Abstract
Oral potentially malignant disorders (OPMD) and oral squamous cell carcinoma (OSCC) represent a significant global health burden due to their potential for malignant transformation and the challenges associated with their diagnosis and treatment. Chemoprevention, an innovative approach aimed at halting or reversing the neoplastic process before full malignancy, has emerged as a promising avenue for mitigating the impact of OPMD and OSCC. The pivotal role of chemopreventive strategies is underscored by the need for effective interventions that go beyond traditional therapies. In this regard, chemopreventive agents offer a unique opportunity to intercept disease progression by targeting the molecular pathways implicated in carcinogenesis. Natural compounds, such as curcumin, green tea polyphenols, and resveratrol, exhibit anti-inflammatory, antioxidant, and anti-cancer properties that could make them potential candidates for curtailing the transformation of OPMD to OSCC. Moreover, targeted therapies directed at specific molecular alterations hold promise in disrupting the signaling cascades driving OSCC growth. Immunomodulatory agents, like immune checkpoint inhibitors, are gaining attention for their potential to harness the body’s immune response against early malignancies, thus impeding OSCC advancement. Additionally, nutritional interventions and topical formulations of chemopreventive agents offer localized strategies for preventing carcinogenesis in the oral cavity. The challenge lies in optimizing these strategies for efficacy, safety, and patient compliance. This review presents an up to date on the dynamic interplay between molecular insights, clinical interventions, and the broader goal of reducing the burden of oral malignancies. As research progresses, the synergy between early diagnosis, non-invasive biomarker identification, and chemopreventive therapy is poised to reshape the landscape of OPMD and OSCC management, offering a glimpse of a future where these diseases are no longer insurmountable challenges but rather preventable and manageable conditions.
1. Introduction
Oral cancer is the sixth tumor by incidence that affects the world population and the diagnosis of around 90% of the cases is oral squamous cell carcinoma [1]. Oral squamous carcinoma is an aggressive type of cancer that gives the patients a survival rate of less than 50% at 5 years [2,3]. Smoking tobacco and the abuse of alcohol are the main risk factors for oral cancer development [4]. Along with these two risk factors, there are precancerous lesions called oral potential malignance disorders (OPMDs) that include oral leukoplakia, erythroplakia, lichen planus, and submucosal fibrosis [5]. The oral epithelium malignant transformation is the result of various mechanisms that require time for the clinic manifestation (Figure 1). The epithelial transition is not clinically visible, and it begins to be visible in the form of OPMDs [6].
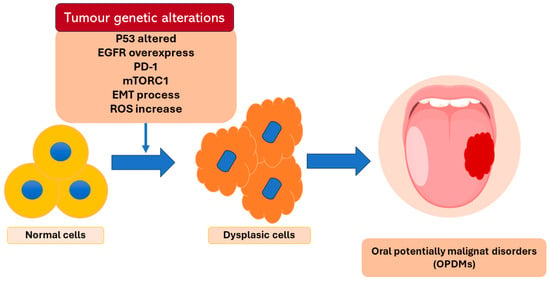
Figure 1.
Description of some of the genetic alterations at the base of the epithelium dysplasia transformation.
These oral precancerous lesions are frequently asymptomatic, so most of the patients do not notice them. Consequently, patients arrive at the clinic observation when carcinoma is just probably present. Therefore, for the clinician, there are limits related to the impossibility of distinguishing premalignant oral lesions from oral cancer in situ for similar clinical manifestations [7]. In these cases, surgery, radiotherapy, and chemotherapy are the traditional treatments that are usually used. Sometimes the tumor can extend into accessible anatomical areas and the use of surgery is not always possible. Then, in these cases, surgery is frequently associated with radiotherapy or chemotherapy. All three previous treatments determine important side effects for a patient’s quality of life [8,9]. Additionally, even if the tumor can be removed with traditional therapies the survival rate after 5 years is still lower, despite the important progress achieved in the oncology field in the last three decades [10]. The survival rate for oral squamous cell carcinoma is still around 50%, and the risk of recurrence is high. Another type of treatment is the reduction of risk factors like quitting smoking, but it is not immediate [11]. For these reasons, prevention plays a fundamental role in contrasting tumor development and increases survival rates. The introduction of chemopreventive strategies in the oral cancer field aims to intercept the presence of an altered oral epithelium to suppress the possible malignant progression. Cancer chemoprevention is defined as the administration of a synthetic, natural, or biological agent to reverse, suppress, or prevent either the initial phases of carcinogenesis or the progression of premalignant cells to malignancy. Over the past ten years, there has been a significant shift in the paradigm for creating new chemopreventive drugs. Currently, agents undergo thorough preclinical mechanistic testing before beginning clinical trials, and there is a greater emphasis on identifying biomarkers of activity that can be utilized as early indicators of efficacy [12]. Various preclinic, animal studies, in vitro studies, and clinic trials, have been conducted over the years but there are still no existing guidelines for their use.
This review aims to describe the chemoprevention strategies that have been developed over the years that could be used for the treatment of oral potentially premalignant disorders and oral squamous cell carcinoma.
2. Oral Squamous Carcinoma and Oral Potentially Malignant Disorders
Oral cancer is a type of cancer that takes part in the group of head and neck cancers. Oral squamous cell carcinoma (OSCC) is the most common oral cancer that represents 90% of the other oral, head and neck cancers related with others oral diseases [13,14]. It is a malignant epithelial neoplasm characterized by the presence of keratin or intercellular bridges in the oral epithelium [15]. OSCC can be observed in all parts of the oral cavity [16]. The tongue, the buccal mucosa, and the lips are the typical sites where it is most frequently encountered [17]. Tobacco and alcohol are the two main risk factors of OSCC. 75% of oral cancer cases are related to tobacco smoking [4], in fact, smokers have a five times greater risk of oral cancer evolving than nonsmokers [18]. Tobacco smoke includes not less than 70 carcinogens and cancer-promoting essences [19]. The carcinogen benzo[a]pyrene (BaP) is the main constituent of cigarettes. The metabolization of BaP by cytochrome P450 enzyme allows the production of an active carcinogenic substance that can obstruct the DNA replication mechanism [20], causing cytotoxicity, teratogenicity, genotoxicity, immunotoxicity, mutagenesis, and carcinogenesis [20,21]. Alcohol consumption plays an important role in the evolution of OSCC due to its properties: (a) changes the oral mucosa permeability causing the increase of the carcinogen’s substances, (b) disintegrates the epithelium’s lipids causing the atrophy and the decrease of the mucosa layer, (c) alters the DNA synthesis and the repair mechanisms due to the acetaldehyde metabolism, (d) reduces the physiological carcinogen clearance altering the salivary gland activity [22,23,24,25].
Human papillomavirus infection, in particular HPV type 16, is a secondary risk factor of OSCC that affects less than 15% of the worldwide cases [26,27]. HPV type 16 in the human cell causes the synthesis of two oncoproteins called E6 and E7. These two oncoproteins are capable of altering the physiological function of p53 and RB1 increasing the possibility of causing lesions in the oral epithelial cells [28,29,30].
A diet poor of vegetables and fruits was seen to be another risk factor that can increase the susceptibility to develop OSCC. This is related to the fact that these foods contain phytochemicals (carotenoids, antioxidants, vitamins, phenols, terpenoids, steroids, indoles, and fibers) that are substances able to contrast the risk of developing oral pathologies [31,32]. Immune conditions (including people using immunosuppressant drugs for organ transplants), occupational exposures (UV radiation), environment pollutants, microorganisms, and genetic diseases (Fanconi anemia, dyskeratosis congenita, and Bloom syndrome) are further oral cancer risk factors [33,34,35,36]. The oral potentially malignant disorders (OPMDs) are added to the risk factors of OSCC (Figure 2).
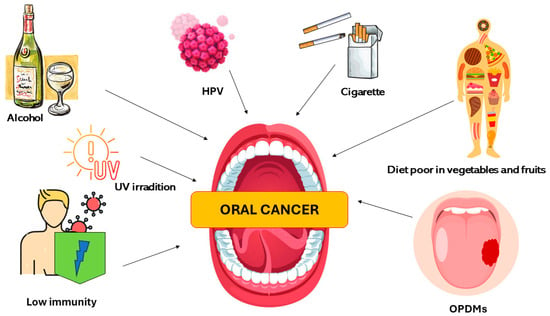
Figure 2.
Description of the major oral cancer risk factors.
In 2017, the World Health Organization (WHO) defined oral potentially malignant disorders (OPMDs) as a group of oral mucosal conditions with a high risk of malignant progression [37]. This new category was born because it was documented that the oral tissue affected by these conditions later evolved into OSCC. Additionally, the red and white tissue alterations that characterize these conditions can be present simultaneously in the border of the frank OSCC tissue [38,39,40]. The term “potentially malignant” underlines that not always the altered oral mucosa affected by these conditions will necessarily evolve in oral carcinoma. This term means that one of the OPMDs increases the susceptibility to the development of OSCC anywhere in the oral cavity [5,41]. The precancerous lesions (leukoplakia, erythroplakia, and proliferative verrucous leukoplakia) and the precancerous conditions (lichen planus and submucosal fibrosis) [42] take part in the OPMDs group. Leukoplakia is the most common precancerous oral lesion that affects 1–4% of the population [37,43]. Clinically it appears as white with rugose, granulomatous, or warty and nodular lesions, similar to lichen lesions [37,44,45]. In front of the leukoplakia lesions, no other diagnosis can relate the oral lesions to other causes. Leukoplakia shows a variable percentual risk of malignancy transformation from 1.5% to 34%. It is important to say that leukoplakia lesions can be homologous, and the risk of malignancy transformation is related to this clinic’s appearance. There is a non-homologous rare leukoplakia lesion called proliferative verrucous leukoplakia. It has the highest risk of oral cancer development which is from 63.3% to 100% [5]. The clinical aspect of the proliferative verrucous leukoplakia starts from a flat white lesion and develops into a verrucous and multilocular white lesion. The adjective “proliferative” underlines its characteristic of gradual extension in the near area [46,47].
Erythroplakia is another precancerous oral lesion that affects 0.02% to 0.83% of the population [48,49]. Clinically, it appears as a red spot with or without nodules, erosions, and granules. As for leukoplakia, no other diagnosis can be done [48]. For all the precancerous lesions and precancerous conditions, the diagnosis is only histological after the tissue biopsy analysis. The risk of malignancy development erythroplakia lesion is 14% to 50% [49].
Lichen planus is an oral condition characterized by the presence of chronic inflammation of the mucosa. It affected from 0.1% to 4% of the population [50]. It is an oral premalignant condition that clinically manifests itself as a bilateral white network spot [51]. Oral submucous fibrosis is the other condition that takes part in the OPMDs group. Oral submucous fibrosis is an oral condition with a high risk of oral cancer transformation that is around 9–13%. This oral condition is characterized by the gradual transformation from functional tissue to functional due to the deposit of fibrous bands [52].
3. Chemoprevention
In 1976 Sporn was the first who introduce the term chemoprevention [53]. Chemoprevention relies on using different natural, synthetic, biological, and chemical substances that possess anticarcinogenic actions (reverse, suppress, and prevent carcinogenic progression) [54,55,56]. Based on the target people, cancer chemoprevention strategies are divided into two categories, primary prevention, and secondary prevention. Primary prevention aims to persuade people with high risk to develop OSCC or OPMDs by changing their habits, for instance by reducing or quitting smoking. Secondary prevention has targeted patients with OPMDs or OSCC. In these cases, the prevention aims to reduce or eliminate the possibility that an OPMD lesion can have a malignant transformation and the primary OSCC lesion can have recurrences [57]. Over the years various studies have been conducted to test chemopreventive agents. The chemopreventive agents can be administered systemically, locally, and by nanoparticle delivery systems. Each of these types of administration has been shown to possess efficacy but also limits. The chemopreventive agents show many mechanisms of action against tumor cells. They can suppress the initial phase of the tumor cell transformation, operate on the altered genome induce apoptosis, and modulate the metabolic activities of the tumor cell arresting it [58].
A chemoprotective agent must possess no toxicity, show efficacy in many parts of the human body, be cheap, be orally administered, be acceptable for human uses, and be secure in its mechanisms of action [59]. The proprieties that chemopreventive agents possess allow their use for the treatment of oral precancerous lesions, but also in the early phases of the OSCC establishment. Then, chemopreventive agents can be used as a method of secondary and tertiary prevention. However, studies conducted in oral chemoprevention are still in their primordial phase and the pathogenetic mechanisms underlying oral dysplasia and carcinogenesis are not fully clarified. Consequently, most of the agents evaluated to date act predominantly with anti-oxidant, anti-inflammatory, and/or oncolytic mechanisms [60].
4. Phytochemical Compounds as Chemopreventive Strategy
Phytochemical compounds can be used in the chemopreventive strategies for the treatment of OSCC and OPMDs. As mentioned before, one of the factors that increase the risk of developing OPMDs and OSCC is following an incorrect diet. In fact, many studies have shown that a diet full of vegetables and fruits is associated with a low risk of premalignant and malignant lesion development [61,62,63,64,65,66,67]. Given that, the possibility of using phytochemicals contained in natural food as chemoprevention has caught the academic community’s interest (Table 1). Moreover, several researchers have found that the natural compounds present in food and drinks have no side effects [68]. Classifying phytochemicals into polyphenolic compounds, carotenoids, phytosterols, nitrogen compounds, and organosulfur compounds is possible.
4.1. Polyphenolic Compounds
This group of phytochemical agents possesses antioxidant, anti-inflammatory, and anti-carcinogenesis properties (Figure 3). Related to the anti-carcinogenesis propriety these agents inhibit different phases of the cancer growth from the beginning to the progression. Polyphenolic agents can induce oral cancer cell death reducing the progression, invasion, and metastasis of the tumor [69,70,71]. Polyphenolic substances can be divided based on their chemical structure into flavonoids and non-flavonoids [72].
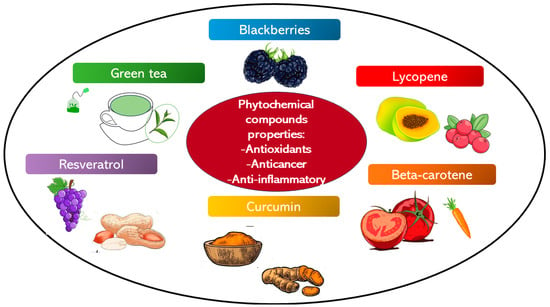
Figure 3.
The illustration regroups the phytochemical compounds with antioxidant, anti-cancer, and anti-inflammatory properties, which have been studied as chemopreventive agents.
4.1.1. Green Tea
Green tea (Camellia sinensis) is a component of the class of polyphenolic agents. It is normally consumed as a beverage in water. Green tea is mainly composed of four polyphenols called Epicatechin (EC), epigallocatechin (EGC), epicatechin-3-gallate (ECG), epigallocatechin-3-gallate (EGCG) [73]. Researchers have seen that green tea protects from oral-digestive cancer development, and it possesses inhibitory properties against the progress of oral precancerous lesions [74]. The main constituent of green tea that expresses many of the anti-carcinogenesis actions is EGCG. EGCG can regulate the expression of the epidermal growth factor receptor (EGFR) [75,76], the NF-κB and AP-1 factors reducing the tumoral cell’s proliferation and migration [63]. In Irimie’s study, ECGC has been shown to cause tumor cell death inducing apoptosis and autophagy [77]. The polyphenols that make green tea possess antioxidant properties. Therefore, from numerous investigations other anti-carcinogenesis mechanisms of ECGC have emerged. In a study conducted by Koh et al. [78] ECGC was administered in mice affected by squamous cell carcinoma. In the mice tested, there was a suppression of the cancer progress and invasion [78]. In an in vivo study, a mix of tropical green tea was orally and topically administered in patients affected by oral leukoplakia. The patients were treated for 6 months. After this period 40% of the patients tested showed a reduction of the oral lesion size compared to the control group (not treated). The histological analysis results were related to the significative reduction of cell proliferation [79]. In a study conducted by Gao et al. [80] another biological antitumor target against oral cancer of ECGC has emerged. In the in vitro study ECGC was administered in different concentrations in multiple human tongue carcinoma cell cultures. From this experiment has emerged that ECGC has a dose-dependent effect in decreasing EGFR expression. The same effect of ECGC against EGFR was seen against the hexokinase 2 (HK2). HK2 is an important enzyme that allows to start of glycolysis. Glycolysis is fundamental for the beginning of tumor development and progression. The authors have concluded that HK2 could be a new target for ECGC in preventing and treating human tongue carcinoma [80]. In two clinical trials, people who drink more than 10 cups of green tea daily have less risk of developing cancer than those who drink 3 or fewer cups. Furthermore, smokers who consume tea extract (2000–2500 mg/day) for 4 weeks have shown a decrease in DNA damage in oral squamous cells [81,82]. In a study conducted by Neetha et al. [83] the effect of the administration of curcumin and green tea in patients affected by OPMDs for 3 months was evaluated. From the histologic analyses of the tissue of the group of patients that received the combination of the two phytochemical agents, there was a high clinical response and improvement of the tissues. Moreover, in the group tested with the mixed combination, there was a higher downregulation of p53 and proliferation markers (cyclin D1, Ki 67) compared to the other group treated with only one of the natural agents [83]. In another study, the synergy of green tea with resveratrol was evaluated. From this in vitro study a mix with different concentrations of the two natural compounds was administered in a culture of head and neck cancer cell lines. At the end of the study have emerged that there was a dose-dependency of effects based on the combination of green tea and resveratrol. The group treated with both the natural agents showed a higher tumor cell death compared to the other group treated with the single natural compounds. Additionally, this mix of compounds was tested in an in vivo tester. From this in vivo study has emerged that in the group tested with the natural agents mix there was a superior induction of apoptosis of tumor cells and a downregulation of Ki67 compared to the other groups. For these reasons, the weight of the tumor in the in vivo caves was less than the other groups treated with single natural compounds [84].
