
Making Visible the Invisible: Automatically Measured Global and Regional Brain Volume Is Associated with Cognitive Impairment and Fatigue in Multiple Sclerosis

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. MRI Acquisition and Analysis
- -
- 3D T1-weighted turbo field echo, repetition time (TR) = 8.1 ms, echo time (TE) = 3.7 ms, 180 slices, voxel size = 1 × 1 × 1 mm3;
- -
- 3D fluid-attenuated inversion recovery (FLAIR), TR = 8000 ms, TE = 290 ms, inversion time (TI) = 2360 ms, 180 slices, FOV = 1 × 1 × 1 mm3.
2.2. Neuropsychological Assessment
2.3. Fatigue
2.4. Statistical Analysis
3. Results
3.1. Physical Disability
3.2. Fatigue
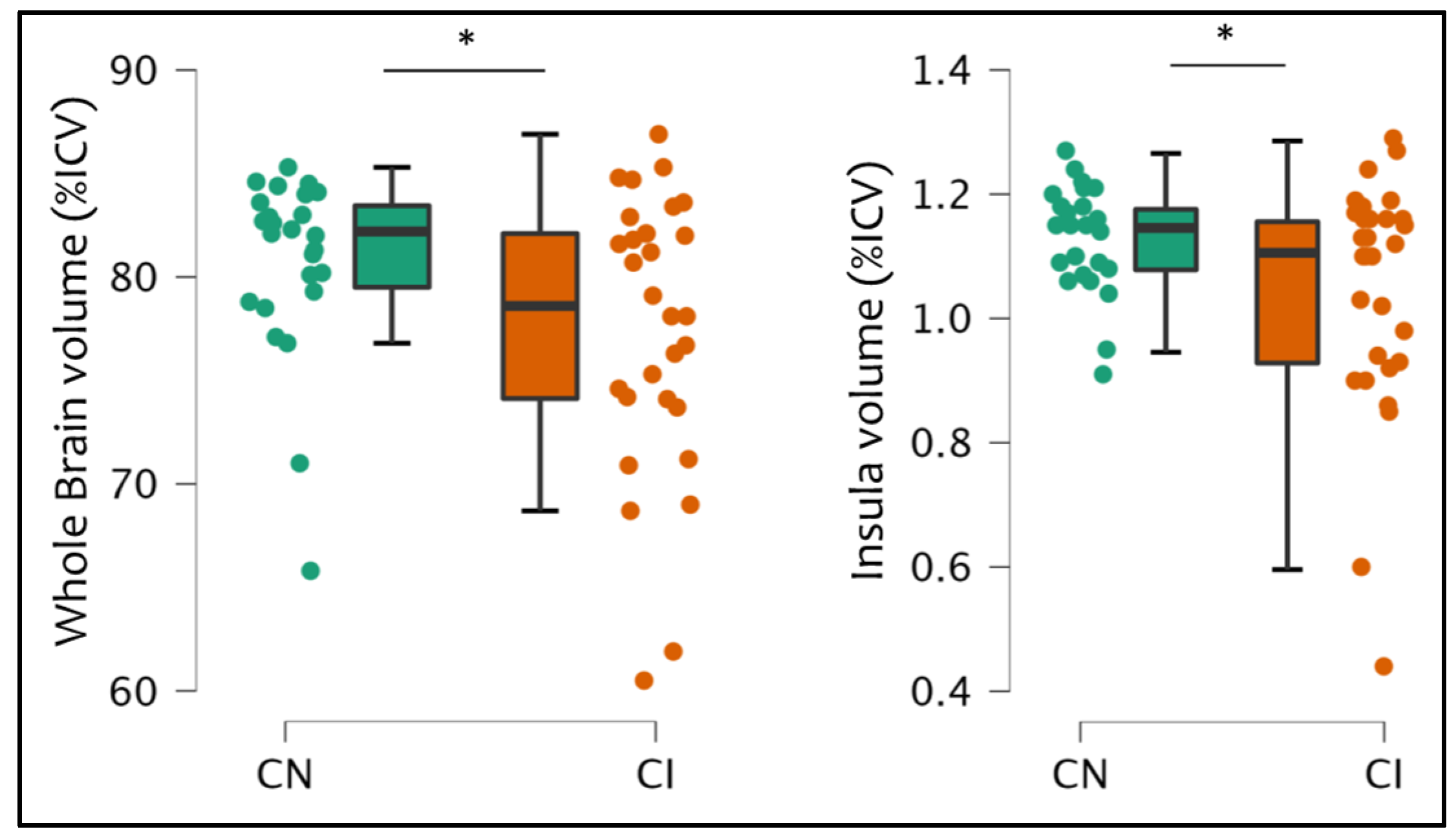
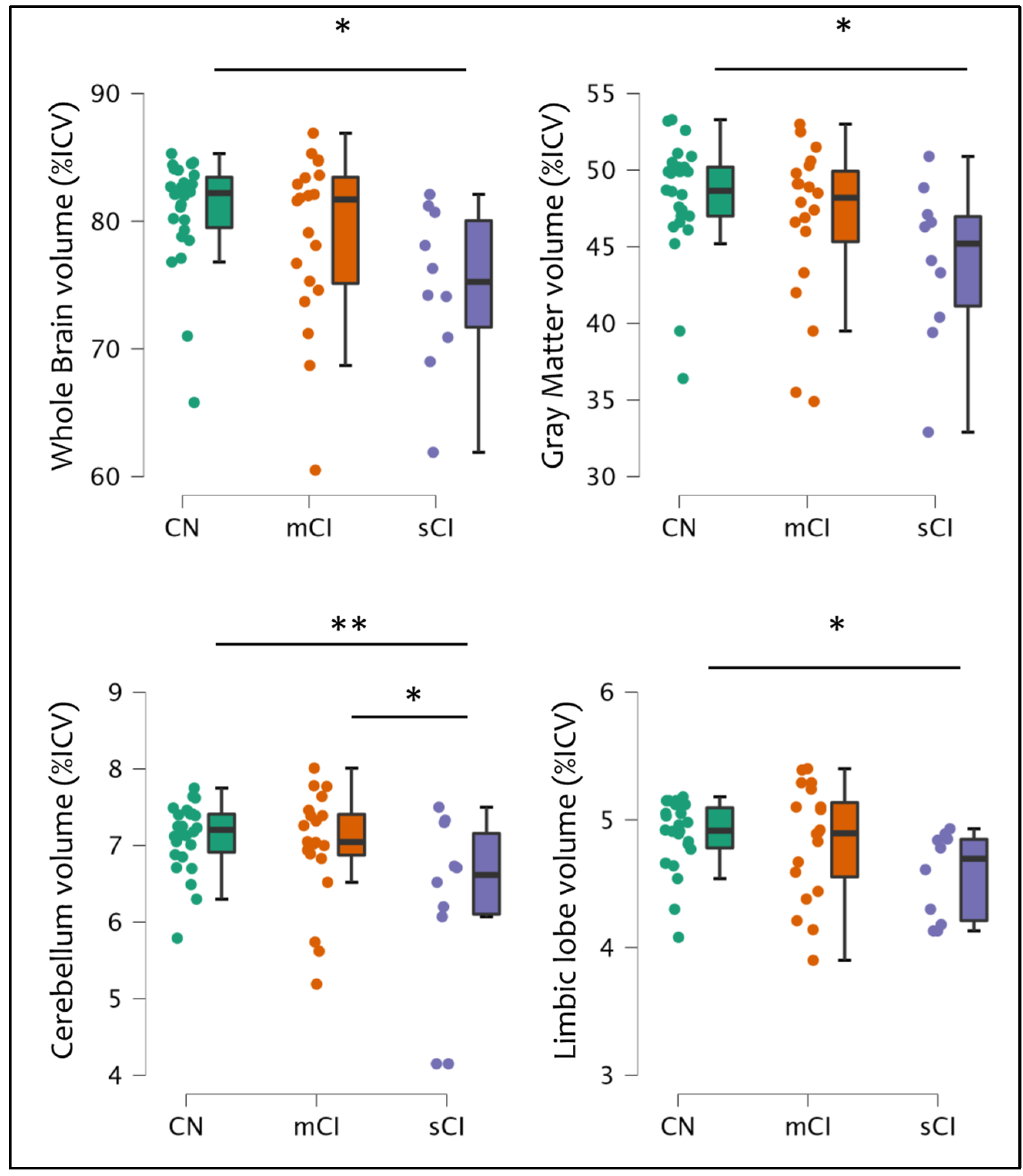
3.3. Cognitive Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Browne, P.; Chandraratna, D.; Angood, C.; Tremlett, H.; Baker, C.; Taylor, B.V.; Thompson, A.J. Atlas of Multiple Sclerosis 2013: A growing global problem with widespread inequity. Neurology 2014, 83, 1022–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinman, L. Multiple sclerosis: A two-stage disease. Nat. Immunol. 2001, 2, 762–764. [Google Scholar] [CrossRef] [PubMed]
- Confavreux, C.; Vukusic, S.; Moreau, T.; Adeleine, P. Relapses and progression of disability in multiple sclerosis. N. Engl. J. Med. 2000, 343, 1430–1438. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, H. Pathogenic Mechanisms Associated With Different Clinical Courses of Multiple Sclerosis. Front. Immunol. 2019, 9, 3116. [Google Scholar] [CrossRef] [Green Version]
- Leray, E.; Yaouanq, J.; Le Page, E.; Coustans, M.; Laplaud, D.; Oger, J.; Edan, G. Evidence for a two-stage disability progression in multiple sclerosis. Brain 2010, 133, 1900–1913. [Google Scholar] [CrossRef] [Green Version]
- Kleiter, I.; Ayzenberg, I.; Havla, J.; Lukas, C.; Penner, I.K.; Stadelmann, C.; Linker, R.A. The transitional phase of multiple sclerosis: Characterization and conceptual framework. Mult. Scler. Relat. Disord. 2020, 44, 102242. [Google Scholar] [CrossRef]
- Cree, B.A.C.; Hollenbach, J.A.; Bove, R.; Kirkish, G.; Sacco, S.; Caverzasi, E.; Bischof, A.; Gundel, T.; Zhu, A.H.; Papinutto, N.; et al. Silent progression in disease activity-free relapsing multiple sclerosis. Ann. Neurol. 2019, 85, 653–666. [Google Scholar] [CrossRef]
