

Rehabilitation Practitioners’ Perceptions of Optimal Sitting and Standing Posture in Men with Normal Weight and Obesity

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Survey Design and Piloting
- A closed question regarding the perceived importance of postural education in clinical practice (4-point Likert scale: 1 = not important at all, 4 = very important);
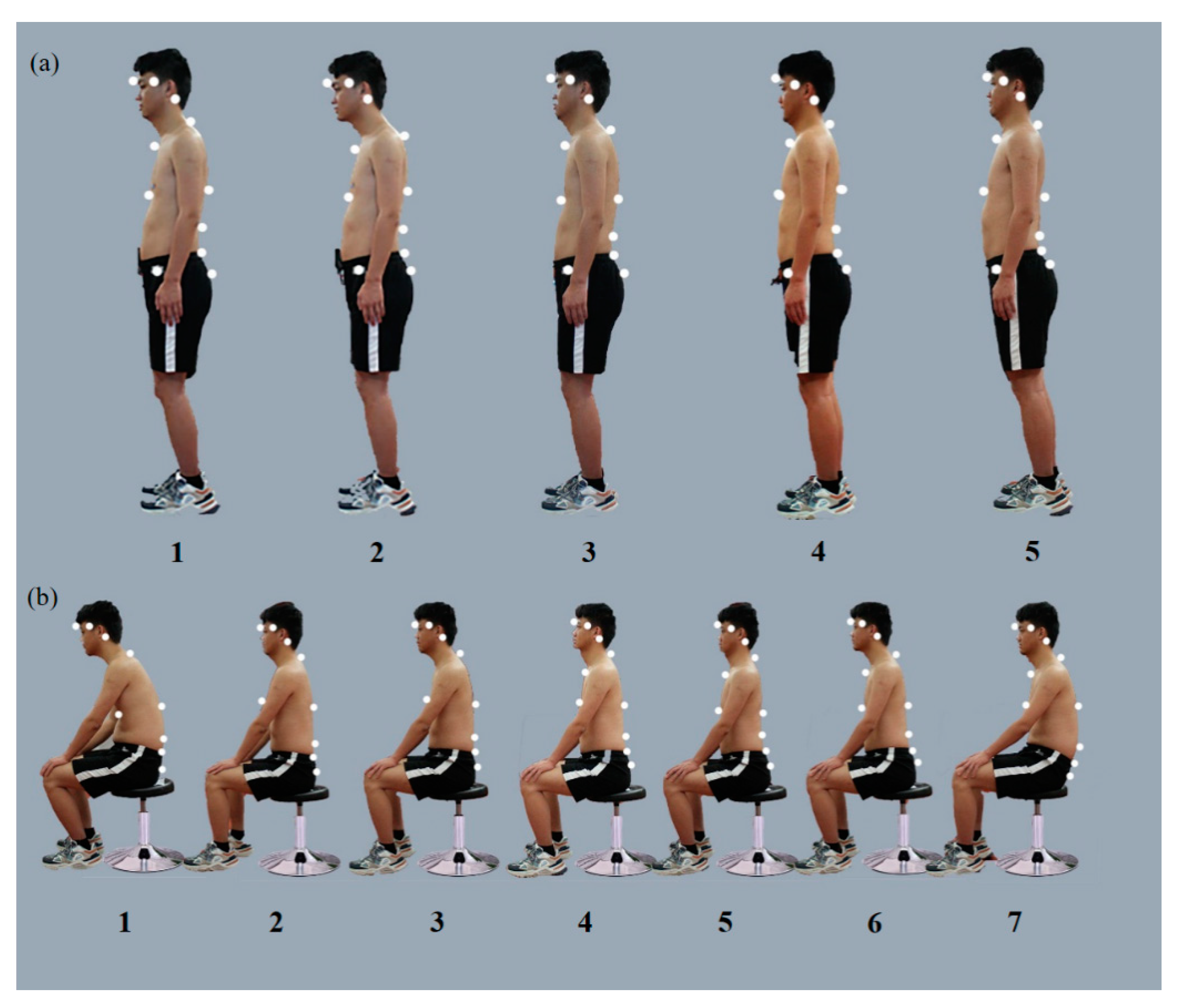
- A multiple-choice between seven SPs and five StPs in different BMI models from photographs to select at least one of each as “optimal” and “harmful” for postural education;
- Free text boxes for choice justification;
- Demographic information, including sex, age, level of educational qualifications, years of experience, clinical area of expertise and certifications, work location, and employment status, was obtained to explore whether these variables could explain any variation in the selection of OP and HP.