4.1.2. Resveratrol
Resveratrol (3,4′,5-trihydroxy-trans-stilbene) is another phytochemical agent present in many foods, including peanuts, mulberries, chocolate, and grapes. It possesses various anti-carcinogenesis properties [85] expressed by the enzymes participating in its metabolization. It causes the tumor cells death due to its effect of induced DNA damage in them [86]. The anti-inflammatory properties of resveratrol allow it to modulate the inflammation factors that participate in tumor progression and reduce the risk of cancer development [87,88]. Despite being seen that the administration of resveratrol up to 5 g per day in healthy patients is well-tolerated [89,90] in patients affected by diseases such as diabetes or cancers is difficult to understand the correct dose [91]. In a study conducted by Lin et al. [92], the resveratrol activities against two oral cancer cell lines were analyzed [92]. From other studies, the thyroid hormone axis actively participates in different mechanisms of human cancers [93,94]. In Lin’s study, it has emerged that resveratrol downregulates the thyroid hormones modulating the activities of PD-L1 and BTLA (two checkpoint-co-inhibitor receptors expressed on the surface of the immune system cell that when overexpressed participate in the tumor cells proliferation) [92]. Two more anti-carcinogenic mechanisms of resveratrol were discovered in different studies. Resveratrol inhibits the expression of Rab coupling protein (RCP). RCP is a protein that takes part in the proliferation and invasion of tumor cells. Furthermore, resveratrol indirectly downregulates the expression of EMT (epithelial-mesenchymal transition) reducing the metastasis proliferation in OSCC [95]. As well as for other natural compounds, combining resveratrol with other agents can enhance its anti-carcinogenesis activity. In a study by Ho et al. [96], resveratrol was administrated in association with nano-diamino-tetrac (NDAT) in two oral cancer cell lines. This study has emerged that the combination of these two substances had significantly enhanced the reduction of PD-L1 expression and tumor cell proliferation compared to the group that was treated with resveratrol alone. Moreover, NDAT in the presence of thyroxine has improved the anticarcinogenic activity of resveratrol by inhibiting a cell signaling transduction operated by SATA3 [96]. In an in vitro study on oral tumor cells, the administration of resveratrol and quercetin has been shown to induce oral tumor cell death due to DNA damage, PARP1 modification, and the upregulation of Bax. Additionally, both substances have arrested phase S of the cell’s cycle and cell’s growth allowing the inhibition of tumor cell proliferation [97].
4.1.3. Blackberries
Blackberries are a fruit rich in bioactive agents including phenolic compounds, vitamins, and minerals. Different studies on various tumors have emerged that blackberries possess many anti-carcinogenesis activities [98]. In oral cancer, blackberries have been shown to induce tumor cell apoptosis [99] and modulate the pro-inflammatory factors that contribute to cancer development [99,100]. Furthermore, blackberries can modulate the cell metabolism regulating the expression of genes and metabolites related to the glycolytic pathway [101]. In a study conducted on rats affected by oral epithelial cells, the administration of blackberries showed a reduction in the cell’s DNA damage. In particular, these DNA damages were caused by the dibenzo-[a,l]-pyrene (DBP), a primary metabolite of a carcinogen component of tobacco [102,103]. Many researchers investigated the possible use of blackberries for the treatment of OPMDs. In the study conducted by Shumway et al. [104] 0.5 g of local blackberry gel was administered in patients affected by oral intraepithelial neoplasia. The gel was applied four times per day for a total of 6 months of treatment. After this time, a histological analysis was performed and compared with the initial biopsy. There was a reduction of the oral lesions dimension, an improvement of the histological grade, and a decrease in the initial loss of heterozygosity indices (LOH) [104]. In another study, a gel containing 0,5 g of blackberries was administered to a group of patients affected by oral intraepithelial neoplasia. The control group was treated with a gel with a placebo. The treatment was performed for 12 weeks. At the end of the study, the group tested showed a reduction of the size and an improvement of the histological grade and LOH compared to the control group which showed an increase of the size and no improvement in the histological characteristics [105].
4.2. Carotenoids
Carotenoids are a group of pigments that belong to the tetraterpenes family. The carotenoid compound is drawn from the 13-carotene, the precursor of the vitamin A [106,107]. Carotenoids are present in the organisms that do photosynthesis, and they protect them from the possible damage caused by the sun’s rays. Carotenoids provide the typical yellow, orange, and red colors to fruits and flowers. It is possible to classify carotenoids into provitamin A and non-provitamin A substances [108]. α-carotene, β-carotene, lycopene, β-cryptoxanthin, lutein, and zeaxanthin are the main carotenoid compounds assumed in the dietary [109]. The carotenoid compounds are classified into carotenes (α-carotene, β-carotene, and lycopene) and xanthophylls (β-cryptoxanthin, lutein, and zeaxanthin) based on their chemical structure [110]. These compounds possess anti-inflammatory and antioxidant functions. A large consumption of carotenoids in diet has been shown to reduce the risk of developing cancer [111]. Carotenoids of the provitamin A group perform actions on cell proliferation and differentiation like vitamin A [112] (Table 1).
4.2.1. Beta-Carotene and Vitamin A Derivates
Beta-carotene is the main carotenoid group component. It is present with its red-orange-yellow colors in various fruits and vegetables including tomatoes, carrots, and beans. Beta-carotene possesses antioxidant and anti-carcinogenic properties [113]. Beta-carotene has been shown to reduce the expression of cyclin A allowing the cell cycle arrest. Additionally, it can downregulate the activity of the anti-apoptotic BCL-2 and upregulate the expression of p53 inducing the tumor cells’ apoptosis [114]. In the oral field, different studies were conducted to find the possible use of this compound against premalignant and oral cancers. In a study performed on patients affected by leucoplakia beta-carotene and vitamin C were administered for 1 year. At the end of the study, the authors concluded that the administration of beta-carotene and vitamin C had no effects on the clinical improvement of the leucoplakia lesions [115]. In another study conducted by Buajeed et al. [116], beta-carotene was administered in patients affected by atrophic and erosive oral lichen planus. Beta-carotene was given for 3 months with a dose of 15 mg daily. At the end of the study, the characteristics of the sample of the cells exfoliated have been analyzed. From these analyses, the treatment with beta-carotene reduced the number of the micronucleated exfoliated cells, typical of the lichen planus pathology [116].
Vitamin A is a liposoluble essential vitamin that participates in the epithelium’s normal functioning. Retinoids and carotenoids derive from vitamin A, and they have been shown to possess anti-tumor properties. Retinoids decreased free radicals, induced apoptosis, and downregulated epithelial cell proliferation. Isotretinoin (13-cis-retinoic acid), derived from vitamin A, has shown promising results in the treatment of oral leukoplakia. In a study conducted by Hong et al. [117], isotretinoin was administered at 1–2 mg/kg per day in patients affected by oral leukoplakia. At the end of the study, 67% of the patients tested showed clinical response. The histological analysis has exhibited that isotretinoin had reduced the size and the grade of dysplasia in the oral leukoplakia lesions of the group tested compared to the control group which was administered a placebo. Despite these promising results, the study has shown limitations, which are the toxicity of isotretinoin and the high rate of recurrence after a few months [117]. Further investigations have been conducted to discover the nontoxic isotretinoin dose, but no one has found it [118]. Retinyl palmitate and beta-carotene, other vitamin A derivates, have shown efficacy but less toxicity than isotretinoin [119]. In a study conducted by Papadimitrakopoulou et al. [120] the efficacy of isotretinoin, retinyl palmitate, and beta-carotene in the treatment of OSCC was compared. The study results have shown that all three substances have proved effective in the treatment of OSCC, but isotretinoin possesses a higher clinical response [120]. It was proved that the association of vitamin E reduces isotretinoin toxicity [121].
4.2.2. Lycopene
Lycopene is a carotenoid present in many foods including tomatoes, cranberries, papayas, peaches, grapes, apricots, watermelon, and pink grapefruits [122]. It possesses antioxidant and anticancer properties. Due to these activities, lycopene was tested for treating different oral diseases, including OPMDs and OSCC. Kumar et al. [123] after their study concluded that lycopene should be used in the first-line therapy for the treatment of oral submucous fibrosis. From an in vivo study have emerged that the administration of lycopene in mice affected by oral squamous cancer can induce the apoptosis of the oral tumor cells due to the regulation of BAX (a pro-apoptotic protein) and bcl-2 (an anti-apoptotic protein). Specifically, lycopene administration induced an increase in the ratio of Bax to bcl-2, which resulted in apoptosis of cancer cells. Additionally, lycopene administration has been shown to inhibit the epithelial-mesenchymal transition (EMT) mechanism and the PI3K/AKT/mTOR signaling pathway [124]. These two mechanisms are related to tumorigenesis, cancer progression [125,126,127,128] and metastasis [129,130]. In a study conducted on cultures of cells affected by OSCC the treatment with lycopene showed a decrease of the expression of the insulin-like grow factor 1 (IGF1) and a reduction of the cancer tissue size compared to the control group (treated with a placebo). IGF1 contributes to the carcinogenesis mechanism, allowing tumor cell proliferation. Furthermore, the efficacy of different dosages of lycopene (0.25, 0.5, 1, and 2 µM) was studied. At the end of the study, the results obtained were dose-dependent based on the lycopene quantity [131]. Another study has emerged that lycopene increasing the glutathione redox cycle inhibits tumor progression in cells affected by oral cancer [132]. Additionally, lycopene modulates the expression of connexin-43 (a gap-junction protein) and reduces the killer B1 cells in oral cancer [133]. In a study conducted by Singh et al. [134] lycopene’s efficacy was tested in treating leucoplakia. The tester groups were administered different dosages (8 mg/day, 4 mg/day) of lycopene and a placebo was administered in the control group. At the end of the study, after 3 months, in the two groups tested it were seen a reduction in the size and the hyperkeratosis of the leucoplakia lesions compared to the control group. Despite higher improvement in the clinical results, no statistical differences existed between the group administered 8 mg/day and the group tested with 4 mg/day [134].
4.2.3. Curcumin
Curcumin contained in the rhizome of Turmeric (Curcuma longa) takes part in this class of phytochemical agents. Curcumin possesses different properties including anti-inflammatory, antioxidant, antimicrobial, immunomodulatory, and antitumor. Curcumin inhibits the activity of nuclear factor kappa B (NF-κB). NF-κB is an important factor that participates in the inflammatory process. It is known that the persistence of an inflammatory process participates in the stages of cancer establishment, for instance, tissue hyperplasia [135,136]. In fact, in different cancers, including oral cancer, the persistence of inflammation due to the NF-κB activity was seen [137]. Moreover, from an in vitro experiment curcumin has downregulated the matrix metalloprotease 2 and 9 (MMP-2 and MMP-9) and modulated the expression of E-cadherin and p53 [138]. MMP-2 and MMP-9 are enzymes that participate in extracellular matrix degradation, which is crucial for cancer cell invasion and metastasis [139]. E-cadherin is a cell adhesion molecular. Different studies have found in many cancers that the loss of E-cadherin expression is a marker of tumor invasion and metastasis progression [140,141]. From an in vitro study curcumin can reduce the expression of the two transcription factors (Twist and Snail) that caused the inhibition of E-cadherin expression [138]. P53 is one of the main tumor suppressor proteins, the p53 alteration causes metastasis and invasion progression [142,143]. In a study conducted by Kuttan et al. [144], curcumin was locally administered to 62 patients affected by oral cancers. At the end of the study, 10% of the participants showed a reduction in the dimension of the cancer lesions [144]. Cheng et al. [145] have conducted a study to evaluate the effects of the oral administration of curcumin for 3 months in patients affected by oral leukoplakia. Before and at the end of this period the biopsies of the oral lesions were made. From the histological analysis, there was an improvement in the seven cases treated [145]. In a study conducted by Tuttle et al. [146] the efficacy of curcumin in association with radiotherapy was tested for the treatment of OSCC. From this study, it has emerged that mice affected by OSCC negative to HPV treated with this combination of therapy have shown an increase in the survival rate compared to the other group [146]. The results obtained in Tuttle’s study could be related to the fact that curcumin has been shown to protect the non-tumor cells and tissue from ionic radiation during tumor radiation therapy, and it has induced radiosensitive in the oral squamous carcinoma cells [147,148]. The authors concluded by saying that the association of curcumin with radiotherapy could be used as a first-line therapy for the OSCC treatment [146].
Although the results obtained in the previous study related to the possible use of phytochemical compounds as chemotherapy there are limits. The bioavailability of these substances is one of the main limits because they are distributed in the organism and quickly removed in the liver after their administration. Additionally, natural compounds are difficult to absorb in the stomach; this is another important limit. Then, not all the substance administered arrives in the specific area where it is needed [149,150,151]. To contrast these limits, there is the possibility to use nanoparticles and lipids that can be loaded with natural compounds [149,151,152].

Table 1.
A summary of the different phytochemical compounds with their dietary sources and mechanisms of action.
Table 1.
A summary of the different phytochemical compounds with their dietary sources and mechanisms of action.
| Phytochemical Compound | Substance | Dietary Source | Mechanism of Action | Reference |
|---|---|---|---|---|
| Polyphenolic | Green tea | Regulate the expression of the EGFR, the NF-κB and AP-1 factors, induce tumor cell death | [63,75,77] | |
| Resveratrol | peanuts, mulberries, chocolate, and grapes | Causes tumor cell death, performs an anti-inflammatory activity, downregulates the thyroid hormones modulating PD-L1 and BTLA, inhibits the expression of RCP, indirectly downregulates the expression of EMT | [86,87,88,92,95] | |
| Blackberries | Induce tumor cell apoptosis, decrease inflammatory factors, and modulate the cell’s metabolism | [99,100,101] | ||
| Carotenoids | Beta-carotene | tomato, carrots, and beans | Reduces the expression of cyclin A, downregulates the activity of BCL-2, and upregulates the expression | [114] |
| Vitamin A derivates | decrease free radicals, induce apoptosis, and downregulate the epithelial cells’ proliferation | [117] | ||
| Lycopene | tomato, cranberries, papayas, peaches, grapes, apricots, watermelon, and pink grapefruits | Regulates BAX and bcl-2, inhibits EMT mechanism and the PI3K/AKT/mTOR signaling pathway, decreases the expression of IGF1 | [124,131] | |
| Curcumin | Inhibits NF-κB activity, downregulates MMP-2 and MMP-9, reduces the expression of Twist and Snail, modulates the expression of E-cadherin and p53 | [135,137] | ||
5. Immunomodulatory Agents
Through the improvement of the information about the tumor cell development mechanisms, it has been discovered that tumor cells can escape the immune system control. Normally immune cells bind surface proteins present on the cells and with this mechanism, immune cells can discover the presence of stranger antigens. Although this mechanism protects the organism, at the same time the organism can attack itself. For this reason, proteins that can turn off the immune response are linked to the organism’s cell surface. This mechanism avoids autoimmunity. Tumor cells express on their surface the same proteins to switch off the immune system allowing it to survive and proliferate. Therefore, experts are starting to study and develop new cancer therapy that targets the immune checkpoint receptors. The idea is to create a monoclonal antibody able to bind the immune checkpoints. PD-1 is one of the main immune checkpoints studied. Despite the immune system tumor cell being recognized as a stranger, it produces PD-L1, a protein that binds PD-1 and turns off the immune responses against itself [153] (Figure 4).
