
Cannabis Use in Physicians: A Systematic Review and Meta-Analysis

 , ,
, , 
 ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Methods
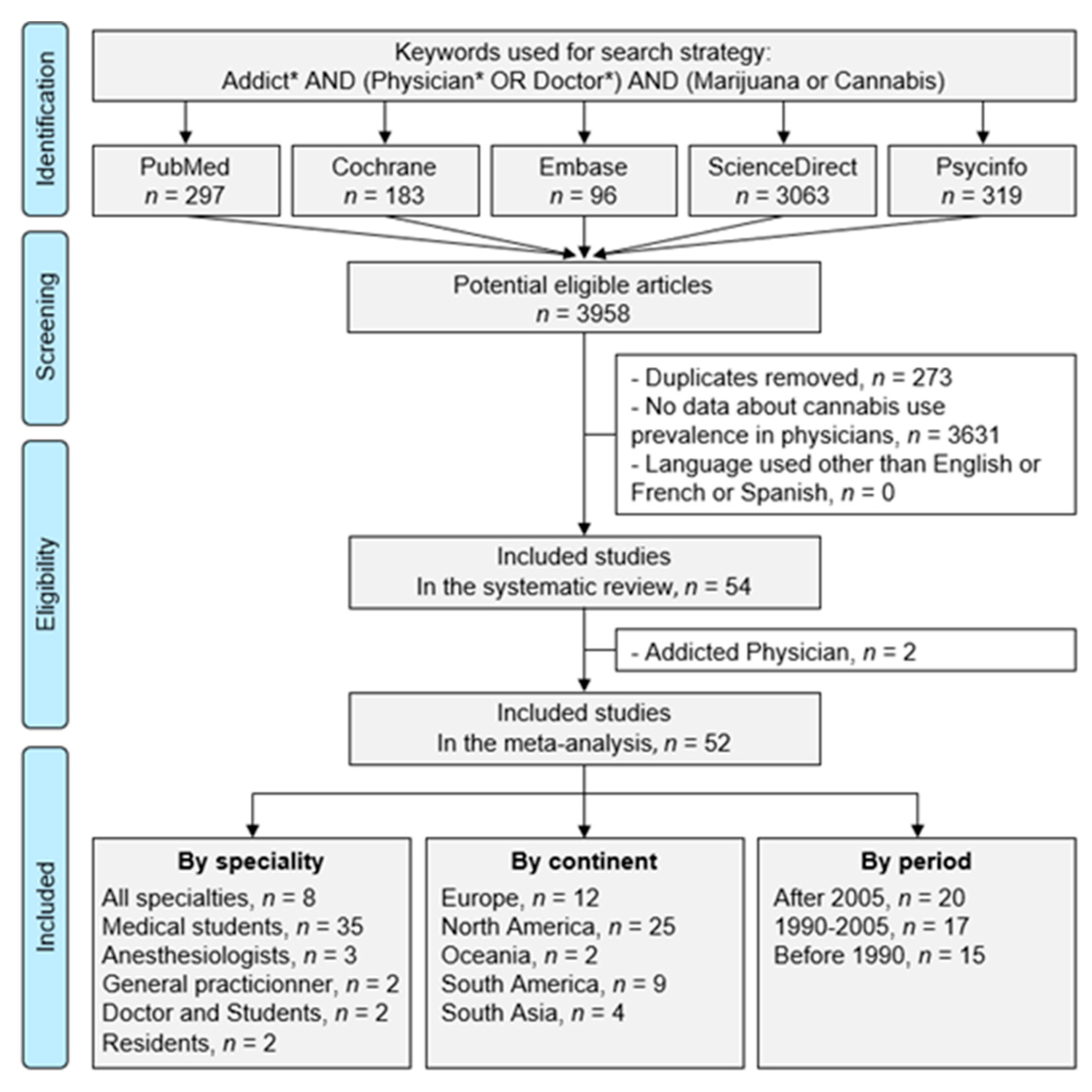
2.1. Literature Search
2.2. Data Extraction
2.3. Quality of Assessment
2.4. Statistical Considerations
3. Results
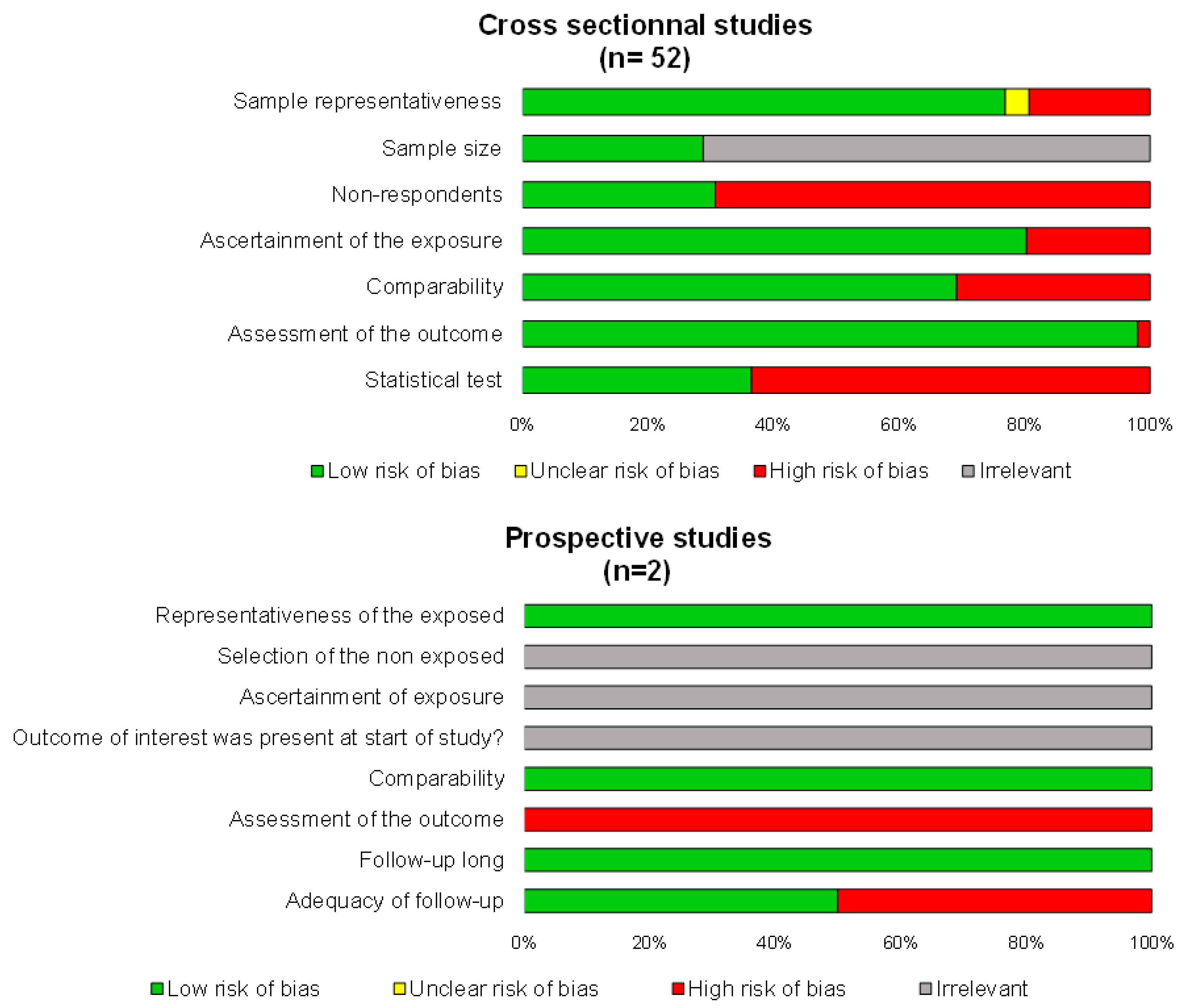
3.1. Quality of Articles
3.2. Study Designs and Objectives
3.3. Recruitment of Physicians
3.4. Populations Studied
3.5. Cannabis Use Assessment
3.6. Frequency of Use and Period of Data Collection
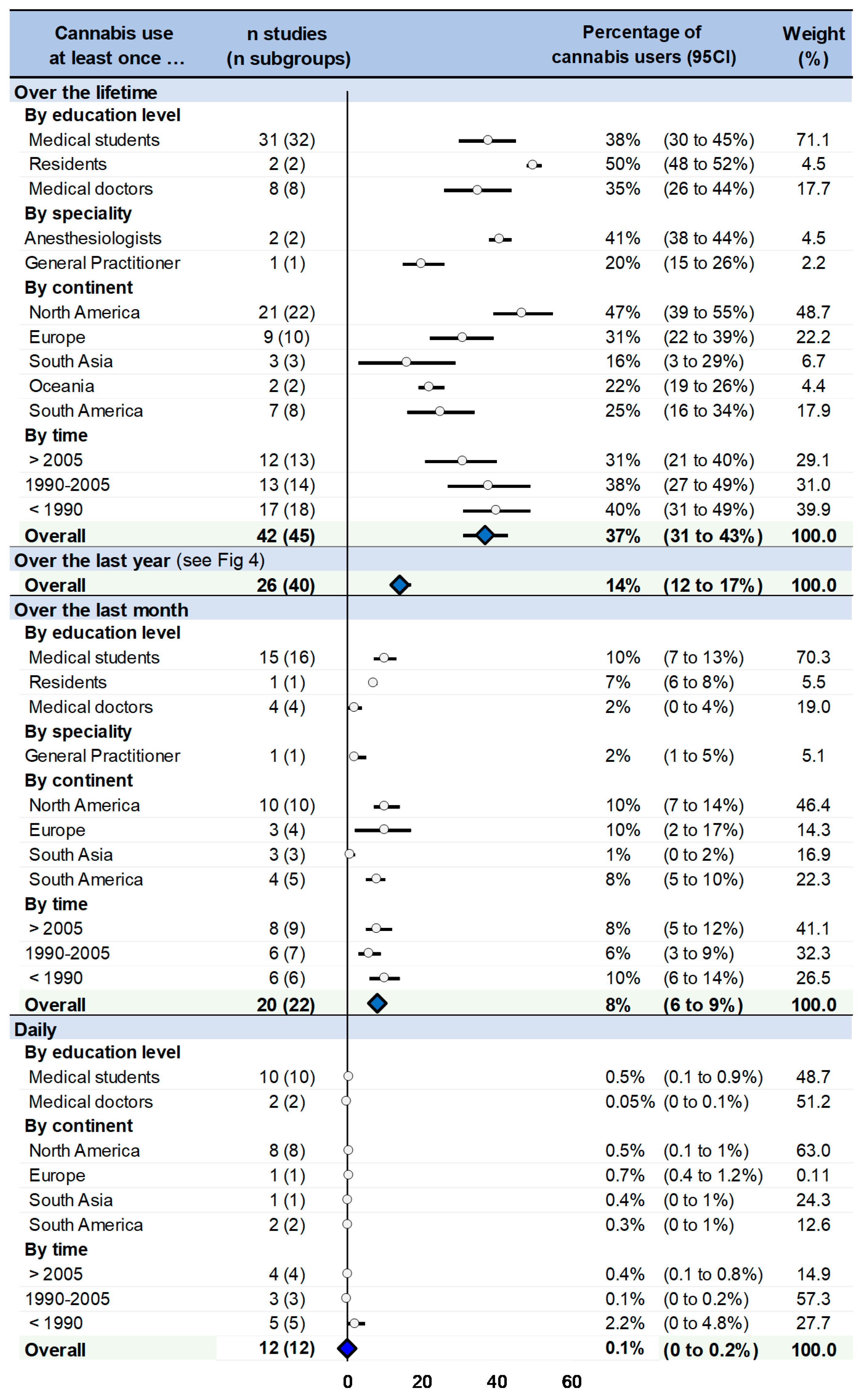
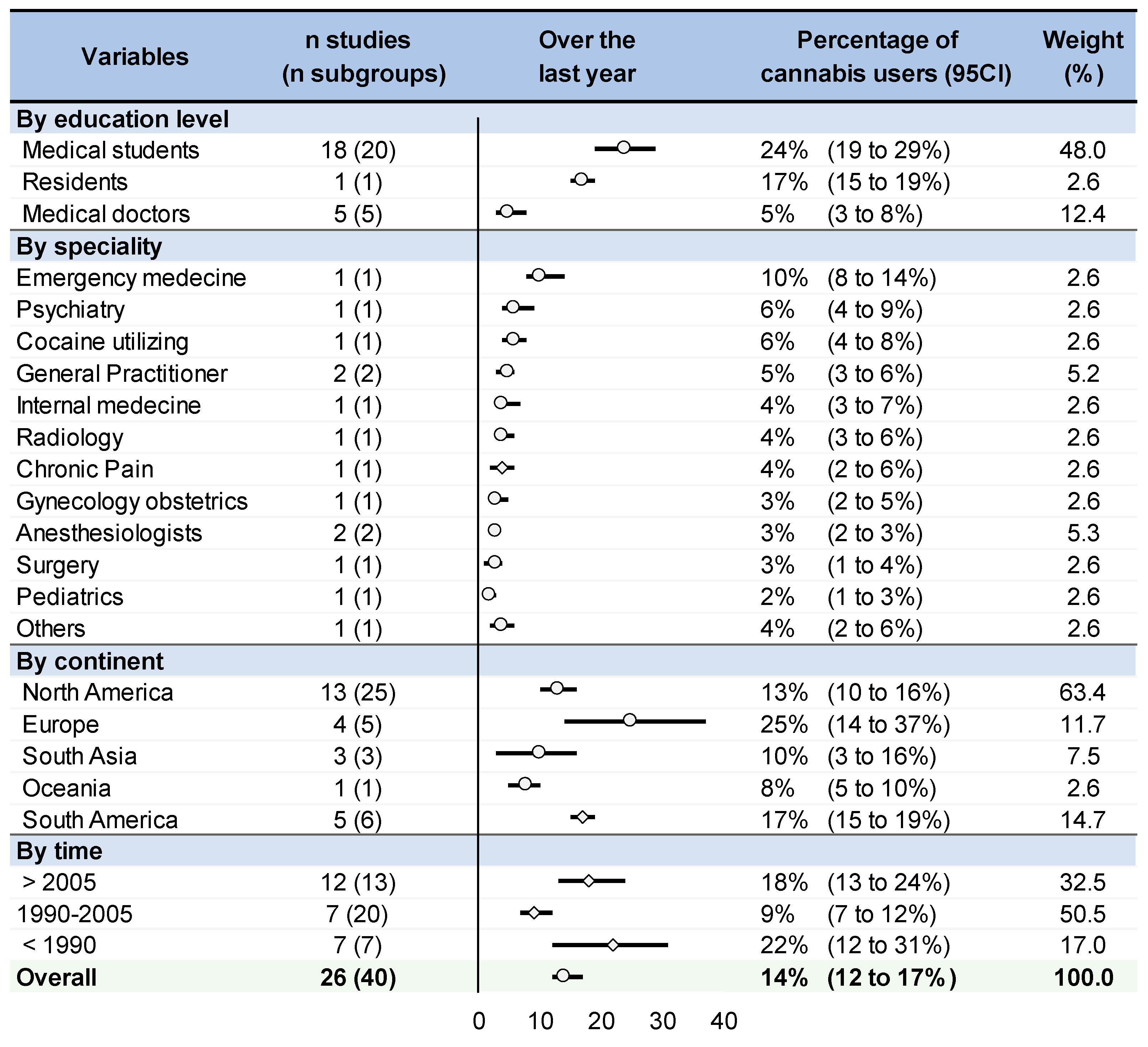
3.7. Meta-Analysis on the Prevalence of Cannabis Use in Physicians
3.8. Meta-Regressions
4. Discussion
4.1. Cannabis Use by Physicians: A Public Health Issue
4.2. From Daily to Lifetime Use
4.3. Medical Students as the Heaviest Consumers
4.4. Cannabis Use Worldwide and through Time
4.5. Other Influencing Variables
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- GBD 2016 Alcohol and Drug Use Collaborators. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 2018, 5, 987–1012. [Google Scholar] [CrossRef]
- Daniulaityte, R.; Zatreh, M.Y.; Lamy, F.R.; Nahhas, R.W.; Martins, S.S.; Sheth, A.; Carlson, R.G. A Twitter-based survey on marijuana concentrate use. Drug Alcohol Depend. 2018, 187, 155–159. [Google Scholar] [CrossRef]
- Callaghan, R.C.; Sanches, M.; Benny, C.; Stockwell, T.; Sherk, A.; Kish, S.J. Who consumes most of the cannabis in Canada? Profiles of cannabis consumption by quantity. Drug Alcohol Depend. 2019, 205, 107587. [Google Scholar] [CrossRef]
- Rose, G.L.; Brown, R.E. The impaired anesthesiologist: Not just about drugs and alcohol anymore. J. Clin. Anesth. 2010, 22, 379–384. [Google Scholar] [CrossRef]
- Silverstein, J.H.; Silva, D.A.; Iberti, T.J. Opioid addiction in anesthesiology. Anesthesiology 1993, 79, 354–375. [Google Scholar] [CrossRef]
- Bryson, E.O.; Silverstein, J.H. Addiction and substance abuse in anesthesiology. Anesthesiology 2008, 109, 905–917. [Google Scholar] [CrossRef] [PubMed]
- European Monitoring Centre for Drugs and Drug Addiction. Rapport Annuel 2012: État du Phénomène de la Drogue en Europe; Publications Office: Luxembourg, 2012; Available online: https://data.europa.eu/doi/10.2810/6532 (accessed on 8 February 2022).
- Kory, W.P.; Crandall, L.A. Nonmedical drug use patterns among medical students. Int. J. Addict. 1984, 19, 871–884. [Google Scholar] [CrossRef] [PubMed]
- Bouillon-Minois, J.-B.; Thivel, D.; Croizier, C.; Ajebo, É.; Cambier, S.; Boudet, G.; Adeyemi, O.J.; Ugbolue, U.C.; Bagheri, R.; Vallet, G.T.; et al. The Negative Impact of Night Shifts on Diet in Emergency Healthcare Workers. Nutrients 2022, 14, 829. [Google Scholar] [CrossRef] [PubMed]
- Besson, A.; Tarpin, A.; Flaudias, V.; Brousse, G.; Laporte, C.; Benson, A.; Navel, V.; Bouillon-Minois, J.-B.; Dutheil, F. Smoking Prevalence among Physicians: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 13328. [Google Scholar] [CrossRef] [PubMed]
- Dutheil, F.; Parreira, L.M.; Eismann, J.; Lesage, F.-X.; Balayssac, D.; Lambert, C.; Clinchamps, M.; Pezet, D.; Pereira, B.; Le Roy, B. Burnout in French General Practitioners: A Nationwide Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 12044. [Google Scholar] [CrossRef]
- Hublet, A.; Bendtsen, P.; de Looze, M.E.; Fotiou, A.; Donnelly, P.; Vilhjalmsson, R.; Baska, T.; Aasvee, K.; Franelic, I.P.; Nic Gabhainn, S.; et al. Trends in the co-occurrence of tobacco and cannabis use in 15-year-olds from 2002 to 2010 in 28 countries of Europe and North America. Eur. J. Public Health 2015, 25 (Suppl. 2), 73–75. [Google Scholar] [CrossRef] [PubMed]
