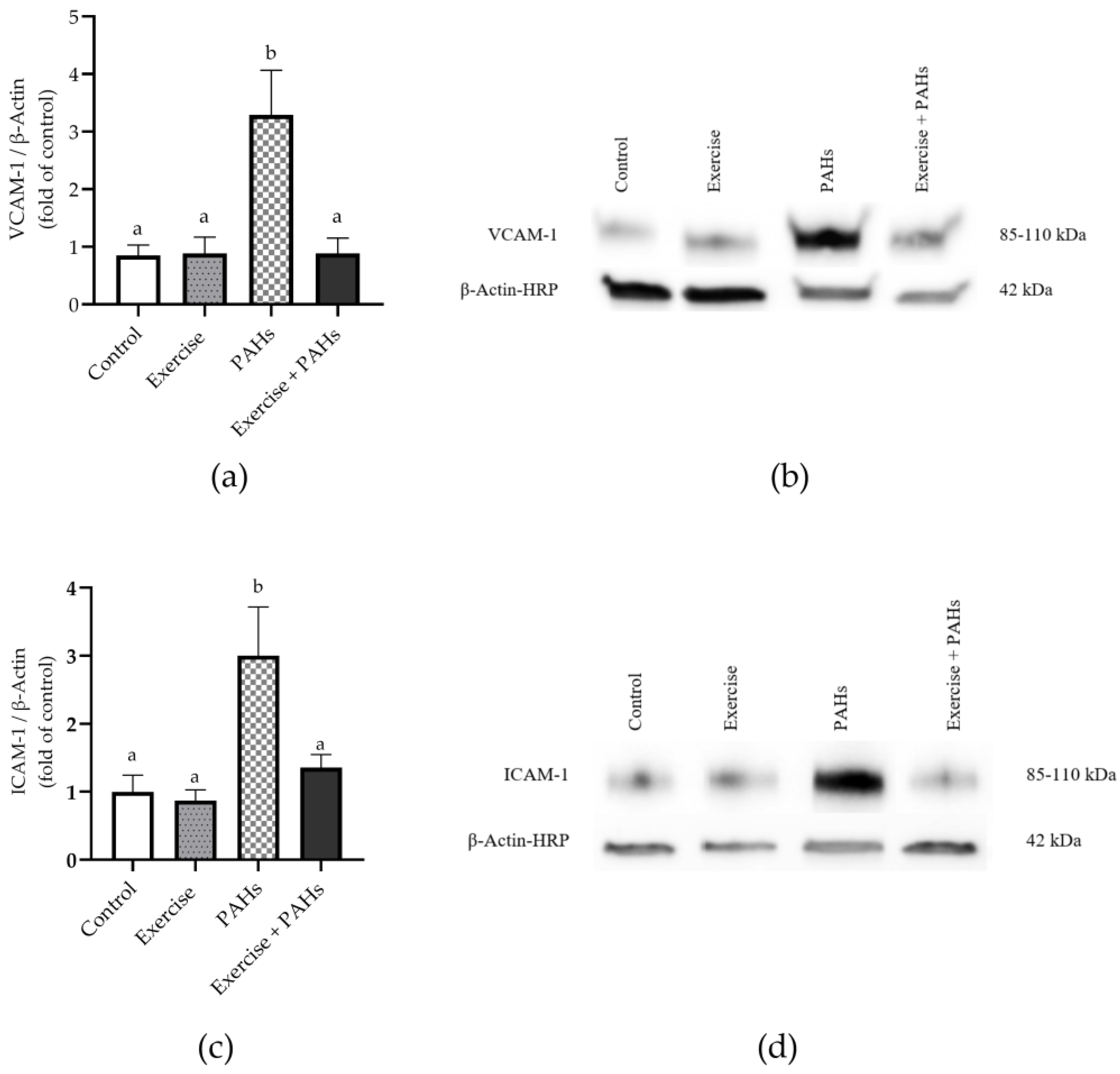
3.5. Protein Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schraufnagel, D.E.; Balmes, J.R.; De Matteis, S.; Hoffman, B.; Kim, W.J.; Perez-Padilla, R.; Rice, M.; Sood, A.; Vanker, A.; Wuebbles, D.J. Health Benefits of Air Pollution Reduction. Ann. Am. Thorac. Soc. 2019, 16, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, P.M.; Harari, S.; Franchini, M. Novel evidence for a greater burden of ambient air pollution on cardiovascular disease. Haematologica 2019, 104, 2349–2357. [Google Scholar] [CrossRef] [PubMed]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public. Health 2020, 8, 14. [Google Scholar] [CrossRef] [PubMed]
- Achilleos, S.; Kioumourtzoglou, M.A.; Wu, C.D.; Schwartz, J.D.; Koutrakis, P.; Papatheodorou, S.I. Acute effects of fine particulate matter constituents on mortality: A systematic review and meta-regression analysis. Environ. Int. 2017, 109, 89–100. [Google Scholar] [CrossRef]
- Oh, S.J.; Yoon, D.; Park, J.H.; Lee, J.H. Effects of Particulate Matter on Healthy Skin: A Comparative Study between High- and Low-Particulate Matter Periods. Ann. Dermatol. 2021, 33, 263–270. [Google Scholar] [CrossRef]
- Loomis, D.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Baan, R.; Mattock, H.; Straif, K. The carcinogenicity of outdoor air pollution. Lancet Oncol. 2013, 14, 1262–1263. [Google Scholar] [CrossRef]
- Jankowska-Kieltyka, M.; Roman, A.; Nalepa, I. The Air We Breathe: Air Pollution as a Prevalent Proinflammatory Stimulus Contributing to Neurodegeneration. Front. Cell Neurosci. 2021, 15, 647643. [Google Scholar] [CrossRef]
- Oliveira, M.; Slezakova, K.; Delerue-Matos, C.; Pereira, M.C.; Morais, S. Children environmental exposure to particulate matter and polycyclic aromatic hydrocarbons and biomonitoring in school environments: A review on indoor and outdoor exposure levels, major sources and health impacts. Environ. Int. 2019, 124, 180–204. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Some Non-Heterocyclic Polycyclic Aromatic Hydrocarbons and Some Related Exposures. In IARC Monogr Eval Carcinog Risks Hum LYON CEDEX 07, France 2010; IARC Working Group on the Evaluation of Carcinogenic Risks to Humans: Lyon, France, 2010; Volume 92, pp. 1–853. [Google Scholar]
- Shen, H.; Huang, Y.; Wang, R.; Zhu, D.; Li, W.; Shen, G.; Wang, B.; Zhang, Y.; Chen, Y.; Lu, Y.; et al. Global atmospheric emissions of polycyclic aromatic hydrocarbons from 1960 to 2008 and future predictions. Environ. Sci. Technol. 2013, 47, 6415–6424. [Google Scholar] [CrossRef]