- Kappos, L.; Wolinsky, J.S.; Giovannoni, G.; Arnold, D.L.; Wang, Q.; Bernasconi, C.; Model, F.; Koendgen, H.; Manfrini, M.; Belachew, S.; et al. Contribution of Relapse-Independent Progression vs Relapse-Associated Worsening to Overall Confirmed Disability Accumulation in Typical Relapsing Multiple Sclerosis in a Pooled Analysis of 2 Randomized Clinical Trials. JAMA Neurol. 2020, 77, 1132–1140. [Google Scholar] [CrossRef]
- Amato, M.P.; Prestipino, E.; Bellinvia, A.; Niccolai, C.; Razzolini, L.; Pastò, L.; Fratangelo, R.; Tudisco, L.; Fonderico, M.; Mattiolo, P.L.; et al. Cognitive impairment in multiple sclerosis: An exploratory analysis of environmental and lifestyle risk factors. PLoS ONE 2019, 14, e0222929. [Google Scholar] [CrossRef] [Green Version]
- Sumowski, J.F.; Benedict, R.; Enzinger, C.; Filippi, M.; Geurts, J.J.; Hamalainen, P.; Hulst, H.; Inglese, M.; Leavitt, V.M.; Rocca, M.A.; et al. Cognition in multiple sclerosis: State of the field and priorities for the future. Neurology 2018, 90, 278–288. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Amato, M.P.; DeLuca, J.; Geurts, J.J.G. Cognitive impairment in multiple sclerosis: Clinical management, MRI, and therapeutic avenues. Lancet Neurol. 2020, 19, 860–871. [Google Scholar] [CrossRef] [PubMed]
- DeLuca, J.; Chiaravalloti, N.D.; Sandroff, B.M. Treatment and management of cognitive dysfunction in patients with multiple sclerosis. Nat. Rev. Neurol. 2020, 16, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Fisk, J.D.; Pontefract, A.; Ritvo, P.G.; Archibald, C.; Murray, T.J. The impact of fatigue on patients with multiple sclerosis. Can. J. Neurol. Sci. 1994, 21, 9–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobelt, G.; Thompson, A.; Berg, J.; Gannedahl, M.; Eriksson, J.; MSCOI Study Group; European Multiple Sclerosis Platform. New insights into the burden and costs of multiple sclerosis in Europe. Mult. Scler. 2017, 23, 1123–1136. [Google Scholar] [CrossRef] [Green Version]
- Penner, I.K. Evaluation of cognition and fatigue in multiple sclerosis: Daily practice and future directions. Acta Neurol. Scand. 2016, 134, 19–23. [Google Scholar] [CrossRef]
