
Enhancing Dermatological Diagnostics with EfficientNet: A Deep Learning Approach

 and
and
Abstract

1. Introduction
- Ranks among the top-performing models in the European region, indicating its potential to address regional medical challenges effectively.
- Achieves competitive results based on EfficientNetB3, demonstrating efficient utilization of limited training data.
- Enhances practical feasibility and cost-effectiveness of deployment due to its modest computational requirements.
- Shows robust performance with fewer images compared to models that achieve similar or better results with larger datasets.
2. Methodology of Research
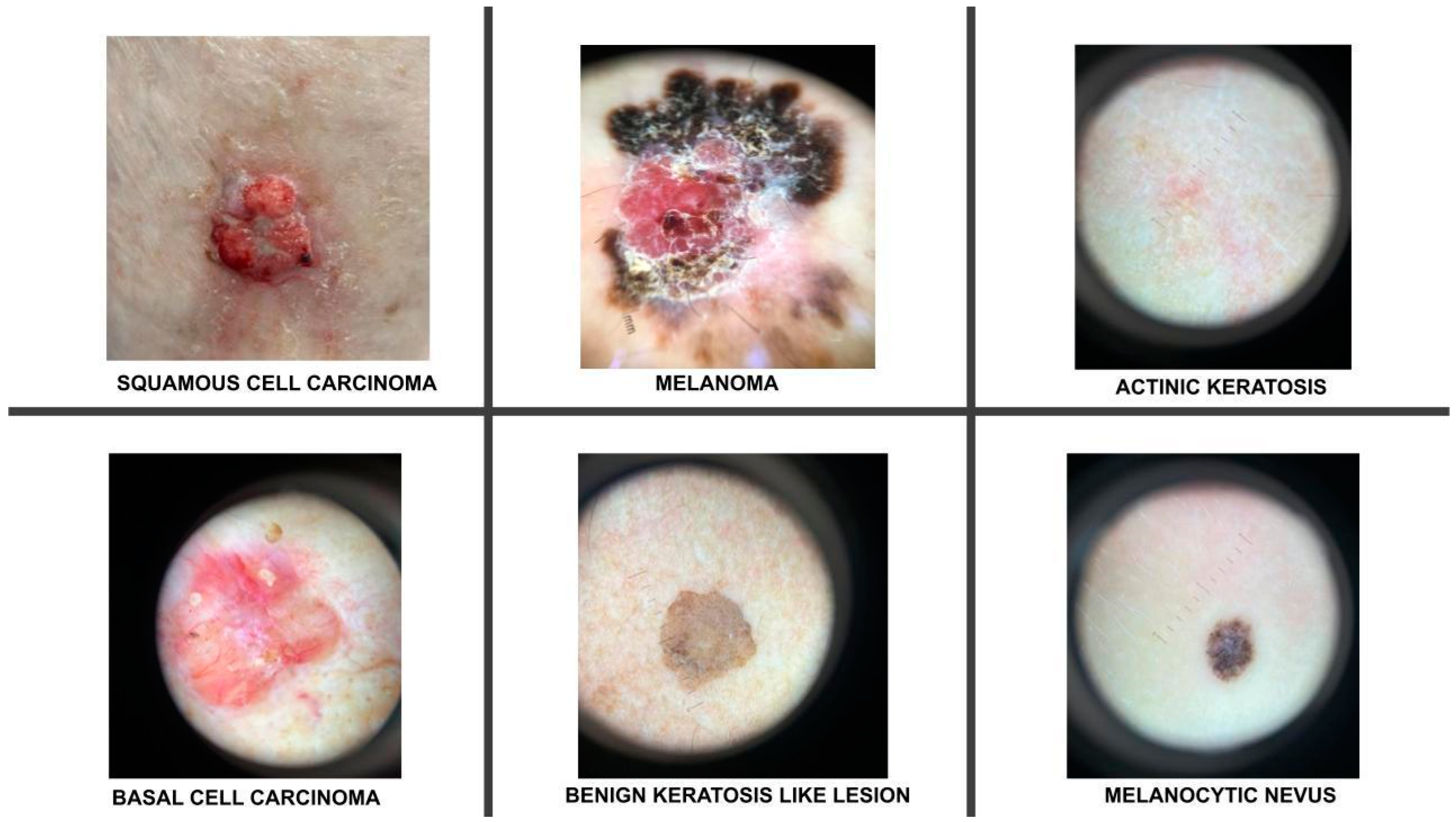
2.1. Description of the Training Dataset
2.2. Data Preprocessing
- Resizing: Images were resized to 300 × 300, ensuring uniformity in input sizes.