2.3. Image Collection of Standing and Sitting Postures
2.4. Angle Analysis among Segments
- Head Angle: The Euler angle between the vertical vector of the head segment and torso segment, reflecting the tilt of the head in the sagittal plane.
- Neck Angle: The angle of neck orientation in the global coordinate system. The neck orientation is the vector connecting the C7 marker to the center of lateral margins of the orbit (CLMO), reflecting the degree of neck flexion.
- Head Title Angle: The angle between the vector connecting CLMO to MPFE and the vertical axis in the global Cartesian coordinate system, reflecting the degree of the head in the coronal plane.
- Cervicothoracic Angle (CTA): The angle formed between the vector constructed from CLMO to C7 and the vector from C7 to T5, reflecting the degree of the head.
- Thoracic Angle: The angle between the vector connecting C7 and T5 and the vector connecting T5 and T10, describing the degree of thoracic kyphosis.
- Thoracolumbar Angle: The angle between the T5 to T10 vectors and the T10 to L3 vectors.
- Lumbar–sacrum Angle (LSA): The Angle between the T10 and L3 vectors and the L3 and S2 vectors, representing the lumbar lordosis angle.
- Pelvic Angle (PA): The angle between the line from the center of the anterior superior iliac spine and the center of the posterior superior iliac spine and its projection on the horizontal plane, reflecting the degree of inclination of the pelvis in the sagittal position.
2.5. Participants
2.6. Data Analysis
3. Results
3.1. Participants and Demographics
3.2. Sagittal Spinal Angles for Sitting and Standing Postures with Normal Weight and Obesity
3.3. The Choice of OP and HP with Different BMI
3.4. Importance of Postural Education and Targeted Training
4. Discussion
4.1. Clinical Significance of Spinal Angle
4.2. The Choice of Optimal Standing and Sitting Postures in Different Body Mass Index
- Lower lumbar segmental kyphosis and kyphosis in the thoracolumbar joint and thoracic vertebrae;
- Flatter spine, less thoracic kyphosis, and lumbar kyphosis;
- The inflection point of thoracic kyphosis, lumbar kyphosis at the thoracolumbar junction, and the peak of lumbar kyphosis at L4;
- Both the lumbar vertebrae and thoracolumbar joints are kyphotic.
4.3. The Choice of Harmful SP and StP with Different BMI
4.4. The Influence of Subspecialty on Posture-Related Choice
4.5. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Grade III Hospital | Grade II Hospital | Grade I Hospital | Self-Employed | Unemployed | Others | |
|---|---|---|---|---|---|---|
| Standing | ||||||
| 1-1 | 8(2.7) | 4(2.2) | 2(10) | 0 | 0 | 0 |
| 1-2 | 2(0.7) | 0 | 0 | 0 | 0 | 0 |
| 1-3 | 21(7.5) | 15(7.7) | 2(10) | 0 | 4(20) | 4(15.4) |
| 1-4 | 235(79.6) | 157(85.7) | 12(60) | 9(90) | 16(80) | 18(69.2) |
| 1-5 | 21(7.5) | 21(12.1) | 4(20) | 0 | 1(5) | 4(15.4) |
| None | 22(7.5) | 6(3.3) | 0 | 1(10) | 1(5) | 4(15.4) |
| 2-1 | 4(1.4) | 8(4.4) | 0 | 2(20) | 1(5) | 3(12.3) |
