
Qualitative Exploration of Anesthesia Providers’ Perceptions Regarding Philips Visual Patient Avatar in Clinical Practice


 ,
,  and
and
Abstract

1. Introduction
2. Materials and Methods
2.1. Approval and Consent
2.2. Implementation of Philips Visual Patient Avatar in the Study Center
2.3. Study Design
2.4. Online Questionnaire
2.5. Accounting for Bias
2.6. Reflexivity
2.7. Data Analysis
2.7.1. Open-Ended Questions
2.7.2. Demographic Data
3. Results
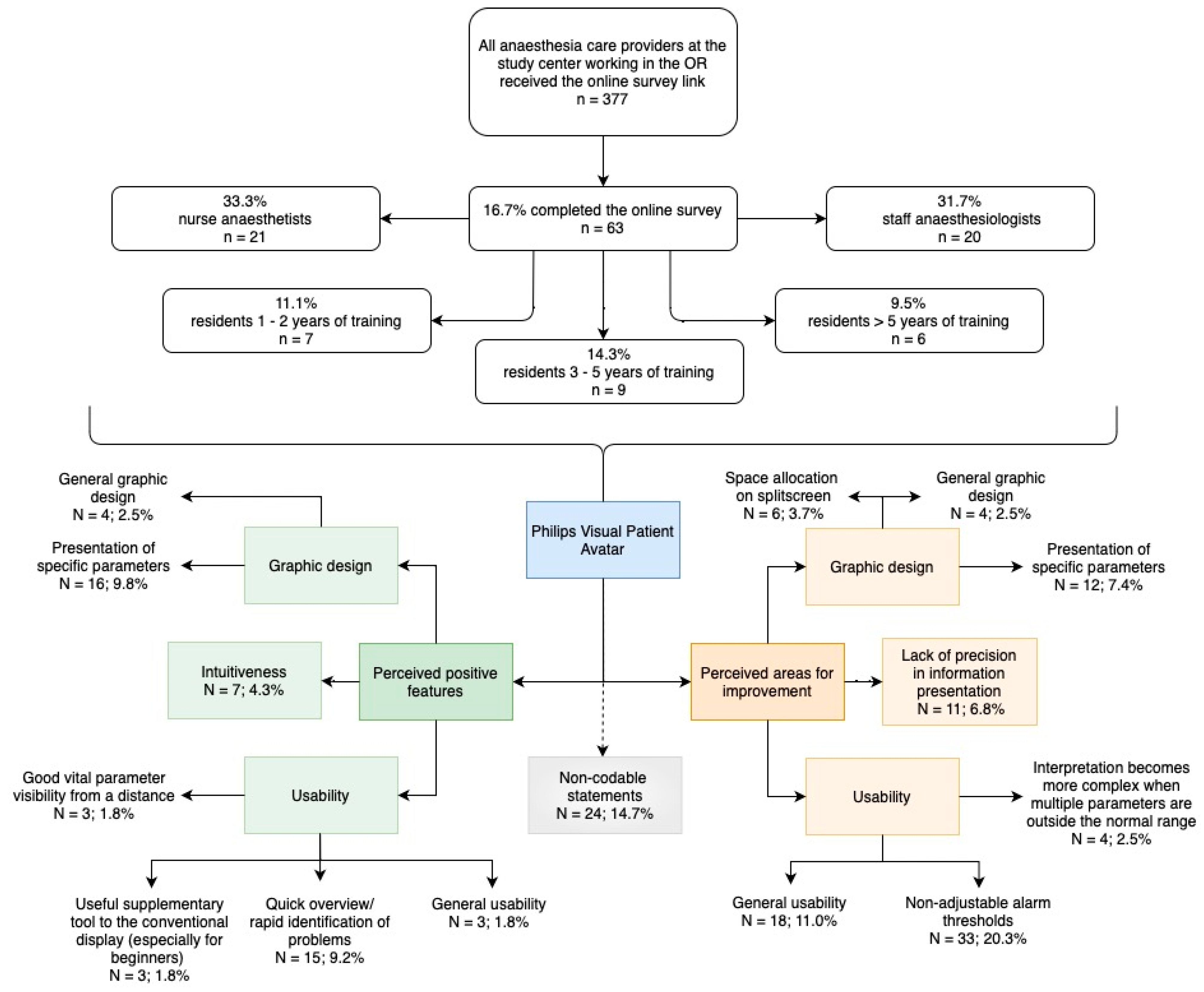
3.1. Participant Characteristics
3.2. Statements about Philips Visual Patient Avatar
3.2.1. Perceived Positive Features of Philips Visual Patient Avatar from Anesthesia Providers’ Perspective
Favorable Usability Characteristics
Visual Patient gives me the ability to quickly identify all problems in a dynamic situation.(Participant 16)
Visual Patient provides a quick overview, especially when things get hectic, without triggering alarms.(Participant 24)
Good visibility of alarms, even from a greater distance.(Participant 9)
Pathologies can be easily detected from a distance.(Participant 35)
A tool that can be helpful, especially for beginners.(Participant 45)
A good addition to the numerical display.(Participant 19)
Appealing Graphic Design
I notice when Visual Patient shows a low temperature or poor saturation because the visual appearance changes significantly.(Participant 27)
I like the easier identification of ST changes.(Participant 33)
Intuitiveness
I like the intuitive understanding of my patient’s circulation.(Participant 32)
The visual representation is intuitive and easy to understand.(Participant 63)
3.2.2. Perceived Areas of Improvement of Philips Visual Patient Avatar from Anesthesia Providers’ Perspective
Identified Areas for Usability Enhancement
Ability to independently adjust limits would be great, so that values that are too high or too low could be adjusted for the individual patient.(Participant 13)
Alarm thresholds need to be adjustable. For example, in thoracic surgery, a “blue” patient with SpO2 92% is often more confusing than helpful.(Participant 63)
If multiple parameters deviate near the limits, the overview is lost because too many stimuli are displayed at the same time.(Participant 30)
When displaying multiple parameters (in ICU patients, neurosurgery, cardiac surgery), it becomes bothersome.(Participant 1)
Potential Avenues for Enhancing Graphic Design
The current visual representation during tachycardia is too hectic. I cannot work with the VP for tachycardic patients. It is like a stroboscope.(Participant 32)
The eyes are spooky.(Participant 57)
It takes up too much space on the monitor.(Participant 5)
A larger portion of the split monitor should be dedicated to curves and measurements that are incorporated into the avatar.(Participant 7)
