
Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum

 ,
, 
 ,
,  ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
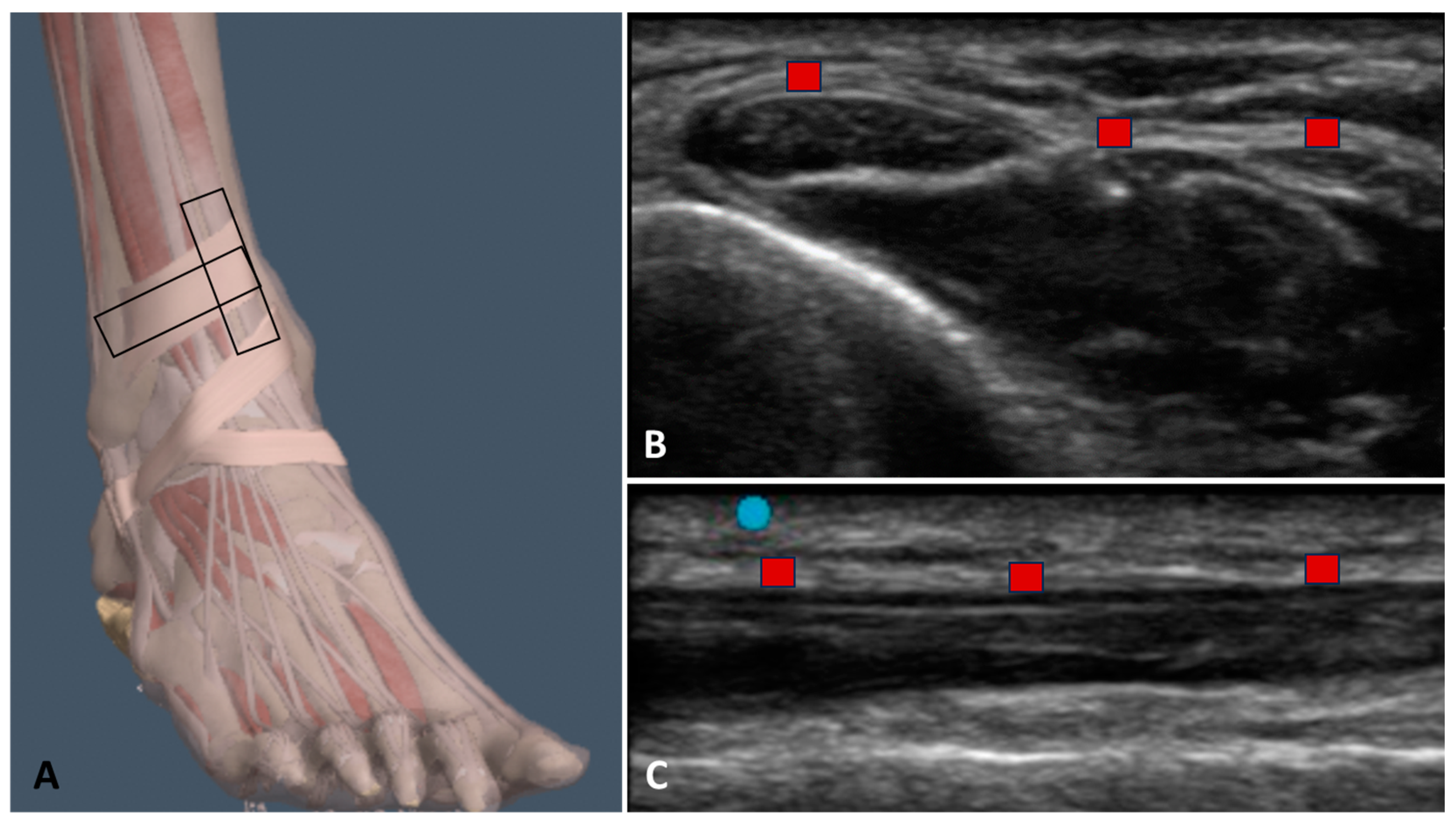
2.3. Ultrasound Examination Measurements
2.4. Statistical Analysis
3. Results
3.1. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum
3.1.1. Group 1 (Football Players with Previous Multiple Ankle Sprains)
3.1.2. Group 2 (Healthy Volunteers)
3.2. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between Previous Multiple Ankle Sprains and Healthy Sides in Group 1
3.3. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between Two Sides in Group 2
3.4. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between the Previously Sprained Side of Group 1 with the Corresponding Side in Group 2