- Normalization: Pixel values were scaled to the [0, 1] interval to reduce data discrepancies and aid training convergence.
- Mean Subtraction and Standardization: Each pixel’s value had the dataset’s mean subtracted and was then divided by the standard deviation to normalize the data further, enhancing model convergence.
- Data Augmentation: This technique creates new images by modifying existing ones. We employed mirroring, translation, rotation, scaling, brightness adjustment, and noise addition to augment the existing pictures [15]. These augmented images were then added to the categories with less data, thereby balancing the training dataset.
2.3. The Usage and the Architecture of the Model
- On top of the EfficientNetB3 model, adding a batch normalization [21] layer improved accuracy by enhancing convergence and helped reduce overfitting. Batch normalization contributed to smoother training and improved generalization on unseen data by stabilizing and normalizing activations throughout the network.
- Two additional dense layers significantly enhanced classification performance by introducing non-linear features, extracting higher-level features, reducing parameter count and dimensionality of input images, and serving as a regularization technique.
- Finally, one dropout layer [22] randomly deactivated the neurons during training, which helped prevent overfitting by encouraging the model to generalize better. This technique improves the robustness and performance of the neural network on unseen data.
2.4. Training and Validating the Model
2.4.1. Hyperparameters
2.4.2. Techniques Used to Combat Overfitting