| 2-2 | 2(0.7) | 0 | 0 | 0 | 0 | 0 |
| 2-3 | 130(44.2) | 80(44.) | 6(30) | 6(60) | 6(30) | 12(46.2) |
| 2-4 | 35(11.6) | 31(17.5) | 2(10) | 0 | 2(10) | 5(20.1) |
| 2-5 | 142(48.3) | 89(48.3) | 12(60) | 0 | 13(65) | 12(46.2) |
| None | 12(4.1) | 2(1.1) | 0 | 2(20) | 2(10) | 2(7.6) |
| Sitting | ||||||
| 1-1 | 2(0.7) | 0 | 0 | 0 | 0 | 0 |
| 1-2 | 70(23.8) | 53(28.6) | 6(30) | 2(20) | 6(30) | 6(23.1) |
| 1-3 | 18(6.1) | 12(6.6) | 0 | 0 | 0 | 1(3.9) |
| 1-4 | 133(44.9) | 88(48.4) | 10(50) | 6(60) | 12(60) | 19(72.4) |
| 1-5 | 156(53.1) | 87(52.8) | 8(40) | 0 | 8(40) | 6(23.1) |
| 1-6 | 14(4.8) | 8(4.4) | 2(10) | 0 | 2(10) | 0 |
| 1-7 | 2(0.7) | 4(2.2) | 1(5) | 0 | 0 | 4(15.4) |
| None | 5(2.0) | 4(2.2) | 0 | 2(20) | 0 | 0 |
| 2-1 | 2(0.7) | 0 | 0 | 0 | 0 | 0 |
| 2-2 | 79(27.2) | 36(19.8) | 4(20) | 1(10) | 6(30) | 8(30.77) |
| 2-3 | 1(0.4) | 0 | 0 | 0 | 0 | 1(3.8) |
| 2-4 | 245(86.5) | 158(86.8) | 18(90) | 7(70) | 16(80) | 20(76.9) |
| 2-5 | 26(8.8) | 21(11.4) | 1(5) | 0 | 4(20) | 2(7.6) |
| 2-6 | 16(5.4) | 10(5.5) | 0 | 2(20) | 0 | 4(15.3) |
| 2-7 | 1(0.4) | 2(1.10) | 0 | 0 | 0 | 0 |
| None | 6(2.0) | 0 | 0 | 0 | 0 | 4(15.3) |
| Grade III Hospital | Grade II Hospital | Grade I Hospital | Self-Employed | Unemployed | Others | |
|---|---|---|---|---|---|---|
| Standing | ||||||
| 1-1 | 186(63.3) | 100(55.0) | 14(70) | 6(60) | 16(80) | 12(46.2) |
| 1-2 | 257(87.1) | 141(78.0) | 18(90) | 9(90) | 19(95) | 20(76.9) |
| 1-3 | 139(47.6) | 79(42.9) | 8(40) | 6(60) | 8(40) | 8(30.77) |
| 1-4 | 16(5.4) | 4(2.2) | 0 | 0 | 1(5) | 1(3.5) |
| 1-5 | 152(51.7) | 94(51.7) | 14(70) | 8(80) | 14(70) | 16(61.5) |
| None | 4(1.4) | 2(1.1) | 0 | 0 | 0 | 0 |
| 2-1 | 133(45.4) | 60(33.0) | 10(50) | 6(60) | 14(70) | 8(30.78 |
| 2-2 | 282(95.9) | 163(90.1) | 20(100) | 6(60) | 18(90) | 20(76.9) |
| 2-3 | 34(11.6) | 24(13.2) | 1(10) | 1(10) | 1(5) | 4(15.4) |
| 2-4 | 140(47.6) | 72(39.6) | 15(75) | 9(90) | 13(65) | 10(38.5) |
| 2-5 | 44(15.0) | 24(13.2) | 0 | 4(40) | 2(10) | 6(23.1) |
| None | 3(1.8) | 4(2.20) | 0 | 0 | 0 | 0 |
| Sitting | ||||||
| 1-1 | 279(94.6) | 166(91.2) | 20(100) | 10(100) | 20(100) | 20(76.9) |
| 1-2 | 50(17.0) | 26(14.3) | 1(5) | 0 | 1(5) | 2(7.69) |
| 1-3 | 127(42.9) | 54(29.7) | 11(55) | 4(40) | 13(65) | 10(38.5) |
| 1-4 | 40(13.61) | 16(8.8) | 6(30) | 2(20) | 4(20) | 0 |
| 1-5 | 40(13.61) | 20(11.0) | 0 | 2(20) | 4(20) | 4(15.4) |
| 1-6 | 116(39.46) | 68(37.4) | 8(40) | 4(40) | 4(40) | 8(30.8) |
| 1-7 | 196(66.67) | 118(64.8) | 10(50) | 6(60) | 16(80) | 16(61.5) |
| None | 4(1.36) | 2(1.10) | 0 | 0 | 0 | 0 |
| 2-1 | 264(93.2) | 152(83.5) | 16(80) | 10(100) | 20(100) | 21(84.6) |
| 2-2 | 54(18.4) | 36(19.8) | 0 | 2(20) | 4(20) | 2(7.7) |
| 2-3 | 181(61.9) | 101(56.0) | 16(80) | 6(60) | 14(70) | 12(46.2) |
| 2-4 | 12(4.1) | 2(1.10) | 0 | 4(40) | 2(10) | 4(15.4) |
| 2-5 | 96(31.3) | 42(23.1) | 3(15) | 6(60) | 8(40) | 6(23.1) |
| 2-6 | 194(32.0) | 42(23.1) | 8(40) | 3(30) | 6(30) | 6(23.1) |
| 2-7 | 226(76.9) | 141(78.0) | 17(85) | 5(50) | 18(90) | 18(69.2) |