3.5. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between the Healthy Side of Group 1 with the Corresponding Side in Group 2
3.6. Echogenicity Measurements
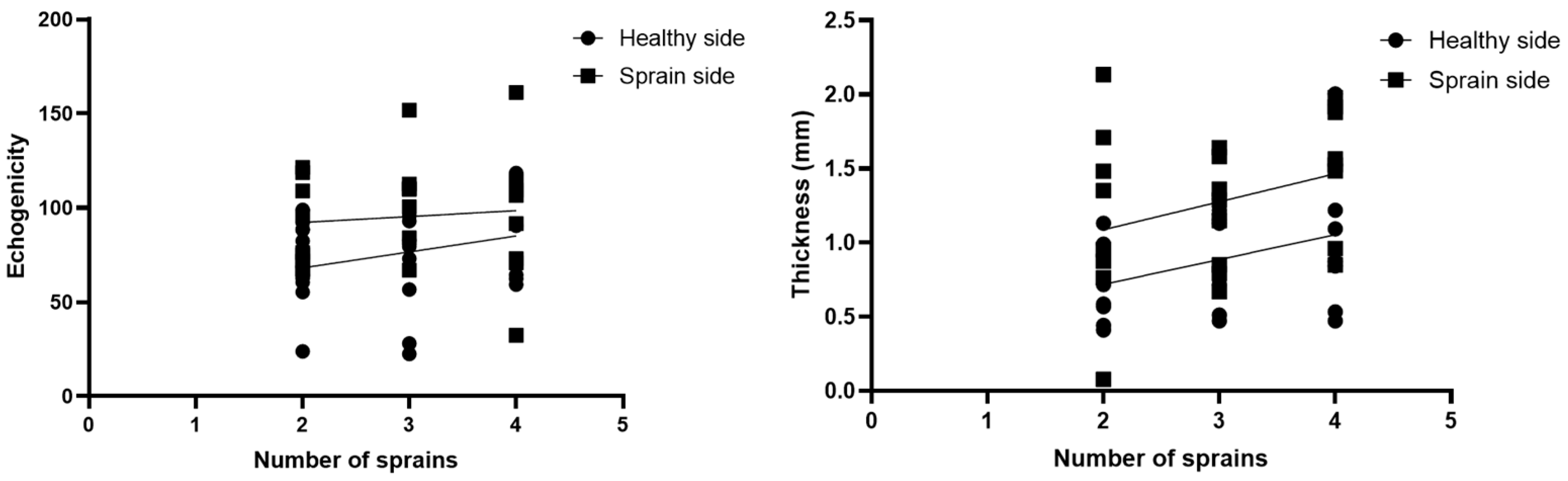
3.7. Correlations US Measurements and Number of Ankle Sprains
3.8. Intra-Rater Reliability
4. Discussion
Limitation of Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FIFA. FIFA Big Count; FIFA Communications Division, Information Services: Zürichberg, Switzerland, 2006; Available online: https://www.fifa.com/mm/document/fifafacts/%20bcoffsurv/%20bigcount.%20statspackage_%207024.pdf (accessed on 28 February 2024).