- Dropout: Dropout selectively deactivates neurons in neural network layers during training, simulating smaller networks within the model. This approach encourages the network to diversify its learning strategies, enhancing generalization and mitigating overfitting by preventing reliance on individual neurons [31].
- Batch Normalization: Normalization adjusts data to a mean of zero and a standard deviation of one, aligning and scaling inputs. Batch normalization speeds up training by preventing gradients from becoming too small, facilitating faster convergence with higher learning rates. It also acts as a regularizer, reducing overfitting and improving model generalization on new data. This stability reduces sensitivity to initial weight choices and simplifies experimenting with different architectures [32].
- Regularization: We used the regularization techniques to reduce overfitting: L2 regularization with a strength of 0.016 for the kernel and L1 regularization at a strength of 0.006 for both activity and bias regularization. These methods were chosen to mitigate overfitting by penalizing large parameter values in the model, thereby promoting more straightforward and more generalized outcomes across varying datasets and scenarios.
3. Results
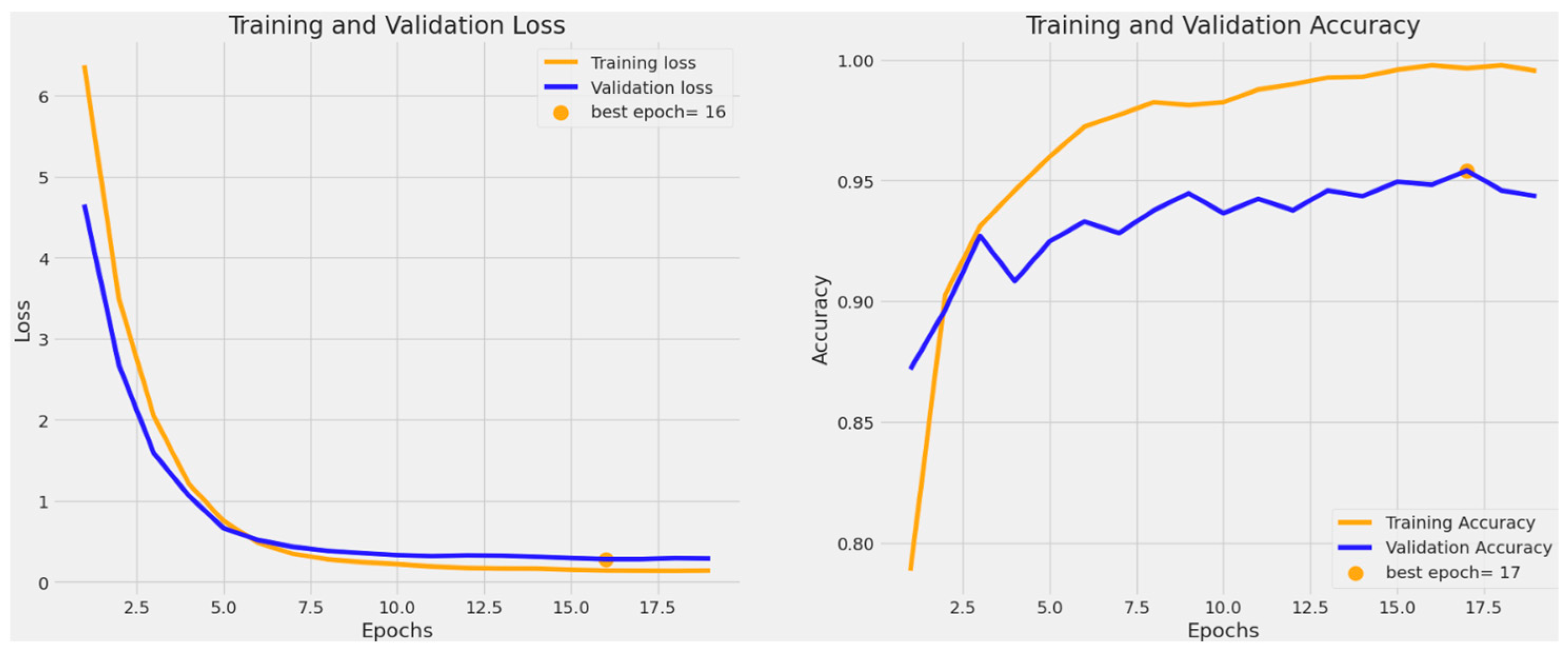
3.1. Training and Validation Accuracy and Loss
3.2. Classification Performance
3.3. Receiver Operating Characteristic (ROC) Curve
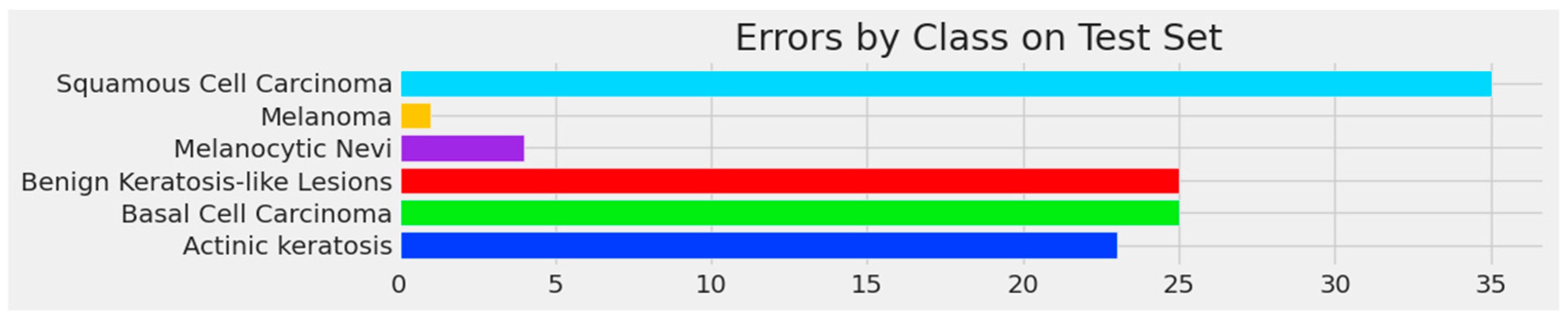
3.4. Confusion Matrix and Errors by Class
4. Discussion
4.1. Model’s Performance
4.2. Model’s Deployment and Clinical Applications
4.3. Limitations of Current Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.skincancer.org/skin-cancer-information/skin-cancer-facts/ (accessed on 9 June 2024).