- Cuttler, C.; Mischley, L.K.; Sexton, M. Sex Differences in Cannabis Use and Effects: A Cross-Sectional Survey of Cannabis Users. Cannabis Cannabinoid Res. 2016, 1, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, G.M.; Giang, H.T.N.; Ghozy, S.; Altibi, A.M.; Kandil, H.; Le, H.-H.; Eid, P.S.; Radwan, I.; Makram, O.M.; Hien, T.T.T.; et al. Protocol registration issues of systematic review and meta-analysis studies: A survey of global researchers. BMC Med. Res. Methodol. 2020, 20, 213. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Ann. Intern. Med. 2007, 147, W163–W194. [Google Scholar] [CrossRef]
- Courtin, R.; Pereira, B.; Naughton, G.; Chamoux, A.; Chiambaretta, F.; Lanhers, C.; Dutheil, F. Prevalence of dry eye disease in visual display terminal workers: A systematic review and meta-analysis. BMJ Open 2016, 6, e009675. [Google Scholar] [CrossRef]
- Dutheil, F.; Méchin, G.; Vorilhon, P.; Benson, A.C.; Bottet, A.; Clinchamps, M.; Barasinski, C.; Navel, V. Breastfeeding after Returning to Work: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8631. [Google Scholar] [CrossRef]
- Mansky, P.A. Issues in the recovery of physicians from addictive illnesses. Psychiatr. Q. 1999, 70, 107–122. [Google Scholar] [CrossRef]
- Cottler, L.B.; Ajinkya, S.; Merlo, L.J.; Nixon, S.J.; Ben Abdallah, A.; Gold, M.S. Lifetime psychiatric and substance use disorders among impaired physicians in a physicians health program: Comparison to a general treatment population: Psychopathology of impaired physicians. J. Addict. Med. 2013, 7, 108–112. [Google Scholar] [CrossRef]
- McAuliffe, W.E.; Rohman, M.; Wechsler, H. Alcohol, substance use, and other risk-factors of impairment in a sample of physicians-in-training. Adv. Alcohol Subst. Abuse 1984, 4, 67–87. [Google Scholar] [CrossRef]
- Shyangwa, P.M.; Joshi, D.; Lal, R. Alcohols and other substance use/abuse among junior doctors and medical students in a teaching institute. JNMA J. Nepal Med. Assoc. 2007, 46, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.A.; Honeycutt, G.; Ogden, B.; McMillan, D.E.; O’Sullivan, P.S.; Light, K.; Wingfield, W. Assessing substance abuse among health care students and the efficacy of educational interventions. J. Prof. Nurs. 1997, 13, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Solursh, L.P.; Weinstock, S.J.; Saunders, C.S.; Ungerleider, J.T. Attitudes of Medical Students Toward Cannabis. JAMA 1971, 217, 1371–1372. [Google Scholar] [CrossRef]
- Slaby, A.E.; Schwartz, A.H. Changing attitudes and patterns of behavior among emerging physicians. Psychiatry Med. 1971, 2, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Romero, M.I.; Santander, J.; Hitschfeld, M.J.; Labbé, M.; Zamora, V. Consumo de sustancias ilícitas y psicotrópicos entre los estudiantes de medicina de la Pontificia Universidad Católica de Chile. Rev. Méd. Chile 2009, 137, 459–465. [Google Scholar] [CrossRef]
- Laure, P.; Binsinger, C. Consumption of “performance-enhancing” products by general practitioners. Therapie 2003, 58, 445–450. [Google Scholar] [CrossRef]
- Singh, G.; Singh, R.P. Drugs on a medical campus I. Drug use among medical undergraduates. Drug Alcohol Depend. 1979, 4, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Jindal, K.C. Drugs on a medical campus. II. Drug use among faculty members. Drug Alcohol Depend. 1980, 6, 123–130. [Google Scholar] [CrossRef]
- Merlo, L.J.; Curran, J.S.; Watson, R. Gender differences in substance use and psychiatric distress among medical students: A comprehensive statewide evaluation. Subst. Abuse 2017, 38, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Saeys, F.; Cammu, H. GPs’ attitudes on a healthy lifestyle: A survey of GPs in Flanders. Br. J. Gen. Pract. 2014, 64, e664–e669. [Google Scholar] [CrossRef]
- Lipp, M.R.; Benson, S.G.; Taintor, Z. Marijuana Use by Medical Students. Am. J. Psychiatry 1971, 128, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Hughes, P.H.; Storr, C.L.; Brandenburg, N.A.; Baldwin, D.C.; Anthony, J.C.; Sheehan, D.V. Physician substance use by medical specialty. J. Addict. Dis. 1999, 18, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Beaujouan, L.; Czernichow, S.; Pourriat, J.-L.; Bonnet, F. Prevalence and risk factors for substance abuse and dependence among anaesthetists: A national survey. Ann. Fr. Anesth. Reanim. 2005, 24, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Kenna, G.A.; Wood, M.D. Prevalence of Substance Use by Pharmacists and Other Health Professionals. J. Am. Pharm. Assoc. 2004, 44, 684–693. [Google Scholar] [CrossRef]
