
Short-Term Exposure to PM2.5 Chemical Components and Depression Outpatient Visits: A Case-Crossover Analysis in Three Chinese Cities



Abstract
:
1. Introduction
2. Material and Methods
2.1. Study Area
2.2. Outcome
2.3. Air Pollution Exposure Assessment
2.4. Statistical Analysis
3. Results
3.1. Descriptive Results
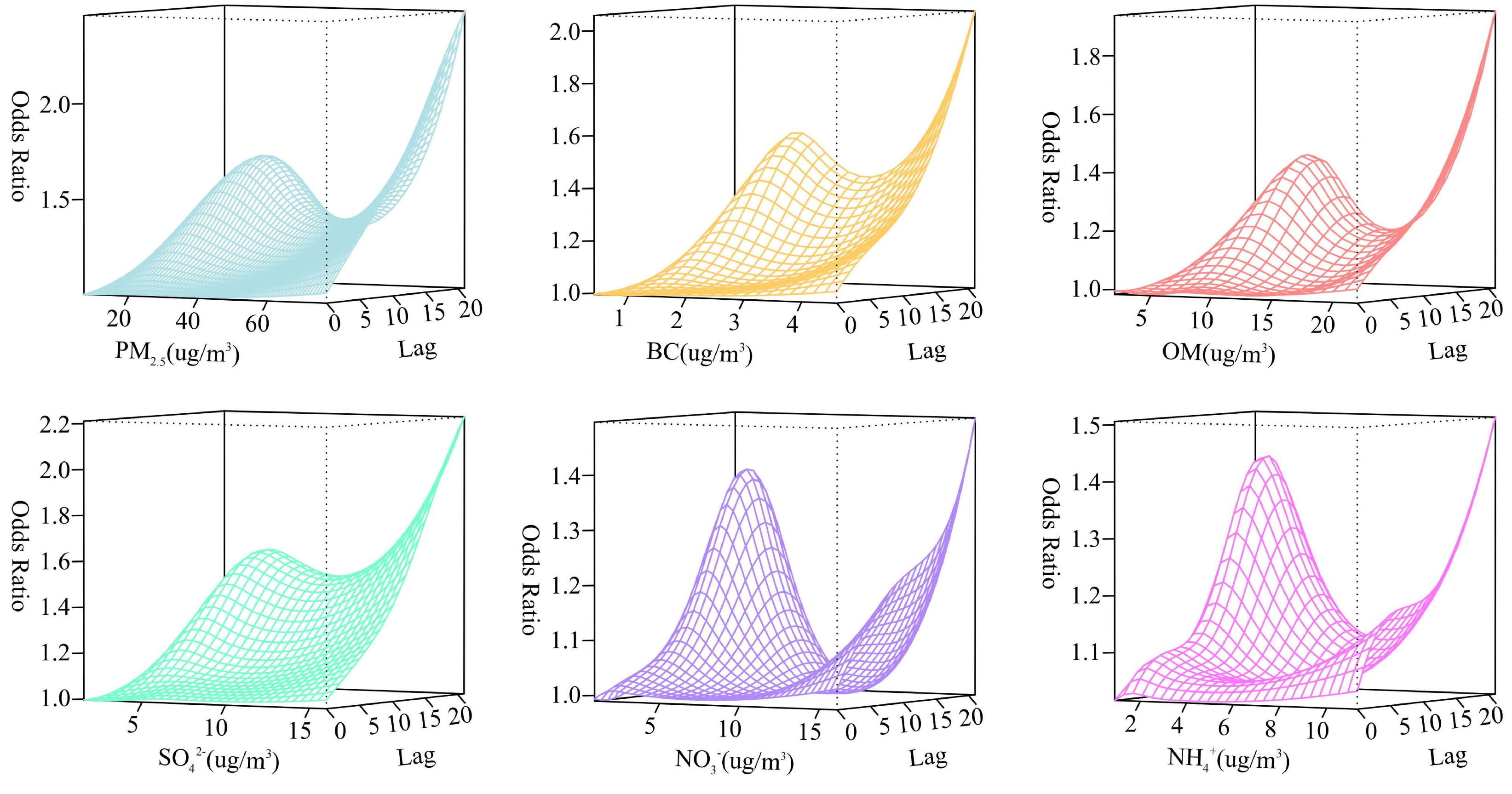
3.2. The Associations of PM2.5 and Its Chemical Components with Outpatient Visits for Depression
3.3. Associations by Gender and Age
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 31 March 2023).