- Leiter, U.; Keim, U.; Garbe, C. Epidemiology of Skin Cancer: Update 2019. Adv. Exp. Med. Biol. 2020, 1268, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2022.html (accessed on 9 June 2024).
- Argenziano, G.; Soyer, H.P.; Chimenti, S.; Talamini, R.; Corona, R.; Sera, F.; Binder, M.; Cerroni, L.; De Rosa, G.; Ferrara, G.; et al. Dermoscopy of pigmented skin lesions: Results of a consensus meeting via the Internet. J. Am. Acad. Dermatol. 2003, 48, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.iarc.who.int/cancer-type/skin-cancer/ (accessed on 9 June 2024).
- Tschandl, P.; Codella, N.; Akay, B.N.; Argenziano, G.; Braun, R.P.; Cabo, H.; Gutman, D.; Halpern, A.; Helba, B.; Hofmann-Wellenhof, R.; et al. Comparison of the accuracy of human readers versus machine-learning algorithms for pigmented skin lesion classification: An open, web-based, international, diagnostic study. Lancet Oncol. 2019, 20, 938–947. [Google Scholar] [CrossRef]
- Marchetti, M.A.; Liopyris, K.; Dusza, S.W.; Codella, N.C.; Gutman, D.A.; Helba, B.; Kalloo, A.; Halpern, A.C.; Soyer, H.P.; Curiel-Lewandrowski, C.; et al. Computer algorithms show potential for improving dermatologists’ accuracy to diagnose cutaneous melanoma: Results of the International Skin Imaging Collaboration 2017. J. Am. Acad. Dermatol. 2019, 82, 622–627. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Codella, N.C.F.; Nguyen, Q.-B.; Pankanti, S.; Gutman, D.A.; Helba, B.; Halpern, A.C.; Smith, J.R. Deep learning ensembles for melanoma recognition in dermoscopy images. IBM J. Res. Dev. 2017, 61, 5:1–5:15. [Google Scholar] [CrossRef]
- Brinker, T.J.; Hekler, A.; Enk, A.H.; Berking, C.; Haferkamp, S.; Hauschild, A.; Weichenthal, M.; Klode, J.; Schadendorf, D.; Holland-Letz, T.; et al. Deep neural networks are superior to dermatologists in melanoma image classification. Eur. J. Cancer 2019, 119, 11–17. [Google Scholar] [CrossRef]
- Liu, Y.; Jain, A.; Eng, C.; Way, D.H.; Lee, K.; Bui, P.; Kanada, K.; Marinho, G.d.O.; Gallegos, J.; Gabriele, S.; et al. A deep learning system for differential diagnosis of skin diseases. Nat. Med. 2020, 26, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In International Conference on Machine Learning; PMLR: Birmingham, UK, 2019; pp. 6105–6114. [Google Scholar] [CrossRef]
- The International Skin Imaging Collaboration. Available online: https://gallery.isic-archive.com/ (accessed on 2 February 2024).
- ImageNet Website and Dataset. Available online: https://www.image-net.org/ (accessed on 2 February 2024).
- Shorten, C.; Khoshgoftaar, T.M. A survey on image data augmentation for deep learning. J. Big Data. 2019, 6, 60. [Google Scholar] [CrossRef]
- Sharma, N.; Jain, V.; Mishra, A. An analysis of convolutional neural networks for image classification. Procedia Comput. Sci. 2018, 132, 377–384. [Google Scholar] [CrossRef]
- Pan, S.J.; Yang, Q. A survey on transfer learning. IEEE Trans. Knowl. Data Eng. 2010, 22, 1345–1359. [Google Scholar] [CrossRef]
- Jain, S.; Singhania, U.; Tripathy, B.; Nasr, E.A.; Aboudaif, M.K.; Kamrani, A.K. Deep learning-based transfer learning for classification of skin cancer. Sensors 2021, 21, 8142. [Google Scholar] [CrossRef] [PubMed]
- An End-to-End Platform for Machine Learning. Available online: www.tensorflow.org (accessed on 30 March 2024).
