

Therapeutic Efficacy of Adipose Tissue-Derived Components in Neuropathic Pain: A Systematic Review

 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection and Data Collection
2.5. Data Extraction
2.6. Risk of Bias in Individual Studies
3. Results
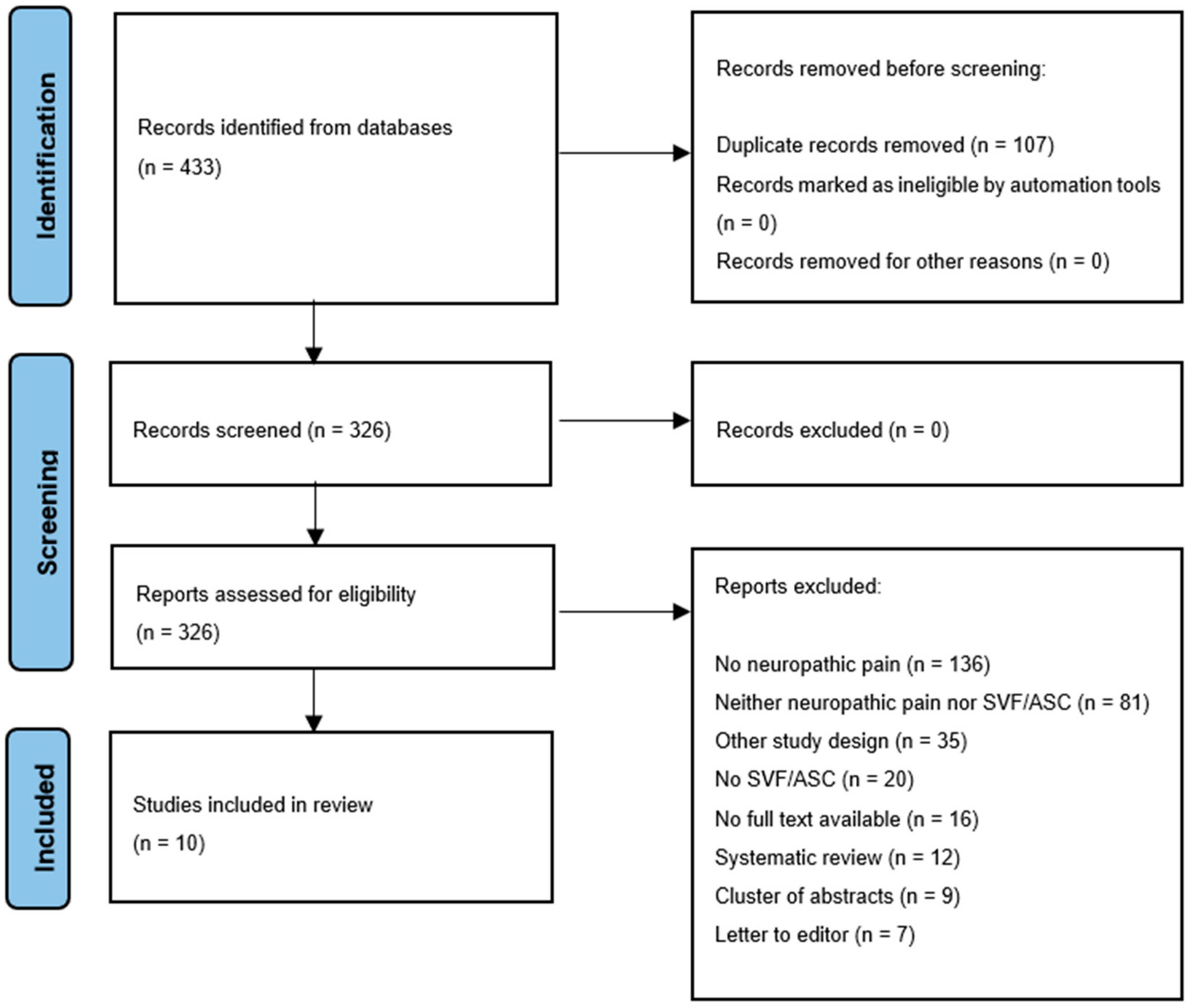
3.1. Study Selection
3.2. Study Characteristics
3.3. Included Studies
3.3.1. Post-Mastectomy Pain Syndrome
3.3.2. Euromas
3.3.3. Post-Herpetic Neuralgia
3.3.4. Neuropathic Scar Pain
3.3.5. Trigeminal Neuropathic Pain
3.3.6. Neuropathic Pain without Any Apparent Cause
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 3, 1–19. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Kuner, R.; Jensen, T.S. Neuropathic Pain: From Mechanisms to Treatment. Physiol. Rev. 2021, 101, 259–301. [Google Scholar] [CrossRef]
- Baron, R.; Tolle, T.R.; Gockel, U.; Brosz, M.; Freynhagen, R. A cross-sectional cohort survey in 2100 patients with painful diabetic neuropathy and postherpetic neuralgia: Differences in demographic data and sensory symptoms. Pain 2009, 146, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.H.; Torrance, N. Epidemiology of Neuropathic Pain and Its Impact on Quality of Life. Curr. Pain Headache Rep. 2012, 16, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Corselli, M.; Chen, C.W.; Sun, B.; Yap, S.; Rubin, J.P.; Peault, B. The tunica adventitia of human arteries and veins as a source of mesenchymal stem cells. Stem Cells Dev. 2012, 21, 1299–1308. [Google Scholar] [CrossRef]
- Lin, G.; Garcia, M.; Ning, H.; Banie, L.; Guo, Y.L.; Lue, T.F.; Lin, C.S. Defining stem and progenitor cells within adipose tissue. Stem Cells Dev. 2008, 17, 1053–1063. [Google Scholar] [CrossRef]
- Yousof, S.M.; ElSayed, D.A.; El-Baz, A.A.; Sallam, H.S.; Abbas, F. Combined Treatment of Adipose Derived-Mesenchymal Stem Cells and Pregabalin Is Superior to Monotherapy for the Treatment of Neuropathic Pain in Rats. Stem Cells Int. 2021, 1, 8847110. [Google Scholar] [CrossRef] [PubMed]
- Perin, E.C.; Sanz-Ruiz, R.; Sánchez, P.L.; Lasso, J. Adipose-derived regenerative cells in patients with ischemic cardiomyopathy: The PRECISE Trial. Am. Heart J. 2014, 168, 88–95. [Google Scholar] [CrossRef]
- van Dongen, J.A.; Tuin, A.J.; Spiekman, M.; Jansma, J.; van der Lei, B.; Harmsen, M.C. Comparison of intraoperative procedures for isolation of clinical grade stromal vascular fraction for regenerative purpose: A systematic review. J. Tissue Eng. Regen. Med. 2017, 12, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Pak, J.; Lee, J.H.; Kartalo, W.A. Cartilage Regeneration in Human with Adipose Tissue-Derived Stem Cells: Current Status in Clinical Implications. BioMed Res. Int. 2016, 12, e261–e274. [Google Scholar] [CrossRef] [PubMed]