- Ayala, E.E.; Roseman, D.; Winseman, J.S.; Mason, H.R.C. Prevalence, perceptions, and consequences of substance use in medical students. Med. Educ. Online 2017, 22, 1392824. [Google Scholar] [CrossRef]
- Bazargan, M.; Makar, M.; Bazargan-Hejazi, S.; Ani, C.; Wolf, K.E. Preventive, lifestyle, and personal health behaviors among physicians. Acad. Psychiatry 2009, 33, 289–295. [Google Scholar] [CrossRef]
- Linn, L.S.; Yager, J.; Leake, B. Professional vs. personal factors related to physicians’ attitudes toward drug testing. J. Drug Educ. 1990, 20, 95–109. [Google Scholar] [CrossRef]
- Lutsky, I.; Hopwood, M.; Abram, S.E.; Jacobson, G.R.; Haddox, J.D.; Kampine, J.P. Psychoactive substance use among American anesthesiologists: A 30-year retrospective study. Can. J. Anaesth. 1993, 40, 915–921. [Google Scholar] [CrossRef]
- Farrell, S.M.; Moir, F.; Molodynski, A.; Bhugra, D. Psychological wellbeing, burnout and substance use amongst medical students in New Zealand. Int. Rev. Psychiatry 2019, 31, 630–636. [Google Scholar] [CrossRef]
- Hughes, P.H.; Conard, S.E.; Baldwin, D.C., Jr.; Storr, C.L.; Sheehan, D.V. Resident Physician Substance Use in the United States. JAMA 1991, 265, 2069–2073. [Google Scholar] [CrossRef]
- Rodriguez, M.E.; Cami, J. Substance use among medical students in Barcelona (Spain). A comparison with previous surveys. Drug Alcohol Depend. 1986, 18, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.; Gaete, J.; Girotra, S.; Pal, H.R.; Araya, R. Substance use among medical students: Time to reignite the debate? Natl. Med. J. India 2008, 21, 75–78. [Google Scholar] [PubMed]
- Baldwin, D.C., Jr.; Hughes, P.H.; Conard, S.E.; Storr, C.L.; Sheehan, D.V. Substance Use Among Senior Medical Students: A Survey of 23 Medical Schools. JAMA 1991, 265, 2074–2078. [Google Scholar] [CrossRef]
- Lutsky, I.; Hopwood, M.; Abram, S.E.; Cerletty, J.M.; Hoffman, R.G.; Kampine, J.P. Use of psychoactive substances in three medical specialties: Anaesthesia, medicine and surgery. Can. J. Anaesth. 1994, 41, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Polakoff, P.L.; Lowinger, P. Do medical students “turn on?”. Compr. Psychiatry 1972, 13, 185–188. [Google Scholar] [CrossRef]
- Lipp, M.R.; Benson, S.G. Physician use of marijuana, alcohol, and tobacco. Am. J. Psychiatry 1972, 129, 612–616. [Google Scholar] [CrossRef]
- Hughes, P.; Brandenburg, N.; Baldwin, D.; Storr, C.; Williams, K.M.; Anthony, J.; Sheehan, D. Prevalence of substance use among US physicians. JAMA 1992, 267, 2333–2339. [Google Scholar] [CrossRef]
- Baptista, T.; Uzcàtegui, E. Substance use among resident doctors in Venezuela. Drug Alcohol Depend. 1993, 32, 127–132. [Google Scholar] [CrossRef]
- Engs, R.C. The drug-use patterns of helping-profession students in Brisbane, Australia. Drug Alcohol Depend. 1980, 6, 231–246. [Google Scholar] [CrossRef]
- Ashton, C.H.; Kamali, F. Personality, lifestyles, alcohol and drug consumption in a sample of British medical students. Med. Educ. 1995, 29, 187–192. [Google Scholar] [CrossRef]
- Boniatti, M.M.; Zubaran, C.; Panarotto, D.; Delazeri, G.J.; Tirello, J.L.; Feldens, M.D.O.; Sperotto, V.F.R. The use of psychoactive substances among medical students in southern Brazil. Drug Alcohol Rev. 2007, 26, 279–285. [Google Scholar] [CrossRef]
- Carvalho, K.A.M.; Sant’Anna, M.J.C.; Coates, V.; Omar, H.A. Medical students: Abuse of psychoactive substances and sexuality aspects. Int. J. Adolesc. Med. Health 2008, 20, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.H.; Knoepke, C.E.; Cole, M.L.; McKinnon, J.; Matlock, D.D. Colorado Medical Students’ Attitudes and Beliefs About Marijuana. J. Gen. Intern. Med. 2017, 32, 458–463. [Google Scholar] [CrossRef]