- Pozo, K.; Estellano, V.H.; Harner, T.; Diaz-Robles, L.; Cereceda-Balic, F.; Etcharren, P.; Pozo, K.; Vidal, V.; Guerrero, F.; Vergara-Fernandez, A. Assessing Polycyclic Aromatic Hydrocarbons (PAHs) using passive air sampling in the atmosphere of one of the most wood-smoke-polluted cities in Chile: The case study of Temuco. Chemosphere 2015, 134, 475–481. [Google Scholar] [CrossRef]
- Schulz, H.; Harder, V.; Ibald-Mulli, A.; Khandoga, A.; Koenig, W.; Krombach, F.; Radykewicz, R.; Stampfl, A.; Thorand, B.; Peters, A. Cardiovascular effects of fine and ultrafine particles. J. Aerosol Med. 2005, 18, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Mallah, M.A.; Mallah, M.A.; Liu, Y.; Xi, H.; Wang, W.; Feng, F.; Zhang, Q. Relationship between Polycyclic Aromatic Hydrocarbons and Cardiovascular Diseases: A Systematic Review. Front. Public. Health 2021, 9, 763706. [Google Scholar] [CrossRef] [PubMed]
- Hansen, D.; Niebauer, J.; Cornelissen, V.; Barna, O.; Neunhäuserer, D.; Stettler, C.; Tonoli, C.; Greco, E.; Fagard, R.; Coninx, K.; et al. Exercise Prescription in Patients with Different Combinations of Cardiovascular Disease Risk Factors: A Consensus Statement from the Expert Working Group. Sports Med. 2018, 48, 1781–1797. [Google Scholar] [CrossRef] [PubMed]
- Villella, M.; Villella, A. Exercise and cardiovascular diseases. Kidney Blood Press. Res. 2014, 39, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Arena, R.; Swift, D.L.; Johannsen, N.M.; Sui, X.; Lee, D.C.; Earnest, C.P.; Church, T.S.; O’Keefe, J.H.; Milani, R.V.; et al. Exercise and the cardiovascular system: Clinical science and cardiovascular outcomes. Circ. Res. 2015, 117, 207–219. [Google Scholar] [CrossRef]
- Lü, J.; Liang, L.; Feng, Y.; Li, R.; Liu, Y. Air Pollution Exposure and Physical Activity in China: Current Knowledge, Public Health Implications, and Future Research Needs. Int. J. Environ. Res. Public. Health 2015, 12, 14887–14897. [Google Scholar] [CrossRef]
- Juneja Gandhi, T.; Garg, P.R.; Kurian, K.; Bjurgert, J.; Sahariah, S.A.; Mehra, S.; Vishwakarma, G. Outdoor Physical Activity in an Air Polluted Environment and Its Effect on the Cardiovascular System-A Systematic Review. Int. J. Environ. Res. Public. Health 2022, 19, 10547. [Google Scholar] [CrossRef]
- Tainio, M.; Jovanovic Andersen, Z.; Nieuwenhuijsen, M.J.; Hu, L.; de Nazelle, A.; An, R.; Garcia, L.M.T.; Goenka, S.; Zapata-Diomedi, B.; Bull, F.; et al. Air pollution, physical activity and health: A mapping review of the evidence. Environ. Int. 2021, 147, 105954. [Google Scholar] [CrossRef]
- Avila, L.C.; Bruggemann, T.R.; Bobinski, F.; da Silva, M.D.; Oliveira, R.C.; Martins, D.F.; Mazzardo-Martins, L.; Duarte, M.M.; de Souza, L.F.; Dafre, A.; et al. Effects of High-Intensity Swimming on Lung Inflammation and Oxidative Stress in a Murine Model of DEP-Induced Injury. PLoS ONE 2015, 10, e0137273. [Google Scholar] [CrossRef]