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Yu, Y.; Kou, C.; Xu, X.; Lu, J.; et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef]
- Lu, J.; Xu, X.; Huang, Y.; Li, T.; Ma, C.; Xu, G.; Yin, H.; Xu, X.; Ma, Y.; Wang, L.; et al. Prevalence of depressive disorders and treatment in China: A cross-sectional epidemiological study. Lancet Psychiatry 2021, 8, 981–990. [Google Scholar] [CrossRef]
- Fu, Z.; Liu, Q.; Liang, J.; Weng, Z.; Li, W.; Xu, J.; Zhang, X.; Xu, C.; Huang, T.; Gu, A. Air pollution, genetic factors and the risk of depression. Sci. Total Environ. 2022, 850, 158001. [Google Scholar] [CrossRef]
- Hammen, C. Risk Factors for Depression: An Autobiographical Review. Annu. Rev. Clin. Psychol. 2018, 14, 1–28. [Google Scholar] [CrossRef]
- Buckman, J.E.J.; Saunders, R.; Stott, J.; Cohen, Z.D.; Arundell, L.L.; Eley, T.C.; Hollon, S.D.; Kendrick, T.; Ambler, G.; Watkins, E.; et al. Socioeconomic Indicators of Treatment Prognosis for Adults with Depression: A Systematic Review and Individual Patient Data Meta-analysis. JAMA Psychiatry 2022, 79, 406–416. [Google Scholar] [CrossRef]
- Gao, X.; Jiang, M.; Huang, N.; Guo, X.; Huang, T. Long-Term Air Pollution, Genetic Susceptibility, and the Risk of Depression and Anxiety: A Prospective Study in the UK Biobank Cohort. Environ. Health Perspect. 2023, 131, 17002. [Google Scholar] [CrossRef]
- Wei, F.; Wu, M.; Qian, S.; Li, D.; Jin, M.; Wang, J.; Shui, L.; Lin, H.; Tang, M.; Chen, K. Association between short-term exposure to ambient air pollution and hospital visits for depression in China. Sci. Total Environ. 2020, 724, 138207. [Google Scholar] [CrossRef]
- Tsai, S.S.; Chiu, Y.W.; Weng, Y.H.; Yang, C.Y. Relationship between fine particulate air pollution and hospital admissions for depression: A case-crossover study in Taipei. J. Toxicol. Environ. Health Part A 2021, 84, 702–709. [Google Scholar] [CrossRef]
- Borroni, E.; Pesatori, A.C.; Bollati, V.; Buoli, M.; Carugno, M. Air pollution exposure and depression: A comprehensive updated systematic review and meta-analysis. Environ. Pollut. 2022, 292, 118245. [Google Scholar] [CrossRef]
- Ju, K.; Lu, L.; Liao, W.; Yang, C.; Xu, Z.; Wang, W.; Zhao, L.; Pan, J. Long-term exposure of PM(2.5) components on the adults’ depressive symptoms in China—Evidence from a representative longitudinal nationwide cohort. Sci. Total Environ. 2023, 857, 159434. [Google Scholar] [CrossRef]
- Shen, M.; Gu, X.; Li, S.; Yu, Y.; Zou, B.; Chen, X. Exposure to black carbon is associated with symptoms of depression: A retrospective cohort study in college students. Environ. Int. 2021, 157, 106870. [Google Scholar] [CrossRef] [PubMed]
- Guangdong Statistical Yearbook. Available online: http://stats.gd.gov.cn/gdtjnj/content/post_4035145.html (accessed on 25 October 2022).