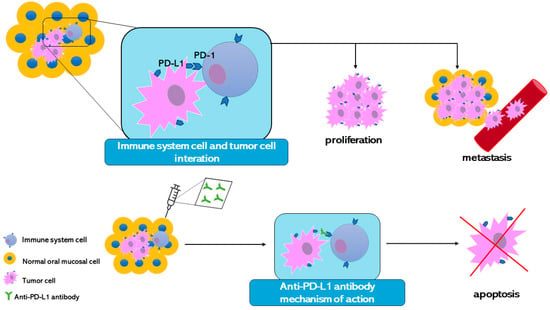
Figure 4.
The illustration represents one mechanism that tumor cells perform to avoid immune system control. The introduction of the monoclonal antibody has allowed the development of an anti-PD-L1 antibody to contrast the tumor cells’ escape mechanism. In this way, the immune system can recognize the tumor cell and induce its apoptosis.
In the oral pathologies and cancer fields, this discovery has permitted the opening of a new type of antitumor therapy. In a study conducted by Wang et al. [154] a monoclonal anti-PD-1 antibody was tested on animals affected by oral leukoplakia. This study has emerged that blocking the interaction of PD-L1 with PD-1 has facilitated T cell activity, inducing the apoptosis of the cell that formed the oral leukoplakia lesion. The histological analysis showed that in the mice treated with the monoclonal antibody, there was a decrease (43.3%) in the grade of dysplasia of the oral leukoplakia lesions compared to the control group. The authors suggested that monoclonal anti-PD-1 could be used for the treatment of the oral precancerous lesions to contrast the malignancy development and to treat OSCC. However, evaluations are necessary before clinical use of this anti-PD-1 antibody. Furthermore, from this study has emerged that another checkpoint should be blocked. In mice treated with anti-PD-1, it was seen an increase in the activity of another checkpoint called CTLA-4. Then, using different monoclonal antibodies against PD-1 and CTLA-4 can enhance the antitumor activity. The blockade combination of these two checkpoints has improved in patients affected by melanoma [155,156,157]. In 2016 the U.S. FDA approved pembrolizumab and nivolumab, two monoclonal anti-PD-1 antibodies. After different trial studies, it was concluded that the use of pembrolizumab and nivolumab increases the survival rate in patients with advanced head and neck cancer who do not respond to platinum-based chemotherapy [158,159]. The possibility to use immunotherapy to treat oral cancer instead of the use of traditional chemotherapy allows the use of drugs with a specific molecular target reducing the side effects connected with the chemotherapy. Even though these are positive characteristics, side effects have occurred also using immunotherapy to inhibit immune checkpoints [160].
6. Topical Formulation
Topical formulation is another chemopreventive strategy against the malignancy development of the OPMDs. This type of administration possesses different advantages including the reduction of toxicity and systemic metabolism, the possibility to use the chemopreventive substances directly in the margins of the oral lesion, and the increase in the local absorption of the chemopreventive substances only in the area where is necessary [161]. Various studies have been conducted to find which agents can contrast the malignancy development of oral precancerous lesions. In particular, the compounds that were most tested are vitamin A derivates (isotretinoin and tretinoin) [162,163,164,165,166,167], bleomycin [168,169,170,171,172], and cyclooxygenase inhibitors [173] (Table 2). There were also natural substances like raspberries that were previously discussed.
6.1. Retinoids
Vitamin A derivatives are the main topical agents that have been studied to treat OPMDs. Retinoids perform their antitumor activities by binding specific receptors that are retinoid receptors (RARs) [174] and activator protein 1 (AP-1) [175,176]. RARs allow retinoids to influence the transcription or not of different genes regulating the growth and proliferation of cell mechanisms [174]. AP-1 regulates various processes, including inflammation, spread, and oncogene function [175,176]. These specific targets allow retinoids to interrupt the tumor cell growth and expansion. In the studies conducted by Piatelli et al. [166] and Tete et al. [163] the action of 0.1% of isotretinoin was tested in patients affected by oral leukoplakia. In Piatelli’s study, 10 patients were enrolled and randomly divided into two groups: the tester group and the control group (treated with a placebo gel). The local gel administration was performed for 4 months. At the end of the study, the group tested saw a clinical improvement in the oral lesion compared to the control group in which there was no variation [166]. Similar results were obtained in Tete’s study in which 15 patients were enrolled and randomly divided into two groups the tester and the control. The tester group was treated for 4 months with 3 daily local administrations of a gel composed of 0.1% isotretinoin. The outcomes of the study showed 3 complete remissions and 11 enhancements of the clinical lesions greater than or equal to 50% [163]. In another study by Scardina et al. [167] the efficacy of a gel of 0.18% isotretinoin was tested for the treatment of oral leukoplakia lesions. 40 patients were enrolled and divided into two groups: group A treated with a gel of 0.18% of isotretinoin and Group B treated with a gel of 0.05% of isotretinoin. The gels were applied two times per day for 3 months. At the end of the study in the group treated with the higher concentration of isotretinoin, there was a total regression of 85% of oral lesions [167]. Even though the use of isotretinoin has been shown to improve the clinical aspect of oral leukoplakia lesion, some patients have suffered side effects including erythema, xerostomia [167], burning tongue, dry lips, and mucositis [162,163,164,165]. As demonstrated by these previous studies the local administration of retinoids has shown efficacy in the treatment of the oral leukoplakia lesions. Despite these positive effects, some common side effects are present and for these reasons, further studies are necessary for a better understanding of the well-tolerated dose.
6.2. Bleomycin
Bleomycin is another agent that was tested for premalignant oral lesions therapy. Bleomycin is an antibiotic that has been shown to possess antitumor effects [177]. It was seen that bleomycin can suppress the DNA replication binding DNA synthesis enzyme [178]. Bleomycin was used to treat different cancers including head and neck cancers, lymphoma, and testicular tumor [179,180]. The systemic administration of these antitumor agents has shown toxicity, in particular for skin and lungs. For this reason, bleomycin started to be used with another type of administration, the iontophoretic [181]. In the study conducted by Hammersley et al. [170] the efficacy of the local administration of bleomycin for 15 days was tested. The study was conducted on 6 patients who at the end of the experiments, showed a reduction of the dysplasia and keratinization in the cells of the clinical oral lesions [170]. Similar results were obtained in a study in which bleomycin was applied for 3 months [171]. Wong et al. [172] used different concentrations of topical bleomycin for the oral leukoplakia lesion treatment. The study was conducted on 12 patients divided into two groups: one group was treated with 0.5% bleomycin and the second group was treated with 1.0% bleomycin. The study results have shown that clinical enhancement is dose-dependent to the bleomycin concentration. Moreover, two of the six patients treated with bleomycin at 1.0% concentration showed total remission at the end of the study. The authors concluded that increasing the topical administration over a long time could allow the total remission [172]. Similar results have been obtained in two long prospective studies conducted by Epstain et al. [168,169]. The local administration of 1% of bleomycin has reduced the grade of dysplasia allowing the regression of the oral leukoplakia lesions [168,169]. All the authors of the previous studies have underlined the importance of regular follow-up in patients affected by oral leukoplakia that is under treatment because some patients have shown the presence of carcinoma in situ despite the treatments.
6.3. Cyclooxygenase Inhibitors
The cyclooxygenase (COX) inhibitors are the other group of agents that have been studied as a chemopreventive strategy against the malignancy development of precancerous lesions and OSCC. This category of drugs is normally used in cases of inflammation because they are a nonsteroidal anti-inflammatory drug. The idea to use COX inhibitors as antitumor drugs in the oral field was born when Panjie et al. [182] reported that with this drug, there were clinical effects on patients affected by head and neck tumors [182]. Additionally, in other studies, it has been seen that the administration of this category of drug in patients affected by lung, colon, esophageal, and breast tumors could reduce the tumor risk [183,184,185]. Two types of COX are expressed in the human body: COX-1 and COX-2. COX-1 is generally expressed for the human body’s physiological mechanism, while COX-2 is expressed in the case of inflammation and proliferation due to incentives. The COX-2 activity determines the increase of prostanoid production, and this overexpression takes part in the carcinogenesis mechanisms [186]. These mechanisms form the basis of the multi-phases of the OSCC development. The use of celecoxib, a COX inhibitor, has allowed the COX-2 and prostanoid levels reduction in patients affected by oral premalignant lesions [187]. In the study conducted by Mulshine et al. [173] the efficacy of a mouth rise composed of 0.1%/10 mL of ketorolac was tested in patients with oral leukoplakia. The study was conducted on 57 patients randomly divided into two groups: one group was treated with an oral rinse with ketorolac and the other group with an oral rinse with a placebo. The oral rinses were administered two times in 3 months. At the end of the study, the clinical size of the oral lesions and the histological analysis were analyzed and compared with the time 0 (before the experiment). The results obtained showed that there were no differences between the two groups. The authors concluded that using this oral rinse with a COX inhibitor was inefficient in the oral leukoplakia treatment [173]. Similar results and conclusions have been obtained in the study achieved by Papadimitrakopoulou et al. [188]. The previous results are probably related to the two main limits of the COX inhibitors: low absorption and bioavailability. Additionally, from other studies, it was seen that the prolonged use of COX-2 inhibitors can cause cardiotoxicity [189] and gastrointestinal problems [190] To contrast these limits researchers have studied the possibility of using nanoparticles as vehicles of COX inhibitors [191,192]. The nanoparticle system allows to carrying of the drug to the target site reducing the side effects of the systemic administration and increasing the local concentration. For these reasons, future studies are needed to test the use of nanoparticles as vehicles for COX inhibitors in the treatment of precancerous and cancerous lesions of the oral cavity.
6.4. Photodynamic Therapy
Photodynamic therapy is another chemopreventive strategy against oral cancer and precancerous oral lesions. This therapy is based on the sensitivity of particular substances (photosensitizers) to a specific range of light. The interaction of these two substances caused oxygen reactions, creating reactive oxygen species (ROS) in the tissue exposed. The possibility of administering the photosensitizer and irradiating small areas of tissue reduces the side effects and increases the bioavailability and efficacy [193]. The ROS produced during the irradiation of the tissue performs antitumor activities, killing tumor cells, damaging the cancer’s vascular tissue, and stimulating the immune system against the tumor [194]. In the tissue that had to be treated, the inactivated photosensitizer is administered topically or with an injection. 5-Aminolevulinic acid (ALA) is the most used inactivated photosensitizer [195,196]. Different clinics have tried to study photodynamic therapy’s use in treating oral precancerous lesions. In a study conducted by Lin et al. [197] the efficacy of the photodynamic therapy was tested to treat oral erythroleukoplakia and oral verrucous hyperplasia. The study was conducted on 40 patients diagnosed with oral erythroleukoplakia and 40 patients diagnosed with oral verrucous hyperplasia. The ALA was administered with a local gel solution at 20% with a composition able to resist saliva dilution. The administration of ALA and the photo irradiation with a diode laser were applied once a week for all the patients. The clinical resolution of the oral lesions was seen after around three treatment sessions. The authors concluded that this therapeutic strategy is the greatest option for the treatment of oral precancerous lesions [197]. Similar results were obtained in the study performed by Yu et al. [198], in which the efficacy of the photodynamic therapy was analyzed for the treatment of oral verrucous hyperplasia. In the study, 36 patients diagnosed with oral verrucous hyperplasia were enrolled. The ALA gel preparation was administered in all patients, and after one hour and a half, the oral lesions were irradiated with a red light using an LED. This protocol was performed once a week up to the resolution of the lesions. From the study results, the patients enrolled have shown a regression of the oral lesions after fewer than seven appointments. The authors underline that the period of treatment is based on the size, the range of the oral lesion color, and the thickness of the keratin surface [198].
6.5. P53 Inhibitor
In about 50% of the patients affected by head and neck cancers, there is an alteration of the p53 gene that caused its inactivity. P53 performs a crucial role in the correct functioning of the cell, and it is called “the guardian of the genome” [199,200,201]. The modification of the p53 determines the beginning of the primary stage of carcinogenesis. The p53 inactivity caused the uncontrolled proliferation of cells with low differentiation [202]. As a result of this discovery, academics have begun to search for an antitumor substance that targets the mutant p53. This category of drug was developed to arrest tumor proliferation. This category of drug performed different mechanisms of action that are: delivering the wild type of the p53 gene into the tumor cell using an adenovirus, inducing the apoptosis in the tumor cell with p53 mutated using an adenovirus, and correcting the mutated p53 through the delivering of small particles. These are the p53 inhibitor mechanisms of action used in oncology therapy to reduce the lack of responses of resistance tumors and recurrence to traditional therapy [203]. In the chemopreventive field, it was seen that using the p53 inhibitors associated with traditional chemopreventive strategies there was an enhancement of their efficacy [204]. From different studies, the attenuated adenovirus named ONYX-015 was able to cause the death of the cells with mutant p53 [204,205,206]. This attenuated adenovirus does not have the specific protein that allows it to replicate itself in human cells. In this way, this adenovirus has to target the cell with p53 inactivated in which it can replicate itself causing the death of the tumor cell. In normal cells the absence of the specific protein and the normal activity of p53 cause the impossibility of replicating the altered adenovirus [204]. Based on these discoveries, an oral rinse composed of ONYX-015 was tested in the study conducted by Rudi et al. [207]. The study was conducted on 22 patients affected by oral leukoplakia and erythroplakia divided into three groups. In the first group, the oral rinse was administered once a day for 5 days to repeat every month for a maximum of 12 cycles. In the second group, the oral rinse was administered once a week for 6 months. In the third group, the oral rinse was administered daily for 5 days and after these days weekly for more than 1 month. The histological results have shown that 37% of the patients treated had the dysplasia resolution. Despite these results the long-term efficacy there was not seen [207]. Similar conclusions have emerged from the study of Li et al. [208] in which the attenuated adenovirus was administered with local infiltrations [208]. The p53 mutation, present in the oral tumor cell, can be a specific target to induce apoptosis, arresting tumor proliferation.
Table 2.
This table summarizes the different types of chemopreventive topic agents and their mechanisms of action against the altered cells.
Table 2.
This table summarizes the different types of chemopreventive topic agents and their mechanisms of action against the altered cells.
| Substance | Mechanism of Action | Reference |
|---|---|---|
| Retinoids | Bind RARs and AP-1 regulating the expression of genes related to cell growth and proliferation | [174,175,176] |
| Bleomycin | Suppress the DNA replication binding DNA synthesis enzyme | [178] |
| Cyclooxygenase inhibitors | Permitted the reduction of the production of COX-2 and prostanoids leading to the reduction of the inflammatory state | [187] |
| Photodynamic therapy | The local administration of a photosensitizer (ALA) after its activation with light causes the production of ROS that provokes tumor cell death | [193,194] |
| P53 inhibitor (ONYX-015) | Bind the altered p53 gene, causing tumor cell death | [204,205,206] |
7. EGFR Inhibitor
Epidermal growth factor receptor (EGFR) is important for the physiological proliferation of epithelial cells. In many cancers, including head and neck cancers, there is an alteration of the EGFR expression that causes an increase in cell proliferation and the resistance to apoptosis, allowing invasion and metastasis processes [209]. For this reason, various studies have been conducted to find a target drug able to inhibit EGFR. A monoclonal antibody called cetuximab was developed to inhibit the EGFR activity. It was authorized by the U.S. FDA in 2006. Cetuximab has been shown to prevent epithelial cell proliferation [210,211,212,213,214]. Additionally, it was studied that the overexpression of EGFR in oral cell cancers is related to less radiation sensitivity [215]. The administration of cetuximab and radiotherapy has shown higher efficacy in preventing the proliferation of oral tumor cells. This is related to the fact that cetuximab can increase the radiosensitivity of the tumor cells [210,211,212]. Therefore, the administration of cetuximab associated with the radiotherapy treatment has increased the survival rate at 5 years compared to the survival rate at 5 years after the use of radiotherapy alone (45.6% vs. 36.4%) [214]. Different studies have underlined the efficacy of cetuximab for the treatment of OSCC in association or not with radiotherapy. Despite that, cetuximab is administered intravenously and its extended use must be limited [216] and targeted for secondary chemoprevention. In a study conducted by Ohnishi et al. [217] it was discovered that long use of cetuximab can cause a loss of efficacy in treating precancerous and cancerous oral lesions. Further studies are necessary to be performed for a better knowledge of the efficacy of cetuximab over the long period of its administration.