- Silva-Renno, A.; Baldivia, G.C.; Oliveira-Junior, M.C.; Brandao-Rangel, M.A.R.; El-Mafarjeh, E.; Dolhnikoff, M.; Mauad, T.; Britto, J.M.; Saldiva, P.H.N.; Oliveira, L.V.F.; et al. Exercise Performed Concomitantly with Particulate Matter Exposure Inhibits Lung Injury. Int. J. Sports Med. 2018, 39, 133–140. [Google Scholar] [CrossRef]
- Vieira, R.P.; Toledo, A.C.; Silva, L.B.; Almeida, F.M.; Damaceno-Rodrigues, N.R.; Caldini, E.G.; Santos, A.B.; Rivero, D.H.; Hizume, D.C.; Lopes, F.D.; et al. Anti-inflammatory effects of aerobic exercise in mice exposed to air pollution. Med. Sci. Sports Exerc. 2012, 44, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Hanson, L.R.; Fine, J.M.; Svitak, A.L.; Faltesek, K.A. Intranasal administration of CNS therapeutics to awake mice. J. Vis. Exp. 2013, 74, e4440. [Google Scholar] [CrossRef]
- Morton, D.B.; Griffiths, P.H. Guidelines on the recognition of pain, distress and discomfort in experimental animals and an hypothesis for assessment. Vet. Rec. 1985, 116, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Huenchullan, S.F.; Maharjan, B.R.; Williams, P.F.; Tam, C.S.; McLennan, S.V.; Twigg, S.M. Differential metabolic effects of constant moderate versus high intensity interval training in high-fat fed mice: Possible role of muscle adiponectin. Physiol. Rep. 2018, 6, e13599. [Google Scholar] [CrossRef] [PubMed]
- Ruijter, J.M.; Lorenz, P.; Tuomi, J.M.; Hecker, M.; van den Hoff, M.J. Fluorescent-increase kinetics of different fluorescent reporters used for qPCR depend on monitoring chemistry, targeted sequence, type of DNA input and PCR efficiency. Mikrochim. Acta 2014, 181, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Rojas, G.A.; Saavedra, N.; Saavedra, K.; Hevia, M.; Morales, C.; Lanas, F.; Salazar, L.A. Polycyclic Aromatic Hydrocarbons (PAHs) Exposure Triggers Inflammation and Endothelial Dysfunction in BALB/c Mice: A Pilot Study. Toxics 2022, 10, 497. [Google Scholar] [CrossRef]
- Møller, P.; Christophersen, D.V.; Jacobsen, N.R.; Skovmand, A.; Gouveia, A.C.; Andersen, M.H.; Kermanizadeh, A.; Jensen, D.M.; Danielsen, P.H.; Roursgaard, M.; et al. Atherosclerosis and vasomotor dysfunction in arteries of animals after exposure to combustion-derived particulate matter or nanomaterials. Crit. Rev. Toxicol. 2016, 46, 437–476. [Google Scholar] [CrossRef]
- Yang, W.; Liu, Y.; Yang, G.; Meng, B.; Yi, Z.; Yang, G.; Chen, M.; Hou, P.; Wang, H.; Xu, X. Moderate-Intensity Physical Exercise Affects the Exercise Performance and Gut Microbiota of Mice. Front. Cell Infect. Microbiol. 2021, 11, 712381. [Google Scholar] [CrossRef]