- Geng, G.; Xiao, Q.; Liu, S.; Liu, X.; Cheng, J.; Zheng, Y.; Xue, T.; Tong, D.; Zheng, B.; Peng, Y.; et al. Tracking Air Pollution in China: Near Real-Time PM(2.5) Retrievals from Multisource Data Fusion. Environ. Sci. Technol. 2021, 55, 12106–12115. [Google Scholar] [CrossRef] [PubMed]
- Geng, G.; Zhang, Q.; Tong, D.; Li, M.; Zheng, Y.; Wang, S.; He, K. Chemical composition of ambient PM2. 5 over China and relationship to precursor emissions during 2005–2012. Atmos. Chem. Phys. 2017, 17, 9187–9203. [Google Scholar] [CrossRef]
- Muñoz-Sabater, J.; Dutra, E.; Agustí-Panareda, A.; Albergel, C.; Arduini, G.; Balsamo, G.; Boussetta, S.; Choulga, M.; Harrigan, S.; Hersbach, H.; et al. ERA5-Land: A state-of-the-art global reanalysis dataset for land applications. Earth Syst. Sci. Data 2021, 13, 4349–4383. [Google Scholar] [CrossRef]
- Ren, M.; Li, N.; Wang, Z.; Liu, Y.; Chen, X.; Chu, Y.; Li, X.; Zhu, Z.; Tian, L.; Xiang, H. The short-term effects of air pollutants on respiratory disease mortality in Wuhan, China: Comparison of time-series and case-crossover analyses. Sci. Rep. 2017, 7, 40482. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Kang, J.M.; Cho, S.E.; Jung, J.; Kang, S.G. Significant association between increased risk of emergency department visits for psychiatric disorders and air pollutants in South Korea. J. Expo. Sci. Environ. Epidemiol. 2023, 33, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Liu, H.; Li, H.; Liu, J.; Guo, X.; Yuan, J.; Hu, Y.; Wang, J.; Lu, L. Ambient concentrations of particulate matter and hospitalization for depression in 26 Chinese cities: A case-crossover study. Environ. Int. 2018, 114, 115–122. [Google Scholar] [CrossRef]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [CrossRef]
- Yang, H.; Ge, A.; Xie, H.; Li, W.; Qin, Y.; Yang, W.; Wang, D.; Gu, W.; Wang, X. Effects of Ambient Air Pollution on Precocious Puberty: A Case-Crossover Analysis in Nanjing, China. J. Clin. Med. 2022, 12, 282. [Google Scholar] [CrossRef]
- Zhang, S.; Yang, Y.; Xie, X.; Li, H.; Han, R.; Hou, J.; Sun, J.; Qian, Z.M.; Wu, S.; Huang, C.; et al. The effect of temperature on cause-specific mental disorders in three subtropical cities: A case-crossover study in China. Environ. Int. 2020, 143, 105938. [Google Scholar] [CrossRef]
- Yu, G.; Li, Y.; Cai, J.; Yu, D.; Tang, J.; Zhai, W.; Wei, Y.; Chen, S.; Chen, Q.; Qin, J. Short-term effects of meteorological factors and air pollution on childhood hand-foot-mouth disease in Guilin, China. Sci. Total Environ. 2019, 646, 460–470. [Google Scholar] [CrossRef]
- Shi, W.; Li, T.; Zhang, Y.; Sun, Q.; Chen, C.; Wang, J.; Fang, J.; Zhao, F.; Du, P.; Shi, X. Depression and Anxiety Associated with Exposure to Fine Particulate Matter Constituents: A Cross-Sectional Study in North China. Environ. Sci. Technol. 2020, 54, 16006–16016. [Google Scholar] [CrossRef]