The alteration of EGFR is also present in the precancerous lesions and the normal tissues [218]. In the study conducted by William et al. [216] the efficacy of erlotinib was investigated in the treatment of oral leukoplakia [216]. Erlotinib is a tyrosine kinase inhibitor able to bind EGFR suppressing its activity [219]. In the trial made by William et al. [216] 379 patients affected by oral lesions with a high malignancy diagnosis were enrolled and divided into two groups. Patients of the first group were treated with 150 mg of erlotinib and patients of the second group were treated with a placebo for 12 months. At the end of the study, no statistically significant change in the survival rate was seen between the group treated with erlotinib and the placebo group. From the results obtained, the authors concluded that in the long period, erlotinib had no efficacy in treating oral leukoplakia lesions with a high risk of malignancy evolution. However, William’s study has underlined the importance of EGFR in the diagnosis and prognosis of precancerous lesions [216]. Even though erlotinib reduces the activity of EGFR overexpress, the administration of this drug has caused different side effects. The development of rash is the main side effect. This is because the EGFR inhibitor settles in the lesion in which there is a high expression of EGFR. This side effect of erlotinib is the only reason researchers are discouraged from increasing its dosage [220,221]. Different studies conducted on animals and in vitro showed that the combination of erlotinib and celecoxib could contrast the OSCC tumor progression [222,223,224]. Consequently, Saba et al. [225] have performed a study in which the efficacy of the combination of celecoxib and erlotinib was investigated in the treatment of advanced precancerous lesions. For the study, 36 patients with different grades of oral leukoplakia or with carcinoma in situ were enrolled. Patients have received 400 mg of celecoxib and three different doses of erlotinib 50 mg, 75 mg, and 100 mg, during the 6 months of treatment. At the end of the study, the histological analysis showed a decrease in EGFR expression. Despite this promising result, different patients have exhibited the main side effect related to the use of erlotinib which is rash [225]. Due to the applicant rash in patients and the few studies conducted, further research is necessary to better understand the use of EGFR inhibitors as chemopreventive agents against OSCC and OPMDs.
8. Metformin
As mentioned previously in this article glycolysis is fundamental for the beginning and maintenance of the tumor cells’ activities. Given that, various investigations have been conducted to understand if the use of anti-diabetic drugs has efficacy in the OSCC and in the OPMDs chemoprevention. Metformin is the most common anti-diabetic drug used in the world for the treatment of type 2 diabetes. Some studies have discovered that diabetic patients who assumed metformin for diabetic therapy have shown a lower risk of developing cancer [226,227,228]. This discovery is related to the fact that metformin can control the functioning of the mTORC1 pathway [229]. Additional studies have shown how the mTORC1 pathway actively contributes to developing head and neck cancers and precancerous oral lesions [230,231,232]. Metformin causes tumor cell apoptosis suppressing the mTORC1 pathway [233,234,235,236,237]. Moreover, metformin has another antitumor activity that is performed by the activation of liver kinase B1 (LKB1)–5′ AMP-activated protein kinase (AMPK), a different cell’s pathway [238,239,240]. The possibility of using metformin as a chemopreventive agent is also validated by one investigation in which the diabetic patients affected by OSCC that assumed metformin showed the lowest risk of recurrences and metastasis with a better prognosis [241]. It is also well known that the use of metformin has a very low toxicity for humans [242]. In the study conducted by El-Zalabany et al. [243] the efficacy of metformin as a chemopreventive agent was investigated for treating OPMDs. For the study, 40 patients affected by leukoplakia and lichen planus without diabetes were enrolled. The patients were divided into the tester group, which administered 500 mg of metformin hydrochloride once a day, and the control group treated with a placebo. At the end of 3 months, the group tested showed a reduction of the oral lesions size and the grade of epithelium dysplasia compared to the control group in which the lesions were bigger than in the beginning. From the historical analysis has also emerged that metformin has allowed the decrease of Cyclin-A2 (a regulator of cell proliferation), miRNA-31, and miRNA 210 concentrations (tumor cancer biomarkers). Based on the results obtained, the authors of this investigation suggested the use of metformin to prevent the malignant evolution of OPMDs [243]. In another study, metformin was administered in patients affected by leukoplakia or erythroplakia for 3 months. Metformin was assumed by patients with different dosages in the three months of therapy: first month 500 mg, second mouth 1000 mg, and the last month 2000 mg. From the results obtained, it has emerged that 60% of the patients treated have shown clinical responses. The histological analysis indicated that metformin has performed antitumor activity, causing a statistically significant reduction in the proliferation of dysplasia cells [244]. A combination of different substances is possible to be used as a chemopreventive strategy. In the study conducted by Siddappa et al. [245] the efficacy of the use of metformin and curcumin was tested for the treatment of ODPMs. The study was conducted on mice affected by OSCC divided into two groups. The tester group received 5 mL of water daily which contained curcumin at 14.3 µg/mL and metformin at 5 mg/mL, while the control group received water with a placebo. At the end of the study, the group treated with the combination of curcumin and metformin showed a decrease in the oral lesions size compared to the control group. Additionally, the treatment has enhanced the animals’ survival rate [245]. For the promising results obtained in these and other studies, researchers underline the potential that metformin can be performed as a chemopreventive agent in the treatment of OSCC and OPMDs.
9. Vitamin E
Vitamin E is a vitamin that performs antioxidant activities. It is present in different common foods including margarine and plant oils. Alpha-tocopherol is the main ingredient of vitamin E. Vitamin E has been proposed as a chemopreventive agent due to the antitumor activity performed as an antioxidant compound. In the study conducted by Benner et al. [246] the efficacy and the limit of vitamin E were investigated in the oral leukoplakia lesions treatment. For the study, 34 patients were enrolled and were treated with two daily administration of 400 IU of vitamin E for 6 months. At the end of the study, 46% of the patients showed clinical improvement and 21% showed histological enhancement [246]. In another study, the efficacy of a mix of different antioxidant supplements that were beta-carotene, ascorbic acid, and alpha-tocopherol was investigated for the oral leukoplakia treatment. The study was conducted for 9 months and after that 55% of patients saw clinical improvement. Additionally, even in patients who did not have reduced risk factors like tobacco and alcohol clinical improvement was noted [247]. The daily limit dosage of vitamin E for men and women was discovered to be 8 mg and 10 mg. A higher dose has been shown to cause a problem, increasing the mortality risk, and this has to be prevented [248]. Due to the few studies, further investigations must be conducted for a better understanding of the efficacy of vitamin E as a chemopreventive agent.
10. Chemopreventive Agents Loaded on Nanoparticles
In the last years, the introduction of nanoparticles has increased researchers’ interest in different medical fields. Nanoparticles can lead to chemical substances bringing them into a target area. They also allow for to reduction of the common side effects typically of the systemic administration of drugs. Due to the numerous advantages that nanoparticles possess; researchers have begun testing their use with chemotherapeutic substances. Following are some examples of studies conducted about chemopreventive agents and delivery systems. In the study conducted by Maller et al. [105] it was formulated and tested a mucoadhesive berry gels. The absorption and penetration capacity of the substances within the oral tissues was analyzed. From the analyses conducted in this study, the authors concluded that their mucoadhesive gel formulation was well adapted for oral mucosa penetration and absorption [105]. Chang et al. [249] have created a delivery system to reduce the low solubility of curcumin composed of PLGA nanoparticles loaded with curcumin. This nano delivery system was tested on an in vitro culture of oral tumor cells cisplatin resistant. From the study have emerged that nanoparticles allow curcumin to penetrate more easily into the cells increasing its concentration. Moreover, the nanoparticle with curcumin injected into oral tumor cells has been shown to stimulate apoptosis activating the caspase cascade mechanism [249]. Similar results were obtained in the study of Mazzarino et al. [250] in which curcumin was loaded with chitosan. From this study, it was seen that chitosan had permitted an increase of the curcumin penetration into the culture of oral tumor cells. These had determined the reduction of the oral tumor cells viability and the apoptosis [250] These studies show some of the advantages that nanoparticle systems can bring when combined with traditional chemopreventive agents. Further studies concerning the use of nanoparticles with various chemopreventive agents on a larger population are needed to verify the efficacy of their use in the treatment of preneoplastic and neoplastic lesions of the oral cavity.
11. Conclusions
Although the primary prevention, the prevalence and the incidence of OPMDs and OSCC are high. Given the necessity to develop new strategies, chemoprevention was born to halt OPMDs’s malignant transformation and oral cancer progression. The studies conducted until today have been performed on a small sample of the population, and many of them have only been conducted on cell cultures or animals. Moreover, the partial efficacy and possible side effects are other limits of the compounds investigated. For these reasons, future investigations should be analyzed and tested in a wide population to introduce them in clinical practice.
Author Contributions
Conceptualization, G.I.; methodology, G.V. and A.P.; validation, C.G., R.L. and S.C.; formal analysis, G.V. and A.P.; investigation, C.G. and S.C.; writing—original draft preparation, G.V. and A.P.; writing—review and editing, R.L. and G.I.; supervision, R.L. and G.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available from corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rhodus, N.L.; Kerr, A.R.; Patel, K. Oral cancer: Leukoplakia, premalignancy, and squamous cell carcinoma. Dent. Clin. 2014, 58, 315–340. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Shan, Z.; Liu, Z.; Liu, S.; Yang, L.; Fang, X.; Li, K.; Wang, B.; Deng, Z.; Hu, Y. The repertoire of tumor-infiltrating lymphocytes within the microenvironment of oral squamous cell carcinoma reveals immune dysfunction. Cancer Immunol. Immunother. 2020, 69, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Mascitti, M.; Orsini, G.; Tosco, V.; Monterubbianesi, R.; Balercia, A.; Putignano, A.; Procaccini, M.; Santarelli, A. An overview on current non-invasive diagnostic devices in oral oncology. Front. Physiol. 2018, 9, 1510. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, P.; Singh, A.; Chien, C.-Y.; Warnakulasuriya, S. Tobacco related oral cancer. BMJ 2019, 365, l2142. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S. Clinical features and presentation of oral potentially malignant disorders. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 582–590. [Google Scholar] [CrossRef]
- Kumar, A.; Sarode, S.C.; Sarode, G.S.; Majumdar, B.; Patil, S.; Sharma, N.K. Beyond gene dictation in oral squamous cell carcinoma progression and its therapeutic implications. Transl. Res. Oral Oncol. 2017, 2, 2057178X17701463. [Google Scholar] [CrossRef]
- Mehanna, H.M.; Rattay, T.; Smith, J.; McConkey, C.C. Treatment and follow-up of oral dysplasia—A systematic review and meta-analysis. Head Neck J. Sci. Spec. Head Neck 2009, 31, 1600–1609. [Google Scholar] [CrossRef]
- Andrews, N.; Griffiths, C. Dental complications of head and neck radiotherapy: Part 2. Aust. Dent. J. 2001, 46, 174–182. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Brewer, I.; Leonardi, R.; Roberts, N.; Bagnato, G. Pain threshold and temporomandibular function in systemic sclerosis: Comparison with psoriatic arthritis. Clin. Rheumatol. 2018, 37, 1861–1867. [Google Scholar] [CrossRef]
- Priebe, S.; Aleksejūnienė, J.; Zed, C.; Dharamsi, S.; Thinh, D.; Hong, N.; Cuc, T.; Thao, N. Oral squamous cell carcinoma and cultural oral risk habits in Vietnam. Int. J. Dent. Hyg. 2010, 8, 159–168. [Google Scholar] [CrossRef]
- Gupta, P.; Murti, P.; Bhonsle, R.; Mehta, F.; Pindborg, J. Effect of cessation of tobacco use on the incidence of oral mucosal lesions in a 10–yr follow-up study of 12,212 users. Oral Dis. 1995, 1, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Steward, W.P.; Brown, K. Cancer chemoprevention: A rapidly evolving field. Br. J. Cancer 2013, 109, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Caccianiga, G.; Crimi, S.; Cavallini, C.; Leonardi, R. Frequency and type of ponticulus posticus in a longitudinal sample of nonorthodontically treated patients: Relationship with gender, age, skeletal maturity, and skeletal malocclusion. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Hema, K.; Smitha, T.; Sheethal, H.; Mirnalini, S.A. Epigenetics in oral squamous cell carcinoma. J. Oral Maxillofac. Pathol. JOMFP 2017, 21, 252. [Google Scholar] [CrossRef]