- Lai, Z.; Shan, W.; Li, J.; Min, J.; Zeng, X.; Zuo, Z. Appropriate exercise level attenuates gut dysbiosis and valeric acid increase to improve neuroplasticity and cognitive function after surgery in mice. Mol. Psychiatry 2021, 26, 7167–7187. [Google Scholar] [CrossRef]
- Urdinguio, R.G.; Tejedor, J.R.; Fernández-Sanjurjo, M.; Pérez, R.F.; Peñarroya, A.; Ferrero, C.; Codina-Martínez, H.; Díez-Planelles, C.; Pinto-Hernández, P.; Castilla-Silgado, J.; et al. Physical exercise shapes the mouse brain epigenome. Mol. Metab. 2021, 54, 101398. [Google Scholar] [CrossRef]
- Mai, A.S.; Dos Santos, A.B.; Beber, L.C.C.; Basso, R.D.B.; Sulzbacher, L.M.; Goettems-Fiorin, P.B.; Frizzo, M.N.; Rhoden, C.R.; Ludwig, M.S.; Heck, T.G. Exercise Training under Exposure to Low Levels of Fine Particulate Matter: Effects on Heart Oxidative Stress and Extra-to-Intracellular HSP70 Ratio. Oxid. Med. Cell Longev. 2017, 2017, 9067875. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Zhu, R.; He, X.; Feng, Y.; Yang, L.; Zhu, X.; Deng, Q.; Wu, T.; Zhang, X. Association of plasma IL-6 and Hsp70 with HRV at different levels of PAHs metabolites. PLoS ONE 2014, 9, e92964. [Google Scholar] [CrossRef]
- Zhang, Y.; Dong, S.; Wang, H.; Tao, S.; Kiyama, R. Biological impact of environmental polycyclic aromatic hydrocarbons (ePAHs) as endocrine disruptors. Environ. Pollut. 2016, 213, 809–824. [Google Scholar] [CrossRef] [PubMed]
- Totlandsdal, A.I.; Ovrevik, J.; Cochran, R.E.; Herseth, J.I.; Bolling, A.K.; Lag, M.; Schwarze, P.; Lilleaas, E.; Holme, J.A.; Kubatova, A. The occurrence of polycyclic aromatic hydrocarbons and their derivatives and the proinflammatory potential of fractionated extracts of diesel exhaust and wood smoke particles. J. Environ. Sci. Health A Tox Hazard. Subst. Environ. Eng. 2014, 49, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Stone, V.; Miller, M.R.; Clift, M.J.D.; Elder, A.; Mills, N.L.; Møller, P.; Schins, R.P.F.; Vogel, U.; Kreyling, W.G.; Alstrup Jensen, K.; et al. Nanomaterials Versus Ambient Ultrafine Particles: An Opportunity to Exchange Toxicology Knowledge. Environ. Health Perspect. 2017, 125, 106002. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Samet, J.M.; Bromberg, P.A.; Tong, H. Cardiovascular health impacts of wildfire smoke exposure. Part. Fibre Toxicol. 2021, 18, 2. [Google Scholar] [CrossRef]
- Hassanvand, M.S.; Naddafi, K.; Kashani, H.; Faridi, S.; Kunzli, N.; Nabizadeh, R.; Momeniha, F.; Gholampour, A.; Arhami, M.; Zare, A.; et al. Short-term effects of particle size fractions on circulating biomarkers of inflammation in a panel of elderly subjects and healthy young adults. Environ. Pollut. 2017, 223, 695–704. [Google Scholar] [CrossRef]