- Ramondt, S.; Ramírez, A.S. Media Reporting on Air Pollution: Health Risk and Precautionary Measures in National and Regional Newspapers. Int. J. Environ. Res. Public Health 2020, 17, 6516. [Google Scholar] [CrossRef]
- Deng, X.; Fu, J.; Song, Y.; Xu, B.; Ji, Z.; Guo, Q.; Ma, S. Glucocorticoid receptor dysfunction orchestrates inflammasome effects on chronic obstructive pulmonary disease-induced depression: A potential mechanism underlying the cross talk between lung and brain. Brain Behav. Immun. 2019, 79, 195–206. [Google Scholar] [CrossRef]
- Qiu, H.; Zhu, X.; Wang, L.; Pan, J.; Pu, X.; Zeng, X.; Zhang, L.; Peng, Z.; Zhou, L. Attributable risk of hospital admissions for overall and specific mental disorders due to particulate matter pollution: A time-series study in Chengdu, China. Environ. Res. 2019, 170, 230–237. [Google Scholar] [CrossRef]
- Giannakopoulou, O.; Lin, K.; Meng, X.; Su, M.H.; Kuo, P.H.; Peterson, R.E.; Awasthi, S.; Moscati, A.; Coleman, J.R.I.; Bass, N.; et al. The Genetic Architecture of Depression in Individuals of East Asian Ancestry: A Genome-Wide Association Study. JAMA Psychiatry 2021, 78, 1258–1269. [Google Scholar] [CrossRef]
- Babadjouni, R.M.; Hodis, D.M.; Radwanski, R.; Durazo, R.; Patel, A.; Liu, Q.; Mack, W.J. Clinical effects of air pollution on the central nervous system; a review. J. Clin. Neurosci. 2017, 43, 16–24. [Google Scholar] [CrossRef]
- Blier, P. Neurobiology of depression and mechanism of action of depression treatments. J. Clin. Psychiatry 2016, 77, e319. [Google Scholar] [CrossRef]
- Reuben, A.; Arseneault, L.; Beddows, A.; Beevers, S.D.; Moffitt, T.E.; Ambler, A.; Latham, R.M.; Newbury, J.B.; Odgers, C.L.; Schaefer, J.D.; et al. Association of Air Pollution Exposure in Childhood and Adolescence with Psychopathology at the Transition to Adulthood. JAMA Netw. Open 2021, 4, e217508. [Google Scholar] [CrossRef]
- Fang, Y.; Chen, Y.; Huang, G.; Hu, L.; Tian, C.; Xie, J.; Lin, J.; Lin, T. Particulate and Dissolved Black Carbon in Coastal China Seas: Spatiotemporal Variations, Dynamics, and Potential Implications. Environ. Sci. Technol. 2021, 55, 788–796. [Google Scholar] [CrossRef]
- Cheng, Z.; Luo, L.; Wang, S.; Wang, Y.; Sharma, S.; Shimadera, H.; Wang, X.; Bressi, M.; de Miranda, R.M.; Jiang, J.; et al. Status and characteristics of ambient PM2.5 pollution in global megacities. Environ. Int. 2016, 89–90, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Vaezzadeh, V.; Yi, X.; Rais, F.R.; Bong, C.W.; Thomes, M.W.; Lee, C.W.; Zakaria, M.P.; Wang, A.J.; Zhong, G.; Zhang, G. Distribution of black carbon and PAHs in sediments of Peninsular Malaysia. Mar. Pollut. Bull. 2021, 172, 112871. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.S.; Duan, F.K.; He, K.B.; Ma, Y.L. Review on recent progress in observations, source identifications and countermeasures of PM2.5. Environ. Int. 2016, 86, 150–170. [Google Scholar] [CrossRef] [PubMed]