- Zuk, P.A.; Zhu, M.I.N.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage cells from human adipose tissue: Implications for cell-based therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef] [PubMed]
- Bourin, P.; Bunnell, B.A.; Casteilla, L.; Dominici, M.; Katz, A.J.; March, K.L.; Redl, H.; Rubin, J.P.; Yoshimura, K.; Gimble, J.M. Stromal cells from the adipose tissue-derived stromal vascular fraction and culture expanded adipose tissue-derived stromal/stem cells: A joint statement of the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy 2013, 15, 641–648. [Google Scholar] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Beugels, J.; Hommes, J.E.; Balthasar, A.J.R.; van der Hulst, R. Autologous Fat Transfer as a Treatment for Peripheral Neuropathic Pain without Apparent Cause. Plast. Reconstr. Surg. Glob. Open 2018, 166, 1905. [Google Scholar] [CrossRef] [PubMed]
- Calcagni, M.; Zimmermann, S.; Scaglioni, M.F.; Giesen, T. The novel treatment of SVF-enriched fat grafting for painful end-neuromas of superficial radial nerve. Microsurgery 2018, 38, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Caviggioli, F.; Maione, L.; Forcellini, D.; Klinger, F.; Klinger, M. Autologous fat graft in postmastectomy pain syndrome. Plast. Reconstr. Surg. 2011, 128, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Caviggioli, F.; Maione, L.; Klinger, F.; Lisa, A.; Klinger, M. Autologous Fat Grafting Reduces Pain in Irradiated Breast: A Review of Our Experience. Stem Cells Int. 2016, 2016, 2527349. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.H.; Wu, S.H.; Chang, K.P.; Lin, C.H.; Chang, C.H.; Wu, Y.C.; Lee, S.S.; Lin, S.D.; Lai, C.S. Alleviation of neuropathic scar pain using autologous fat grafting. Ann. Plast. Surg. 2015, 74, S99–S104. [Google Scholar] [CrossRef]
- Juhl, A.A.; Karlsson, P.; Damsgaard, T.E. Fat grafting for alleviating persistent pain after breast cancer treatment: A randomized controlled trial. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 1192–1202. [Google Scholar] [CrossRef] [PubMed]
- Lisa, A.V.E.; Murolo, M.; Maione, L.; Vinci, V.; Battistini, A.; Morenghi, E.; De Santis, G.; Klinger, M. Autologous fat grafting efficacy in treating PostMastectomy pain syndrome: A prospective multicenter trial of two Senonetwork Italia breast centers. Breast J. 2020, 26, 1652–1658. [Google Scholar] [CrossRef] [PubMed]
- Sollie, M.; Thomsen, J.B.; Sørensen, J.A. Autologous fat grafting seems to alleviate postherpetic neuralgia—A feasibility study investigating patient-reported levels of pain. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Sollie, M.; Toyserkani, N.M.; Bille, C.; Thomsen, J.B.; Sørensen, J.A. Autologous Fat Grafting as Treatment of Postmastectomy Pain Syndrome: A Randomized Controlled Trial. Plast. Reconstr. Surg. 2022, 149, 295–305. [Google Scholar] [CrossRef]