- Conard, S.; Hughes, P.; Baldwin, D.C.; Achenbach, K.E.; Sheehan, D.V. Substance use by fourth-year students at 13 U.S. medical schools. J. Med. Educ. 1988, 63, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Da Silveira, D.X.; Rosa-Oliveira, L.; Di Pietro, M.; Niel, M.; Doering-Silveira, E.; Jorge, M.R. Evolutional pattern of drug use by medical students. Addict. Behav. 2008, 33, 490–495. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, L.G.; Barroso, L.P.; Wagner, G.A.; Ponce, J.d.C.; Malbergier, A.; Stempliuk, V.d.A.; de Andrade, A.G. Drug consumption among medical students in São Paulo, Brazil: Influences of gender and academic year. Rev. Bras. Psiquiatr. 2009, 31, 227–239. [Google Scholar] [CrossRef]
- De Sousa, G.S.; Fitzsimons, M.G.; Mueller, A.; Quintão, V.C.; Simões, C.M. Drug abuse amongst anesthetists in Brazil: A national survey. Braz. J. Anesthesiol. Engl. Ed. 2021, 71, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Gignon, M.; Havet, E.; Ammirati, C.; Traullé, S.; Manaouil, C.; Balcaen, T.; Loas, G.; Dubois, G.; Ganry, O. Alcohol, cigarette, and illegal substance consumption among medical students: A cross-sectional survey. Workplace Health Saf. 2015, 63, 54–63. [Google Scholar] [CrossRef]
- Lambert Passos, S.R.; Alvarenga Americano do Brasil, P.E.; Borges dos Santos, M.A.; Costa de Aquino, M.T. Prevalence of psychoactive drug use among medical students in Rio de Janeiro. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 989–996. [Google Scholar] [CrossRef]
- Laporte, J.R.; Cami, J.; Gutiérrez, R.; Laporte, J. Caffeine, tobacco, alcohol and drug consumption among medical students in Barcelona. Eur. J. Clin. Pharmacol. 1977, 11, 449–453. [Google Scholar] [CrossRef]
- McKay, A.J.; Hawthorne, V.M.; McCartney, H.N. Drug taking among medical students at Glasgow university. Br. Med. J. 1973, 1, 540–543. [Google Scholar] [CrossRef] [PubMed]
- Petroianu, A.; dos Reis, D.C.F.; Cunha, B.D.S.; de Souza, D.M. Prevalence of alcohol, tobacco and psychotropic drug use among medical students at the Universidade Federal de Minas Gerais. Rev. Assoc. Medica Bras. 2010, 56, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Pickard, M.; Bates, L.; Dorian, M.; Greig, H.; Saint, D. Alcohol and drug use in second-year medical students at the University of Leeds. Med. Educ. 2000, 34, 148–150. [Google Scholar] [CrossRef]
- Rochford, J.; Grant, I.; LaVigne, G. Medical students and drugs: Further neuropsychological and use pattern considerations. Int. J. Addict. 1977, 12, 1057–1065. [Google Scholar] [CrossRef]
- Schwartz, R.H.; Lewis, D.C.; Hoffmann, N.G.; Kyriazi, N. Cocaine and Marijuana Use by Medical Students Before and During Medical School. Arch. Intern. Med. 1990, 150, 883–886. [Google Scholar] [CrossRef]
- Vujcic, I.; Pavlovic, A.; Dubljanin, E.; Maksimovic, J.; Nikolic, A.; Sipetic-Grujicic, S. Attitudes Toward Medical Cannabis Legalization Among Serbian Medical Students. Subst. Use Misuse 2017, 52, 1225–1231. [Google Scholar] [CrossRef]
- Webb, E.; Ashton, C.H.; Kelly, P.; Kamah, F. An update on British medical students’ lifestyles. Med. Educ. 1998, 32, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Van Devanter, N.; Fenstermaker, M.; Cawkwell, P.; Sherman, S.; Weitzman, M. A Study of the Use, Knowledge, and Beliefs About Cigarettes and Alternative Tobacco Products Among Students at One U.S. Medical School. Acad. Med. J. Assoc. Am. Med. Coll. 2015, 90, 1713–1719. [Google Scholar] [CrossRef] [PubMed]
- Newbury-Birch, D.; Walshaw, D.; Kamali, F. Drink and drugs: From medical students to doctors. Drug Alcohol Depend. 2001, 64, 265–270. [Google Scholar] [CrossRef]
- Croen, L.G.; Woesner, M.; Herman, M.; Reichgott, M. A longitudinal study of substance use and abuse in a single class of medical students. Acad. Med. J. Assoc. Am. Med. Coll. 1997, 72, 376–381. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, T.M. Update on marijuana. J. Psychosoc. Nurs. Ment. Health Serv. 2009, 47, 19–22. [Google Scholar] [CrossRef]