- Khan, F.; Amatya, B.; Galea, M. Management of fatigue in persons with multiple sclerosis. Front. Neurol. 2014, 5, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Green, R.; Cutter, G.; Friendly, M.; Kister, I. Which symptoms contribute the most to patients’ perception of health in multiple sclerosis? Mult. Scler. J. Exp. Transl. Clin. 2017, 3, 2055217317728301. [Google Scholar] [CrossRef] [Green Version]
- Lakin, L.; Davis, B.E.; Binns, C.C.; Currie, K.M.; Rensel, M.R. Comprehensive Approach to Management of Multiple Sclerosis: Addressing Invisible Symptoms-A Narrative Review. Neurol. Ther. 2021, 10, 75–98. [Google Scholar] [CrossRef]
- Calabrese, M.; Rinaldi, F.; Mattisi, I.; Grossi, P.; Favaretto, A.; Atzori, M.; Bernardi, V.; Barachino, L.; Romualdi, C.; Rinaldi, L.; et al. Widespread cortical thinning characterizes patients with MS with mild cognitive impairment. Neurology 2010, 74, 321–328. [Google Scholar] [CrossRef]
- Eijlers, A.J.C.; van Geest, Q.; Dekker, I.; Steenwijk, M.D.; Meijer, K.A.; Hulst, H.E.; Barkhof, F.; Uitdehaag, B.M.J.; Schoonheim, M.M.; Geurts, J.J.G. Predicting cognitive decline in multiple sclerosis: A 5-year follow-up study. Brain 2018, 141, 2605–2618. [Google Scholar] [CrossRef]
- Pitteri, M.; Romualdi, C.; Magliozzi, R.; Monaco, S.; Calabrese, M. Cognitive impairment predicts disability progression and cortical thinning in MS: An 8-year study. Mult. Scler. 2017, 23, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Tillema, J.M.; Hulst, H.E.; Rocca, M.A.; Vrenken, H.; Steenwijk, M.D.; Damjanovic, D.; Enzinger, C.; Ropele, S.; Tedeschi, G.; Gallo, A.; et al. Regional cortical thinning in multiple sclerosis and its relation with cognitive impairment: A multicenter study. Mult. Scler. 2016, 22, 901–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabrese, M.; Rinaldi, F.; Grossi, P.; Mattisi, I.; Bernardi, V.; Favaretto, A.; Perini, P.; Gallo, P. Basal ganglia and frontal/parietal cortical atrophy is associated with fatigue in relapsing-remitting multiple sclerosis. Mult. Scler. 2010, 16, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, V.; Ciolac, D.; Gonzalez-Escamilla, G.; Grothe, M.; Strauss, S.; Molina Galindo, L.S.; Radetz, A.; Salmen, A.; Lukas, C.; Klotz, L.; et al. Subcortical Volumes as Early Predictors of Fatigue in Multiple Sclerosis. Ann. Neurol. 