| None | 4(1.4) | 2(1.10) | 0 | 0 | 0 | 0 |
References
- AAOS. Posture and Its Relationship to Orthopaedic Disabilities. A Report of the Posture Committee of the American Academy of Orthopaedic Surgeons; AAOS: Rosemont, IL, USA, 1947. [Google Scholar]
- Woodhull, A.M.; Maltrud, K.; Mello, B.L. Alignment of the human body in standing. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 109–115. [Google Scholar] [CrossRef]
- Kendall, F.P.; Mccreary, E.K.; Provance, P.G.; Rodgers, M.I.; Romani, W.A. Testing and Function, with Posture and Pain. In Muscles; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Harrison, D.D.; Harrison, S.O.; Croft, A.C.; Harrison, D.E.; Troyanovich, S.J. Sitting biomechanics part I: Review of the literature. J. Manip. Physiol. Ther. 1999, 22, 594–609. [Google Scholar] [CrossRef]
- Kuchera, M. Gravitational stress, musculoligamentous strain, and postural alignment. Spine State Art Rev. 1995, 9, 463–489. [Google Scholar]
- Kapandji, I.A. The Physiology of the Joints; Churchill Livingstone: New York, NY, USA, 1970; pp. 215–216. [Google Scholar]
- Gallagher, K.M.; Callaghan, J.P. Early static standing is associated with prolonged standing induced low back pain. Hum. Mov. Sci. 2015, 44, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, S.; Azevedo, D.C.; Dillen, L.V. Diagnosis and treatment of movement system impairment syndromes. Braz. J. Phys. Ther. 2017, 21, 391–399. [Google Scholar] [CrossRef]
- Mckenzie, R.; May, S. Orthopedic Physical Therapy Products. In The Lumbar Spine: Mechanical Diagnosis and Therapy; OPTP: Plymouth, MN, USA, 2003; p. 462. [Google Scholar]
- Magee, D.J. Orthopedic Physical Assessment, 4th ed.; Elsevier Health Sciences: Saunders, MO, USA, 2005; pp. 978–982. [Google Scholar]
- Korakakis, V.; Sideris, V.; Giakas, G. Sitting bodily configuration: A study investigating the intra-tester reliability of positioning subjects into a predetermined sitting posture. Man Ther. 2014, 19, 197–202. [Google Scholar] [CrossRef]
- Nachemson, A. The load on lumbar disks in different positions of the body. Clin. Orthop. Relat. Res. 1966, 45, 107–122. [Google Scholar] [CrossRef]
- Andersson, G.B.; Ortengren, R.; Nachemson, A. Intradiskal pressure, intra-abdominal pressure and myoelectric back muscle activity related to posture and loading. Clin. Orthop. Relat. Res. 1977, 129, 156–164. [Google Scholar] [CrossRef]
- Adams, M.A.; Mcmillan, D.W.; Green, T.P.; Dolan, P. Sustained loading generates stress concentrations in lumbar intervertebral discs. Spine 1996, 21, 434–438. [Google Scholar] [CrossRef]
- Korakakis, V.; O’Sullivan, K.; O’Sullivan, P.B.; Evagelinou, V.; Sotiralis, Y.; Sideris, A.; Sakellariou, K.; Karanasios, S.; Giakas, G. Physiotherapist perceptions of optimal sitting and standing posture. Musculoskelet. Sci. Pract. 2019, 39, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Korakakis, V.; Giakas, G.; Sideris, V.; Whiteley, R. Repeated end range spinal movement while seated abolishes the proprioceptive deficit induced by prolonged flexed sitting posture. A study assessing the statistical and clinical significance of spinal position sense. Musculoskelet. Sci. Pract. 2017, 31, 9–20. [Google Scholar] [CrossRef]