- Vickers, E.R.; Karsten, E.; Floor, J.; Lilischkis, R. A preliminary report on stem cell therapy for neuropathic pain in humans. J. Pain Res. 2014, 7, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Ashjian, P.H.; Elbarbary, A.S.; Edmonds, B.; DeUgarte, D.; Zhu, M.; Zuk, P.A.; Lorenz, P.H.; Benhaim, P.; Hedrick, M.H. In vitro differentiation of human processed lipoaspirate cells into early neuroal progenitors. Plast. Reconstr. Surg. 2003, 111, 1922–1931. [Google Scholar] [CrossRef] [PubMed]
- Safford, K.M.; Safford, S.D.; Gimble, J.M.; Shetty, A.K.; Rice, H.E. Characterization of neuronal/glial differentiation of murine adipose-derived adult stromal cells. Exp. Neurol. 2004, 187, 319–328. [Google Scholar] [CrossRef]
- Choi, J.; Kim, S.; Jung, J.; Lim, Y.; Kang, K.; Park, S.; Kang, S. Wnt5a-mediating neurogenesis of human adipose tissue-derived stem cells in a 3D microfluidic cell culture system. Biomaterials 2011, 32, 7013–7022. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Rey, E.; Gonzalez, M.A.; Varela, N.; O’Valle, F.; Hernandez-Cortes, P.; Rico, L.; Büscher, D.; Delgado, M. Human adipose-derived mesenchymal stem cells reduce inflammatory and T cell responses and induce regulatory T cells in vitro in rheumatoid arthritis. Annu. Rheum. Dis. 2010, 69, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Yañez, R.; Lamana, M.L.; García-Castro, J.; Colmenero, I.; Ramírez, M.; Bueren, J.A. Adipose tissue-derived mesenchymal stem cells have in vivo immunosuppressive properties applicable for the control of the graft-versus-host disease. Stem Cells 2006, 24, 2582–2591. [Google Scholar] [CrossRef]
- Puissant, B.; Barreau, C.; Bourin, P.; Clavel, C.; Corre, J.; Bousquet, C.; Taureau, C.; Cousin, B.; Abbal, M.; Laharrague, P.; et al. Immunomodulatory effect of human adipose tissue-derived adult stem cells: Comparison with bone marrow mesechymal stem cells. Br. J. Haematol. 2005, 129, 118–129. [Google Scholar] [CrossRef]
- Kim, Y.K.; Na, K.S.; Myint, A.M.; Leonard, B.E. The role of pro-inflammatory cytokines in neuroinflammation, neurogenesis and the neuroendocrine system in major depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2015, 64, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Martucci, C.; Trovato, A.E.; Costa, B.; Borsani, E.; Franchi, S.; Magnaghi, V.; Panerai, A.E.; Rodella, L.F.; Valsecchi, A.E.; Sacerdote, P.; et al. The purinergic antagonist PPADS reduces pain related behaviours and interleukin-1 beta, interleukin-6, iNOS and nNOS overproduction in central and peripheral nervous system after peripheral neuropathy in mice. Pain 2008, 137, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Valsecchi, A.E.; Franchi, S.; Panerai, A.E.; Sacerdote, P.; Trovato, A.E.; Colleoni, M. Genistein, a natural phytoestrogen from soy, relieves neuropathic pain following chronic constriction sciatic nerve injury in mice: Anti-inflammatory and antioxidant activity. J. Neurochem. 2008, 107, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Sacerdote, P.; Niada, S.; Franchi, S.; Arrigoni, E.; Rossi, A.; Yenagi, V.; de Girolamo, L.; Panerai, A.E.; Brini, A.T. Systemic Administration of Human Adipose Derived Stem Cells Reverts Nociceptive Hypersensitivity in an Experimental Model of Neuropathy. Stem Cells Dev. 2013, 22, 8. [Google Scholar] [CrossRef] [PubMed]