- Aragon, M.J.; Chrobak, I.; Brower, J.; Roldan, L.; Fredenburgh, L.E.; McDonald, J.D.; Campen, M.J. Inflammatory and Vasoactive Effects of Serum Following Inhalation of Varied Complex Mixtures. Cardiovasc. Toxicol. 2016, 16, 163–171. [Google Scholar] [CrossRef]
- Gaffen, S.L. An overview of IL-17 function and signaling. Cytokine 2008, 43, 402–407. [Google Scholar] [CrossRef]
- Yang, J.; Chen, Y.; Yu, Z.; Ding, H.; Ma, Z. Changes in gene expression in lungs of mice exposed to traffic-related air pollution. Mol. Cell Probes 2018, 39, 33–40. [Google Scholar] [CrossRef]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, D.D.L.; Latini, A. Exercise-induced immune system response: Anti-inflammatory status on peripheral and central organs. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165823. [Google Scholar] [CrossRef]
- Steyers, C.M., 3rd; Miller, F.J., Jr. Endothelial dysfunction in chronic inflammatory diseases. Int. J. Mol. Sci. 2014, 15, 11324–11349. [Google Scholar] [CrossRef] [PubMed]
- Siragusa, M.; Fleming, I. The eNOS signalosome and its link to endothelial dysfunction. Pflug. Arch. 2016, 468, 1125–1137. [Google Scholar] [CrossRef]
- Lawal, A.O. Air particulate matter induced oxidative stress and inflammation in cardiovascular disease and atherosclerosis: The role of Nrf2 and AhR-mediated pathways. Toxicol. Lett. 2017, 270, 88–95. [Google Scholar] [CrossRef]
- Araujo, J.A.; Barajas, B.; Kleinman, M.; Wang, X.; Bennett, B.J.; Gong, K.W.; Navab, M.; Harkema, J.; Sioutas, C.; Lusis, A.J.; et al. Ambient particulate pollutants in the ultrafine range promote early atherosclerosis and systemic oxidative stress. Circ. Res. 2008, 102, 589–596. [Google Scholar] [CrossRef]
- Bellezza, I.; Giambanco, I.; Minelli, A.; Donato, R. Nrf2-Keap1 signaling in oxidative and reductive stress. Biochim. Biophys. Acta Mol. Cell Res. 2018, 1865, 721–733. [Google Scholar] [CrossRef]
- Suzuki, T.; Yamamoto, M. Molecular basis of the Keap1-Nrf2 system. Free Radic. Biol. Med. 2015, 88, 93–100. [Google Scholar] [CrossRef]
- Telen, M.J. Cellular Adhesion and the Endothelium: E-Selectin, L-Selectin, and Pan-Selectin Inhibitors. Hematol./Oncol. Clin. N. Am. 2014, 28, 341–354. [Google Scholar] [CrossRef]
- Klein, S.G.; Cambier, S.; Hennen, J.; Legay, S.; Serchi, T.; Nelissen, I.; Chary, A.; Moschini, E.; Krein, A.; Blömeke, B.; et al. Endothelial responses of the alveolar barrier in vitro in a dose-controlled exposure to diesel exhaust particulate matter. Part. Fibre Toxicol. 2017, 14, 7. [Google Scholar] [CrossRef]