- O’Sullivan, K.; O’Sullivan, P.; O’Sullivan, L.; Dankaerts, W. What do physiotherapists consider to be the best sitting spinal posture? Man Ther. 2012, 17, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Gollogly, S.; Berthonnaud, E.; Dimnet, J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine 2005, 30, 346–353. [Google Scholar] [CrossRef]
- Muyor, J.M.; Arrabal-Campos, F.M.; Martínez-Aparicio, C.; Sánchez-Crespo, A.; Villa-Pérez, M. Test-retest reliability and validity of a motion capture (MOCAP) system for measuring thoracic and lumbar spinal curvatures and sacral inclination in the sagittal plane. J. Back Musculoskelet. Rehabil. 2017, 30, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.J.; Tromp, R.; Swann, M.C.; White, A.P.; Anderson, D.E. Between-session reliability of opto-electronic motion capture in measuring sagittal posture and 3-D ranges of motion of the thoracolumbar spine. J. Biomech. 2018, 79, 248–252. [Google Scholar] [CrossRef]
- Castanharo, R.; Duarte, M.; Mcgill, S. Corrective sitting strategies: An examination of muscle activity and spine loading. J. Electromyogr. Kinesiol. 2014, 24, 114–119. [Google Scholar] [CrossRef]
- Claus, A.P.; Hides, J.A.; Moseley, G.L.; Hodges, P.W. Is ’ideal’ sitting posture real? Measurement of spinal curves in four sitting postures. Man Ther. 2009, 14, 404–408. [Google Scholar] [CrossRef]
- O’Sullivan, K.; O’Sullivan, L.; O’Sullivan, P.; Dankaerts, W. Investigating the effect of real-time spinal postural biofeedback on seated discomfort in people with non-specific chronic low back pain. Ergonomics 2013, 56, 1315–1325. [Google Scholar] [CrossRef]
- Richards, K.V.; Beales, D.J.; Smith, A.J.; O’Sullivan, P.B.; Straker, L.M. Neck posture clusters and their association with biopsychosocial factors and neck pain in Australian adolescents. Phys. Ther. 2016, 96, 1576–1587. [Google Scholar] [CrossRef]
- Dankaerts, W.; O’Sullivan, P.; Burnett, A.; Straker, L. Differences in sitting postures are associated with nonspecific chronic low back pain disorders when patients are subclassified. Spine 2006, 31, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Vergara, M.; Page, A. Relationship between comfort and back posture and mobility in sitting-posture. Appl. Ergon. 2002, 33, 1–8. [Google Scholar] [CrossRef]
- Scannell, J.P.; McGill, S.M. Lumbar posture--Should it, and can it, be modified? A study of passive tissue stiffness and lumbar position during activities of daily living. Phys. Ther. 2003, 83, 907–917. [Google Scholar] [CrossRef]
- Pillastrini, P.; Mugnai, R.; Bertozzi, L.; Costi, S.; Curti, S.; Guccione, A.; Mattioli, S.; Violante, F.S. Effectiveness of an ergonomic intervention on work-related posture and low back pain in video display terminal operators: A 3 year cross-over trial. Appl. Ergon. 2010, 41, 436–443. [Google Scholar] [CrossRef]