- van Dongen, J.A.; Getova, V.; Brouwer, L.A.; Liguori, G.R.; Sharma, P.K.; Stevens, H.P.; van der Lei, B.; Harmsen, M.C. Adipose tissue-derived extracellular matrix hydrogels as a release platform for secreted paracrine factors. J. Tissue Eng. Regen. Med. 2019, 13, 973–985. [Google Scholar] [CrossRef] [PubMed]
- Santiago, L.Y.; Clavijo-Alvarez, J.; Brayfield, C.; Rubin, J.P.; Marra, K.G. Delivery of Adipose-Derived Precursor Cells for Peripheral Nerve Repair. Cell Transplant. 2009, 18, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration, HHS. Public Health Service Act (PHS Act), under 21 CFR Part 1271, Section 361. Available online: https://www.ecfr.gov/current/title-21/chapter-I/subchapter-L/part-1271 (accessed on 1 January 2024).
- Forouzanfar, F.; Amin, B.; Ghorbani, A.; Ghazavi, H.; Ghasemi, F.; Sadri, K.; Mehri, S.; Sadeghnia, H.R.; Hosseinzadeh, H. New approach for the treatment of neuropathic pain: Fibroblast growth factor 1 gene-transfected adipose-derived mesenchymal stem cells. Eur. J. Pain 2018, 22, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Forouzanfar, F.; Sadeghnia, H.R.; Hoseini, S.J.; Ghorbani, A.; Ghazavi, H.; Ghasemi, F.; Hosseinzadeh, H. Fibroblast Growth Factor 1 Gene-Transfected Adipose-Derived Mesenchymal Stem Cells Modulate Apoptosis and Inflammation in the Chronic Constriction Injury Model of Neuropathic Pain. Iran. J. Pharm. Res. 2020, 19, 151–159. [Google Scholar] [PubMed]
- Mohammadi, R.; Azizi, S.; Delirezh, N.; Hobbenaghi, R.; Amini, K. Comparison of beneficial effect of undifferentiated cultured bone marrow stromal cells and omental adipose-derived nucleated cell fractions on sciatic nerve regeneration. Muscle Nerve 2022, 43, 157–163. [Google Scholar] [CrossRef]
- Oses, C.; Olivares, B.; Ezquer, M.; Acosta, C.; Bosch, P.; Donoso, M.; Léniz, P.; Ezquer, F. Preconditioning of adipose tissue-derived mesenchymal stem cells with deferoxamine increases the production of proangiogenic, neuroprotective and anti-inflammatory factors: Potential application in the treatment of diabetic neuropathy. PLoS ONE 2017, 12, e017011. [Google Scholar] [CrossRef]

{kind=link}
| Beugels et al., 2018 [15] | Calcagni et al., 2016 [16] | Caviggioli et al., 2011 [17] | Caviggioli et al., 2016 [18] | Huang et al., 2015 [19] | Juhl et al., 2016 [20] | Lisa et al., 2020 [21] | Sollie et al., 2020 [22] | Sollie et al., 2022 [23] | Vickers et al., 2014 [24] | |
|---|---|---|---|---|---|---|---|---|---|---|