- Rahman, H.H.; Niemann, D.; Munson-McGee, S.H. Association among urinary polycyclic aromatic hydrocarbons and depression: A cross-sectional study from NHANES 2015–2016. Environ. Sci. Pollut. Res. Int. 2022, 29, 13089–13097. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wen, Y.; Zhang, S.; Zheng, G.; Zheng, H.; Chang, X.; Huang, C.; Wang, S.; Wu, Y.; Hao, J. Vehicular Ammonia Emissions Significantly Contribute to Urban PM(2.5) Pollution in Two Chinese Megacities. Environ. Sci. Technol. 2023, 57, 2698–2705. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Huang, X.; Song, Y.; Tang, J.; Cao, J.; Zhang, X.; Zhang, Q.; Wang, S.; Xu, T.; Kang, L.; et al. Ammonia emission control in China would mitigate haze pollution and nitrogen deposition, but worsen acid rain. Proc. Natl. Acad. Sci. USA 2019, 116, 7760–7765. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Lau, W.K.W.; Fung, T.K.H.; Lau, B.W.M.; Chau, B.K.H.; Liang, Y.; Wang, Z.; So, K.F.; Wang, T.; Chan, C.C.H.; et al. PM(2.5) Exposure Suppresses Dendritic Maturation in Subgranular Zone in Aged Rats. Neurotox. Res. 2017, 32, 50–57. [Google Scholar] [CrossRef]
- Ku, T.; Ji, X.; Zhang, Y.; Li, G.; Sang, N. PM2.5, SO2 and NO2 co-exposure impairs neurobehavior and induces mitochondrial injuries in the mouse brain. Chemosphere 2016, 163, 27–34. [Google Scholar] [CrossRef]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Deng, M.G.; Liu, F.; Liang, Y.; Wang, K.; Nie, J.Q.; Liu, J. Association between frailty and depression: A bidirectional Mendelian randomization study. Sci. Adv. 2023, 9, eadi3902. [Google Scholar] [CrossRef]
- Marquet, O.; Tello-Barsocchini, J.; Couto-Trigo, D.; Gómez-Varo, I.; Maciejewska, M. Comparison of static and dynamic exposures to air pollution, noise, and greenness among seniors living in compact-city environments. Int. J. Health Geogr. 2023, 22, 3. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Huizhou | Shenzhen | Zhaoqing | All |
|---|---|---|---|---|
| Gender | ||||
| Male | 13 (47.92%) | 74 (42.28%) | 11 (41.45%) | 98 (43.17%) |
| Female | 14 (52.08%) | 100 (57.72%) | 15 (58.55%) | 129 (56.83%) |
| Age | ||||
| <60 years | 24 (87.93%) | 158 (90.80%) | 21 (82.28%) | 203 (89.43%) |
| ≥60 years | 3 (12.07%) | 16 (9.20%) | 5 (17.72%) | 24 (10.57%) |
| Case Day | Control Day | |
|---|---|---|
| No. of days | 247,281 | 931,355 |
| Meteorological factors | ||
| Daily temperature (°C) | 21.94 ± 5.63 | 22.03 ± 5.56 |
| Relative humidity (%) | 78.49 ± 12.11 | 78.63 ± 12.08 |
| PM2.5 and its chemical components | ||
| PM2.5 (μg/m3) | 29.03 ± 15.00 | 28.96 ± 15.07 |