- Gurau, T.V.; Gurau, G.; Voinescu, D.C.; Anghel, L.; Onose, G.; Iordan, D.A.; Munteanu, C.; Onu, I.; Musat, C.L. Epidemiology of Injuries in Men’s Professional and Amateur Football (Part I). J. Clin. Med. 2023, 12, 5569. [Google Scholar] [CrossRef] [PubMed]
- Gurau, T.V.; Gurau, G.; Musat, C.L.; Voinescu, D.C.; Anghel, L.; Onose, G.; Munteanu, C.; Onu, I.; Iordan, D.A. Epidemiology of Injuries in Professional and Amateur Football Men (Part II). J. Clin. Med. 2023, 12, 6293. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Magnusson, H.; Kristenson, K.; Bengtsson, H.; Ekstrand, J. Injuries affect team performance negatively in professional football: An 11-year follow-up of the UEFA Champions League injury study. Br. J. Sports Med. 2013, 47, 738–742. [Google Scholar] [CrossRef] [PubMed]
- Roe, M.; Murphy, J.C.; Gissane, C.; Blake, C. Time to get our four priorities right: An 8-year prospective investigation of 1326 player-seasons to identify the frequency, nature, and burden of time-loss injuries in elite Gaelic football. PeerJ 2018, 6, e4895. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Shalaj, I.; Tishukaj, F.; Bachl, N.; Tschan, H.; Wessner, B.; Csapo, R. Injuries in professional male football players in Kosovo: A descriptive epidemiological study. BMC Musculoskel. Disord. 2016, 17, 338. [Google Scholar] [CrossRef] [PubMed]
- Junge, A.; Dvořák, J. Football injuries during the 2014 FIFA World Cup. Br. J. Sports Med. 2015, 49, 599–602. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of Injury Incidences in Male Professional Adult and Elite Youth Soccer Players: A Systematic Review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Tropp, H. The incidence of ankle sprains in soccer. Foot Ankle 1990, 11, 41–44. [Google Scholar] [CrossRef]
- Junge, A.; Dvorak, J. Soccer injuries: A review on incidence and prevention. Sports Med. 2004, 34, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Woods, C.; Hawkins, R.; Hulse, M.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football: An analysis of ankle sprains. Br. J. Sports Med. 2003, 37, 233–238. [Google Scholar] [CrossRef]
- Hawkins, R.D.; Fuller, C.W. A prospective epidemiological study of injuries in four English professional football clubs. Br. J. Sports Med. 1999, 33, 196–203. [Google Scholar] [CrossRef]
- Waldén, M.; Hägglund, M.; Ekstrand, J. Injuries in Swedish elite football—A prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand. J. Med. Sci. Sports 2005, 15, 118–125. [Google Scholar] [CrossRef]
- Giza, E.; Fuller, C.; Junge, A.; Dvorak, J. Mechanisms of foot and ankle injuries in soccer. Am. J. Sports Med. 2003, 31, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Andersen, T.E.; Floerenes, T.W.; Arnason, A.; Bahr, R. Video analysis of the mechanisms for ankle injuries in football. Am. J. Sports Med. 2004, 32 (Suppl. 1), 69S–79S. [Google Scholar] [CrossRef]
- Demondion, X.; Canella, C.; Moraux, A.; Cohen, M.; Bry, R.; Cotton, A. Retinacular disorders of the ankle and foot. Semin. Musculoskelet. Radiol. 2010, 14, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Numkarunarunrote, N.; Malik, A.; Aguiar, R.O.; Trudell, D.J.; Resnick, D. Retinacula of the foot and ankle: MRI with anatomic correlation in cadavers. Am. J. Roentgenol. 2007, 188, W348–W354. [Google Scholar] [CrossRef]