| A clearly stated aim | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 1 | 1 | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 |
| Prospective collection of data | 1 | 1 | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 |
| Endpoints appropriate to the aim of the study | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study endpoint | 0 | 0 | 2 | 2 | 0 | 2 | 0 | 0 | 2 | 0 |
| Follow-up period appropriate to the aim of the study | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 1 |
| Loss to follow-up less than 5% | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Prospective calculation of the study size | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 2 | 0 |
| Only for comparative studies | ||||||||||
| An adequate control group | 1 | 1 | 2 | 2 | ||||||
| Contemporary groups | 2 | 2 | 2 | 2 | ||||||
| Baseline equivalence of groups | 1 | 1 | 1 | 1 | ||||||
| Adequate statistical analyses | 1 | 1 | 2 | 2 | ||||||
| Total MINORS score | 6 | 8 | 18 | 17 | 8 | 20 | 9 | 7 | 20 | 10 |
| Maximum possible score | 16 | 16 | 24 | 24 | 16 | 24 | 16 | 16 | 24 | 16 |
| Author (Year) | Study Design | N total (F) | Indication | Treatment | Age (Years) | Outcome | Follow Up (W/M) | Conclusion |
|---|---|---|---|---|---|---|---|---|
| Beugels et al., 2018 [15] | RCS | 14 (8) | NP e.c.i | AFG | 51 (17–78) | Tinel’s sign, VAS, patient satisfaction, quality of sleep. | 2M 28M | AFG decreased treatment refractory NP. No conclusions can be drawn on patient-reported satisfaction and quality of sleep as they were not statistically tested. |
| Calcagni et al., 2016 [16] | RCS | 5 (0) | Painful neuromas of radial nerve | Microsurgical resection SVF-enriched FG | 49.8 ± 16.6 | Subjective outcomes, overall pain score. | 1M 6M 12M 36M | SVF-enriched FG did not reduce NP but tended to reduce NP over time. |
| Caviggioli et al., 2011 [17] | PSS | 113 (113) | PMPS + scar retraction | AFG | NR | VAS Analgesic drug intake. | 12M | AFG with scar retraction reduced NP. 28 out of 34 patients quit their analgesic drug therapy in the AFG treated group. |
| Caviggioli et al., 2016 [18] | PSS | 209 (209) | PMPS | AFG | NR | VAS Analgesic drug intake. | 12M | AFG reduced NP. 48 out of 120 patients quit their analgesic drug therapy in the AFG treated group. |
| Huang et al., 2015 [19] | PSS | 13 (4) | Scar pain | AFG | 33.1 ± 16.4 | VAS, NPSI. | 1W 1M 6M | AFG reduced NP. |
| Juhl et al., 2016 [20] | RCT | 15 (15) | PMPS | AFG | T 58.9 ± 7.4 C 59.9 ± 9.8 | DoloTest, VAS, NPSI, POSAS. | 3M 6M | AFG reduced NP. Health-related QoL and scar quality improved. |
| Lisa et al., 2020 [21] | PMS | 37 (37) | PMPS | AFG | 48 ± 6.2 | VAS, POSAS. | 1M 3M 6M | AFG significantly reduced NP and improved scar quality. |
| Sollie et al., 2020 [22] | PSS | 10 (NR) | Post-herpetic neuralgia | AFG | 76 (53–94) | VAS, NPSI, SF-36. | 3M | AFG reduced NP on all parameters. QoL did not improve (SF-36). |