- Sivapathasundharam, B.; Rajendran, A. Shafer’s Textbook of Oral Pathology; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Montero, P.H.; Patel, S.G. Cancer of the oral cavity. Surg. Oncol. Clin. 2015, 24, 491–508. [Google Scholar] [CrossRef]
- Pires, F.R.; Ramos, A.B.; Oliveira, J.B.C.D.; Tavares, A.S.; Luz, P.S.R.D.; Santos, T.C.R.B.D. Oral squamous cell carcinoma: Clinicopathological features from 346 cases from a single oral pathology service during an 8-year period. J. Appl. Oral Sci. 2013, 21, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, A.; Kerns, T.J.; Sorkin, J.D.; Dwyer, D.M.; Groves, C.; Steinberger, E.K. Self-reported oral cancer screening by smoking status in Maryland: Trends over time. J. Public Health Dent. 2013, 73, 261–270. [Google Scholar] [CrossRef]
- Agaku, I.; King, B.; Husten, C.; Bunnell, R.; Ambrose, B.; Hu, S.; Holder-Hayes, E.; Day, H. Centers for Disease Control and Prevention (CDC) Tobacco product use among adults—United States, 2012–2013. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 542–547. [Google Scholar]
- Conney, A.H. Induction of microsomal enzymes by foreign chemicals and carcinogenesis by polycyclic aromatic hydrocarbons: GHA Clowes Memorial Lecture. Cancer Res. 1982, 42, 4875–4917. [Google Scholar]
- Rengarajan, T.; Rajendran, P.; Nandakumar, N.; Lokeshkumar, B.; Rajendran, P.; Nishigaki, I. Exposure to polycyclic aromatic hydrocarbons with special focus on cancer. Asian Pac. J. Trop. Biomed. 2015, 5, 182–189. [Google Scholar] [CrossRef]
- Rivera, C. Essentials of oral cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884. [Google Scholar] [PubMed]
- Reidy, J.T.; McHugh, E.E.; Stassen, L. A review of the role of alcohol in the pathogenesis of oral cancer and the link between alcohol-containing mouthrinses and oral cancer. J. Ir. Dent. Assoc. 2011, 57, 200–202. [Google Scholar] [PubMed]
- Reidy, J.; McHugh, E.; Stassen, L. A review of the relationship between alcohol and oral cancer. Surgeon 2011, 9, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Ogden, G. Alcohol and mouth cancer. Br. Dent. J. 2018, 225, 880–883. [Google Scholar] [CrossRef] [PubMed]
- Pulte, D.; Brenner, H. Changes in survival in head and neck cancers in the late 20th and early 21st century: A period analysis. Oncologist 2010, 15, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J. Clin. Oncol. 2011, 29, 4294. [Google Scholar] [CrossRef] [PubMed]
- Dalianis, T. Human papillomavirus and oropharyngeal cancer, the epidemics, and significance of additional clinical biomarkers for prediction of response to therapy. Int. J. Oncol. 2014, 44, 1799–1805. [Google Scholar] [CrossRef] [PubMed]
- Hallikeri, K.; Burde, K.; Anehosur, V.; Kulkarni, B.B.; Hiremath, S.V. p53 polymorphism and association of human papillomavirus in oral submucous fibrosis and oral squamous cell carcinoma: A case–control study. J. Oral Maxillofac. Pathol. JOMFP 2019, 23, 97. [Google Scholar] [CrossRef]
- Dai, M.; Clifford, G.M.; le Calvez, F.; Castellsagué, X.; Snijders, P.J.; Pawlita, M.; Herrero, R.; Hainaut, P.; Franceschi, S.; IARC Multicenter Oral Cancer Study Group. Human papillomavirus type 16 and TP53 mutation in oral cancer: Matched analysis of the IARC multicenter study. Cancer Res. 2004, 64, 468–471. [Google Scholar] [CrossRef]
- Pflipsen, M.; Zenchenko, Y. Nutrition for oral health and oral manifestations of poor nutrition and unhealthy habits. Gen. Dent. 2017, 65, 36–43. [Google Scholar]
- Grimm, M.; Cetindis, M.; Biegner, T.; Lehman, M.; Munz, A.; Teriete, P.; Reinert, S. Serum vitamin D levels of patients with oral squamous cell carcinoma (OSCC) and expression of vitamin D receptor in oral precancerous lesions and OSCC. Med. Oral Patol. Oral Y Cir. Bucal 2015, 20, e188. [Google Scholar] [CrossRef] [PubMed]
- Chi, A.C.; Day, T.A.; Neville, B.W. Oral cavity and oropharyngeal squamous cell carcinoma—An update. CA Cancer J. Clin. 2015, 65, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.; Gueiros, L.A.; Leão, J.C.; Fedele, S. Risk factors and etiopathogenesis of potentially premalignant oral epithelial lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 603–611. [Google Scholar] [CrossRef]
- Agrawal, A.; Shindell, E.; Jordan, F.; Baeva, L.; Pfefer, J.; Godar, D.E. UV radiation increases carcinogenic risks for oral tissues compared to skin. Photochem. Photobiol. 2013, 89, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Srinivasprasad, V.; Dineshshankar, J.; Sathiyajeeva, J.; Karthikeyan, M.; Sunitha, J.; Ragunathan, R. Liaison between micro-organisms and oral cancer. J. Pharm. Bioallied Sci. 2015, 7, S354. [Google Scholar] [CrossRef] [PubMed]
- Reibel, J.; Gale, N.; Hille, J.; Hunt, J.; Lingen, M.; Muller, S.; Sloan, P.; Tilakaratne, W.; Westra, W.; Willams, M. Oral potentially malignant disorders and oral epithelial dysplasia. In WHO Classification of Head and Neck Tumours; World Health Organization: Geneva, Switzerland, 2017; pp. 112–115. [Google Scholar]
- Johnson, N.W. Cancer biology and carcinogenesis: Fundamental biological processes and how they are deranged in oral cancer. In Textbook of Oral Cancer: Prevention, Diagnosis and Management; Springer: Cham, Switzerland, 2020; pp. 399–425. [Google Scholar]
- Johnson, N.W. Introduction—The Biology and Pathology of Squamous Cell Carcinomata in the Head and Neck. In Squamous Cell Carcinoma: Molecular Therapeutic Targets; Springer: Dordrecht, The Netherlands, 2017; pp. 1–35. [Google Scholar]
- Khan, Z. Survivin as a therapeutic target in squamous cell carcinoma. In Squamous Cell Carcinoma: Molecular Therapeutic Targets; Springer: Dordrecht, The Netherlands, 2017; pp. 183–203. [Google Scholar]
- Warnakulasuriya, S. Oral potentially malignant disorders: A comprehensive review on clinical aspects and management. Oral Oncol. 2020, 102, 104550. [Google Scholar] [CrossRef]
- Nikitakis, N.G.; Pentenero, M.; Georgaki, M.; Poh, C.F.; Peterson, D.E.; Edwards, P.; Lingen, M.; Sauk, J.J. Molecular markers associated with development and progression of potentially premalignant oral epithelial lesions: Current knowledge and future implications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 650–669. [Google Scholar] [CrossRef]
- Angjelova, A.; Jovanova, E.; Polizzi, A.; Santonocito, S.; Lo Giudice, A.; Isola, G. The Potential of Nano-Based Photodynamic Treatment as a Therapy against Oral Leukoplakia: A Narrative Review. J. Clin. Med. 2023, 12, 6819. [Google Scholar] [CrossRef]
- Polizzi, A.; Santonocito, S.; Distefano, A.; De Pasquale, R.; Alibrandi, A.; Alanazi, A.M.; Li Volti, G.; Isola, G. Analysis of oral lichen planus severity on micro-RNA linked with malignant transformation risks. Oral Dis. 2023. [Google Scholar] [CrossRef]
- Polizzi, A.; Santonocito, S.; Lo Giudice, A.; Alibrandi, A.; De Pasquale, R.; Isola, G. Analysis of the response to two pharmacological protocols in patients with oral lichen planus: A randomized clinical trial. Oral Dis. 2023, 29, 755–763. [Google Scholar] [CrossRef]
- Nadeau, C.; Kerr, A.R. Evaluation and management of oral potentially malignant disorders. Dent. Clin. 2018, 62, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Speight, P.M.; Khurram, S.A.; Kujan, O. Oral potentially malignant disorders: Risk of progression to malignancy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 612–627. [Google Scholar] [CrossRef] [PubMed]
- Reichart, P. S2. 4 Erythroplakia—Clinical markers. Oral Oncol. Suppl. 2005, 1, 47. [Google Scholar] [CrossRef]
- Villa, A.; Villa, C.; Abati, S. Oral cancer and oral erythroplakia: An update and implication for clinicians. Aust. Dent. J. 2011, 56, 253–256. [Google Scholar] [CrossRef]
- Scully, C.; Beyli, M.; Ferreiro, M.C.; Ficarra, G.; Gill, Y.; Griffiths, M.; Holmstrup, P.; Mutlu, S.; Porter, S.; Wray, D. Update on oral lichen planus: Etiopathogenesis and management. Crit. Rev. Oral Biol. Med. 1998, 9, 86–122. [Google Scholar] [CrossRef] [PubMed]
- Carrozzo, M.; Porter, S.; Mercadante, V.; Fedele, S. Oral lichen planus: A disease or a spectrum of tissue reactions? Types, causes, diagnostic algorhythms, prognosis, management strategies. Periodontology 2000 2019, 80, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Yao, Z.; Liu, G.; Cui, L.; Li, H.; Huang, J. Oral submucous fibrosis: A clinicopathological study of 674 cases in China. J. Oral Pathol. Med. 2019, 48, 321–325. [Google Scholar] [CrossRef]
- Sporn, M.B. Approaches to prevention of epithelial cancer during the preneoplastic period. Cancer Res. 1976, 36, 2699–2702. [Google Scholar]
- Bodhade, A.S.; Dive, A.M. Chemoprevention of premalignant and malignant lesions of oral cavity: Recent trends. Eur. J. Dent. 2013, 7, 246–250. [Google Scholar] [CrossRef]
- Garewal, H.; Meyskens, F.; Friedman, S.; Alberts, D.; Ramsey, L. Oral cancer prevention: The case for carotenoids and anti-oxidant nutrients. Prev. Med. 1993, 22, 701–711. [Google Scholar] [CrossRef][Green Version]
- Holpuch, A.S.; Desai, K.-G.H.; Schwendeman, S.P.; Mallery, S.R. Optimizing therapeutic efficacy of chemopreventive agents: A critical review of delivery strategies in oral cancer chemoprevention clinical trials. J. Carcinog. 2011, 10, 23. [Google Scholar] [PubMed]
- Foy, J.-P.; Bertolus, C.; William, W.N.; Saintigny, P. Oral premalignancy: The roles of early detection and chemoprevention. Otolaryngol. Clin. N. Am. 2013, 46, 579–597. [Google Scholar] [CrossRef] [PubMed]
- Gopal, K. Chemopreventive agents in head and neck cancer. Int. J. Curr. Res. 2017, 9, 47228–47234. [Google Scholar]
- Rajamanickam, S.; Agarwal, R. Natural products and colon cancer: Current status and future prospects. Drug Dev. Res. 2008, 69, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Chau, L.; Jabara, J.T.; Lai, W.; Svider, P.F.; Warner, B.M.; Lin, H.-S.; Raza, S.N.; Fribley, A.M. Topical agents for oral cancer chemoprevention: A systematic review of the literature. Oral Oncol. 2017, 67, 153–159. [Google Scholar] [CrossRef]
- Zhou, Y.; Zheng, J.; Li, Y.; Xu, D.-P.; Li, S.; Chen, Y.-M.; Li, H.-B. Natural polyphenols for prevention and treatment of cancer. Nutrients 2016, 8, 515. [Google Scholar] [CrossRef]
- Farrand, L.; Oh, S.-W.; Song, Y.S.; Tsang, B.K. Phytochemicals: A multitargeted approach to gynecologic cancer therapy. BioMed Res. Int. 2014, 2014, 890141. [Google Scholar] [CrossRef]
- Iriti, M.; Varoni, E.M. Chemopreventive potential of flavonoids in oral squamous cell carcinoma in human studies. Nutrients 2013, 5, 2564–2576. [Google Scholar] [CrossRef]
- Gullett, N.P.; Amin, A.R.; Bayraktar, S.; Pezzuto, J.M.; Shin, D.M.; Khuri, F.R.; Aggarwal, B.B.; Surh, Y.-J.; Kucuk, O. Cancer prevention with natural compounds. Semin. Oncol. 2010, 37, 258–281. [Google Scholar] [CrossRef]
- Abidi, A.H.; Abhyankar, V.; Alghamdi, S.S.; Tipton, D.A.; Dabbous, M. Phytocannabinoids regulate inflammation in IL-1β-stimulated human gingival fibroblasts. J. Periodontal Res. 2022, 57, 1127–1138. [Google Scholar] [CrossRef]
- Sola, V.M.; Aguilar, J.J.; Vazquez Mosquera, A.P.; Carpentieri, A.R. Melatonin is an effective protector of gingival cells damaged by the cytotoxic effect of glutamate and DL-buthionine sulfoximine. J. Periodontal Res. 2021, 56, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Paolantoni, G.; Marenzi, G.; Blasi, A.; Mignogna, J.; Sammartino, G. Findings of a four-year randomized controlled clinical trial comparing two-piece and one-piece zirconia abutments supporting single prosthetic restorations in maxillary anterior region. BioMed Res. Int. 2016, 2016, 8767845. [Google Scholar] [CrossRef] [PubMed]
- Manson, M.M.; Farmer, P.B.; Gescher, A.; Steward, W.P. Innovative agents in cancer prevention. In Tumor Prevention and Genetics III; Springer: Berlin/Heidelberg, Germany, 2005; pp. 257–275. [Google Scholar]
- Ding, Y.; Yao, H.; Yao, Y.; Yenwong Fai, L.; Zhang, Z. Protection of dietary polyphenols against oral cancer. Nutrients 2013, 5, 2173–2191. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.A.R.; Camilli, A.C.; Maldonado, L.A.G.; Pacheco, C.G.P.; Silva, A.F.; Molon, R.S.; Spolidorio, L.C.; Ribeiro de Assis, L.; Regasini, L.O.; Rossa Junior, C. Chalcone T4, a novel chalconic compound, inhibits inflammatory bone resorption in vivo and suppresses osteoclastogenesis in vitro. J. Periodontal Res. 2021, 56, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Chin, Y.T.; Tu, H.P.; Lin, C.Y.; Kuo, P.J.; Chiu, H.C.; Liu, S.H.; Lee, S.Y.; Fu, E. Antioxidants protect against gingival overgrowth induced by cyclosporine A. J. Periodontal Res. 2021, 56, 397–407. [Google Scholar] [CrossRef]
- Frond, A.D.; Iuhas, C.I.; Stirbu, I.; Leopold, L.; Socaci, S.; Andreea, S.; Ayvaz, H.; Andreea, S.; Mihai, S.; Diaconeasa, Z. Phytochemical characterization of five edible purple-reddish vegetables: Anthocyanins, flavonoids, and phenolic acid derivatives. Molecules 2019, 24, 1536. [Google Scholar] [CrossRef]
- Mukhtar, H.; Ahmad, N. Tea polyphenols: Prevention of cancer and optimizing health. Am. J. Clin. Nutr. 2000, 71, 1698S–1702S. [Google Scholar] [CrossRef]
- Yuan, J.-M. Cancer prevention by green tea: Evidence from epidemiologic studies. Am. J. Clin. Nutr. 2013, 98, 1676S–1681S. [Google Scholar] [CrossRef]
- Belobrov, S.; Seers, C.; Reynolds, E.; Cirillo, N.; McCullough, M. Functional and molecular effects of a green tea constituent on oral cancer cells. J. Oral Pathol. Med. 2019, 48, 604–610. [Google Scholar] [CrossRef]
- Melo, J.G.; Sousa, J.P.; Firmino, R.T.; Matins, C.C.; Granville-Garcia, A.F.; Nonaka, C.F.; Costa, E.M. Different applications forms of green tea (Camellia sinensis (L.) Kuntze) for the treatment of periodontitis: A systematic review and meta-analysis. J. Periodontal Res. 2021, 56, 443–453. [Google Scholar] [CrossRef]
- Irimie, A.I.; Braicu, C.; Zanoaga, O.; Pileczki, V.; Gherman, C.; Berindan-Neagoe, I.; Campian, R.S. Epigallocatechin-3-gallate suppresses cell proliferation and promotes apoptosis and autophagy in oral cancer SSC-4 cells. OncoTargets Ther. 2015, 8, 461–470. [Google Scholar]