2022, 91, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, O.; Vizzino, C.; Meani, A.; Conti, L.; Riccitelli, G.C.; Preziosa, P.; Filippi, M.; Rocca, M.A. Fatigue in multiple sclerosis patients with different clinical phenotypes: A clinical and magnetic resonance imaging study. Eur. J. Neurol. 2020, 27, 2549–2560. [Google Scholar] [CrossRef] [PubMed]
- Marrie, R.A.; Fisher, E.; Miller, D.M.; Lee, J.C.; Rudick, R.A. Association of fatigue and brain atrophy in multiple sclerosis. J. Neurol. Sci. 2005, 228, 161–166. [Google Scholar] [CrossRef]
- Tedeschi, G.; Dinacci, D.; Lavorgna, L.; Prinster, A.; Savettieri, G.; Quattrone, A.; Livrea, P.; Messina, C.; Reggio, A.; Servillo, G.; et al. Correlation between fatigue and brain atrophy and lesion load in multiple sclerosis patients independent of disability. J. Neurol. Sci. 2007, 263, 15–19. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.P.; Portaccio, E.; Goretti, B.; Zipoli, V.; Ricchiuti, L.; De Caro, M.F.; Patti, F.; Vecchio, R.; Sorbi, S.; Trojano, M. The Rao’s Brief Repeatable Battery and Stroop Test: Normative values with age, education and gender corrections in an Italian population. Mult. Scler. 2006, 12, 787–793. [Google Scholar] [CrossRef]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. A short version of the Stroop test: Normative data in an Italian population sample. Nuova. Riv. Neurol. 2002, 12, 111–115. [Google Scholar]
- Pitteri, M.; Magliozzi, R.; Nicholas, R.; Ziccardi, S.; Pisani, A.I.; Pezzini, F.; Marastoni, D.; Calabrese, M. Cerebrospinal fluid inflammatory profile of cognitive impairment in newly diagnosed multiple sclerosis patients. Mult. Scler. 2022, 28, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Cavedo, E.; Tran, P.; Thoprakarn, U.; Martini, J.B.; Movschin, A.; Delmaire, C.; Gariel, F.; Heidelberg, D.; Pyatigorskaya, N.; Ströer, S.; et al. Validation of an automatic tool for the rapid measurement of brain atrophy and white matter hyperintensity: QyScore®. Eur. Radiol. 2022, 32, 2949–2961. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.K.; Altmann, D.; Barkhof, F.; Miszkiel, K.; Brex, P.A.; O’Riordan, J.; Ebner, M.; Prados, F.; Cardoso, M.J.; Vercauteren, T.; et al. A 30-Year Clinical and Magnetic Resonance Imaging Observational Study of Multiple Sclerosis and Clinically Isolated Syndromes. Ann. Neurol. 