| Sollie et al., 2022 [23] | RCT | 35 (35) | PMPS | Scar release AFG | 63.8 ± 9.9 | NRS, NPSI, SF-36. | 3M 6M | AFG did not reduce NP. QoL significantly improved in the control group and detoriated after AFG (on emotional parameters). |
| Vickers et al., 2014 [24] | PSS | 10 (10) | Trigeminal pain | cSVF | 55.3 ± 14.7 | NRS Dosage of NP medication | 6M | cSVF reduced NP. Dosage of NP medication tended to reduce over time. |
| Author (Year) | Donor Site | Process | Injection Layer | Volume Injected |
|---|---|---|---|---|
| Beugels et al., 2018 [15] | Abdomen | NR | NR | NR |
| Caviggioli et al., 2011 [17] | Abdomen | Centrifugation 3000 rpm for 5 min. | Dermo-hypodermal junction | NR |
| Caviggioli et al., 2016 [18] | Abdomen | Centrifugation 3000 rpm for 5 min. | Dermo-hypodermal junction | 52 ± 8.9 cc |
| Huang et al., 2015 [19] | Abdomen | Centrifugation 3000 rpm for 3 min. | Rigottomy Dermal-hypodermal junction | 2.25 mL (range 0.3–14.0) |
| Juhl et al., 2016 [20] | Abdomen | Centrifugation 1800 rpm for 3 min. | Rigottomy Dermal-hypodermal junction | 71 ± 24.6 mL |
| Lisa et al., 2020 [21] | Hips | Centrifugation 837× g for 5 min. | Dermal-hypodermal junction | NR |
| Sollie et al., 2020 [22] | Abdomen Thighs | Centrifugation 10 min. Speed NR. | Dermal-hypodermal junction | 208 mL (range 100–300) |
| Sollie et al., 2022 [23] | NR | NR | Rigottomy Subdermal area | NR |
| Author (Year) | Donor Site | Laboratory Process | Injection Layer | Volume Injected |
|---|---|---|---|---|
| Calcagni et al., 2016 [16] | NR | Transferring lipoaspirate to the Celution 800/CRS System followed by adding one ampule of Celase enzyme reagent to isolate SVF. | Perineural area | A mixture of 5 mL concentrated SVF and 2 mL aspirated and sedimented lipid fraction. |
| Vickers et al., 2014 [24] | Bilateral lumbar region | Adding collagenase digestion of human grade collagenase to the lipoaspirate to isolate cSVF. Followed by the centrifugation in sterile saline-containing vancomycin. | Perineural area | NR |
| Patients | Author (Year) | Intervention | Preoperative Outcome Measure | Postoperative Outcome Measure | Δ Pre- and Postoperative | Significance |
|---|---|---|---|---|---|---|
| 14 | Beugels et al., 2018 [15] | T: AFG in areas with demarcated NP (n = 14) C: N/A | T: VAS 7.4 (range 6.0–10.0) | T 2M: VAS 3.8 (range 0–8.0) T 6M: VAS 4.3 (range 0–10.0) | 3.6 ↓ 3.1 ↓ | p < 0.0001 p < 0.0017 |
| 5 | Calcagni et al., 2016 [16] | T: Microsurgical resection + SVF-enriched FG (n = 5) C: N/A | T: Overall Pain Score (OPS) 2.2 ± 1.0 | T 2M: OPS 1.3 ± 1.2 T 6M: OPS 1.5 ± 1.5 T 12M: OPS 1.6 ± 1.4 T 36M: OPS 1.4 ± 1.3 | 0.9 ↓ 0.7 ↓ 0.6 ↓ 0.8 ↓ | p = 0.225 p = 0.345 p = 0.345 p = 0.104 |