- Volkow, N.D.; Baler, R.D.; Compton, W.M.; Weiss, S.R.B. Adverse health effects of marijuana use. N. Engl. J. Med. 2014, 370, 2219–2227. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.; Degenhardt, L. The adverse health effects of chronic cannabis use. Drug Test. Anal. 2014, 6, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Curtis, L.; Rey-Bellet, P.; Merlo, M.C.G. Cannabis and psychosis. Rev. Med. Suisse 2006, 2, 2099–2100, 2102–2103. [Google Scholar]
- Matsuo, T.; Takahashi, O.; Kitaoka, K.; Arioka, H.; Kobayashi, D. Resident Burnout and Work Environment. Intern. Med. 2021, 60, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Dutheil, F.; Aubert, C.; Pereira, B.; Dambrun, M.; Moustafa, F.; Mermillod, M.; Baker, J.S.; Trousselard, M.; Lesage, F.-X.; Navel, V. Suicide among physicians and health-care workers: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0226361. [Google Scholar] [CrossRef]
- Schifferdecker, M.; Schmidt, R.; Loevenich, A.; Krahl, A. Drug dependence among physicians. Z. Arztl. Fortbild. 1996, 90, 295–300. [Google Scholar]
- Clough, B.A.; March, S.; Chan, R.J.; Casey, L.M.; Phillips, R.; Ireland, M.J. Psychosocial interventions for managing occupational stress and burnout among medical doctors: A systematic review. Syst. Rev. 2017, 6, 144. [Google Scholar] [CrossRef]
- Shortt, S.E. Psychiatric illness in physicians. Can. Med. Assoc. J. 1979, 121, 283–288. [Google Scholar]
- Kondev, V.; Winters, N.; Patel, S. Cannabis use and posttraumatic stress disorder comorbidity: Epidemiology, biology and the potential for novel treatment approaches. Int. Rev. Neurobiol. 2021, 157, 143–193. [Google Scholar] [CrossRef]
- Hyman, S.M.; Sinha, R. Stress-related factors in cannabis use and misuse: Implications for prevention and treatment. J. Subst. Abuse Treat. 2009, 36, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Cougle, J.R.; Bonn-Miller, M.O.; Vujanovic, A.A.; Zvolensky, M.J.; Hawkins, K.A. Posttraumatic stress disorder and cannabis use in a nationally representative sample. Psychol. Addict. Behav. 2011, 25, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Barengo, N.C.; Sandström, H.P.; Jormanainen, V.J.; Myllykangas, M.T. Attitudes and behaviours in smoking cessation among general practitioners in Finland 2001. Soz. Praventivmed. 2005, 50, 355–360. [Google Scholar] [CrossRef]
- Mughal, F.; Rashid, A.; Jawad, M. Tobacco and electronic cigarette products: Awareness, cessation attitudes, and behaviours among general practitioners. Prim. Health Care Res. Dev. 2018, 19, 605–609. [Google Scholar] [CrossRef]
- Pretti, G.; Roncarolo, F.; Bonfanti, M.; Bettinelli, E.; Invernizzi, G.; Ceccarelli, M.; Carreri, V.; Tenconi, M.T. Survey among GP’s about their smoking habits, opinions and behaviours in smoking prevention in Lombardy (Northern Italy). Epidemiol. Prev. 2006, 30, 343–347. [Google Scholar] [PubMed]
- Hughes, J.R.; Naud, S.; Budney, A.J.; Fingar, J.R.; Callas, P.W. Attempts to Stop or Reduce Daily Cannabis Use: An Intensive Natural History Study. Psychol. Addict. Behav. 2016, 30, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.R.; Ali, D.W. Pharmacology of Medical Cannabis. Adv. Exp. Med. Biol. 2019, 1162, 151–165. [Google Scholar] [CrossRef]
- Budney, A.J.; Vandrey, R.G.; Stanger, C. Pharmacological and psychosocial interventions for cannabis use disorders. Rev. Bras. Psiquiatr. 2010, 32 (Suppl. 1), S46–S55. [Google Scholar]
- Lee, D.C.; Budney, A.J.; Brunette, M.F.; Hughes, J.R.; Etter, J.-F.; Stanger, C. Treatment models for targeting tobacco use during treatment for cannabis use disorder: Case series. Addict. Behav. 2014, 39, 1224–1230. [Google Scholar] [CrossRef]
- Simpson, S.; Mclellan, R.; Wellmeyer, E.; Matalon, F.; George, O. Drugs and Bugs: The Gut-Brain Axis and Substance Use Disorders. J. Neuroimmune Pharmacol. 2022, 17, 33–61. [Google Scholar] [CrossRef]