- Koh, Y.W.; Choi, E.C.; Kang, S.U.; Hwang, H.S.; Lee, M.H.; Pyun, J.; Park, R.; Lee, Y.; Kim, C.-H. Green tea (−)-epigallocatechin-3-gallate inhibits HGF-induced progression in oral cavity cancer through suppression of HGF/c-Met. J. Nutr. Biochem. 2011, 22, 1074–1083. [Google Scholar] [CrossRef] [PubMed]
- Klass, C.M.; Shin, D.M. Current status and future perspectives of chemoprevention in head and neck cancer. Curr. Cancer Drug Targets 2007, 7, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Li, M.; Liu, W.-B.; Zhou, Z.-S.; Zhang, R.; Li, J.-L.; Zhou, K.-C. Epigallocatechin gallate inhibits human tongue carcinoma cells via HK2-mediated glycolysis. Oncol. Rep. 2015, 33, 1533–1539. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, H.; Yoshida, H.; Matsuda, S.; Ryoke, T.; Ohta, K.; Ohmori, M.; Yamamoto, S.; Kiyoshima, T.; Kobayashi, M.; Sano, K. The therapeutic potential of epigallocatechin-3-gallate against human oral squamous cell carcinoma through inhibition of cell proliferation and induction of apoptosis: In vitro and in vivo murine xenograft study. Mol. Med. Rep. 2019, 20, 1139–1148. [Google Scholar] [CrossRef]
- Imai, K.; Suga, K.; Nakachi, K. Cancer-preventive effects of drinking green tea among a Japanese population. Prev. Med. 1997, 26, 769–775. [Google Scholar] [CrossRef]
- Neetha, M.C.; Panchaksharappa, M.G.; Pattabhiramasastry, S.; Shivaprasad, N.V.; Venkatesh, U.G. Chemopreventive synergism between green tea extract and curcumin in patients with potentially malignant oral disorders: A double-blind, randomized preliminary study. J. Contemp. Dent. Pract. 2020, 21, 521–531. [Google Scholar] [CrossRef]
- Amin, A.; Wang, D.; Nannapaneni, S.; Lamichhane, R.; Chen, Z.G.; Shin, D.M. Combination of resveratrol and green tea epigallocatechin gallate induces synergistic apoptosis and inhibits tumor growth in vivo in head and neck cancer models. Oncol. Rep. 2021, 45, 87. [Google Scholar] [CrossRef]
- Zlotogorski, A.; Dayan, A.; Dayan, D.; Chaushu, G.; Salo, T.; Vered, M. Nutraceuticals as new treatment approaches for oral cancer: II. Green tea extracts and resveratrol. Oral Oncol. 2013, 49, 502–506. [Google Scholar] [CrossRef]
- Tyagi, A.; Gu, M.; Takahata, T.; Frederick, B.; Agarwal, C.; Siriwardana, S.; Agarwal, R.; Sclafani, R.A. Resveratrol selectively induces DNA Damage, independent of Smad4 expression, in its efficacy against human head and neck squamous cell carcinoma. Clin. Cancer Res. 2011, 17, 5402–5411. [Google Scholar] [CrossRef]
- Ghiringhelli, F.; Rebe, C.; Hichami, A.; Delmas, D. Immunomodulation and anti-inflammatory roles of polyphenols as anticancer agents. Anti-Cancer Agents Med. Chem. (Former. Curr. Med. Chem.-Anti-Cancer Agents) 2012, 12, 852–873. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Paik, J.H.; Cho, D.; Cho, J.-A.; Kim, C.-W. Resveratrol induces the suppression of tumor-derived CD4+ CD25+ regulatory T cells. Int. Immunopharmacol. 2008, 8, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Brown, V.A.; Patel, K.R.; Viskaduraki, M.; Crowell, J.A.; Perloff, M.; Booth, T.D.; Vasilinin, G.; Sen, A.; Schinas, A.M.; Piccirilli, G. Repeat dose study of the cancer chemopreventive agent resveratrol in healthy volunteers: Safety, pharmacokinetics, and effect on the insulin-like growth factor axis. Cancer Res. 2010, 70, 9003–9011. [Google Scholar] [CrossRef] [PubMed]
- Singh, C.K.; Ndiaye, M.A.; Ahmad, N. Resveratrol and cancer: Challenges for clinical translation. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2015, 1852, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Popat, R.; Plesner, T.; Davies, F.; Cook, G.; Cook, M.; Elliott, P.; Jacobson, E.; Gumbleton, T.; Oakervee, H.; Cavenagh, J. A phase 2 study of SRT501 (resveratrol) with bortezomib for patients with relapsed and or refractory multiple myeloma. Br. J. Haematol. 2012, 160, 714–717. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Chin, Y.-T.; Shih, Y.-J.; Chen, Y.-R.; Chung, Y.-Y.; Lin, C.-Y.; Hsiung, C.-N.; Whang-Peng, J.; Lee, S.-Y.; Lin, H.-Y. Resveratrol antagonizes thyroid hormone-induced expression of checkpoint and proliferative genes in oral cancer cells. J. Dent. Sci. 2019, 14, 255–262. [Google Scholar] [CrossRef]
- Hsieh, M.-T.; Wang, L.-M.; Changou, C.A.; Chin, Y.-T.; Yang, Y.-C.S.; Lai, H.-Y.; Lee, S.-Y.; Yang, Y.-N.; Whang-Peng, J.; Liu, L.F. Crosstalk between integrin αvβ3 and ERα contributes to thyroid hormone-induced proliferation of ovarian cancer cells. Oncotarget 2017, 8, 24237. [Google Scholar] [CrossRef]
- Lin, H.Y.; Chin, Y.T.; Nana, A.W.; Shih, Y.J.; Lai, H.Y.; Tang, H.Y.; Leinung, M.; Mousa, S.A.; Davis, P.J. Actions of l-thyroxine and Nano-diamino-tetrac (Nanotetrac) on PD-L1 in cancer cells. Steroids 2016, 114, 59–67. [Google Scholar] [CrossRef]
- Kim, J.Y.; Cho, K.H.; Jeong, B.Y.; Park, C.G.; Lee, H.Y. Zeb1 for RCP-induced oral cancer cell invasion and its suppression by resveratrol. Exp. Mol. Med. 2020, 52, 1152–1163. [Google Scholar] [CrossRef]
- Ho, Y.; Wu, C.Y.; Chin, Y.T.; Li, Z.L.; Pan, Y.S.; Huang, T.Y.; Su, P.Y.; Lee, S.Y.; Crawford, D.R.; Su, K.W.; et al. NDAT suppresses pro-inflammatory gene expression to enhance resveratrol-induced anti-proliferation in oral cancer cells. Food Chem. Toxicol. 2020, 136, 111092. [Google Scholar] [CrossRef]
- Singh, V.; Singh, R.; Kujur, P.K.; Singh, R.P. Combination of Resveratrol and Quercetin Causes Cell Growth Inhibition, DNA Damage, Cell Cycle Arrest, and Apoptosis in Oral Cancer Cells. ASSAY Drug Dev. Technol. 2020, 18, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Kresty, L.A.; Mallery, S.R.; Stoner, G.D. Black raspberries in cancer clinical trials: Past, present and future. J. Berry Res. 2016, 6, 251. [Google Scholar] [CrossRef] [PubMed]
- Knobloch, T.J.; Uhrig, L.K.; Pearl, D.K.; Casto, B.C.; Warner, B.M.; Clinton, S.K.; Sardo-Molmenti, C.L.; Ferguson, J.M.; Daly, B.T.; Riedl, K. Suppression of proinflammatory and prosurvival biomarkers in oral cancer patients consuming a black raspberry phytochemical-rich troche. Cancer Prev. Res. 2016, 9, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Oghumu, S.; Casto, B.C.; Ahn-Jarvis, J.; Weghorst, L.C.; Maloney, J.; Geuy, P.; Horvath, K.Z.; Bollinger, C.E.; Warner, B.M.; Summersgill, K.F. Inhibition of pro-inflammatory and anti-apoptotic biomarkers during experimental oral cancer chemoprevention by dietary black raspberries. Front. Immunol. 2017, 8, 1325. [Google Scholar] [CrossRef] [PubMed]
- Knobloch, T.J.; Ryan, N.M.; Bruschweiler-Li, L.; Wang, C.; Bernier, M.C.; Somogyi, A.; Yan, P.S.; Cooperstone, J.L.; Mo, X.; Brüschweiler, R.P. Metabolic regulation of glycolysis and AMP activated protein kinase pathways during black raspberry-mediated oral cancer chemoprevention. Metabolites 2019, 9, 140. [Google Scholar] [CrossRef] [PubMed]
- Guttenplan, J.B.; Chen, K.-M.; Sun, Y.-W.; Lajara, B.; Shalaby, N.A.; Kosinska, W.; Benitez, G.; Gowda, K.; Amin, S.; Stoner, G. Effects of black raspberry extract and berry compounds on repair of DNA damage and mutagenesis induced by chemical and physical agents in human oral leukoplakia and rat oral fibroblasts. Chem. Res. Toxicol. 2017, 30, 2159–2164. [Google Scholar] [CrossRef] [PubMed]
- Guttenplan, J.B.; Chen, K.-M.; Sun, Y.-W.; Kosinska, W.; Zhou, Y.; Kim, S.; Sung, Y.; Gowda, K.; Amin, S.; Stoner, G.D. Effects of black raspberry extract and protocatechuic acid on carcinogen-DNA adducts and mutagenesis, and oxidative stress in rat and human oral cells. Cancer Prev. Res. 2016, 9, 704–712. [Google Scholar] [CrossRef]
- Shumway, B.S.; Kresty, L.A.; Larsen, P.E.; Zwick, J.C.; Lu, B.; Fields, H.W.; Mumper, R.J.; Stoner, G.D.; Mallery, S.R. Effects of a topically applied bioadhesive berry gel on loss of heterozygosity indices in premalignant oral lesions. Clin. Cancer Res. 2008, 14, 2421–2430. [Google Scholar] [CrossRef]
- Mallery, S.R.; Tong, M.; Shumway, B.S.; Curran, A.E.; Larsen, P.E.; Ness, G.M.; Kennedy, K.S.; Blakey, G.H.; Kushner, G.M.; Vickers, A.M. Topical application of a mucoadhesive freeze-dried black raspberry gel induces clinical and histologic regression and reduces loss of heterozygosity events in premalignant oral intraepithelial lesions: Results from a multicentered, placebo-controlled clinical trial. Clin. Cancer Res. 2014, 20, 1910–1924. [Google Scholar]
- Garewal, H. Potential role of β-carotene in prevention of oral cancer. Am. J. Clin. Nutr. 1991, 53, S294–S297. [Google Scholar] [CrossRef]
- Stich, H.F.; Hornby, A.P.; Dunn, B.P. Beta-carotene levels in exfoliated mucosa cells of population groups at low and elevated risk for oral cancer. Int. J. Cancer 1986, 37, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Milani, A.; Basirnejad, M.; Shahbazi, S.; Bolhassani, A. Carotenoids: Biochemistry, pharmacology and treatment. Br. J. Pharmacol. 2017, 174, 1290–1324. [Google Scholar] [CrossRef] [PubMed]
- Bhavana, S.M.; Lakshmi, C.R. Oral oncoprevention by phytochemicals-a systematic review disclosing the therapeutic dilemma. Adv. Pharm. Bull. 2014, 4, 413. [Google Scholar] [PubMed]
- Tan, B.L.; Norhaizan, M.E. Carotenoids: How effective are they to prevent age-related diseases? Molecules 2019, 24, 1801. [Google Scholar] [CrossRef] [PubMed]
- Leoncini, E.; Nedovic, D.; Panic, N.; Pastorino, R.; Edefonti, V.; Boccia, S. Carotenoid intake from natural sources and head and neck cancer: A systematic review and meta-analysis of epidemiological studies. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1003–1011. [Google Scholar] [CrossRef]
- De Luca, L.; Maestri, N.; Bonanni, F.; Nelson, D. Maintenance of epithelial cell differentiation: The mode of action of vitamin A. Cancer 1972, 30, 1326–1331. [Google Scholar] [CrossRef]
- Hathcock, J.N.; Hattan, D.G.; Jenkins, M.Y.; McDonald, J.T.; Sundaresan, P.R.; Wilkening, V.L. Evaluation of vitamin A toxicity. Am. J. Clin. Nutr. 1990, 52, 183–202. [Google Scholar] [CrossRef]
- Niranjana, R.; Gayathri, R.; Mol, S.N.; Sugawara, T.; Hirata, T.; Miyashita, K.; Ganesan, P. Carotenoids modulate the hallmarks of cancer cells. J. Funct. Foods 2015, 18, 968–985. [Google Scholar] [CrossRef]
- Nagao, T.; Warnakulasuriya, S.; Nakamura, T.; Kato, S.; Yamamoto, K.; Fukano, H.; Suzuki, K.; Shimozato, K.; Hashimoto, S. Treatment of oral leukoplakia with a low-dose of beta-carotene and vitamin C supplements: A randomized controlled trial. Int. J. Cancer 2015, 136, 1708–1717. [Google Scholar] [CrossRef] [PubMed]
- Buajeeb, W.; Kraivaphan, P.; Amornchat, C.; Suthamajariya, K. Reduction of micronuclei in oral lichen planus supplemented with beta-carotene. J. Oral Sci. 2008, 50, 461–467. [Google Scholar] [CrossRef]
- Hong, W.K.; Endicott, J.; Itri, L.M.; Doos, W.; Batsakis, J.G.; Bell, R.; Fofonoff, S.; Byers, R.; Atkinson, E.N.; Vaughan, C. 13-cis-retinoic acid in the treatment of oral leukoplakia. N. Engl. J. Med. 1986, 315, 1501–1505. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.F.; Stevens, M.; Rabie, I.; Yarker, M.-E.; Cochrane, J.; Perry, E.; Traficante, R.; Coman, W. Chemoprevention of head and neck cancer with retinoids: A negative result. Arch. Otolaryngol.-Head Neck Surg. 2005, 131, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Garewal, H.S.; Katz, R.; Meyskens, F.; Pitcock, J.; Morse, D.; Friedman, S.; Peng, Y.; Pendrys, D.; Mayne, S.; Alberts, D. β-carotene produces sustained remissions in patients with oral leukoplakia: Results of a multicenter prospective trial. Arch. Otolaryngol.-Head Neck Surg. 1999, 125, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Papadimitrakopoulou, V.A.; Lee, J.J.; William, W.N., Jr.; Martin, J.W.; Thomas, M.; Kim, E.S.; Khuri, F.R.; Shin, D.M.; Feng, L.; Hong, W.K. Randomized trial of 13-cis retinoic acid compared with retinyl palmitate with or without beta-carotene in oral premalignancy. J. Clin. Oncol. 2009, 27, 599. [Google Scholar] [CrossRef] [PubMed]
- Seixas-Silva, J.A.; Richards, T.; Khuri, F.R.; Wieand, H.S.; Kim, E.; Murphy, B.; Francisco, M.; Hong, W.K.; Shin, D.M. Phase 2 bioadjuvant study of interferon alfa-2a, isotretinoin, and vitamin E in locally advanced squamous cell carcinoma of the head and neck: Long-term follow-up. Arch. Otolaryngol.-Head Neck Surg. 2005, 131, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Jawanda, M.K.; Arora, V.; Mehta, N.; Yadav, V. Role of lycopene in preventing oral diseases as a nonsurgical aid of treatment. Int. J. Prev. Med. 2015, 6, 70. [Google Scholar] [CrossRef]
- Kumar, A.; Bagewadi, A.; Keluskar, V.; Singh, M. Efficacy of lycopene in the management of oral submucous fibrosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 207–213. [Google Scholar] [CrossRef]
- Wang, R.; Lu, X.; Yu, R. Lycopene inhibits epithelial–mesenchymal transition and promotes apoptosis in oral cancer via PI3K/AKT/m-TOR signal pathway. Drug Des. Dev. Ther. 2020, 14, 2461–2471. [Google Scholar] [CrossRef]
- Chang, L.; Graham, P.; Hao, J.; Ni, J.; Bucci, J.; Cozzi, P.; Kearsley, J.; Li, Y. Acquisition of epithelial–mesenchymal transition and cancer stem cell phenotypes is associated with activation of the PI3K/Akt/mTOR pathway in prostate cancer radioresistance. Cell Death Dis. 2013, 4, e875. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Meng, Q.; Guo, H.; Xiao, L.; Yang, X.; Cui, Y.; Huang, Y. TGF-β2 induces epithelial-mesenchymal transition in cultured human lens epithelial cells through activation of the PI3K/Akt/mTOR signaling pathway. Mol. Med. Rep. 2016, 13, 1105–1110. [Google Scholar] [CrossRef]
- Chang, L.; Graham, P.; Hao, J.; Ni, J.; Bucci, J.; Cozzi, P.; Kearsley, J.; Li, Y. PI3K/Akt/mTOR pathway inhibitors enhance radiosensitivity in radioresistant prostate cancer cells through inducing apoptosis, reducing autophagy, suppressing NHEJ and HR repair pathways. Cell Death Dis. 2014, 5, e1437. [Google Scholar] [CrossRef]
