

Automated Lumen Segmentation in Carotid Artery Ultrasound Images Based on Adaptive Generated Shape Prior

Abstract
:1. Introduction
2. Method
2.1. Preliminary
2.1.1. The Chan–Vese Model
2.1.2. The Distance Regularization Level Set Evolution Model
2.2. The Proposed Model
2.2.1. Shape Prior
2.2.2. The Proposed Segmentation Model with Shape Constraint
2.2.3. Shape Prior Generation
2.2.4. Automatic Initialization
3. Experiments Results
3.1. Datasets
- (1)
- This dataset originates from Nanjing Brain Hospital and comprises a randomly selected collection of 149 unique longitudinal carotid artery ultrasound images. These images were collected over a period spanning from September 2019 to March 2024. To ensure the accuracy and quality of the data, all images were captured by two experienced experts in the field.
- (2)
- This dataset, sourced from Nanjing Drum Tower Hospital, consists of 98 distinct longitudinal ultrasound images of the carotid artery, randomly selected from studies of 24 patients. These images were gathered between October 2023 and December 2023. To ensure high-quality data, all imaging was also performed by two experienced experts.
3.2. Evaluation Metrics
- (1)
- Dice coefficient
- (2)
- Hausdorff distance
- (3)
- Sensitivity value
- (4)
- Specificity value
- (5)
- IOU
3.3. Experimental Details
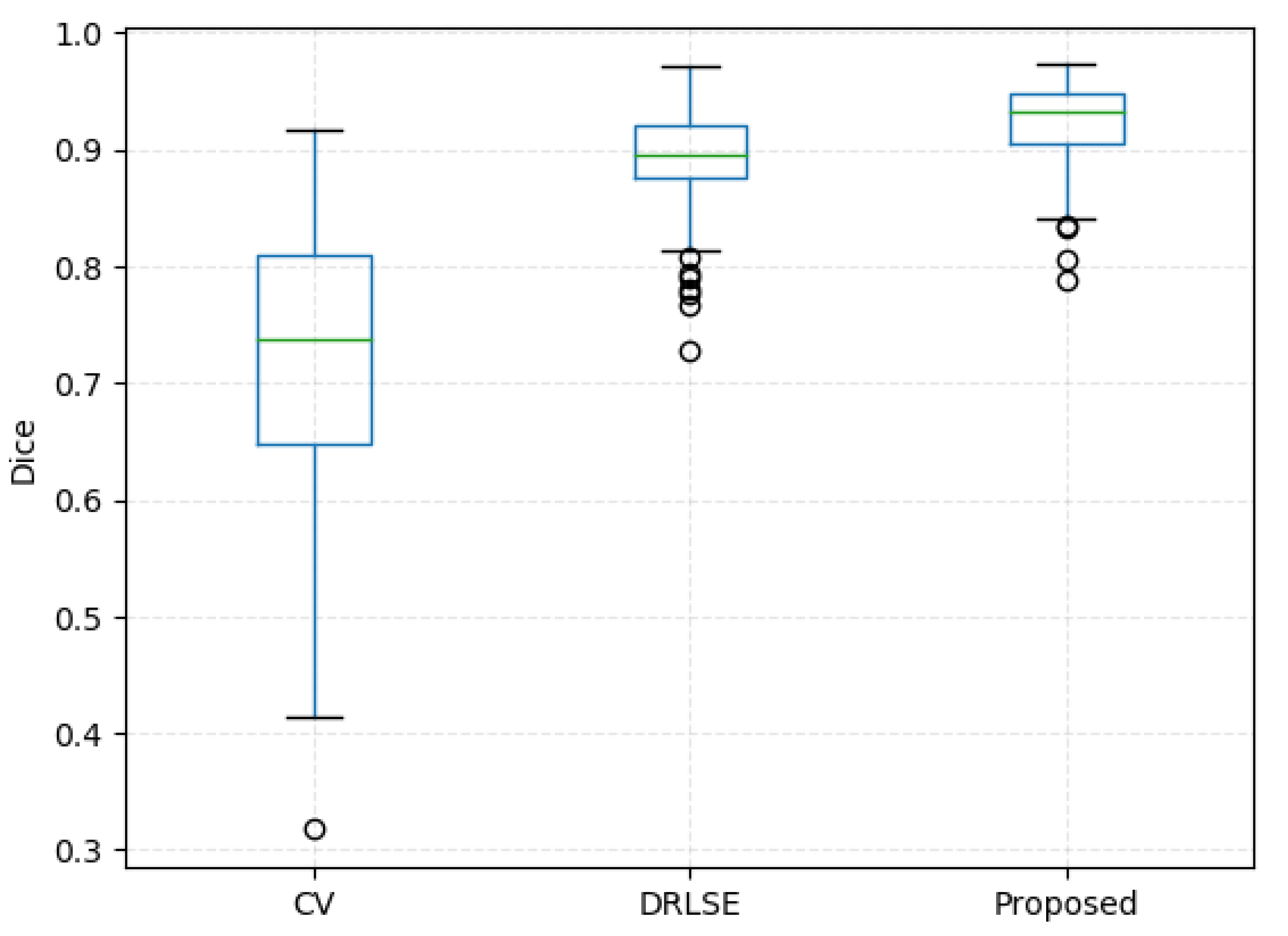
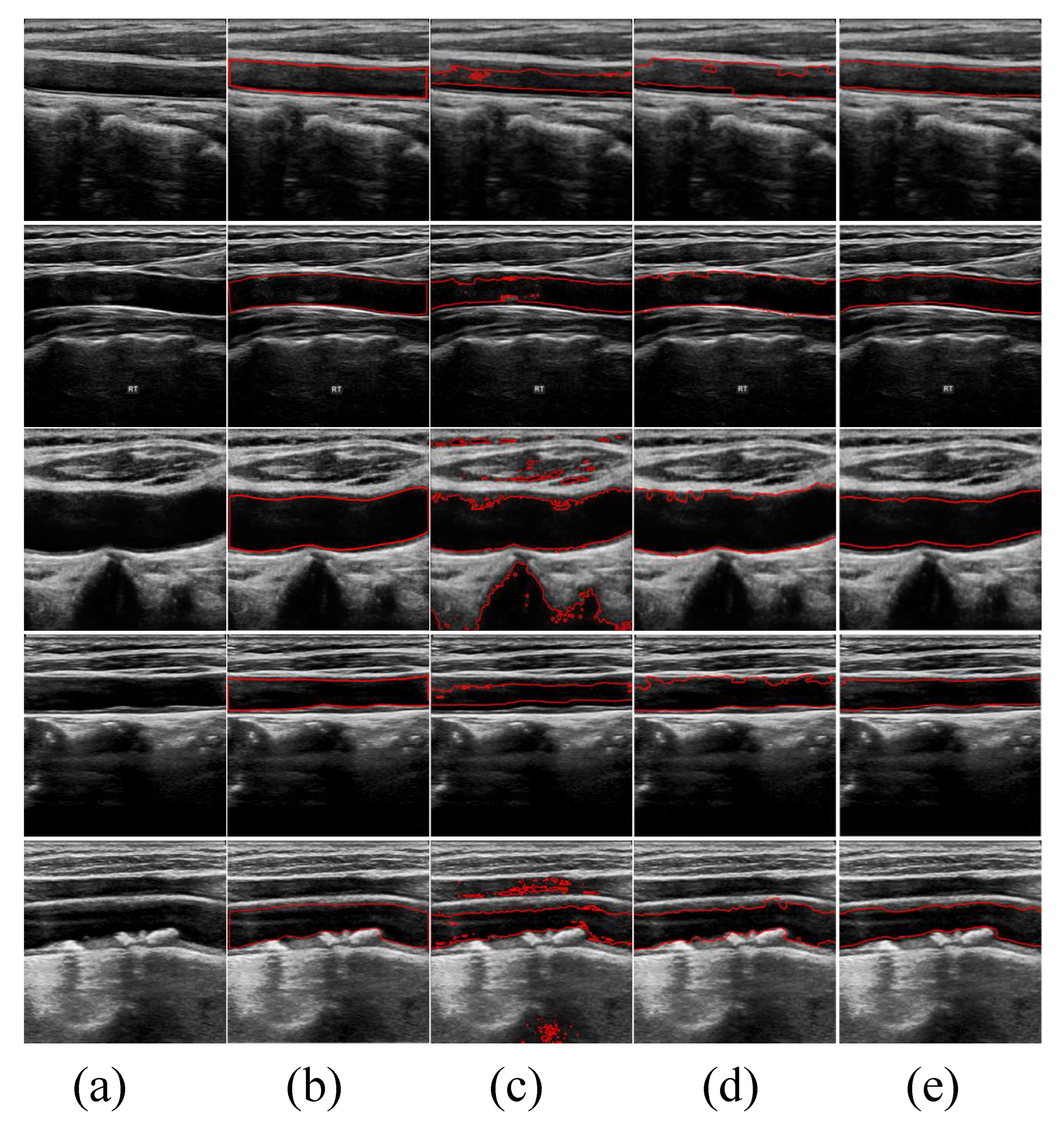
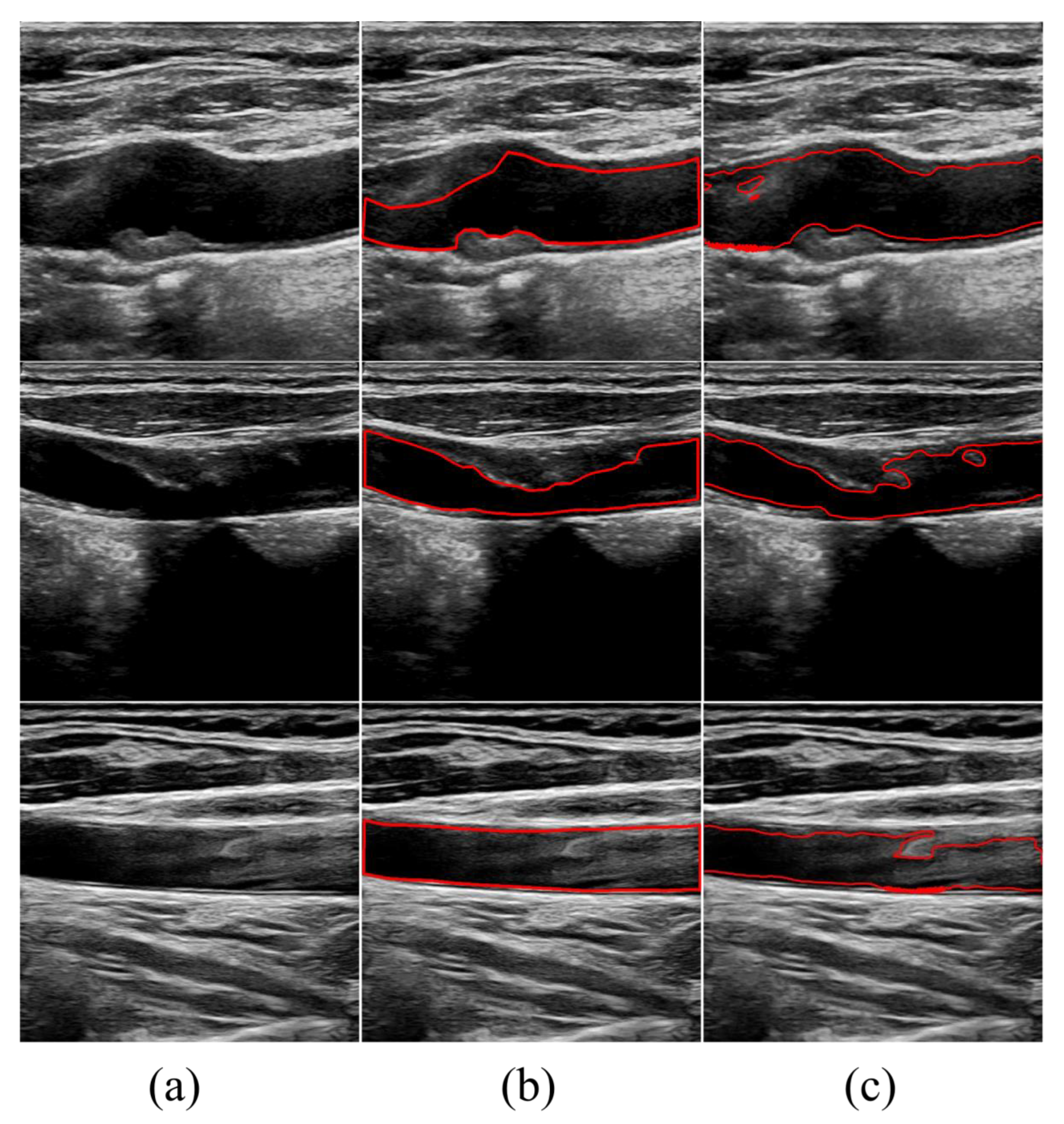
3.4. Experimental Results
3.5. Sensitivity Analysis
4. Discussion
4.1. Superiority of the Proposed Method
4.2. Limitations
4.3. Clinical Application
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CV | Chan–Vese |
| DRLSE | Distance Regularized Level Set Evolution |
| M-S | Mumford–Shah |
| LSF | Level Set Function |
| HD | Hausdorff Distance |
| IOU | Intersection Over Union |
| TP | True Positives |
| FP | False Positives |