- Kuo, Y.L.; Tully, E.A.; Galea, M.P. Video based measurement of sagittal range of spinal motion in young and older adults. Man Ther. 2009, 14, 618–622. [Google Scholar] [CrossRef]
- Yip, C.H.; Chiu, T.T.; Poon, A.T. The relationship between head posture and severity and disability of patients with neck pain. Man Ther. 2008, 13, 148–154. [Google Scholar] [CrossRef]
- Andersen, J.H.; Haahr, J.P.; Frost, P. Risk factors for more severe regional musculoskeletal symptoms: A two-year prospective study of a general working population. Arthritis Rheum. 2007, 56, 1355–1364. [Google Scholar] [CrossRef]



| (n) | % | ||
|---|---|---|---|
| Sex | Male | 285 | 51.81 |
| Female | 267 | 48.19 | |
| Age | 18–25 | 151 | 27.54 |
| 26–30 | 189 | 34.42 | |
| 31–40 | 173 | 31.16 | |
| 41–50 | 31 | 5.43 | |
| 51–60 | 8 | 1.45 | |
| Qualifications | Undergraduate | 27 | 4.71 |
| Bachelor | 449 | 81.52 | |
| Master | 64 | 11.59 | |
| Doctor | 12 | 2.17 | |
| Expertise | Rehabilitation doctor | 77 | 13.95 |
| PT | 365 | 66.12 | |
| OT | 33 | 5.98 | |
| ST | 22 | 3.99 | |
| Others | 55 | 9.96 | |
| Area of PT (multiple choices) | Musculoskeletal | 236 | 63.19 |
| Neurological | 194 | 46.15 | |
| Cardiopulmonary | 34 | 8.59 | |
| Children | 46 | 11.62 | |
| Orthopedic | 164 | 43.96 | |
| Sports injuries | 140 | 37.91 | |
| Others | 42 | 11.54 | |
| Years of expertise | 0–3 | 175 | 31.88 |
| Work status | 3–6 | 119 | 21.38 |
| 6–10 | 137 | 24.64 | |
| >10 | 121 | 22.1 | |
| Grade III hospital | 293 | 53.26 | |
| Grade II hospital | 183 | 32.97 | |
| Grade I hospital | 19 | 3.62 | |
| Self-employed | 10 | 1.81 | |
| Unemployed | 21 | 3.62 | |
| Others | 26 | 4.71 |
| Posture | HA(°) | NA(°) | HTA(°) | CTA(°) | TA(°) | TLA(°) | LSA(°) | PA(°) | |
| STANDING | 1-1 | 74.9 | 57.9 | 103.4 | 149.1 | 157.1 | 154.7 | 153.8 | 7.1 |
| 1-2 | 66.0 | 45.0 | 99.1 | 155.5 | 163.2 | 160.1 | 153.7 | 9.6 | |
| 1-3 | 62.5 | 36.9 | 100.7 | 161.1 | 166.4 | 160.6 | 152.8 | 9.4 | |
| 1-4 | 61.0 | 43.9 | 96.0 | 157.9 | 161.5 | 157.6 | 148.3 | 9.9 | |
| 1-5 | 64.2 | 45.7 | 97.1 | 155.7 | 162.8 | 160.1 | 152.4 | 10.3 | |
| Posture | HA(°) | NA(°) | HTA(°) | CTA(°) | TA(°) | TLA(°) | LSA(°) | PA(°) | |
| SITTING | 1-1 | 86.5 | 60.5 | 102.8 | 137.2 | 164.7 | 158.5 | 174.5 | −14.4 |
| 1-2 | 61.7 | 48.0 | 94.0 | 155.2 | 169.5 | 169.7 | 170.9 | −13.1 | |
| 1-3 | 70.1 | 61.1 | 96.3 | 147.5 | 163.6 | 166.1 | 171.4 | −14.2 | |
| 1-4 | 57.2 | 43.4 | 94.2 | 160.0 | 168.7 | 169.7 | 163.2 | −10.5 | |
| 1-5 | 62.6 | 45.7 | 95.7 | 156.0 | 169.4 | 165.3 | 176.4 | −25.9 | |
| 1-6 | 62.1 | 49.1 | 93.6 | 154.5 | 168.4 | 164.9 | 175.9 | −25.1 | |
| 1-7 | 69.0 | 52.9 | 95.9 | 149.5 | 164.3 | 162.9 | 175.2 | −23.7 |
| Posture | HA(°) | NA(°) | HTA(°) | CTA(°) | TA(°) | TLA(°) | LSA(°) | PA(°) | |