2020, 87, 63–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Stefano, N.; Stromillo, M.L.; Giorgio, A.; Bartolozzi, M.L.; Battaglini, M.; Baldini, M.; Portaccio, E.; Amato, M.P.; Sormani, M.P. Establishing pathological cut-offs of brain atrophy rates in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry. 2016, 87, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Filippi, M.; Preziosa, P.; Copetti, M.; Riccitelli, G.; Horsfield, M.A.; Martinelli, V.; Comi, G.; Rocca, M.A. Gray matter damage predicts the accumulation of disability 13 years later in MS. Neurology 2013, 81, 1759–1767. [Google Scholar] [CrossRef]
- Calabrese, M.; Agosta, F.; Rinaldi, F.; Mattisi, I.; Grossi, P.; Favaretto, A.; Atzori, M.; Bernardi, V.; Barachino, L.; Rinaldi, L.; et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch. Neurol. 2009, 66, 1144–1150. [Google Scholar] [CrossRef] [Green Version]
- Calabrese, M.; Poretto, V.; Favaretto, A.; Alessio, S.; Bernardi, V.; Romualdi, C.; Rinaldi, F.; Perini, P.; Gallo, P. Cortical lesion load associates with progression of disability in multiple sclerosis. Brain 2012, 135, 2952–2961. [Google Scholar] [CrossRef] [Green Version]
- Brissart, H.; Sauvée, M.; Latarche, C.; Dillier, C.; Debouverie, M. Integration of cognitive impairment in the expanded disability status scale of 215 patients with multiple sclerosis. Eur. Neurol. 2010, 64, 345–350. [Google Scholar] [CrossRef]
- Morrow, S.A.; Conway, D.; Fuchs, T.; Wojcik, C.; Unverdi, M.; Yasin, F.; Pol, J.; Eckert, S.; Hojnacki, D.H.; Dwyer, M.; et al. Quantifying cognition and fatigue to enhance the sensitivity of the EDSS during relapses. Mult. Scler. 2021, 27, 1077–1087. [Google Scholar] [CrossRef]
- Manjaly, Z.M.; Harrison, N.A.; Critchley, H.D.; Do, C.T.; Stefanics, G.; Wenderoth, N.; Lutterotti, A.; Müller, A.; Stephan, K.E. Pathophysiological and cognitive mechanisms of fatigue in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, O.; Vizzino, C.; Filippi, M.; Rocca, M.A. Current perspectives on the diagnosis and management of fatigue in multiple sclerosis. Expert. Rev. Neurother. 