Lack of Precision in Presenting Information
I would like to see more gradations, for example, in cases of hyper- or hypotension or SpO2 (not just good or bad or more than 2 colors).(Participant 17)
Integration of trends (e.g., temperature).(Participant 10)
E.g., The monitors often have problems.(Participant 20)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vital-Sign Presentation | ||
|---|---|---|
| Vital Sign | Conventional Monitoring Presentation | Philips Visual Patient Avatar |
| Pulse rate | Numeric, auditory QRS signal | Heart and body silhouettes pulse at different speeds: slow, normal, and fast |
| Arterial blood pressure | Waveform, numeric | Body expands/contracts slightly, normally, or intensely beyond “normal line” |
| Central venous pressure | Waveform; numeric | Vena cava size small, normal, or large beyond the white “normal line” |
| Respiratory rate | Numeric | Lungs expand/contract at slow, normal, or fast rates; CO2 cloud exhaled synchronously (if data from a CO2 sensor are available) |
| Tidal volume | Waveform, numeric | Lungs reach just barely, normally, or far beyond the white “normal line” |
| Expiratory CO2 concentration | Waveform, numeric | CO2 cloud just barely visible, normal, or extends beyond the white “normal line” |
| Body temperature | Numeric | Heatwaves or ice crystals around avatar |
| Brain activity | Waveform, numeric | Eyes open or closed |
| Peripheral oxygen saturation | Numeric, auditory QRS signal | Healthy or purple skin color |
| Neuromuscular function | Numeric | Extremities and thumbs extended or floppy |
| Electrocardiography ST-segment | Waveform, numeric | Heart muscle vivid red or dark purple |
References
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, D.A.; Witkowsk, E.; Gao, L.; Meireles, O.; Rosman, G. Artificial Intelligence in Anesthesiology: Current Techniques, Clinical Applications, and Limitations. Anesthesiology 2020, 132, 379–394. [Google Scholar] [CrossRef]
- Gelb, A.W.; Morriss, W.W.; Johnson, W.; Merry, A.F. World Health Organization-World Federation of Societies of Anaesthesiologists (WHO-WFSA) International Standards for a Safe Practice of Anesthesia. Can. J. Anaesth. 2018, 65, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-resuscitation care. Resuscitation 2021, 161, 220–269. [Google Scholar] [CrossRef] [PubMed]
- Kipnis, E.; Ramsingh, D.; Bhargava, M.; Dincer, E.; Cannesson, M.; Broccard, A.; Vallet, B.; Bendjelid, K.; Thibault, R. Monitoring in the intensive care. Crit. Care Res. Pract. 2012, 2012, 473507. [Google Scholar] [CrossRef] [PubMed]
- Fraser, K.L.; Ayres, P.; Sweller, J. Cognitive load theory for the design of medical simulations. Simul. Healthc. 2015, 10, 295–307. [Google Scholar] [CrossRef]