| FN | False Negatives |
References
- Mensah, G.A.; Roth, G.A.; Fuster, V. The global burden of cardiovascular diseases and risk factors: 2020 and beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar]
- Frostegård, J. Immunity, atherosclerosis and cardiovascular disease. BMC Med. 2013, 11, 117. [Google Scholar] [CrossRef] [PubMed]
- Sakakura, K.; Nakano, M.; Otsuka, F.; Ladich, E.; Kolodgie, F.D.; Virmani, R. Pathophysiology of atherosclerosis plaque progression. Hear. Lung Circ. 2013, 22, 399–411. [Google Scholar] [CrossRef]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim Carotid Intima-Media Thickness and Plaque Consensus (2004–2006–2011) An Update on Behalf of the Advisory Board of the 3rd, 4th and 5th Watching the Risk Symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [PubMed]
- Naqvi, T.Z.; Lee, M.S. Carotid intima-media thickness and plaque in cardiovascular risk assessment. JACC Cardiovasc. Imaging 2014, 7, 1025–1038. [Google Scholar] [CrossRef] [PubMed]
- Rashid, S.A.; Mahmud, S.A. Correlation between carotid artery intima-media thickness and luminal diameter with body mass index and other cardiovascular risk factors in adults. Sultan Qaboos Univ. Med. J. 2015, 15, e344–e350. [Google Scholar] [CrossRef]
- Sarkar, S.; Ghosh, S.; Ghosh, S.K.; Collier, A. Role of transcranial Doppler ultrasonography in stroke. Postgrad. Med. J. 2007, 83, 683–689. [Google Scholar] [CrossRef]
- Branas, C.C.; Weingarten, M.S.; Czeredarczuk, M.; Schafer, P.F. Examination of carotid arteries with quantitative color Doppler flow imaging. J. Ultrasound Med. 1994, 13, 121–127. [Google Scholar] [CrossRef]