- Keras, a Deep Learning API Written in Python. Available online: https://keras.io/about/ (accessed on 30 March 2024).
- Available online: https://keras.io/api/layers/normalization_layers/batch_normalization/ (accessed on 2 April 2024).
- Available online: https://www.tensorflow.org/api_docs/python/tf/keras/layers/Dropout (accessed on 2 April 2024).
- Available online: https://www.tensorflow.org/guide/mixed_precision (accessed on 2 April 2024).
- Available online: https://www.tensorflow.org/api_docs/python/tf/keras/callbacks/EarlyStopping (accessed on 4 April 2024).
- Available online: https://keras.io/api/callbacks/reduce_lr_on_plateau/ (accessed on 4 April 2024).
- Available online: https://www.tensorflow.org/tutorials/images/transfer_learning (accessed on 20 March 2024).
- Available online: https://keras.io/api/callbacks/model_checkpoint/ (accessed on 30 March 2024).
- Available online: https://www.kaggle.com/code/residentmario/full-batch-mini-batch-and-online-learning (accessed on 10 March 2024).
- Ruder, S. An overview of gradient descent optimization algorithms. arXiv 2016, arXiv:1609.04747. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. In International Conference on Machine Learning; PMLR: Birmingham, UK, 2015; pp. 448–456. [Google Scholar] [CrossRef]
- Karthik, R.; Vaichole, T.S.; Kulkarni, S.K.; Yadav, O.; Khan, F. Eff2Net: An efficient channel attention-based convolutional neural network for skin disease classification. Biomed. Signal Process Control 2022, 73, 103406. [Google Scholar] [CrossRef]
- Ali, K.; Shaikh, Z.A.; Khan, A.A.; Laghari, A.A. Multiclass skin cancer classification using EfficientNets–a first step towards preventing skin cancer. Neurosci. Inform. 2022, 2, 100034. [Google Scholar] [CrossRef]
- Rafay, A.; Hussain, W. EfficientSkinDis: An EfficientNet-based classification model for a large manually curated dataset of 31 skin diseases. Biomed Signal Process Control 2023, 85, 104869. [Google Scholar] [CrossRef]
- Venugopal, V.; Raj, N.I.; Nath, M.K.; Stephen, N. A deep neural network using modified EfficientNet for skin cancer detection in dermoscopic images. Decis. Anal. J. 2023, 8, 100278. [Google Scholar] [CrossRef]
- Harahap, M.; Husein, A.M.; Kwok, S.C.; Wizley, V.; Leonardi, J.; Ong, D.K.; Ginting, D.; Silitonga, B.A. Skin cancer classification using EfficientNet architecture. Bull. Electr. Eng. Inform. 2024, 13, 2716–2728. [Google Scholar] [CrossRef]
- Bazgir, E.; Haque, E.; Maniruzzaman; Hoque, R. Skin cancer classification using Inception Network. World J. Adv. Res. Rev. 2024, 21, 839–849. [Google Scholar] [CrossRef]
- Rahman, M.A.; Bazgir, E.; Hossain, S.M.S. Maniruzzaman Skin cancer classification using NASNet. Int. J. Sci. Res. Arch. 2024, 11, 775–785. [Google Scholar] [CrossRef]
- Anand, V.; Gupta, S.; Altameem, A.; Nayak, S.R.; Poonia, R.C.; Saudagar, A.K.J. An enhanced transfer learning based classification for diagnosis of skin cancer. Diagnostics 2022, 12, 1628. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.K.; Gorantla, R.; Allada, S.G.R.; Narra, P. SkiNet: A deep learning framework for skin lesion diagnosis with uncertainty estimation and explainability. PLoS ONE 2022, 17, e0276836. [Google Scholar] [CrossRef]