- Johnson, K.R.; Hagadorn, J.I.; Sink, D.W. Alarm safety and alarm fatigue. Clin. Perinatol. 2017, 44, 713–728. [Google Scholar] [CrossRef] [PubMed]
- Cvach, M. Monitor alarm fatigue: An integrative review. Biomed. Instrum. Technol. 2012, 46, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.M.; Burden, A.; Posner, K.L.; Mincer, S.L.; Steadman, R.; Wagner, K.J.; Domino, K.B. Frequency and Type of Situational Awareness Errors Contributing to Death and Brain Damage: A Closed Claims Analysis. Anesthesiology 2017, 127, 326–337. [Google Scholar] [CrossRef]
- Schulz, C.M.; Krautheim, V.; Hackemann, A.; Kreuzer, M.; Kochs, E.F.; Wagner, K.J. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesth. Anesthesiol. 2016, 16, 4. [Google Scholar] [CrossRef]
- Katz, D. Gestalt Psychology: Its Nature and Significance, 2nd ed.; Ronald Press Company: New York City, NY, USA, 1950. [Google Scholar]
- Wagemans, J.; Elder, J.H.; Kubovy, M.; Palmer, S.E.; Peterson, M.A.; Singh, M.; von der Heydt, R. A century of Gestalt psychology in visual perception: I. Perceptual grouping and figure–ground organization. Psychol. Bull. 2012, 138, 1172. [Google Scholar] [CrossRef]
- Kahneman, D. Thinking, Fast and Slow; Farrar, Straus and Giroux: New York City, NY, USA, 2011. [Google Scholar]
- Drews, F.A. Patient monitors in critical care: Lessons for improvement. In Advances in Patient Safety: New Directions and Alternative Approaches; Henriksen, K., Battles, J.B., Keyes, M.A., Grady, M.L., Eds.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008; Volume 3. Available online: https://www.ncbi.nlm.nih.gov/books/NBK43684/ (accessed on 21 March 2024).
- Tremper, K.K.; Mace, J.J.; Gombert, J.M.; Tremper, T.T.; Adams, J.F.; Bagian, J. Design of a Novel Multifunction Decision Support Display for Anesthesia Care: AlertWatch® OR. BMC Anesthesiol. 2018, 18, 16. [Google Scholar] [CrossRef]
- Hamilton Medical AG. The Ventilation Cockpit: The Dynamic Lung Panel. Available online: https://www.hamilton-medical.com/Products/Technologies/Ventilation-Cockpit.html (accessed on 21 March 2024).
- Mindray Medical International Limited. SV800/SV600 Ventilator: PulmoSight. Available online: https://www.mindray.com/en/products/ventilators/sv800-sv600 (accessed on 21 March 2024).
- Mindray Medical International Limited Clinical Information Leaflet: HemoSightTM. Available online: https://www.mindray.com/content/dam/xpace/en/resources/clinical-paper/HemoSight_Clinical_Information_Leaflet.pdf (accessed on 21 March 2024).
- Philips. Patient Monitoring: Visual Patient Avatar. Available online: https://www.philips.co.uk/healthcare/technology/visual-patient-avatar. (accessed on 27 February 2024).