2022, 22, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Pitteri, M.; Ziccardi, S.; Dapor, C.; Guandalini, M.; Calabrese, M. Lost in Classification: Lower Cognitive Functioning in Apparently Cognitive Normal Newly Diagnosed RRMS Patients. Brain Sci. 2019, 9, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joy, J.E.; Johnston, R.B. Multiple Sclerosis: Current Status and Strategies for the Future, 1st ed; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Monk, C.; Fernández, C.R. Neuroscience Advances and the Developmental Origins of Health and Disease Research. JAMA Netw. Open. 2022, 5, e229251. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Brain Volume (Percentiles) | |||||
|---|---|---|---|---|---|
| 0–25 | 25–50 | 50–75 | 75–100 | ||
| Cognitive Status | sCI | 8 | 1 | 0 | 1 |
| mCI | 9 | 6 | 3 | 2 | |
| CN | 6 | 11 | 7 | 2 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziccardi, S.; Pizzini, F.B.; Guandalini, M.; Tamanti, A.; Cristofori, C.; Calabrese, M. Making Visible the Invisible: Automatically Measured Global and Regional Brain Volume Is Associated with Cognitive Impairment and Fatigue in Multiple Sclerosis. Bioengineering 2023, 10, 41. https://doi.org/10.3390/bioengineering10010041
Ziccardi S, Pizzini FB, Guandalini M, Tamanti A, Cristofori C, Calabrese M. Making Visible the Invisible: Automatically Measured Global and Regional Brain Volume Is Associated with Cognitive Impairment and Fatigue in Multiple Sclerosis. Bioengineering. 2023; 10(1):41. https://doi.org/10.3390/bioengineering10010041
Chicago/Turabian StyleZiccardi, Stefano, Francesca Benedetta Pizzini, Maddalena Guandalini, Agnese Tamanti, Cecilia Cristofori, and Massimiliano Calabrese. 2023. "Making Visible the Invisible: Automatically Measured Global and Regional Brain Volume Is Associated with Cognitive Impairment and Fatigue in Multiple Sclerosis" Bioengineering 10, no. 1: 41. https://doi.org/10.3390/bioengineering10010041
APA StyleZiccardi, S., Pizzini, F. B., Guandalini, M., Tamanti, A., Cristofori, C., & Calabrese, M. (2023). Making Visible the Invisible: Automatically Measured Global and Regional Brain Volume Is Associated with Cognitive Impairment and Fatigue in Multiple Sclerosis. Bioengineering, 10(1), 41. https://doi.org/10.3390/bioengineering10010041