| 113 | Caviggioli et al., 2011 [17] | T: AFG in areas of NP + scars (n = 63) C: No intervention (n = 35) | T: VAS NR C: VAS NR | T 13M: VAS NR C 13M: VAS NR | 3.2 ± 3.0 ↓ 1.0 ± 2.7 ↓ | p = 0.0005 p = NR |
| 190 | Caviggioli et al., 2016 [18] | T: AFG in irradiated areas (n = 120) C: No intervention (n = 70) | T: VAS 7.2 ± 2.1 C: VAS 6.9 ± 2.2 | T 12M: VAS 3.3 ± 3.1 C 12M: VAS 5.8 ± 1.9 | 3.2 ± 2.9 ↓ 1.1 ± 2.7 ↓ | p < 0.005 p > 0.05 |
| 13 | Huang et al., 2015 [19] | T: AFG in affected areas (n = 13) C: N/A | T: VAS 7.5 ± 1.1 NPSI 49.4 ± 13.3 | T 1W: VAS 3.1 ± NR NPSI 25.0 ± 14.0 | VAS 4.4 ± 1.7 ↓ NPSI 24.4 ± NR ↓ | p = 0.009 VAS p = 0.004 NPSI |
| T 1M: VAS 2.1 ± NR NPSI 21.0 ± 17.8 | VAS 5.4 ± 2.1 ↓ NPSI 28.4 ± NR ↓ | p = 0.008 VAS p = 0.0009 NPSI | ||||
| T 6M: VAS 1.9 ± NR NPSI 14.6 ± 16.9 | VAS 5.6 ± 2.2 ↓ NPSI 34.8 ± NR ↓ | p = 0.007 VAS p = 0.0008 NPSI | ||||
| 15 | Juhl et al., 2016 [20] | T: AFG in painful areas (n= 8) C: Analgesic therapy (n= 7) | T: NR C: NR | T 3M: DoloTest NR VAS NR NPSI NR | DoloTest 220 ↓ (95% CI 146–294) VAS 36.0 ↓ (95% CI 27.1–44.9) NPSI 12.9 ↓ (95% CI 9.6–17.8) | p < 0.001 DoloTest p < 0.01 VAS p < 0.001 NPSI |
| T 6M: DoloTest NR VAS NR NSPI NR | DoloTest 202 ↓ (95% CI 98–304) VAS 35.8 ↓ (95% CI 20.6–50.9) NPSI 13.7 ↓ (95% CI 9.6–17.8) | p < 0.001 DoloTest p < 0.01 VAS p < 0.001 NPSI | ||||
| C 3M: DoloTest NR VAS NR NPSI NR | DoloTest No change VAS No change NPSI No change | p = 0.36 DoloTest p = 0.43 VAS p = 0.55 NPSI | ||||
| C 6M: DoloTest NR VAS NR NPSI NR | DoloTest No change VAS No change NPSI No change | p = 0.25 DoloTest p = 0.28 VAS p = 0.68 NPSI | ||||
| 37 | Lisa et al., 2020 [21] | T: AFG in area of NP (n = 37) C: N/A | T: VAS 6.9 ± 1.3 | T 1M: VAS 3.8 ± 1.6 T 3M: VAS 3.0 ± 1.6 T 6M: VAS 2.6 ± 2.1 | VAS 3.1 ± NR ↓ VAS 3.9 ± NR ↓ VAS 4.3 ± NR ↓ | p < 0.001 p < 0.005 p = NR |
| 10 | Sollie et al., 2020 [22] | T: AFG to dermal area of neuralgia (n = 10) C: N/A | T: VAS average 7.0 ± 1.6 VAS max. 8.6 ± 1.3 NPSI average 5.8–7.2 ± 1.8–3.2 SF-36 pain 38.8 ± 28.4 | T 3M: VAS average 3.0 ± 3.0 VAS max. 3.5 ± 3.1 NPSI average 1.9–3.0 ± 2.2–3.1 SF-36 pain 49.8 ± 26.4 | VAS average 4.0 ± 3.1 ↓ VAS max. 5.1 ± 3.9 ↓ NPSI average 3.2–4.5 ± 3.1–4.9 ↓ SF-36 pain 11.0 ± 39.7 ↑ | p < 0.05 VAS p < 0.05 VAS p < 0.05 NPSI average p = 0.40 SF-36 pain |
| 35 | Sollie et al., 2022 [23] | T: Scar releasing rigottomy + AFG (n = 18) C: Scar releasing rigottomy + saline injection (n = 17) | T: NRS average 5.3 (95% CI 4.6–6.0) NRS max 6.6 (95% CI 5.9–7.4) NPSI average calculated 3.3 (95% CI) SF-36 pain 53.9 (95% CI 45.3–62.4) C: NRS average 5.3 (95% CI 4.4–6.2) NRS max 7.1 (95% CI 6.3–8.0) NPSI average calculated 4.1 (CI 95%) SF-36 pain 49.1 (CI 95% 42.6–55.7) | T 3M: NRS average 4.1 (95% CI 2.9–5.3) NRS max 5.8 (95% CI 4.8–6.8) NPSI average calculated 2.8 (95% CI) SF-36 pain NR | NRS average 1.2 ± NR ↓ NRS max 0.8 ± NR ↓ NPSI average calculated 0.7 ↑ SF-36 pain NR | p = NSD for NRS, NPSI and SF-36 after 3M and 6M compared to baseline |