- Gasciauskaite, G.; Lunkiewicz, J.; Roche, T.R.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Human-centered visualization technologies for patient monitoring are the future: A narrative review. Crit. Care 2023, 27, 254. [Google Scholar] [CrossRef]
- Roche, T.R.; Said, S.; Braun, J.; Maas, E.J.C.; Machado, C.; Grande, B.; Kolbe, M.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Avatar-based patient monitoring in critical anaesthesia events: A randomised high-fidelity simulation study. Br. J. Anaesth. 2021, 126, 1046–1054. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Handschin, L.; Neubauer, P.; Weiss, M.; Seifert, B.; Spahn, D.R.; Noethiger, C.B. Using an animated patient avatar to improve perception of vital sign information by anaesthesia professionals. Br. J. Anaesth. 2018, 121, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Endsley, M.R. Designing for Situation Awareness: An Approach to User-Centered Design, 2nd ed.; CRC Press Inc.: Boca Raton, FL, USA, 2011. [Google Scholar]
- Wittgestein, L. Tractatus Logico-Philosophicus; Routledge & Kegan Paul: London, UK, 1922. [Google Scholar]
- Degani, A.; Jorgensen, D.; Iverson, D.L.; Shafto, M.; Olson, L. On Organization of Information: Approach and Early Work; NASA Ames Research Center: Moffett Field, CA, USA, 2009.
- Hendra, R.; Hill, A. Rethinking Response Rates: New Evidence of Little Relationship between Survey Response Rates and Nonresponse Bias. Eval. Rev. 2019, 43, 307–330. [Google Scholar] [CrossRef]
- Elston, D.M. Participation bias, self-selection bias, and response bias. J. Am. Acad. Dermatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef]
- Olmos-Vega, F.M.; Stalmeijer, R.E.; Varpio, L.; Kahlke, R. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med. Teach. 2022, 45, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- O’Connor, C.; Joffe, H. Intercoder Reliability in Qualitative Research: Debates and Practical Guidelines. Int. J. Qual. Methods 2020, 19. [Google Scholar] [CrossRef]
- Akbas, S.; Said, S.; Roche, T.R.; Nöthiger, C.B.; Spahn, D.R.; Tscholl, D.W.; Bergauer, L. User Perceptions of Different Vital Signs Monitor Modalities during High-Fidelity Simulation: Semiquantitative Analysis. JMIR Hum. Factors 2022, 9, e34677. [Google Scholar] [CrossRef] [PubMed]
- Endsley, M.R. Theoretical underpinnings of situation awareness: A critical review. In Situation Awareness Analysis and Measurement; Endsley, M.R., Garland, D.J., Eds.; Lawrence Erlbaum Associates, Inc.: Mahwah, NJ, USA, 2000. [Google Scholar]
- Wetli, D.J.; Bergauer, L.; Nöthiger, C.B.; Roche, T.R.; Spahn, D.R.; Tscholl, D.W.; Said, S. Improving Visual-Patient-Avatar Design Prior to Its Clinical Release: A Mixed Qualitative and Quantitative Study. Diagnostics 2022, 12, 555. [Google Scholar] [CrossRef] [PubMed]
- Lunkiewicz, J.; Fries, D.; Milovanovic, P.; Noethiger, C.B.; Tscholl, D.W.; Gasciauskaite, G. Pediatric Anesthesia Providers’ Perspective on the Real-Life Implementation of the Philips Visual Patient Avatar: A Qualitative Study. Children 2023, 10, 1841. [Google Scholar] [CrossRef]
- Atieno, O.P. An analysis of the strengths and limitation of qualitative and quantitative research paradigms. Probl. Educ. 21st Century 2009, 13, 13–38. [Google Scholar]


| Participants (n = 63) | ||
|---|---|---|
| Sex | Female | 31 (49.2%) |
| Male | 29 (46.0%) | |
| Other gender identity | 3 (4.8%) | |
| Participant age in years | 20–35 | 23 (36.5%) |
| 36–50 | 32 (50.8%) | |
| 51–65 | 8 (12.7%) | |
| Work in anesthesia experience in years, median (IQR) | 8 (4–13.5) | |
| Role | Nurse anesthetist in training | 1 (1.6%) |
| Certified nurse anesthetist | 20 (31.7%) | |
| Resident 1–2 years of training | 7 (11.1%) | |
| Resident 3–5 years of training | 9 (14.3%) | |
| Resident with >5 years of experience | 6 (9.5%) | |
| Staff anesthesiologist | 20 (31.7%) | |
| Educational material consulted | Short manual only | 17 (27.0%) |
| Tutorial video only | 7 (11.1%) | |
| Both | 33 (52.4%) | |