- Zou, L.; Cai, Z.; Qiu, Y.; Gui, L.; Mao, L.; Yang, X. CTG-Net: An efficient cascaded framework driven by terminal guidance mechanism for dilated pancreatic duct segmentation. Phys. Med. Biol. 2023, 68, 215006. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Cai, Z.; Qiu, Y.; Gui, L.; Mao, L.; Yang, X. Automated peripancreatic vessel segmentation and labeling based on iterative trunk growth and weakly supervised mechanism. Artif. Intell. Med. 2024, 68, 102825. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Jin, J.; Xu, M.; Wu, H.; He, W.; Yuchi, M.; Ding, M. Ultrasound common carotid artery segmentation based on active shape model. Comput. Math. Methods Med. 2013, 2013, 345968. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.R.H.; Teotia, K.; Raj, P.K.; Andrade, J.; Rajagopal, K.V.; Seelamantula, C.S. Automatic segmentation of common carotid artery in longitudinal mode ultrasound images using active oblongs. In Proceedings of the ICASSP 2019-2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1353–1357. [Google Scholar]
- Qian, C.; Su, E.; Yang, X. Segmentation of the common carotid intima-media complex in ultrasound images using 2-D continuous max-flow and stacked sparse auto-encoder. Ultrasound Med. Biol. 2020, 46, 3104–3124. [Google Scholar] [PubMed]
- Lian, S.; Luo, Z.; Feng, C.; Li, S.; Li, S. APRIL: Anatomical prior-guided reinforcement learning for accurate carotid lumen diameter and intima-media thickness measurement. Med. Image Anal. 2021, 71, 102040. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.F.; Vese, L.A. Active contours without edges. IEEE Trans. Image Process. 2001, 10, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Mumford, D.B.; Shah, J. Optimal approximations by piecewise smooth functions and associated variational problems. Commun. Pure Appl. Math. 1989, 42, 577–685. [Google Scholar]
- Li, C.; Xu, C.; Gui, C.; Fox, M.D. Distance regularized level set evolution and its application to image segmentation. IEEE Trans. Image Process. 2010, 19, 3243–3254. [Google Scholar]
- Caselles, V.; Kimmel, R.; Sapiro, G. Geodesic active contours. Int. J. Comput. Vis. 1997, 22, 61–79. [Google Scholar] [CrossRef]