| T 6M: NRS average 4.3 (95% CI 3.1–5.4) NRS max 5.7 (95% CI 4.4–7.0) NPSI average calculated 2.7 (95% CI) SF-36 pain 57.1 (46.6–67.5) | NRS average 1.0 ± NR ↓ NRS max 0.9 ± NR ↓ NPSI average range 2.0–0.2 ↓ SF-36 pain 3.2 ↓ | |||||
| C 3M: NRS average 4.7 (95% CI 3.5–5.9) NRS max 6.3 (95% CI 5.0–7.5) NPSI NR SF-36 pain NR | NRS average 0.6 ± NR ↓ NRS max 0.8 ± NR ↓ NPSI NR SF-36 NR | |||||
| C 6M: NRS average 4.3 (95% CI 3.1–5.4) NRS max 5.9 (95% CI 4.6–7.2) NPSI NR SF-36 pain 52.1 (95% CI 42.1–62.0) | NRS 1.0 ± NR ↓ NRS 1.2 ± NR ↓ NPSI NR SF-36 pain NR | |||||
| 10 | Vickers et al., 2014 [24] | T: cSVF in facial NP (n = 10) C: N/A | T: NRS 7.5 ± 1.6 | T 6M: NRS 4.3 ± 3.3 | 3.2 ± NR ↓ | p = 0.018 |
| Topic | Recommendations |
|---|---|
| Study quality | 1. Controlled (comparison with gold standard or placebo) 2. Randomized 3. Follow up 12 months 4. Statistical testing for differences between groups |
| Procedure standardization | 1. Standardize AFG, SVF or ASCs harvesting, processing and injection technique 2. Document and correct for fat specific characteristic such as gender, BMI, smoking and co-morbidities e.g., diabetes 3. Standardize injected volume per surface area. In case of supplemented-AFG: standardized volume-to volume ratio 4. Avoid concomitant procedures or correct for them |
| Pain measurements | 1. Define pain and pain reduction. Standardize follow-up moments 2. Use valid pain outcome measures (VAS *, NPSI **) 3. Report on all possible bias on pain experience e.g., use of analgesia, pain blocking procedures, psychological factors |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claessens, A.A.E.; Vriend, L.; Ovadja, Z.N.; Harmsen, M.C.; van Dongen, J.A.; Coert, J.H. Therapeutic Efficacy of Adipose Tissue-Derived Components in Neuropathic Pain: A Systematic Review. Bioengineering 2024, 11, 992. https://doi.org/10.3390/bioengineering11100992
Claessens AAE, Vriend L, Ovadja ZN, Harmsen MC, van Dongen JA, Coert JH. Therapeutic Efficacy of Adipose Tissue-Derived Components in Neuropathic Pain: A Systematic Review. Bioengineering. 2024; 11(10):992. https://doi.org/10.3390/bioengineering11100992
Chicago/Turabian StyleClaessens, Anouk A. E., Linda Vriend, Zachri N. Ovadja, Martin C. Harmsen, Joris. A. van Dongen, and J. Henk Coert. 2024. "Therapeutic Efficacy of Adipose Tissue-Derived Components in Neuropathic Pain: A Systematic Review" Bioengineering 11, no. 10: 992. https://doi.org/10.3390/bioengineering11100992
APA StyleClaessens, A. A. E., Vriend, L., Ovadja, Z. N., Harmsen, M. C., van Dongen, J. A., & Coert, J. H. (2024). Therapeutic Efficacy of Adipose Tissue-Derived Components in Neuropathic Pain: A Systematic Review. Bioengineering, 11(10), 992. https://doi.org/10.3390/bioengineering11100992