- Hossain, M.; Mazzone, P.; Tierney, W.; Cucullo, L. In vitro assessment of tobacco smoke toxicity at the BBB: Do antioxidant supplements have a protective role? BMC Neurosci. 2011, 12, 92. [Google Scholar] [CrossRef] [PubMed]
- Montiel-Dávalos, A.; Alfaro-Moreno, E.; López-Marure, R. PM2.5 and PM10 Induce the Expression of Adhesion Molecules and the Adhesion of Monocytic Cells to Human Umbilical Vein Endothelial Cells. Inhal. Toxicol. 2007, 19, 91–98. [Google Scholar] [CrossRef]
- Xue, M.; Qiqige, C.; Zhang, Q.; Zhao, H.; Su, L.; Sun, P.; Zhao, P. Effects of Tumor Necrosis Factor alpha (TNF-alpha) and Interleukina 10 (IL-10) on Intercellular Cell Adhesion Molecule-1 (ICAM-1) and Cluster of Differentiation 31 (CD31) in Human Coronary Artery Endothelial Cells. Med. Sci. Monit. 2018, 24, 4433–4439. [Google Scholar] [CrossRef] [PubMed]
- Haberzettl, P.; O’Toole, T.E.; Bhatnagar, A.; Conklin, D.J. Exposure to Fine Particulate Air Pollution Causes Vascular Insulin Resistance by Inducing Pulmonary Oxidative Stress. Environ. Health Perspect. 2016, 124, 1830–1839. [Google Scholar] [CrossRef] [PubMed]
- Jalava, P.I.; Hirvonen, M.-R.; Sillanpää, M.; Pennanen, A.S.; Happo, M.S.; Hillamo, R.; Cassee, F.R.; Gerlofs-Nijland, M.; Borm, P.J.A.; Schins, R.P.F.; et al. Associations of urban air particulate composition with inflammatory and cytotoxic responses in RAW 246.7 cell line. Inhal. Toxicol. 2009, 21, 994–1006. [Google Scholar] [CrossRef]
- Price, D.T.; Loscalzo, J. Cellular adhesion molecules and atherogenesis. Am. J. Med. 1999, 107, 85–97. [Google Scholar] [CrossRef]
- Fotis, L.; Agrogiannis, G.; Vlachos, I.S.; Pantopoulou, A.; Margoni, A.; Kostaki, M.; Verikokos, C.; Tzivras, D.; Mikhailidis, D.P.; Perrea, D. Intercellular adhesion molecule (ICAM)-1 and vascular cell adhesion molecule (VCAM)-1 at the early stages of atherosclerosis in a rat model. In Vivo 2012, 26, 243–250. [Google Scholar]
- Chistiakov, D.A.; Melnichenko, A.A.; Grechko, A.V.; Myasoedova, V.A.; Orekhov, A.N. Potential of anti-inflammatory agents for treatment of atherosclerosis. Exp. Mol. Pathol. 2018, 104, 114–124. [Google Scholar] [CrossRef]
- Cui, A.; Xiang, M.; Xu, M.; Lu, P.; Wang, S.; Zou, Y.; Qiao, K.; Jin, C.; Li, Y.; Lu, M.; et al. VCAM-1-mediated neutrophil infiltration exacerbates ambient fine particle-induced lung injury. Toxicol. Lett. 2019, 302, 60–74. [Google Scholar] [CrossRef]
- Rui, W.; Guan, L.; Zhang, F.; Zhang, W.; Ding, W. PM2.5-induced oxidative stress increases adhesion molecules expression in human endothelial cells through the ERK/AKT/NF-κB-dependent pathway. J. Appl. Toxicol. 2016, 36, 48–59. [Google Scholar] [CrossRef]