- Hill, M.L.; Loflin, M.; Nichter, B.; Norman, S.B.; Pietrzak, R.H. Prevalence of cannabis use, disorder, and medical card possession in U.S. military veterans: Results from the 2019-2020 National Health and Resilience in Veterans Study. Addict. Behav. 2021, 120, 106963. [Google Scholar] [CrossRef] [PubMed]
- Adverse effects of cannabis. Prescrire Int. 2011, 20, 18–23.
- Bhojani, F.A.; Castillejo-Picco, L.A.; Cathcart, D.; Emmett, E.A.; Frangos, S.; Glencross, P.M.; Herman, C.J.; O’Shea, K.; Rountree, P.; Turner, D.E.; et al. Fitness-for-Duty Assessments of Industrial Firefighters: Guidance for Occupational Medicine Physicians. J. Occup. Environ. Med. 2018, 60, e82–e89. [Google Scholar] [CrossRef] [PubMed]
- Loukzadeh, Z.; Zare, Z.; Mehrparvar, A.H.; Mirmohammadi, S.J.; Mostaghaci, M. Fitness-for-work assessment of train drivers of Yazd railway, central Iran. Int. J. Occup. Environ. Med. 2013, 4, 157–163. Available online: https://pubmed.ncbi.nlm.nih.gov/23860546/ (accessed on 14 April 2023). [PubMed]
- Conway, H.; Simmons, J.; Talbert, T. The purposes of occupational medical surveillance in US industry and related health findings. J. Occup. Med. 1993, 35, 670–686. [Google Scholar] [CrossRef]
- Looby, A.; Earleywine, M. Negative consequences associated with dependence in daily cannabis users. Subst. Abuse Treat. Prev. Policy 2007, 2, 3. [Google Scholar] [CrossRef]
- Fishburne, P.M.; Abelson, H.I.; Cisin, I. National Survey on Drug Abuse: Main Findings; National Institute on Drug Abuse, Division of Research, US Dept of Health: Rockville, MD, USA, 1979.
- Lotrean, L.M.; Santillan, E.A.; Thrasher, J.; Laza, V. An Increasing Trend of Illicit Drug use among Romanian University Students from 1999 to 2011. Zdr. Varst. 2016, 55, 53–58. [Google Scholar] [CrossRef]
- Blum, K.; Khalsa, J.; Cadet, J.L.; Baron, D.; Bowirrat, A.; Boyett, B.; Lott, L.; Brewer, R.; Gondré-Lewis, M.; Bunt, G.; et al. Cannabis-Induced Hypodopaminergic Anhedonia and Cognitive Decline in Humans: Embracing Putative Induction of Dopamine Homeostasis. Front. Psychiatry 2021, 12, 623403. [Google Scholar] [CrossRef]
- Veen, N.D.; Selten, J.-P.; van der Tweel, I.; Feller, W.G.; Hoek, H.W.; Kahn, R.S. Cannabis Use and Age at Onset of Schizophrenia. Am. J. Psychiatry 2004, 161, 501–506. Available online: https://ajp.psychiatryonline.org/doi/full/10.1176/appi.ajp.161.3.501 (accessed on 23 February 2022). [CrossRef]
- Lagerberg, T.V.; Sundet, K.; Aminoff, S.R.; Berg, A.O.; Ringen, P.A.; Andreassen, O.A.; Melle, I. Excessive cannabis use is associated with earlier age at onset in bipolar disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2011, 261, 397–405. [Google Scholar] [CrossRef]
- DeJong, W.; Langford, L.M. A typology for campus-based alcohol prevention: Moving toward environmental management strategies. J. Stud. Alcohol. Suppl. 2002, 140–147. [Google Scholar] [CrossRef]
- Holder, H.D. Community prevention of alcohol problems. Addict. Behav. 2000, 25, 843–859. [Google Scholar] [CrossRef]
- Jungerman, F.S.; Alves, H.N.P.; Carmona, M.J.C.; Conti, N.B.; Malbergier, A. Anesthetic drug abuse by anesthesiologists. Rev. Bras. Anestesiol. 2012, 62, 380–386. [Google Scholar] [CrossRef]
- Linakis, J.G.; Thomas, S.A.; Bromberg, J.R.; Casper, T.C.; Chun, T.H.; Mello, M.J.; Richards, R.; Ahmad, F.; Bajaj, L.; Brown, K.M.; et al. Adolescent alcohol use predicts cannabis use over a three year follow-up period. Subst. Abuse 2022, 43, 514–519. [Google Scholar] [CrossRef]
- Drug Statistics and Trends. Available online: https://www.unodc.org/documents/wdr/WDR_2010/2.0_Drug_statistics_and_Trends.pdf (accessed on 23 February 2022).
- Cannabis Users Worldwide Number by Region 2011–2019 [Internet]. Statista. Available online: https://www.statista.com/statistics/264734/number-of-cannabis-users-worldwide-by-region/ (accessed on 21 March 2022).