- Zhang, D.-M.; Liu, J.-S.; Deng, L.-J.; Chen, M.-F.; Yiu, A.; Cao, H.-H.; Tian, H.-Y.; Fung, K.-P.; Kurihara, H.; Pan, J.-X. Arenobufagin, a natural bufadienolide from toad venom, induces apoptosis and autophagy in human hepatocellular carcinoma cells through inhibition of PI3K/Akt/mTOR pathway. Carcinogenesis 2013, 34, 1331–1342. [Google Scholar] [CrossRef] [PubMed]
- Nieto, M.A.; Huang, R.Y.-J.; Jackson, R.A.; Thiery, J.P. EMT: 2016. Cell 2016, 166, 21–45. [Google Scholar] [CrossRef] [PubMed]
- Brabletz, T.; Kalluri, R.; Nieto, M.A.; Weinberg, R.A. EMT in cancer. Nat. Rev. Cancer 2018, 18, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Tao, A.; Wang, X.; Li, C. Effect of Lycopene on oral squamous cell carcinoma cell growth by inhibiting IGF1 pathway. Cancer Manag. Res. 2021, 13, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Bhuvaneswari, V.; Velmurugan, B.; Balasenthil, S.; Ramachandran, C.R.; Nagini, S. Chemopreventive efficacy of lycopene on 7, 12-dimethylbenz [a] anthracene-induced hamster buccal pouch carcinogenesis. Fitoterapia 2001, 72, 865–874. [Google Scholar] [CrossRef]
- Liu, W.; Cui, Y.; Wei, J.; Sun, J.; Zheng, L.; Xie, J. Gap junction-mediated cell-to-cell communication in oral development and oral diseases: A concise review of research progress. Int. J. Oral Sci. 2020, 12, 17. [Google Scholar] [CrossRef]
- Singh, M.; Krishanappa, R.; Bagewadi, A.; Keluskar, V. Efficacy of oral lycopene in the treatment of oral leukoplakia. Oral Oncol. 2004, 40, 591–596. [Google Scholar] [CrossRef]
- Huang, R.Y.; Wong, M.; Tan, T.; Kuay, K.; Ng, A.; Chung, V.; Chu, Y.; Matsumura, N.; Lai, H.; Lee, Y. An EMT spectrum defines an anoikis-resistant and spheroidogenic intermediate mesenchymal state that is sensitive to e-cadherin restoration by a src-kinase inhibitor, saracatinib (AZD0530). Cell Death Dis. 2013, 4, e915. [Google Scholar] [CrossRef]
- Li, Y.; Jiao, J.; Qi, Y.; Yu, W.; Yang, S.; Zhang, J.; Zhao, J. Curcumin: A review of experimental studies and mechanisms related to periodontitis treatment. J. Periodontal Res. 2021, 56, 837–847. [Google Scholar] [CrossRef]
- Lin, C.-L.; Lin, J.-K. Curcumin: A potential cancer chemopreventive agent through suppressing NF-κB signaling. J. Cancer Mol. 2008, 4, 11–16. [Google Scholar]
- Lee, A.Y.-L.; Fan, C.-C.; Chen, Y.-A.; Cheng, C.-W.; Sung, Y.-J.; Hsu, C.-P.; Kao, T.-Y. Curcumin inhibits invasiveness and epithelial-mesenchymal transition in oral squamous cell carcinoma through reducing matrix metalloproteinase 2, 9 and modulating p53-E-cadherin pathway. Integr. Cancer Ther. 2015, 14, 484–490. [Google Scholar] [CrossRef]
- Lim, J.; Thiery, J.P. Epithelial-mesenchymal transitions: Insights from development. Development 2012, 139, 3471–3486. [Google Scholar] [CrossRef] [PubMed]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.; Nieto, M.A. Epithelial-mesenchymal transitions in development and disease. Cell 2009, 139, 871–890. [Google Scholar] [CrossRef] [PubMed]
- Iwatsuki, M.; Mimori, K.; Yokobori, T.; Ishi, H.; Beppu, T.; Nakamori, S.; Baba, H.; Mori, M. Epithelial–mesenchymal transition in cancer development and its clinical significance. Cancer Sci. 2010, 101, 293–299. [Google Scholar] [CrossRef]
- Muller, P.A.; Vousden, K.H. p53 mutations in cancer. Nat. Cell Biol. 2013, 15, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Muller, P.A.; Vousden, K.H.; Norman, J.C. p53 and its mutants in tumor cell migration and invasion. J. Cell Biol. 2011, 192, 209–218. [Google Scholar] [CrossRef]
- Kuttan, R.; Sudheeran, P.; Josph, C. Turmeric and curcumin as topical agents in cancer therapy. Tumori J. 1987, 73, 29–31. [Google Scholar] [CrossRef]
- Hsieh, C. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, e2900. [Google Scholar]
- Tuttle, S.; Hertan, L.; Daurio, N.; Porter, S.; Kaushick, C.; Li, D.; Myamoto, S.; Lin, A.; O’Malley, B.W.; Koumenis, C. The chemopreventive and clinically used agent curcumin sensitizes HPV-but not HPV+ HNSCC to ionizing radiation, in vitro and in a mouse orthotopic model. Cancer Biol. Ther. 2012, 13, 575–584. [Google Scholar] [CrossRef]
- Javvadi, P.; Hertan, L.; Kosoff, R.; Datta, T.; Kolev, J.; Mick, R.; Tuttle, S.W.; Koumenis, C. Thioredoxin reductase-1 mediates curcumin-induced radiosensitization of squamous carcinoma cells. Cancer Res. 2010, 70, 1941–1950. [Google Scholar] [CrossRef]
- Garg, A.K.; Buchholz, T.A.; Aggarwal, B.B. Chemosensitization and radiosensitization of tumors by plant polyphenols. Antioxid. Redox Signal. 2005, 7, 1630–1647. [Google Scholar] [CrossRef] [PubMed]
- Pescosolido, N.; Giannotti, R.; Plateroti, A.M.; Pascarella, A.; Nebbioso, M. Curcumin: Therapeutical potential in ophthalmology. Planta Med. 2013, 80, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Chen, K.; Huang, L.; Li, J. Pharmacokinetic properties and drug interactions of apigenin, a natural flavone. Expert Opin. Drug Metab. Toxicol. 2017, 13, 323–330. [Google Scholar] [CrossRef]
- Seca, A.M.; Pinto, D.C. Plant secondary metabolites as anticancer agents: Successes in clinical trials and therapeutic application. Int. J. Mol. Sci. 2018, 19, 263. [Google Scholar] [CrossRef]
- Sammartino, G.; Marenzi, G.; Tammaro, L.; Bolognese, A.; Calignano, A.; Costantino, U.; Califano, L.; Mastrangelo, F.; Tete, S.; Vittoria, V. Anti-inflammatory drug incorporation into polymeric nano-hybrids for local controlled release. Int. J. Immunopathol. Pharmacol. 2005, 18, 55–62. [Google Scholar] [PubMed]
- Vaddepally, R.K.; Kharel, P.; Pandey, R.; Garje, R.; Chandra, A.B. Review of indications of FDA-approved immune checkpoint inhibitors per NCCN guidelines with the level of evidence. Cancers 2020, 12, 738. [Google Scholar] [CrossRef]
- Wang, J.; Xie, T.; Wang, B.; William, W.N., Jr.; Heymach, J.V.; El-Naggar, A.K.; Myers, J.N.; Caulin, C. PD-1 blockade prevents the development and progression of carcinogen-induced oral premalignant lesions. Cancer Prev. Res. 2017, 10, 684–693. [Google Scholar] [CrossRef]
- Hodi, F.S.; O’day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Postow, M.A.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.; McDermott, D.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.; Harrington, K.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.; Soria, A.; Machiels, J.; Mach, N.; Mehra, R. Pembrolizumab (pembro) vs standard of care (SOC) for recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC): Phase 3 KEYNOTE-040 trial. Ann. Oncol. 2017, 28, v628. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol. 2018, 81, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Myers, G. Immune-related adverse events of immune checkpoint inhibitors: A brief review. Curr. Oncol. 2018, 25, 342–347. [Google Scholar] [CrossRef]
- Svider, P.F.; Warner, B.M.; Schwartz, S.J.; Garshott, D.M.; Weinstein, J.D.; Fribley, A.M. Mucosal therapy for potentially malignant diseases and OSCC. In Targeting Oral Cancer; Springer: Cham, Switzerland, 2016; pp. 283–299. [Google Scholar]
- Shah, J.P.; Strong, E.W.; DeCosse, J.J.; Itri, L.; Sellers, P. Effect of retinoids on oral leukoplakia. Am. J. Surg. 1983, 146, 466–470. [Google Scholar] [CrossRef]
- Tetè, S.; Pappalardo, S.; Rubini, C.; Salini, L.; Falco, A.; Perfetti, E. The role of apoptosis and bcl-2 protein in topical treatment of oral leukoplakia with isotretinoin. Minerva Stomatol. 1999, 48, 411–418. [Google Scholar]
- Wang, Z.; Polavaram, R.; Fuentes, C.F.; Shapshay, S.M. Topical chemoprevention of oral cancer with tretinoin biofilm. Arch. Otolaryngol.-Head Neck Surg. 2003, 129, 869–873. [Google Scholar] [CrossRef]
- Epstein, J.B.; Gorsky, M. Topical application of vitamin A to oral leukoplakia: A clinical case series. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1999, 86, 921–927. [Google Scholar] [CrossRef]
- Piattelli, A.; Fioroni, M.; Santinelli, A.; Rubini, C. bcl-2 expression and apoptotic bodies in 13-cis-retinoic acid (isotretinoin)-topically treated oral leukoplakia: A pilot study. Oral Oncol. 1999, 35, 314–320. [Google Scholar] [CrossRef]
- Scardina, G.A.; Carini, F.; Leone, A.; Lannino, F.; Messina, P.; Maresi, E.; Valenza, V. Oral leukoplakia–topical isotretinoin treatment. Dent. Med. Probl. 2005, 42, 37–40. [Google Scholar]
- Epstein, J.B.; Gorsky, M.; Wong, F.L.; Millner, A. Topical bleomycin for the treatment of dysplastic oral leukoplakia. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1998, 83, 629–634. [Google Scholar] [CrossRef]
- Epstein, J.B.; Wong, F.L.; Millner, A.; Le, N.D. Topical bleomycin treatment of oral leukoplakia: A randomized double-blind clinical trial. Head Neck 1994, 16, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Hammersley, N.; Ferguson, M.; Rennie, J. Topical bleomycin in the treatment of oral leukoplakia: A pilot study. Br. J. Oral Maxillofac. Surg. 1985, 23, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Malmström, M.; Hietanen, J.; Sane, J.; Sysmäläinen, M. Topical treatment of oral leukoplakia with bleomycin. Br. J. Oral Maxillofac. Surg. 1988, 26, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.; Epstein, J.; Millner, A. Treatment of oral leukoplakia with topical bleomycin. A pilot study. Cancer 1989, 64, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Mulshine, J.L.; Atkinson, J.C.; Greer, R.O.; Papadimitrakopoulou, V.A.; Van Waes, C.; Rudy, S.; Martin, J.W.; Steinberg, S.M.; Liewehr, D.J.; Avis, I. Randomized, double-blind, placebo-controlled phase IIb trial of the cyclooxygenase inhibitor ketorolac as an oral rinse in oropharyngeal leukoplakia. Clin. Cancer Res. 2004, 10, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Glass, C.K.; Rosenfeld, M.G. Coactivator and corepressor complexes in nuclear receptor function. Curr. Opin. Genet. Dev. 1999, 9, 140–147. [Google Scholar] [CrossRef]
- Nagpal, S.; Athanikar, J.; Chandraratna, R.A. Separation of Transactivation and AP1 Antagonism Functions of Retinoic Acid Receptor α (∗). J. Biol. Chem. 1995, 270, 923–927. [Google Scholar] [CrossRef]
- Allenby, G. The Ying-yang of RAR and AP-1: Cancer treatment without overt toxicity: A new class of retinoids with selective inhibition of AP-1 inhibits proliferation. Fanjul A, Dawson MI, Hobbs PD, Jong L, Cameron JF, Harlev E, Graupner G, Xian-Ping L & Pfahl M. Nature, 372 107—111. Hum. Exp. Toxicol. 1995, 14, 226–230. [Google Scholar]
- Umezawa, H.; Suhara, Y.; Takita, T.; Maeda, K. Purification of bleomycins. J. Antibiot. 1966, 19, 210–215. [Google Scholar]
- Kunimoto, T.; Hori, M.; Umezawa, H. Modes of action of phleomycin, bleomycin and formycin on HeLa S3 cells in synchronized culture. J. Antibiot. 1967, 20, 277–281. [Google Scholar]
- Blum, R.H.; Carter, S.K.; Agre, K. A clinical review of bleomycin—A new antineoplastic agent. Cancer 1973, 31, 903–914. [Google Scholar] [CrossRef] [PubMed]
- Shanta, V.; Krishnamurthi, S. Combined bleomycin and radiotherapy in oral cancer. Clin. Radiol. 1980, 31, 617–620. [Google Scholar] [CrossRef]
- Hayasaki, K.; Kitamura, T.; Kaneko, T.; Tachibana, M.; Kobayashi, N.; Tosaka, K.; Yaku, Y. Application of BLM-iontophoresis for the tumor-therapy of the head and neck area (author’s transl). Nihon Gan Chiryo Gakkai Shi 1977, 12, 522–527. [Google Scholar]
- Panje, W.R. Regression of head and neck carcinoma with a prostaglandin-synthesis inhibitor. Arch. Otolaryngol. 1981, 107, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Gallus, S.; La Vecchia, C. Aspirin and cancer risk: An updated quantitative review to 2005. Cancer Causes Control 2006, 17, 871–888. [Google Scholar] [CrossRef] [PubMed]
- Cronin-Fenton, D.P.; Pedersen, L.; Lash, T.L.; Friis, S.; Baron, J.A.; Sørensen, H.T. Prescriptions for selective cyclooxygenase-2 inhibitors, non-selective non-steroidal anti-inflammatory drugs, and risk of breast cancer in a population-based case-control study. Breast Cancer Res. 2010, 12, R15. [Google Scholar] [CrossRef]
- González-Pérez, A.; García Rodríguez, L.A.; López-Ridaura, R. Effects of non-steroidal anti-inflammatory drugs on cancer sites other than the colon and rectum: A meta-analysis. BMC Cancer 2003, 3, 28. [Google Scholar] [CrossRef]
- Shibata, M.; Kodani, I.; Osaki, M.; Araki, K.; Adachi, H.; Ryoke, K.; Ito, H. Cyclo-oxygenase-1 and-2 expression in human oral mucosa, dysplasias and squamous cell carcinomas and their pathological significance. Oral Oncol. 2005, 41, 304–312. [Google Scholar] [CrossRef]
- Wirth, L.J.; Krane, J.F.; Li, Y.; Othus, M.; Moran, A.E.; Dorfman, D.M.; Norris, C.M., Jr.; Goguen, L.; Posner, M.R.; Haddad, R.I. A pilot surrogate endpoint biomarker study of celecoxib in oral premalignant lesions. Cancer Prev. Res. 2008, 1, 339–348. [Google Scholar] [CrossRef]
- Papadimitrakopoulou, V.A.; William, W.N., Jr.; Dannenberg, A.J.; Lippman, S.M.; Lee, J.J.; Ondrey, F.G.; Peterson, D.E.; Feng, L.; Atwell, A.; El-Naggar, A.K. Pilot randomized phase II study of celecoxib in oral premalignant lesions. Clin. Cancer Res. 2008, 14, 2095–2101. [Google Scholar] [CrossRef] [PubMed]
- Sujir, N.; Priyanka, G.; Ahmed, J.; Saha, A.; Chhaparwal, Y.; Shenoy, N. Oral cancer chemoprevention: A review. Acta Marisiensis-Ser. Med. 2023, 69, 17–22. [Google Scholar] [CrossRef]
- Reuter, B.K.; Asfaha, S.; Buret, A.; Sharkey, K.A.; Wallace, J.L. Exacerbation of inflammation-associated colonic injury in rat through inhibition of cyclooxygenase-2. J. Clin. Investig. 1996, 98, 2076–2085. [Google Scholar] [CrossRef]
- Pontes-Quero, G.M.; Benito-Garzón, L.; Pérez Cano, J.; Aguilar, M.R.; Vázquez-Lasa, B. Modulation of inflammatory mediators by polymeric nanoparticles loaded with anti-inflammatory drugs. Pharmaceutics 2021, 13, 290. [Google Scholar] [CrossRef] [PubMed]
- Abo Aasy, N.K.; Ragab, D.; Sallam, M.A.; Abdelmonsif, D.A.; Aly, R.G.; Elkhodairy, K.A. A comparative study: The prospective influence of nanovectors in leveraging the chemopreventive potential of COX-2 inhibitors against skin cancer. Int. J. Nanomed. 2019, 14, 7561–7581. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.H. Phototoxicity and photoallergy. Semin. Cutan. Med. Surg. 1999, 18, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Dolmans, D.E.; Fukumura, D.; Jain, R.K. Photodynamic therapy for cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.C.; Marcus, S.L.; Pottier, R.H. Photodynamic therapy (PDT) and photodiagnosis (PD) using endogenous photosensitization induced by 5-aminolevulinic acid (ALA): Mechanisms and clinical results. J. Clin. Laser Med. Surg. 1996, 14, 289–304. [Google Scholar] [CrossRef]