- Bind, M.A.; Baccarelli, A.; Zanobetti, A.; Tarantini, L.; Suh, H.; Vokonas, P.; Schwartz, J. Air pollution and markers of coagulation, inflammation, and endothelial function: Associations and epigene-environment interactions in an elderly cohort. Epidemiology 2012, 23, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Santos, U.P.; Arbex, M.A.; Braga, A.L.F.; Mizutani, R.F.; Cançado, J.E.D.; Terra-Filho, M.; Chatkin, J.M. Environmental air pollution: Respiratory effects. J. Bras. Pneumol. 2021, 47, e20200267. [Google Scholar] [CrossRef] [PubMed]
- Giorgini, P.; Rubenfire, M.; Bard, R.L.; Jackson, E.A.; Ferri, C.; Brook, R.D. Air Pollution and Exercise: A review of the cardiovascular implications for health care professionALS. J. Cardiopulm. Rehabil. Prev. 2016, 36, 84–95. [Google Scholar] [CrossRef]
- Kocot, K.; Zejda, J.E. Acute cardiorespiratory response to ambient air pollution exposure during short-term physical exercise in young males. Environ. Res. 2021, 195, 110746. [Google Scholar] [CrossRef] [PubMed]
- Laeremans, M.; Dons, E.; Avila-Palencia, I.; Carrasco-Turigas, G.; Orjuela, J.P.; Anaya, E.; Cole-Hunter, T.; de Nazelle, A.; Nieuwenhuijsen, M.; Standaert, A.; et al. Short-term effects of physical activity, air pollution and their interaction on the cardiovascular and respiratory system. Environ. Int. 2018, 117, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Götschi, T.; Int Panis, L.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- Alessio, H.M.; Bassett, D.R.; Bopp, M.J.; Parr, B.B.; Patch, G.S.; Rankin, J.W.; Rojas-Rueda, D.; Roti, M.W.; Wojcik, J.R. Climate Change, Air Pollution, and Physical Inactivity: Is Active Transportation Part of the Solution? Med. Sci. Sports Exerc. 2021, 53, 1170–1178. [Google Scholar] [CrossRef]
- Avila-Palencia, I.; Laeremans, M.; Hoffmann, B.; Anaya-Boig, E.; Carrasco-Turigas, G.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Götschi, T.; Int Panis, L.; et al. Effects of physical activity and air pollution on blood pressure. Environ. Res. 2019, 173, 387–396. [Google Scholar] [CrossRef]
- Fisher, J.E.; Loft, S.; Ulrik, C.S.; Raaschou-Nielsen, O.; Hertel, O.; Tjønneland, A.; Overvad, K.; Nieuwenhuijsen, M.J.; Andersen, Z.J. Physical Activity, Air Pollution, and the Risk of Asthma and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2016, 194, 855–865. [Google Scholar] [CrossRef]
- Kocot, K. The effect of upper respiratory allergy on acute respiratory response to ambient air pollution during physical exercise. Int. J. Occup. Med. Environ. Health 2020, 33, 649–660. [Google Scholar] [CrossRef]