- Goodwin, R.D.; Kim, J.H.; Cheslack-Postava, K.; Weinberger, A.H.; Wu, M.; Wyka, K.; Kattan, M. Trends in cannabis use among adults with children in the home in the United States, 2004-2017: Impact of state-level legalization for recreational and medical use. Addiction 2021, 116, 2770–2778. [Google Scholar] [CrossRef] [PubMed]
- Abuhasira, R.; Shbiro, L.; Landschaft, Y. Medical use of cannabis and cannabinoids containing products—Regulations in Europe and North America. Eur. J. Intern. Med. 2018, 49, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Areesantichai, C.; Perngparn, U.; Pilley, C. Current cannabis-related situation in the Asia-Pacific region. Curr. Opin. Psychiatry 2020, 33, 352–359. [Google Scholar] [CrossRef]
- Mendiburo-Seguel, A.; Vargas, S.; Oyanedel, J.C.; Torres, F.; Vergara, E.; Hough, M. Attitudes towards drug policies in Latin America: Results from a Latin-American Survey. Int. J. Drug Policy 2017, 41, 8–13. [Google Scholar] [CrossRef]
- Pisanti, S.; Bifulco, M. Medical Cannabis: A plurimillennial history of an evergreen. J. Cell. Physiol. 2019, 234, 8342–8351. [Google Scholar] [CrossRef]
- Boden, J.M.; Cleland, L.; Dhakal, B.; Horwood, L.J. Attitudes towards cannabis and cannabis law change in a New Zealand birth cohort. N. Z. Med. J. 2020, 133, 79–88. [Google Scholar]
- Khalili, M.; Rahimi-Movaghar, A.; Shadloo, B.; Mojtabai, R.; Mann, K.; Amin-Esmaeili, M. Global Scientific Production on Illicit Drug Addiction: A Two-Decade Analysis. Eur. Addict. Res. 2018, 24, 60–70. [Google Scholar] [CrossRef]
- Yu, B.; Chen, X.; Chen, X.; Yan, H. Marijuana legalization and historical trends in marijuana use among US residents aged 12–25: Results from the 1979–2016 National Survey on drug use and health. BMC Public Health 2020, 20, 156. [Google Scholar] [CrossRef] [PubMed]
- Carliner, H.; Brown, Q.L.; Sarvet, A.L.; Hasin, D.S. Cannabis use, attitudes, and legal status in the U.S.: A review. Prev. Med. 2017, 104, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Hasin, D.S.; Sarvet, A.L.; Cerdá, M.; Keyes, K.M.; Stohl, M.; Galea, S.; Wall, M.M. US Adult Illicit Cannabis Use, Cannabis Use Disorder, and Medical Marijuana Laws: 1991–1992 to 2012–2013. JAMA Psychiatry 2017, 74, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.P.; Gold, M.S.; Nemeroff, C.B.; McDonald, W.; Grzenda, A.; Widge, A.S.; Rodriguez, C.; Kraguljac, N.V.; Krystal, J.H.; Carpenter, L.L. Risks and Benefits of Cannabis and Cannabinoids in Psychiatry. Am. J. Psychiatry 2022, 179, 98–109. Available online: https://pubmed.ncbi.nlm.nih.gov/34875873/ (accessed on 14 April 2023). [CrossRef]
- Hayatbakhsh, M.R.; O’Callaghan, M.J.; Mamun, A.A.; Williams, G.M.; Clavarino, A.; Najman, J.M. Cannabis use and obesity and young adults. Am. J. Drug Alcohol Abuse 2010, 36, 350–356. [Google Scholar] [CrossRef]
- Ong, L.Q.; Bellettiere, J.; Alvarado, C.; Chavez, P.; Berardi, V. Cannabis use, sedentary behavior, and physical activity in a nationally representative sample of US adults. Harm. Reduct. J. 2021, 18, 48. [Google Scholar] [CrossRef]
- Smith, L.; Sherratt, F.; Barnett, Y.; Cao, C.; Tully, M.A.; Koyanagi, A.; Jacob, L.; Soysal, P.; López Sánchez, G.F.; Shin, J.I.; et al. Physical activity, sedentary behaviour and cannabis use in 15,822 US adults: Cross-sectional analyses from NHANES. Public Health 2021, 193, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, J.E.; Gardner, C.O.; Kendler, K.S. Marriage and reductions in men’s alcohol, tobacco, and cannabis use. Psychol. Med. 2020, 50, 2634–2640. [Google Scholar] [CrossRef]
- Huizink, A.C.; Levälahti, E.; Korhonen, T.; Dick, D.M.; Pulkkinen, L.; Rose, R.J.; Kaprio, J. Tobacco, cannabis, and other illicit drug use among Finnish adolescent twins: Causal relationship or correlated liabilities? J. Stud. Alcohol Drugs 2010, 71, 5–14. [Google Scholar] [CrossRef]
- Agrawal, A.; Neale, M.C.; Prescott, C.A.; Kendler, K.S. A twin study of early cannabis use and subsequent use and abuse/dependence of other illicit drugs. Psychol. Med. 2004, 34, 1227–1237. [Google Scholar] [CrossRef]
- LeLorier, J.; Grégoire, G.; Benhaddad, A.; Lapierre, J.; Derderian, F. Discrepancies between meta-analyses and subsequent large randomized, controlled trials. N. Engl. J. Med. 1997, 337, 536–542. [Google Scholar] [CrossRef]
- Hopwood, C.J.; Morey, L.C.; Edelen, M.O.; Shea, M.T.; Grilo, C.M.; Sanislow, C.A.; McGlashan, T.H.; Daversa, M.T.; Gunderson, J.G.; Zanarini, M.C.; et al. A comparison of interview and self-report methods for the assessment of borderline personality disorder criteria. Psychol. Assess. 2008, 20, 81–85. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Data Collection | Physicians | Specialty | Prevalence | (%) of | Cannabis | Users | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % Men | Age | Overall | By Specialty | Residents | Students | Lifetime | Past Year | Past 6 Months | Last Month | Last Week | Daily Use | |||
| Ashton 1995 [51] | England | 1994 | 185 | 41.3 | 20.4 | X | 49.2 | ||||||||
| Ayala 2017 [36] | USA | 2015–2016 | 855 | 35.5 | 25.6 | X | 26.2 | 11.7 | |||||||
| Baldwin 1991 [44] | USA | 1987 | 2046 | 62.7 | 27.7 | X | 66.4 | 22.5 | 10 | ||||||