- Stecco, A.; Stecco, C.; Macchi, V.; Porzionato, A.; Ferraro, C.; Masiero, S.; De Caro, R. RMI study and clinical correlations of ankle retinacula damage and outcomes of ankle sprain. Surg. Radiol. Anat. 2011, 33, 881–890. [Google Scholar] [CrossRef]
- Bianchi, S.; Becciolini, M. Ultrasound Features of Ankle Retinacula: Normal Appearance and Pathologic Findings. J. Ultrasound Med. 2019, 38, 3321–3334. [Google Scholar] [CrossRef]
- Pirri, C.; Stecco, A.; Stecco, C.; Özçakar, L. Ultrasound imaging and Fascial Manipulation: ’Adding a twist‘ on the ankle retinacula. J. Bodyw. Mov. Ther. 2024, 37, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Stecco, A.; Stecco, C.; Özçakar, L. Ultrasound imaging and Fascial Manipulation for rigid retinacula in two cases of complex regional pain syndrome. Med. Ultrason. 2022, 24, 372–374. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Stecco, C.; Güvener, O.; Mezian, K.; Ricci, V.; Jačisko, J.; Fojtik, P.; Kara, M.; Chang, K.V.; Dughbaj, M.; et al. EURO-MUSCULUS: European Musculoskeletal Ultrasound Study Group in Physical and Rehabilitation Medicine. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for Ankle/Foot. Am. J. Phys. Med. Rehabil. 2024, 103, e29–e34. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Grob, A.T.; Veen, A.A.; Schweitzer, K.J.; Withagen, M.I.; van Veelen, G.A.; van der Vaart, C.H. Measuring echogenicity and area of the puborectalis muscle: Method and reliability. Ultrasound Obstet. Gynecol. 2014, 44, 481–485. [Google Scholar] [CrossRef]
- Cohen, J. Things I have learned (so far). Am. Psychol. 1990, 45, 1304–1312. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Pirri, C.; Caroccia, B.; Angelini, A.; Piazza, M.; Petrelli, L.; Caputo, I.; Montemurro, C.; Ruggieri, P.; De Caro, R.; Stecco, C. A New Player in the Mechanobiology of Deep Fascia: Yes-Associated Protein (YAP). Int. J. Mol. Sci. 2023, 24, 15389. [Google Scholar] [CrossRef]
- Pirri, C.; Petrelli, L.; Pérez-Bellmunt, A.; Ortiz-Miguel, S.; Fede, C.; De Caro, R.; Miguel-Pérez, M.; Stecco, C. Fetal Fascial Reinforcement Development: From “a White Tablet” to a Sculpted Precise Organization by Movement. Biology 2022, 11, 735. [Google Scholar] [CrossRef]
- Pirri, C.; Pirri, N.; Porzionato, A.; Boscolo-Berto, R.; De Caro, R.; Stecco, C. Inter- and Intra-Rater Reliability of Ultrasound Measurements of Superficial and Deep Fasciae Thickness in Upper Limb. Diagnostics 2022, 12, 2195. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Group 1 | Group 2 | p-Value Group 1 vs. Group 2 |
|---|---|---|---|
| Age, year | 29.96 ± 10.54 | 28.09 ± 12.38 | p = 0.14 |
| Weight, kg | 69.22 ± 6.1 | 72.60 ± 12.20 | p = 0.45 |
| Height, cm | 174.3 ± 4.83 | 171.30 ± 6.76 | p = 0.55 |
| Descriptive Statistics | H. Side (long.) | H. Side (trans.) | S. Side (long.) | S. Side (trans.) |
|---|---|---|---|---|
| Number of values | 25 | 25 | 25 | 25 |