| BC (μg/m3) | 1.71 ± 0.94 | 1.71 ± 0.94 |
| OM (μg/m3) | 8.11 ± 4.50 | 8.10 ± 4.52 |
| SO42− (μg/m3) | 6.00 ± 3.29 | 6.00 ± 3.31 |
| NO3− (μg/m3) | 3.86 ± 3.29 | 3.83 ± 3.28 |
| NH4+ (μg/m3) | 3.00 ± 2.32 | 2.98 ± 2.31 |
| Concentration (μg/m3) | Odds Ratio (95% CI) | |||
|---|---|---|---|---|
| Lag 0–7 | Lag 0–14 | Lag 0–21 | ||
| PM2.5 | ||||
| 25th | 18.1 | 1.207 (1.086, 1.341) | 1.528 (1.305, 1.790) | 1.525 (1.231, 1.889) |
| 50th | 25.9 | 1.181 (1.072, 1.302) | 1.541 (1.332, 1.783) | 1.607 (1.321, 1.956) |
| 75th | 36.5 | 1.127 (1.025, 1.239) | 1.374 (1.193, 1.583) | 1.403 (1.160, 1.697) |
| BC | ||||
| 25th | 1.0 | 0.941 (0.873, 1.013) | 0.787 (0.704, 0.879) | 0.684 (0.589, 0.795) |
| 50th | 1.5 | 0.941 (0.873, 1.013) | 0.787 (0.704, 0.879) | 0.684 (0.589, 0.795) |
| 75th | 2.2 | 0.962 (0.917, 1.009) | 0.849 (0.791, 0.912) | 0.766 (0.697, 0.843) |
| OM | ||||
| 25th | 4.7 | 1.036 (0.969, 1.107) | 1.181 (1.069, 1.305) | 1.231 (1.076, 1.408) |
| 50th | 7.2 | 1.044 (0.978, 1.114) | 1.279 (1.161, 1.409) | 1.417 (1.245, 1.612) |
| 75th | 10.4 | 1.007 (0.946, 1.072) | 1.172 (1.069, 1.286) | 1.277 (1.130, 1.443) |
| SO42− | ||||
| 25th | 3.5 | 1.025 (1.006, 1.045) | 1.077 (1.046, 1.109) | 1.098 (1.057, 1.142) |
| 50th | 5.4 | 1.067 (1.016, 1.121) | 1.218 (1.129, 1.313) | 1.287 (1.164, 1.422) |
| 75th | 7.8 | 1.090 (1.023, 1.161) | 1.302 (1.182, 1.435) | 1.418 (1.247, 1.613) |
| NO3− | ||||
| 25th | 1.7 | 0.617 (0.551, 0.690) | 0.459 (0.385, 0.547) | 0.285 (0.226, 0.361) |
| 50th | 2.8 | 0.632 (0.567, 0.703) | 0.487 (0.411, 0.577) | 0.314 (0.250, 0.393) |
| 75th | 4.7 | 0.655 (0.588, 0.729) | 0.539 (0.455, 0.638) | 0.361 (0.288, 0.452) |
| NH4+ | ||||
| 25th | 1.5 | 0.942 (0.905, 0.981) | 0.867 (0.815, 0.921) | 0.820 (0.755, 0.891) |
| 50th | 2.3 | 0.990 (0.983, 0.996) | 0.975 (0.965, 0.985) | 0.966 (0.953, 0.979) |
| 75th | 3.6 | 1.025 (1.009, 1.040) | 1.065 (1.041, 1.090) | 1.086 (1.054, 1.120) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhuang, Z.; Li, D.; Zhang, S.; Hu, Z.; Deng, W.; Lin, H. Short-Term Exposure to PM2.5 Chemical Components and Depression Outpatient Visits: A Case-Crossover Analysis in Three Chinese Cities. Toxics 2024, 12, 136. https://doi.org/10.3390/toxics12020136
Zhuang Z, Li D, Zhang S, Hu Z, Deng W, Lin H. Short-Term Exposure to PM2.5 Chemical Components and Depression Outpatient Visits: A Case-Crossover Analysis in Three Chinese Cities. Toxics. 2024; 12(2):136. https://doi.org/10.3390/toxics12020136
Chicago/Turabian StyleZhuang, Zitong, Dan Li, Shiyu Zhang, Zhaoyang Hu, Wenfeng Deng, and Hualiang Lin. 2024. "Short-Term Exposure to PM2.5 Chemical Components and Depression Outpatient Visits: A Case-Crossover Analysis in Three Chinese Cities" Toxics 12, no. 2: 136. https://doi.org/10.3390/toxics12020136