| Baptista 1993 [49] | Venezuela | 1990 | 191 | 49.7 | 31 | X | 7.3 | ||||||||
| Bazargan 2009 [37] | USA | 763 | 75.1 | 53 | X | 4 | |||||||||
| Beaujouan 2005 [34] | France | 2001 | 3453 | 63.3 | Anesthesiologists | 2.6 | |||||||||
| Boniatti 2007 [52] | Brasil | 2006 | 183 | 45.9 | 22.5 | X | 31.1 | 13.7 | 7.7 | ||||||
| Carvalho 2008 [53] | Brasil | 2005 | 465 | 57 | 21.5 | X | 14.4 | ||||||||
| Chan 2017 [54] | USA | 2014 | 236 | 52 | 30 | X | 53.8 | ||||||||
| Coleman 1997 [23] | USA | 1989–1991 | 152 | X | 32 | 3 | |||||||||
| Conard 1988 [55] | USA | 1975–1985 | 589 | 65 | 27.6 | X | 73.7 | 31.6 | 17.3 | 1.2 | |||||
| Cottler 2013 * [20] | USA | 2008–2009 | 99 | 76.7 | 45.6 | Addicted | X | 29.2 | |||||||
| Croen 1997 [71] | USA | 1991–1993 | 170 | 54.1 | X | 29.4 | |||||||||
| Da Silveira 2008 [56] | Brasil | 2007 | 456 | 54.2 | 21 | X | 16.4 | ||||||||
| De Oliveira 2009 [57] | Brasil | 1996–2001 | 248 | 52 | X | 27.3 | 20.2 | 13.8 | |||||||
| De Sousa2021 [58] | Brasil | 2020 | 978 | 65.6 | Anesthesiologists | 43.2 | |||||||||
| Engs 1980 [50] | Australia | 1980 | 431 | X | 18.3 | 7.5 | |||||||||
| Farrell 2019 [40] | New Zealand | 2019 | 220 | 29.5 | X | 35 | |||||||||
| Gignon 2015 [59] | France | 2011 | 171 | 43.8 | 22.1 | X | 77 | 14 | 7 | ||||||
| Hughes 1991 [41] | USA | 1987 | 1785 | 70 | 30 | X | 65.1 | 17 | 7 | 0.3 | |||||
| Hughes 1992 [48] | USA | 1990 | 5426 | 82.2 | X | X | 35.6 | 4.6 to 10.5 | 2.1 to 7 | 0.1 to 0.3 | |||||
| Kenna 2004 [35] | USA | 2002 | 104 | 74 | 49 | X | 51.9 | 3.8 | 1.9 | 0 | |||||
| Kory 1984 [8] | USA | 1980 | 165 | 71.5 | X | 75.8 | 43.6 | 21.8 | 13.4 | 8.5 | |||||
| Lambert Passos 2006 [60] | Brasil | 1998 | 1054 | 47.4 | 21.1 | X | 20.9 | 5.6 | |||||||
| Laporte 1977 [61] | Spain | 1974 | 808 | 63.7 | X | 9.6 | |||||||||
| Laure 2003 [27] | France | 202 | 75.7 | 45.6 | General practioner | 20 | 2 | ||||||||
| Linn 1990 [38] | USA | 1987 | 303 | 87.1 | 47.6 | X | 55 | 9 | |||||||
| Lipp 1971 [32] | USA | 1970 | 1063 | X | 49.8 | 29.9 | |||||||||
| Lipp 1972 [47] | USA | 1971 | 1314 | X | 25 | ||||||||||
| Lutsky 1993 [39] | Canada | 183 | 84.5 | X | Anesthesiologists | 30 | |||||||||
| Lutsky 1994 [45] | Canada | 824 | 91.9 | X | 16.2 | ||||||||||
| Mansky 1999 * [19] | USA | 576 | Addicted | 1.6 | |||||||||||
| McAuliffe 1984 [21] | USA | 1981–1982 | 134 | 76.1 | X | 61 | 28 | ||||||||
| McKay 1973 [62] | Scotland | 1971 | 749 | 68.7 | X | 13.3 | |||||||||
| Merlo 2017 [30] | USA | 2014 | 862 | 42.8 | X | 46.8 | 4.1 | 1.5 | |||||||
| Newburry-Birch 2001 [70] | UK | 1995–1999 | 122 | 34.4 | 58.3 | X | X | 46.8–65.5 | 21.9–23.6 | 11.4–11.8 | 2.7–7 | ||||
| Petroianu 2010 [63] | Brasil | 332 | 48.2 | X | 15.6 | 0.6 | 0.3 | ||||||||
| Pickard 2000 [64] | UK | 46 | 33.8 | X | 33.5 | ||||||||||
| Polakoff 1972 [46] | USA | 1969 | 395 | X | X | 13 to 42 | |||||||||
| Rai 2008 [43] | India | 2003 | 2135 | 70.8 | 20.5 | X | 6.6 | 1.5 | |||||||
| Rochford 1977 [65] | USA | 134 | X | 68.7 | |||||||||||
| Rodriguez 1986 [42] | Spain | 1984 | 2308 | 48.1 | X | 20.7 | 0.9 | ||||||||
| Romero 2009 [26] | Chile | 2005 | 569 | 55 | 21.5 | X | 33 | 19.7 | 5.1 | 0.17 | |||||
| Saeys 2014 [31] | Belgium | 2011 | 626 | 57.3 | 45 | General practioner | 4 | ||||||||
| Schwartz 1990 [66] | USA | 1987 | 263 | 64.6 | X | 43 | 5 | 3.5 | 1.5 | ||||||
| Shyangwa 2007 [22] | Nepal | 193 | 67.3 | 22.8 | X | 15 | |||||||||
| Singh 1979 [28] | India | 1976–1977 | 672 | 79.9 | X | 23.2 | 11 | 1.3 | 0 | ||||||
| Singh 1980 [29] | India | 1977–1978 | 95 | 75.7 | X | 20 | 3.2 | 0 | |||||||
| Slaby 1971 [25] | USA | 1970 | 46 | 89.1 | 25.7 | X | 52 | ||||||||
| Solursh 1971 [24] | Canada and USA | 234 | X | 54.3 | 32.1 | 22.7 | 8.5 | 1.3 | |||||||
| Vujcic 2017 [67] | Serbia | 2015 | 418 | 37.3 | 22.5 | X | 34.9 | ||||||||
| Webb 1998 [68] | UK | 1996 | 785 | 44 | 20 | X | 43.9 | 9.6 | |||||||
| Zhou 2015 [69] | USA | 2014 | 431 | 50.3 | 25 | X | 31.1 | 12.1 | 8.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naillon, P.-L.; Flaudias, V.; Brousse, G.; Laporte, C.; Baker, J.S.; Brusseau, V.; Comptour, A.; Zak, M.; Bouillon-Minois, J.-B.; Dutheil, F. Cannabis Use in Physicians: A Systematic Review and Meta-Analysis. Medicines 2023, 10, 29. https://doi.org/10.3390/medicines10050029
Naillon P-L, Flaudias V, Brousse G, Laporte C, Baker JS, Brusseau V, Comptour A, Zak M, Bouillon-Minois J-B, Dutheil F. Cannabis Use in Physicians: A Systematic Review and Meta-Analysis. Medicines. 2023; 10(5):29. https://doi.org/10.3390/medicines10050029
Chicago/Turabian StyleNaillon, Pierre-Louis, Valentin Flaudias, Georges Brousse, Catherine Laporte, Julien S. Baker, Valentin Brusseau, Aurélie Comptour, Marek Zak, Jean-Baptiste Bouillon-Minois, and Frédéric Dutheil. 2023. "Cannabis Use in Physicians: A Systematic Review and Meta-Analysis" Medicines 10, no. 5: 29. https://doi.org/10.3390/medicines10050029
APA StyleNaillon, P.-L., Flaudias, V., Brousse, G., Laporte, C., Baker, J. S., Brusseau, V., Comptour, A., Zak, M., Bouillon-Minois, J.-B., & Dutheil, F. (2023). Cannabis Use in Physicians: A Systematic Review and Meta-Analysis. Medicines, 10(5), 29. https://doi.org/10.3390/medicines10050029