| Minimum | 0.41 | 0.44 | 0.67 | 0.50 |
| Maximum | 2 | 1.72 | 2.14 | 2.51 |
| Mean | 0.90 | 0.92 | 1.3 | 1.33 |
| Std. deviation | 0.4 | 0.44 | 0.44 | 0.51 |
| Std. error of mean | 0.08 | 0.08 | 0.08 | 0.1 |
| Descriptive Statistics | R. Side (long.) | R. Side (transv.) | L. Side (long.) | L. Side (transv.) |
|---|---|---|---|---|
| Number of values | 25 | 25 | 25 | 25 |
| Minimum | 0.41 | 0.43 | 0.43 | 0.44 |
| Maximum | 2.1 | 2.1 | 1.9 | 1.9 |
| Mean | 0.90 | 0.83 | 0.90 | 0.90 |
| Std. deviation | 0.44 | 0.42 | 0.43 | 0.44 |
| Std. error of mean | 0.08 | 0.08 | 0.08 | 0.08 |
| Type of Comparison | Mean Diff. | p-Value |
|---|---|---|
| Group 1 S. side (long.) vs. group 2 c.s. (long.) Group 1 S. side (transv.) vs. group 2 c.s. (transv.) | 0.3902 0.4981 | p = 0.003 p = 0.004 |
| Type of Comparison | Mean Diff. | p-Value |
|---|---|---|
| Group 1 H. side (long.) vs. group 2 c.s. (long.) Group 1 H. side (transv.) vs. group 2 c.s. (transv.) | −0.045 0.027 | p = 0.68 p = 0.82 |
| Descriptive Statistics | H. Side (Group 1) | S. Side (Group 1) | R. Side (Group 2) | L. Side (Group 2) |
|---|---|---|---|---|
| Number of values | 25 | 25 | 25 | 25 |
| Minimum | 36.58 | 45.05 | 46.2 | 41.91 |
| Maximum | 166.1 | 158.9 | 145.7 | 133.8 |
| Mean | 93.84 | 94.61 | 80.80 | 89.44 |
| Std. deviation | 29.10 | 27.17 | 29.04 | 26.72 |
| Type of Comparison | Mean Diff. | p-Value |
|---|---|---|
| Group 1 H. side vs. group 1 S. side | −0.77 | p = 0.99 |
| Group 1 H. side vs. group 2 c.s. | 13.04 | p = 0.35 |
| Group 1 H. side vs. group 2 c.s. | 4.39 | p = 0.94 |
| Group 1 S. side vs. group 2 c.s. | 13.81 | p = 0.31 |
| Group 1 S. side vs. group 2 c.s. | 5.16 | p = 0.91 |
| Group 2 right vs. group 2 left | −8.64 | p = 0.69 |
| Type of Axis | ICC |
|---|---|
| Group 1 H. side (long.) | 0.90 (0.89–0.94) |
| Group 1 H. side (transv.) | 0.92 (0.88–0.96) |
| Group 1 S. side (long.) | 0.91 (0.88–0.94) |
| Group 1 S. side (transv.) | 0.92 (0.88–0.96) |
| Group 2 left (long.) | 0.90 (0.89–0.94) |
| Group 2 left (transv.) | 0.91 (0.89–0.96) |
| Group 2 right (long.) | 0.90 (0.89–0.94) |
| Group 2 right (transv.) | 0.91 (0.89–0.94) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirri, C.; Pirri, N.; Guidolin, D.; Macchi, V.; Porzionato, A.; De Caro, R.; Stecco, C. Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum. Bioengineering 2024, 11, 419. https://doi.org/10.3390/bioengineering11050419
Pirri C, Pirri N, Guidolin D, Macchi V, Porzionato A, De Caro R, Stecco C. Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum. Bioengineering. 2024; 11(5):419. https://doi.org/10.3390/bioengineering11050419
Chicago/Turabian StylePirri, Carmelo, Nina Pirri, Diego Guidolin, Veronica Macchi, Andrea Porzionato, Raffaele De Caro, and Carla Stecco. 2024. "Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum" Bioengineering 11, no. 5: 419. https://doi.org/10.3390/bioengineering11050419
APA StylePirri, C., Pirri, N., Guidolin, D., Macchi, V., Porzionato, A., De Caro, R., & Stecco, C. (2024). Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum. Bioengineering, 11(5), 419. https://doi.org/10.3390/bioengineering11050419