- Ahmed, T.; Mou, F.S.; Hossain, A. SCCNet: An Improved Multi-Class Skin Cancer Classification Network using Deep Learning. In Proceedings of the 2024 3rd International Conference on Advancement in Electrical and Electronic Engineering (ICAEEE), Gazipur, Bangladesh, 25–27 April 2024; pp. 1–5. [Google Scholar] [CrossRef]
- Al-Rasheed, A.; Ksibi, A.; Ayadi, M.; Alzahrani, A.I.; Zakariah, M.; Hakami, N.A. An ensemble of transfer learning models for the prediction of skin cancers with conditional generative adversarial networks. Diagnostics 2022, 12, 3145. [Google Scholar] [CrossRef]
- Naeem, A.; Anees, T.; Khalil, M.; Zahra, K.; Naqvi, R.A.; Lee, S.W. SNC_Net: Skin Cancer Detection by Integrating Handcrafted and Deep Learning-Based Features Using Dermoscopy Images. Mathematics 2024, 12, 1030. [Google Scholar] [CrossRef]
- Naeem, A.; Anees, T. DVFNet: A deep feature fusion-based model for the multiclassification of skin cancer utilizing dermoscopy images. PLoS ONE 2024, 19, e0297667. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classes | No. of Images | No. of Augmented Images | Total |
|---|---|---|---|
| Melanoma | 1655 | 489 | 2144 |
| BCC | 1811 | 333 | 2144 |
| Benign keratosis-like lesions | 1663 | 481 | 2144 |
| Melanocytic nevi | 1686 | 458 | 2144 |
| SCC | 606 | 1538 | 2144 |
| AK | 801 | 1343 | 2144 |
| Total | 8222 | 4642 | 12,864 |
| Hyperparameters | Values |
|---|---|
| Learning Rate | 0.001 |
| Batch Size | 32 |
| Number of Epochs | 19 |
| Optimizer | Adamax |
| Dropout Rate | 0.45 |
| Activation Functions | Relu, Softmax |
| Regularization Parameters | Kernel Regularizer: L2 regularization with strength 0.016 Activity Regularizer: L1 regularization with strength 0.006 Bias Regularizer: L1 regularization with strength 0.006 |
| Loss Function | Categorical Cross Entropy |
| Augmentation Techniques | Rotate, Scale, Flip, Zoom |
| Precision | Recall | F1-Score | Support | |
|---|---|---|---|---|
| Basal cell carcinoma | 0.94 | 0.98 | 0.96 | 225 |
| Benign keratosis-like lesions | 0.94 | 0.89 | 0.91 | 208 |
| Melanocytic nevi | 0.95 | 0.97 | 0.96 | 210 |
| Melanoma | 1.00 | 0.99 | 1.00 | 207 |
| Accuracy | 0.96 | 850 | ||
| Macro Avg | 0.96 | 0.96 | 0.96 | 850 |
| Weighted Avg | 0.96 | 0.96 | 0.96 | 850 |
| Precision | Recall | F1-Score | Support | |
|---|---|---|---|---|
| Actinic keratosis | 0.74 | 0.77 | 0.75 | 100 |
| Basal cell carcinoma | 0.87 | 0.84 | 0.85 | 227 |
| Benign keratosis-like lesions | 0.85 | 0.85 | 0.85 | 208 |
| Melanocytic nevi | 0.94 | 0.97 | 0.96 | 210 |
| Melanoma | 1.00 | 1.00 | 1.00 | 207 |
| Squamous cell carcinoma | 0.69 | 0.54 | 0.61 | 76 |
| Accuracy | 0.89 | 1028 | ||
| Macro Avg | 0.85 | 0.84 | 0.85 | 1028 |
| Weighted Avg | 0.89 | 0.89 | 0.89 | 1028 |
| Model | Year | Dataset | Model Used | Scope | Accuracy |
|---|---|---|---|---|---|
| Karthik et al. [33] | 2022 | DermNet NZ, Derm7Pt, DermatoWeb, Fitzpatrick17k | EfficientNetV2, in conjunction with the efficient channel attention block | Classification of four skin diseases: acne, AK, melanoma, and psoriasis. | 84.7% |
| Ali et al. [34] | 2022 | HAM10000 dataset of dermatoscopic images | EfficientNet variants (results presented refer to EfficientNet B0) | Classification of seven skin diseases | 87.9% |