| STANDING | 2-1 | 60.0 | 48.7 | 98.4 | 157.2 | 154.8 | 175.1 | 156.2 | 14.4 |
| 2-2 | 57.2 | 54.4 | 97.8 | 157.5 | 153.4 | 177.3 | 154.8 | 15.9 | |
| 2-3 | 60.8 | 39.9 | 104.5 | 162.7 | 158.4 | 179.2 | 153.8 | 19.4 | |
| 2-4 | 56.1 | 42.8 | 99.2 | 163.6 | 160.1 | 177.9 | 156.1 | 15.8 | |
| 2-5 | 57.5 | 38.1 | 103.6 | 165.7 | 158.3 | 177.1 | 153.5 | 18.6 | |
| Posture | HA(°) | NA(°) | HTA(°) | CTA(°) | TA(°) | TLA(°) | LSA(°) | PA(°) | |
| SITTING | 2-1 | 74.7 | 61.5 | 91.4 | 135.9 | 162.3 | 162.8 | 166.0 | −12.8 |
| 2-2 | 65.9 | 44.8 | 104.7 | 157.1 | 162.7 | 175.6 | 156.4 | −11.4 | |
| 2-3 | 67.0 | 49.9 | 101.3 | 153.0 | 159.0 | 174.2 | 155.0 | −10.6 | |
| 2-4 | 70.2 | 40.6 | 111.2 | 159.0 | 163.0 | 177.4 | 169.0 | 3.08 | |
| 2-5 | 57.7 | 38.3 | 101.8 | 165.1 | 164.1 | 176.7 | 164.2 | 5.09 | |
| 2-6 | 64.5 | 47.0 | 105.2 | 157.9 | 160.7 | 178.2 | 166.6 | 5.5 | |
| 2-7 | 67.2 | 48.0 | 99.7 | 151.9 | 164.9 | 166.5 | 164.6 | −23.5 |
| Subspecialty | Frequency of Postural Assessment | Frequency of Postural Training | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No | Sometimes | Often | Every Time | No | Sometimes | Often | Every Time | |||
| Musculoskeletal | 6(2.5) | 52(22.0) | 91(39.0) | 87(36.5) | * | 3(0.8) | 31(13.6) | 95(39.8) | 107(45.8) | # |
| Neurological | 8(4.1) | 69(35.5) | 67(34.6) | 49(25.8) | 8(4.1) | 30(15.5) | 69(35.1) | 87(45.3) | ||
| Cardiopulmonary | 0(0) | 8(23.5) | 12(35.3) | 14(41.2) | 0 | 4(11.8) | 6(17.7) | 23(70.5) | ||
| Children | 2(4.4) | 3(6.6) | 24(52.2) | 17(34.8) | # | 1(2.1) | 6(13.2) | 14(30.8) | 25(53.9) | |
| Orthopedic | 2(1.2) | 36(21.6) | 68(40.5) | 58(36.7) | 3(1) | 21(13) | 61(37) | 79(49) | ||
| Sports injuries | 0 | 23(17.1) | 62(44.3) | 55(38.6) | * | 0 | 16(11.4) | 50(35.8) | 74(52.8) | # |
| Others | 1(1) | 16(38.1) | 13(33.2) | 12(28.6) | 1(2.4) | 6(14.1) | 18(42.6) | 17(40.9) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, J.; Jiang, Z.; Chen, S.; Cheng, R.; Xu, L.; Tsai, T.-Y. Rehabilitation Practitioners’ Perceptions of Optimal Sitting and Standing Posture in Men with Normal Weight and Obesity. Bioengineering 2023, 10, 210. https://doi.org/10.3390/bioengineering10020210
Ye J, Jiang Z, Chen S, Cheng R, Xu L, Tsai T-Y. Rehabilitation Practitioners’ Perceptions of Optimal Sitting and Standing Posture in Men with Normal Weight and Obesity. Bioengineering. 2023; 10(2):210. https://doi.org/10.3390/bioengineering10020210
Chicago/Turabian StyleYe, Jiling, Ziang Jiang, Shijie Chen, Rongshan Cheng, Lili Xu, and Tsung-Yuan Tsai. 2023. "Rehabilitation Practitioners’ Perceptions of Optimal Sitting and Standing Posture in Men with Normal Weight and Obesity" Bioengineering 10, no. 2: 210. https://doi.org/10.3390/bioengineering10020210
APA StyleYe, J., Jiang, Z., Chen, S., Cheng, R., Xu, L., & Tsai, T.-Y. (2023). Rehabilitation Practitioners’ Perceptions of Optimal Sitting and Standing Posture in Men with Normal Weight and Obesity. Bioengineering, 10(2), 210. https://doi.org/10.3390/bioengineering10020210