- Kennedy, J.; Pottier, R.; Pross, D. Photodynamic therapy with endogenous protoporphyrin: IX: Basic principles and present clinical experience. J. Photochem. Photobiol. B Biol. 1990, 6, 143–148. [Google Scholar] [CrossRef]
- Lin, H.P.; Chen, H.M.; Yu, C.H.; Yang, H.; Wang, Y.P.; Chiang, C.P. Topical photodynamic therapy is very effective for oral verrucous hyperplasia and oral erythroleukoplakia. J. Oral Pathol. Med. 2010, 39, 624–630. [Google Scholar] [CrossRef]
- Yu, C.-H.; Chen, H.-M.; Hung, H.-Y.; Cheng, S.-J.; Tsai, T.; Chiang, C.-P. Photodynamic therapy outcome for oral verrucous hyperplasia depends on the clinical appearance, size, color, epithelial dysplasia, and surface keratin thickness of the lesion. Oral Oncol. 2008, 44, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Boutelle, A.M.; Attardi, L.D. p53 and tumor suppression: It takes a network. Trends Cell Biol. 2021, 31, 298–310. [Google Scholar] [CrossRef]
- Wang, Z.; Strasser, A.; Kelly, G.L. Should mutant TP53 be targeted for cancer therapy? Cell Death Differ. 2022, 29, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Hafner, A.; Bulyk, M.L.; Jambhekar, A.; Lahav, G. The multiple mechanisms that regulate p53 activity and cell fate. Nat. Rev. Mol. Cell Biol. 2019, 20, 199–210. [Google Scholar] [CrossRef]
- Nees, M.; Homann, N.; Discher, H.; Andl, T.; Enders, C.; Herold-Mende, C.; Schuhmann, A.; Bosch, F.X. Expression of mutated p53 occurs in tumor-distant epithelia of head and neck cancer patients: A possible molecular basis for the development of multiple tumors. Cancer Res. 1993, 53, 4189–4196. [Google Scholar] [PubMed]
- Tassone, P.; Old, M.; Teknos, T.N.; Pan, Q. p53-based therapeutics for head and neck squamous cell carcinoma. Oral Oncol. 2013, 49, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Heise, C.; Sampson-Johannes, A.; Williams, A.; Mccormick, F.; Von Hoff, D.D.; Kirn, D.H. ONYX-015, an E1B gene-attenuated adenovirus, causes tumor-specific cytolysis and antitumoral efficacy that can be augmented by standard chemotherapeutic agents. Nat. Med. 1997, 3, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.; Rudin, C.M. ONYX-015. Onyx Pharmaceuticals. Curr. Opin. Investig. Drugs 2001, 2, 1770–1775. [Google Scholar]
- Ries, S.; Korn, W. ONYX-015: Mechanisms of action and clinical potential of a replication-selective adenovirus. Br. J. Cancer 2002, 86, 5–11. [Google Scholar] [CrossRef]
- Rudin, C.M.; Cohen, E.E.; Papadimitrakopoulou, V.A.; Silverman, S., Jr.; Recant, W.; El-Naggar, A.K.; Stenson, K.; Lippman, S.M.; Hong, W.K.; Vokes, E.E. An attenuated adenovirus, ONYX-015, as mouthwash therapy for premalignant oral dysplasia. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 4546. [Google Scholar] [CrossRef]
- Li, Y.; Li, L.-J.; Zhang, S.-T.; Wang, L.-J.; Zhang, Z.; Gao, N.; Zhang, Y.-Y.; Chen, Q.-M. In vitro and clinical studies of gene therapy with recombinant human adenovirus-p53 injection for oral leukoplakia. Clin. Cancer Res. 2009, 15, 6724–6731. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kalyankrishna, S.; Grandis, J.R. Epidermal growth factor receptor biology in head and neck cancer. J. Clin. Oncol. 2006, 24, 2666–2672. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Raisch, K.P.; Trummell, H.Q.; Robert, F.; Meredith, R.F.; Spencer, S.A.; Buchsbaum, D.J.; Saleh, M.N.; Stackhouse, M.A.; LoBuglio, A.F. Enhanced apoptosis with combination C225/radiation treatment serves as the impetus for clinical investigation in head and neck cancers. J. Clin. Oncol. 2000, 18, 47s–53s. [Google Scholar] [PubMed]
- Huang, S.-M.; Bock, J.M.; Harari, P.M. Epidermal growth factor receptor blockade with C225 modulates proliferation, apoptosis, and radiosensitivity in squamous cell carcinomas of the head and neck. Cancer Res. 1999, 59, 1935–1940. [Google Scholar]
- Saleh, M.N.; Raisch, K.P.; Stackhouse, M.A.; Grizzle, W.E.; Bonner, J.A.; Mayo, M.S.; Kim, H.-G.; Meredith, R.F.; Wheeler, R.H.; Buchsbaum, D.J. Combined modality therapy of A431 human epidermoid cancer using anti-EGFr antibody C225 and radiation. Cancer Biother. Radiopharm. 1999, 14, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Cohen, R.B.; Jones, C.U.; Sur, R.K.; Raben, D.; Baselga, J.; Spencer, S.A.; Zhu, J. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol. 2010, 11, 21–28. [Google Scholar] [CrossRef]
- Ang, K.K.; Berkey, B.A.; Tu, X.; Zhang, H.-Z.; Katz, R.; Hammond, E.H.; Fu, K.K.; Milas, L. Impact of epidermal growth factor receptor expression on survival and pattern of relapse in patients with advanced head and neck carcinoma. Cancer Res. 2002, 62, 7350–7356. [Google Scholar]
- William, W.N.; Papadimitrakopoulou, V.; Lee, J.J.; Mao, L.; Cohen, E.E.; Lin, H.Y.; Gillenwater, A.M.; Martin, J.W.; Lingen, M.W.; Boyle, J.O. Erlotinib and the risk of oral cancer: The erlotinib prevention of oral cancer (EPOC) randomized clinical trial. JAMA Oncol. 2016, 2, 209–216. [Google Scholar] [CrossRef]
- Ohnishi, Y.; Minamino, Y.; Kakudo, K.; Nozaki, M. Resistance of oral squamous cell carcinoma cells to cetuximab is associated with EGFR insensitivity and enhanced stem cell-like potency. Oncol. Rep. 2014, 32, 780–786. [Google Scholar] [CrossRef]
- Grandis, J.R.; Melhem, M.F.; Barnes, E.L.; Tweardy, D.J. Quantitative immunohistochemical analysis of transforming growth factor-α and epidermal growth factor receptor in patients with squamous cell carcinoma of the head and neck. Cancer: Interdiscip. Int. J. Am. Cancer Soc. 1996, 78, 1284–1292. [Google Scholar] [CrossRef]
- Leeman-Neill, R.J.; Seethala, R.R.; Singh, S.V.; Freilino, M.L.; Bednash, J.S.; Thomas, S.M.; Panahandeh, M.C.; Gooding, W.E.; Joyce, S.C.; Lingen, M.W. Inhibition of EGFR-STAT3 signaling with erlotinib prevents carcinogenesis in a chemically-induced mouse model of oral squamous cell carcinoma. Cancer Prev. Res. 2011, 4, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Peréz-Soler, R.; Saltz, L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J. Clin. Oncol. 2005, 23, 5235–5246. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Kurzrock, R. Toxicity of targeted therapy: Implications for response and impact of genetic polymorphisms. Cancer Treat. Rev. 2014, 40, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhang, X.; Li, M.; Wang, Z.; Wieand, H.S.; Grandis, J.R.; Shin, D.M. Simultaneously targeting epidermal growth factor receptor tyrosine kinase and cyclooxygenase-2, an efficient approach to inhibition of squamous cell carcinoma of the head and neck. Clin. Cancer Res. 2004, 10, 5930–5939. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, Z.; Choe, M.S.; Lin, Y.; Sun, S.-Y.; Wieand, H.S.; Shin, H.J.C.; Chen, A.; Khuri, F.R.; Shin, D.M. Tumor growth inhibition by simultaneously blocking epidermal growth factor receptor and cyclooxygenase-2 in a xenograft model. Clin. Cancer Res. 2005, 11, 6261–6269. [Google Scholar] [CrossRef] [PubMed]
- Choe, M.S.; Zhang, X.; Shin, H.J.C.; Shin, D.M.; Chen, Z. Interaction between epidermal growth factor receptor–and cyclooxygenase 2–mediated pathways and its implications for the chemoprevention of head and neck cancer. Mol. Cancer Ther. 2005, 4, 1448–1455. [Google Scholar] [CrossRef]
- Saba, N.F.; Hurwitz, S.J.; Kono, S.A.; Yang, C.S.; Zhao, Y.; Chen, Z.; Sica, G.; Müller, S.; Moreno-Williams, R.; Lewis, M. Chemoprevention of head and neck cancer with celecoxib and erlotinib: Results of a phase ib and pharmacokinetic study. Cancer Prev. Res. 2014, 7, 283–291. [Google Scholar] [CrossRef]
- Bodmer, M.; Meier, C.; Krähenbühl, S.; Jick, S.S.; Meier, C.R. Long-term metformin use is associated with decreased risk of breast cancer. Diabetes Care 2010, 33, 1304–1308. [Google Scholar] [CrossRef]
- Bowker, S.L.; Majumdar, S.R.; Veugelers, P.; Johnson, J.A. Increased cancer-related mortality for patients with type 2 diabetes who use sulfonylureas or insulin: Response to Farooki and Schneider. Diabetes Care 2006, 29, 1990–1991. [Google Scholar] [CrossRef]
- Evans, J.M.; Donnelly, L.A.; Emslie-Smith, A.M.; Alessi, D.R.; Morris, A.D. Metformin and reduced risk of cancer in diabetic patients. Bmj 2005, 330, 1304–1305. [Google Scholar] [CrossRef] [PubMed]
- Pollak, M. Metformin and other biguanides in oncology: Advancing the research agenda. Cancer Prev. Res. 2010, 3, 1060–1065. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Marsh, C.A.; Dorsam, R.T.; Mikelis, C.M.; Masedunskas, A.; Amornphimoltham, P.; Nathan, C.A.; Singh, B.; Weigert, R.; Molinolo, A.A. Decreased lymphangiogenesis and lymph node metastasis by mTOR inhibition in head and neck cancer. Cancer Res. 2011, 71, 7103–7112. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Frederick, M.J.; Pickering, C.R.; Bettegowda, C.; Chang, K.; Li, R.J.; Fakhry, C.; Xie, T.-X.; Zhang, J.; Wang, J. Exome sequencing of head and neck squamous cell carcinoma reveals inactivating mutations in NOTCH1. Science 2011, 333, 1154–1157. [Google Scholar] [CrossRef] [PubMed]
- Stransky, N.; Egloff, A.M.; Tward, A.D.; Kostic, A.D.; Cibulskis, K.; Sivachenko, A.; Kryukov, G.V.; Lawrence, M.S.; Sougnez, C.; McKenna, A. The mutational landscape of head and neck squamous cell carcinoma. Science 2011, 333, 1157–1160. [Google Scholar] [CrossRef]
- Dowling, R.J.; Zakikhani, M.; Fantus, I.G.; Pollak, M.; Sonenberg, N. Metformin inhibits mammalian target of rapamycin–dependent translation initiation in breast cancer cells. Cancer Res. 2007, 67, 10804–10812. [Google Scholar] [CrossRef]
- Gwinn, D.M.; Shackelford, D.B.; Egan, D.F.; Mihaylova, M.M.; Mery, A.; Vasquez, D.S.; Turk, B.E.; Shaw, R.J. AMPK phosphorylation of raptor mediates a metabolic checkpoint. Mol. Cell 2008, 30, 214–226. [Google Scholar] [CrossRef]
- Luo, Q.; Hu, D.; Hu, S.; Yan, M.; Sun, Z.; Chen, F. In vitro and in vivoanti-tumor effect of metformin as a novel therapeutic agent in human oral squamous cell carcinoma. BMC Cancer 2012, 12, 517. [Google Scholar] [CrossRef]
- Shaw, R.J.; Bardeesy, N.; Manning, B.D.; Lopez, L.; Kosmatka, M.; DePinho, R.A.; Cantley, L.C. The LKB1 tumor suppressor negatively regulates mTOR signaling. Cancer Cell 2004, 6, 91–99. [Google Scholar] [CrossRef]
- Zakikhani, M.; Dowling, R.; Fantus, I.G.; Sonenberg, N.; Pollak, M. Metformin is an AMP kinase–dependent growth inhibitor for breast cancer cells. Cancer Res. 2006, 66, 10269–10273. [Google Scholar] [CrossRef]
- Hawley, S.A.; Ross, F.A.; Chevtzoff, C.; Green, K.A.; Evans, A.; Fogarty, S.; Towler, M.C.; Brown, L.J.; Ogunbayo, O.A.; Evans, A.M. Use of cells expressing γ subunit variants to identify diverse mechanisms of AMPK activation. Cell Metab. 2010, 11, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Kourelis, T.V.; Siegel, R.D. Metformin and cancer: New applications for an old drug. Med. Oncol. 2012, 29, 1314–1327. [Google Scholar] [CrossRef] [PubMed]
- Rattan, R.; Ali Fehmi, R.; Munkarah, A. Metformin: An emerging new therapeutic option for targeting cancer stem cells and metastasis. J. Oncol. 2012, 2012, 928127. [Google Scholar] [CrossRef]
- Rego, D.F.; Elias, S.T.; Amato, A.A.; De Luca Canto, G.; Guerra, E.N.S. Anti-tumor effects of metformin on head and neck carcinoma cell lines: A systematic review. Oncol. Lett. 2017, 13, 554–566. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D.; Campbell, I.; McBain, A.; Brown, I. Metformin efficacy and tolerance in obese non-insulin dependent diabetics: A comparison of two dosage schedules. Curr. Med. Res. Opin. 1989, 11, 273–278. [Google Scholar] [CrossRef]
- El-Zalabany, N.N.M.; Madkour, G.G.; Farag, H.A.; Shaker, O.G.; Zahran, F.H.M. Cancer chemoprevention by metformin hydrochloride compared to placebo in oral potentially malignant lesions: A randomized clinical trial. Ann. Rom. Soc. Cell Biol. 2021, 25, 19079–19098. [Google Scholar]
- Gutkind, J.S.; Molinolo, A.A.; Wu, X.; Wang, Z.; Nachmanson, D.; Harismendy, O.; Alexandrov, L.B.; Wuertz, B.R.; Ondrey, F.G.; Laronde, D. Inhibition of mTOR signaling and clinical activity of metformin in oral premalignant lesions. JCI Insight 2021, 6, e147096. [Google Scholar] [CrossRef]
- Siddappa, G.; Kulsum, S.; Ravindra, D.R.; Kumar, V.V.; Raju, N.; Raghavan, N.; Sudheendra, H.V.; Sharma, A.; Sunny, S.P.; Jacob, T. Curcumin and metformin-mediated chemoprevention of oral cancer is associated with inhibition of cancer stem cells. Mol. Carcinog. 2017, 56, 2446–2460. [Google Scholar] [CrossRef]
- Benner, S.E.; Winn, R.J.; Lippman, S.M.; Poland, J.; Hansen, K.S.; Luna, M.A.; Hong, W.K. Regression of oral leukoplakia with α-tocopherol: A community clinical oncology program chemoprevention study. JNCI J. Natl. Cancer Inst. 1993, 85, 44–47. [Google Scholar] [CrossRef]
- Kaugars, G.E.; Silverman, S., Jr.; Lovas, J.G.; Brandt, R.B.; Riley, W.T.; Dao, Q.; Singh, V.N.; Gallo, J. A clinical trial of antioxidant supplements in the treatment of oral leukoplakia. Oral Surg. Oral Med. Oral Pathol. 1994, 78, 462–468. [Google Scholar] [CrossRef]
- Behura, S.S.; Singh, D.K.; Masthan, K.; Babu, N.A.; Sah, S. Chemoprevention of oral cancer: A promising venture. Int J Oral Care Res 2015, 3, 80–87. [Google Scholar]
- Chang, P.-Y.; Peng, S.-F.; Lee, C.-Y.; Lu, C.-C.; Tsai, S.-C.; Shieh, T.-M.; Wu, T.-S.; Tu, M.-G.; Chen, M.Y.; Yang, J.-S. Curcumin-loaded nanoparticles induce apoptotic cell death through regulation of the function of MDR1 and reactive oxygen species in cisplatin-resistant CAR human oral cancer cells. Int. J. Oncol. 2013, 43, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Mazzarino, L.; Loch-Neckel, G.; Bubniak, L.d.S.; Mazzucco, S.; Santos-Silva, M.C.; Borsali, R.; Lemos-Senna, E. Curcumin-loaded chitosan-coated nanoparticles as a new approach for the local treatment of oral cavity cancer. J. Nanosci. Nanotechnol. 2015, 15, 781–791. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).