- Guo, C.; Yu, T.; Chang, L.Y.; Lin, C.; Yang, H.T.; Bo, Y.; Zeng, Y.; Tam, T.; Lau, A.K.H.; Lao, X.Q. Effects of air pollution and habitual exercise on the risk of death: A longitudinal cohort study. CMAJ 2021, 193, E1240–E1249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Hoek, G.; Chang, L.-y.; Chan, T.-C.; Guo, C.; Chuang, Y.C.; Chan, J.; Lin, C.; Jiang, W.K.; Guo, Y.; et al. Particulate matter air pollution, physical activity and systemic inflammation in Taiwanese adults. Int. J. Hyg. Environ. Health 2018, 221, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Elliott, E.G.; Laden, F.; James, P.; Rimm, E.B.; Rexrode, K.M.; Hart, J.E. Interaction between Long-Term Exposure to Fine Particulate Matter and Physical Activity, and Risk of Cardiovascular Disease and Overall Mortality in U.S. Women. Environ. Health Perspect. 2020, 128, 127012. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Accession Number | Sequence Forward | Sequence Reverse | Fragment Length (bp) |
|---|---|---|---|---|
| ICAM-1 | NM_010493 | TTCTCATGCCGCACAGAACT | TCCTGGCCTCGGAGACATTA | 73 |
| VCAM-1 | NM_011693 | CTGGGAAGCTGGAACGAAGT | GCCAAACACTTGACCGTGAC | 115 |
| E-selectin | NM_011345 | AGCCTGCCATGTGGTTGAAT | CTTTGCATGATGGCGTCTCG | 197 |
| eNOS | NM_008713 | GCTCCCAACTGGACCATCTC | TCTTGCACGTAGGTCTTGGG | 121 |
| Nrf2 | NM_010902 | GATGACCATGAGTCGCTTGC | CCTGATGAGGGGCAGTGAAG | 73 |
| Ahr | NM_013464 | TAAAGTCCACCCCTGCTGAC | CATTCAGCGCCTGTAACAAGA | 108 |
| RelA | NM_009045 | CCTGGAGCAAGCCATTAGC | CGCACTGCATTCAAGTCATAG | 99 |
| IL-6 | NM_031168 | CCCCAATTTCCAATGCTCTCC | CGCACTAGGTTTGCCGAGTA | 141 |
| TNF-α | NM_013693 | ATGGCCTCCCTCTCATCAGT | TTTGCTACGACGTGGGCTAC | 97 |
| RPL32 | NM_172086 | TAAGCGAAACTGGCGGAAAC | CATCAGGATCTGGCCCTTGA | 73 |
| B2m | NM_009735 | ACTGACCGGCCTGTATGCTA | CAATGTGAGGCGGGTGGAA | 125 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas, G.A.; Saavedra, N.; Morales, C.; Saavedra, K.; Lanas, F.; Salazar, L.A. Modulation of the Cardiovascular Effects of Polycyclic Aromatic Hydrocarbons: Physical Exercise as a Protective Strategy. Toxics 2023, 11, 844. https://doi.org/10.3390/toxics11100844
Rojas GA, Saavedra N, Morales C, Saavedra K, Lanas F, Salazar LA. Modulation of the Cardiovascular Effects of Polycyclic Aromatic Hydrocarbons: Physical Exercise as a Protective Strategy. Toxics. 2023; 11(10):844. https://doi.org/10.3390/toxics11100844
Chicago/Turabian StyleRojas, Gabriel A., Nicolás Saavedra, Cristian Morales, Kathleen Saavedra, Fernando Lanas, and Luis A. Salazar. 2023. "Modulation of the Cardiovascular Effects of Polycyclic Aromatic Hydrocarbons: Physical Exercise as a Protective Strategy" Toxics 11, no. 10: 844. https://doi.org/10.3390/toxics11100844