| None | 6 (9.5%) | |
| Perceived Positive Features | |
| Usability (24/163; 14.6%) | |
| Quick overview/rapid identification of problems (15/163; 9.2%) | Quick overview of various parameters. (Participant 37) Problems are quickly and easily identified. (Participant 15) |
| Good vital parameters visibility from a distance (3/163; 1.8%) | Ability to assess the situation, even from a distance, when numbers are no longer legible. (Participant 7) Good visibility of alarms, even from a greater distance. (Participant 9) |
| Useful supplementary tool to the conventional display (3/163; 1.8%) | Useful supplementary tool. (Participant 25) A good addition to the numerical display. (Participant 19) |
| Graphic design (20/163; 12.3%) | |
| Presentation of specific parameters (16/163; 9.8%) | The purple color immediately catches the eye, indicating a drop in saturation. (Participant 54) The different colors and symbols are easily distinguishable and provide good indicators. (Participant 61) |
| Intuitiveness (7/163; 4.3%) | |
| You get used to it very quickly. (Participant 42) I like the clarity provided by Visual Patient. (Participant 7) | |
| Perceived Areas for Improvement | |
| Usability (55/163; 33.7%) | |
| Non-adjustability of alarm thresholds (33/163; 20.3%) | User-set alarm thresholds should be automatically adopted. (Participant 3) For SpO2, you may want to enter changeable values so that a COPD patient is not displayed as purple all the time. (Participant 14) |
| Interpretation becomes more complex when multiple parameters are outside of the normal range (4/163; 2.5%) | It is difficult to perceive the information when multiple problems occur simultaneously. (Participant 34) In general, are there already too many parameters displayed in Visual Patient and should it be reduced to the basics? (Participant 47) |
| Graphic design (22/163; 13.5%) | |
| Presentation of specific parameters (12/163; 7.4%) | I would like the inclusion of pacemaker function (as in a regular EKG). (Participant 38) The pulsation of Visual Patient indicates whether the pulse is within the normal range. However, the frequency of the pulsation does not match the heartbeat heard via SpO2. This is very confusing because what is seen does not correspond to what is heard. (Participant 37) |
| Space allocation on split screen (6/163; 3.7%) | Too many pieces of information on too little space. (Participant 44) The reduction of the remaining curves is a major point of criticism. (Participant 9) |
| Lack of precision in information presentation (11/163; 6.8%) | |
| The cyanosis could be further differentiated in color. (Participant 18) It would be helpful if the color could be further differentiated. Similarly, CO2could be color-coded for hyper- or hypocapnia. (Participant 21) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hunn, C.A.; Lunkiewicz, J.; Noethiger, C.B.; Tscholl, D.W.; Gasciauskaite, G. Qualitative Exploration of Anesthesia Providers’ Perceptions Regarding Philips Visual Patient Avatar in Clinical Practice. Bioengineering 2024, 11, 323. https://doi.org/10.3390/bioengineering11040323
Hunn CA, Lunkiewicz J, Noethiger CB, Tscholl DW, Gasciauskaite G. Qualitative Exploration of Anesthesia Providers’ Perceptions Regarding Philips Visual Patient Avatar in Clinical Practice. Bioengineering. 2024; 11(4):323. https://doi.org/10.3390/bioengineering11040323
Chicago/Turabian StyleHunn, Cynthia A., Justyna Lunkiewicz, Christoph B. Noethiger, David W. Tscholl, and Greta Gasciauskaite. 2024. "Qualitative Exploration of Anesthesia Providers’ Perceptions Regarding Philips Visual Patient Avatar in Clinical Practice" Bioengineering 11, no. 4: 323. https://doi.org/10.3390/bioengineering11040323
APA StyleHunn, C. A., Lunkiewicz, J., Noethiger, C. B., Tscholl, D. W., & Gasciauskaite, G. (2024). Qualitative Exploration of Anesthesia Providers’ Perceptions Regarding Philips Visual Patient Avatar in Clinical Practice. Bioengineering, 11(4), 323. https://doi.org/10.3390/bioengineering11040323