- Rukundo, O.; Schmidt, S.E.; Von Ramm, O.T. Software implementation of optimized bicubic interpolated scan conversion in echocardiography. arXiv 2020, arXiv:2005.11269. [Google Scholar]
- Rukundo, O.; Schmidt, S.E. Stochastic Rounding for Image Interpolation and Scan Conversion. arXiv 2021, arXiv:2110.12983. [Google Scholar] [CrossRef]
- Cremers, D.; Sochen, N.; Schnörr, C. Towards recognition-based variational segmentation using shape priors and dynamic labeling. In Proceedings of the Scale Space Methods in Computer Vision: 4th International Conference, Scale Space 2003, Isle of Skye, UK, 10–12 June 2003; Springer: Berlin/Heidelberg, Germany; 2003; pp. 388–400. [Google Scholar]
- Tsai, A.; Yezzi, A.; Wells, W.; Tempany, C.; Tucker, D.; Fan, A.; Grimson, W.E.; Willsky, A. A shape-based approach to the segmentation of medical imagery using level sets. IEEE Trans. Med. Imaging 2003, 22, 137–154. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Yang, X.; Chen, Y.; Tang, L. Ultrasound kidney segmentation with a global prior shape. J. Vis. Commun. Image Represent. 2013, 24, 937–943. [Google Scholar] [CrossRef]
- Gui, L.; Ma, J.; Yang, X. Shape prior generation and geodesic active contour interactive iterating algorithm (SPACIAL): Fully automatic segmentation for 3D lumen in intravascular optical coherence tomography images. Med. Phys. 2021, 48, 7099–7111. [Google Scholar] [CrossRef] [PubMed]
- Courant, R.; Friedrichs, K.; Lewy, H. On the partial difference equations of mathematical physics. IBM J. Res. Dev. 1967, 11, 215–234. [Google Scholar] [CrossRef]
- Xie, M.; Li, Y.; Xue, Y.; Huntress, L.; Beckerman, W.; Rahimi, S.; Ady, J.; Roshan, U. Vessel lumen segmentation in carotid artery ultrasounds with the U-Net convolutional neural network. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Republic of Korea, 16–19 December 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 2680–2684. [Google Scholar]