| Rafay et al. [35] | 2023 | Manually curated from Atlas Dermatology and SIC Dataset | Fine-tuned EfficientNetB2 | Classification of 31 skin diseases | 87.15% |
| Venugopal et al. [36] | 2023 | ISIC 2019 dataset | EfficientNetV2-M | Binary classification: malignant vs. benign | 95.49% |
| Venugopal et al. [36] | 2023 | ISIC 2019 dataset | EfficientNetB4 | Binary classification: malignant vs. benign | 93.17% |
| Harahap et al. [37] | 2024 | ISIC 2019 dataset | EfficientNetB0 to EfficientNetB7 (results reported to EfficientNetB3) | Classification of three skin diseases: BCC, SCC, melanoma | 77.6% |
| Harahap et al. [37] | 2024 | ISIC 2019 dataset | EfficientNetB0 to EfficientNetB7 (results reported to EfficientNetB4, the highest result obtained) | Classification of three skin diseases: BCC, SCC, melanoma | 79.69% |
| Proposed model | ISIC 2019 and personal images collection | EfficientNetB3 | Classification of four skin diseases (benign and malign) | 95.4% | |
| Proposed model | ISIC 2019 and personal images collection | EfficientNetB3 | Classification of six skin diseases (benign and malign) | 88.8% |
| Model | Year | Dataset | Model Used | Scope | Accuracy |
|---|---|---|---|---|---|
| Bazgir et al. [38] | 2024 | Kaggle/ISIC | Inception Network | Binary classification: malign vs. benign | 85.94% |
| Rahman et al. [39] | 2024 | Kaggle/ISIC | NASNet | Binary classification: malign vs. benign | 86.73% |
| Anand et al. [40] | 2022 | Kaggle/ISIC | Modified VGG16 architecture | Binary classification: malign vs. benign | 89.9% |
| Singh et al. [41] | 2022 | ISIC 2018 | Bayesian DenseNet-169 | Classification of seven skin diseases | 73.65% |
| Ahmed et al. [42] | 2024 | ISIC 2018 | SCCNet derived from Xpection architecture | Classification of seven skin diseases | 95.2% |
| Al-Rasheed et al. [43] | 2022 | HAM10000 | Combination of VGG16, ResNet50, ResNet101 | Classification of seven skin diseases | 93.5% |
| Naeem et al. [44] | 2024 | ISIC 2019 | SNC_Net | Classification of eight skin diseases | 97.81% |
| Naeem et al. [45] | 2024 | ISIC 2019 | DVFNet | Classification of eight skin diseases | 98.32% |
| Proposed model | ISIC 2019 | EfficientNetB3 | Classification of four skin diseases | 95.4% | |
| Proposed model | ISIC 2019 | EfficientNetB3 | Classification of six skin diseases | 88.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manole, I.; Butacu, A.-I.; Bejan, R.N.; Tiplica, G.-S. Enhancing Dermatological Diagnostics with EfficientNet: A Deep Learning Approach. Bioengineering 2024, 11, 810. https://doi.org/10.3390/bioengineering11080810
Manole I, Butacu A-I, Bejan RN, Tiplica G-S. Enhancing Dermatological Diagnostics with EfficientNet: A Deep Learning Approach. Bioengineering. 2024; 11(8):810. https://doi.org/10.3390/bioengineering11080810
Chicago/Turabian StyleManole, Ionela, Alexandra-Irina Butacu, Raluca Nicoleta Bejan, and George-Sorin Tiplica. 2024. "Enhancing Dermatological Diagnostics with EfficientNet: A Deep Learning Approach" Bioengineering 11, no. 8: 810. https://doi.org/10.3390/bioengineering11080810
APA StyleManole, I., Butacu, A.-I., Bejan, R. N., & Tiplica, G.-S. (2024). Enhancing Dermatological Diagnostics with EfficientNet: A Deep Learning Approach. Bioengineering, 11(8), 810. https://doi.org/10.3390/bioengineering11080810