- Huang, Q.; Jia, L.; Ren, G.; Wang, X.; Liu, C. Extraction of vascular wall in carotid ultrasound via a novel boundary-delineation network. Eng. Appl. Artif. Intell. 2023, 121, 106069. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Dice ↑ | Sensitivity ↑ | Specificity ↑ | IOU ↑ | HD ↓ |
|---|---|---|---|---|---|
| CV | 72.36 ± 10.69 | 85.16 ± 0.00 | 93.94 ± 0.00 | 57.75 ± 1.00 | 60.30 ± 64.83 |
| DRLSE | 89.30 ± 3.81 | 91.64 ± 2.67 | 98.20 ± 4.12 | 80.88 ± 5.23 | 13.88 ± 7.61 |
| Proposed | 92.38 ± 3.34 | 97.23 ± 3.34 | 99.42 ± 3.23 | 86.02 ± 1.00 | 10.52 ± 10.13 |
| Parameters | Dice ↑ | Sensitivity ↑ | Specificity ↑ | IOU ↑ | HD ↓ |
|---|---|---|---|---|---|
| , , , | 92.38 ± 3.34 | 97.23 ± 3.34 | 99.42 ± 3.23 | 86.02 ± 1.00 | 10.52 ± 10.13 |
| , , , | 86.57 ± 8.21 | 74.03 ± 11.86 | 99.70 ± 0.64 | 73.03 ± 11.58 | 15.13 ± 14.58 |
| , , , | 90.50 ± 4.31 | 80.33 ± 7.77 | 99.57 ± 0.80 | 78.82 ± 7.50 | 11.20 ± 8.53 |
| , , , | 91.70 ± 3.71 | 82.28 ± 7.04 | 99.62 ± 0.50 | 80.82 ± 6.83 | 10.19 ± 7.52 |
| , , , | 91.52 ± 7.21 | 90.40 ± 3.99 | 97.49 ± 4.54 | 83.18 ± 9.96 | 21.88 ± 29.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Zou, L.; Song, J.; Gong, K. Automated Lumen Segmentation in Carotid Artery Ultrasound Images Based on Adaptive Generated Shape Prior. Bioengineering 2024, 11, 812. https://doi.org/10.3390/bioengineering11080812
Li Y, Zou L, Song J, Gong K. Automated Lumen Segmentation in Carotid Artery Ultrasound Images Based on Adaptive Generated Shape Prior. Bioengineering. 2024; 11(8):812. https://doi.org/10.3390/bioengineering11080812
Chicago/Turabian StyleLi, Yu, Liwen Zou, Jiajia Song, and Kailin Gong. 2024. "Automated Lumen Segmentation in Carotid Artery Ultrasound Images Based on Adaptive Generated Shape Prior" Bioengineering 11, no. 8: 812. https://doi.org/10.3390/bioengineering11080812