
High-Precision Skin Disease Diagnosis through Deep Learning on Dermoscopic Images

 , ,
, , 
Abstract
:1. Introduction
- A Computer Assisted Diagnosis (CAD) framework has been developed to detect skin illnesses at an early stage.
- We suggest a computationally efficient and lightweight deep learning model that utilizes a CNN architecture.
- The study has contributed by providing brief details on related research on the existing problem.
- The study has contributed by comparing shallow learning and deep learning models.
- Data augmentation is the most important measure in the classification of skin diseases, as this knowledge has been generated by performing different experiments.
2. Literature Survey
2.1. Methodology
2.2. Related Work
3. Materials and Methods
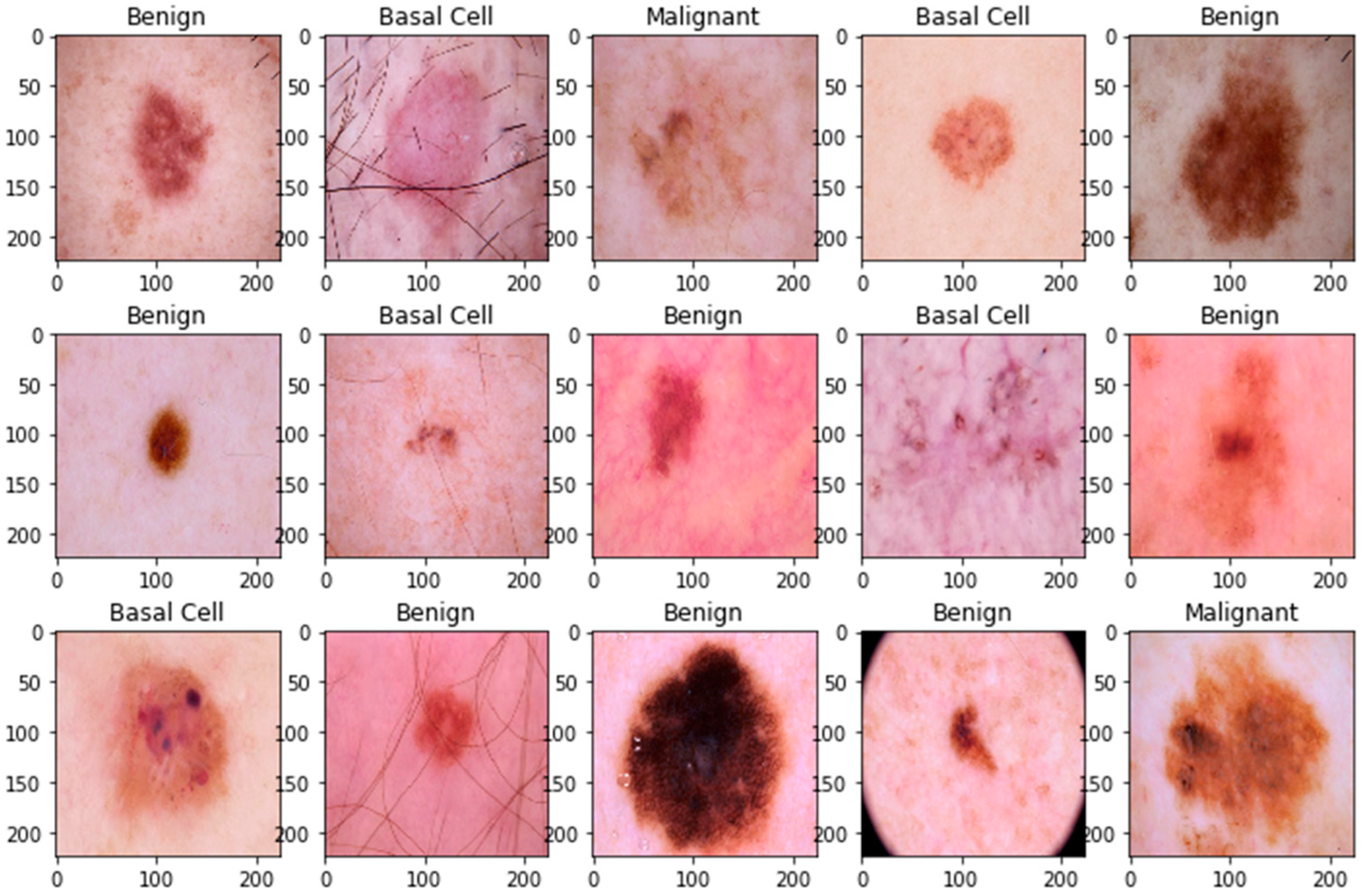
3.1. Datasets and Splitting
3.2. Data Preprocessing
3.3. Data Normalization
3.4. Data Augmentation
3.5. Proposed Framework
3.5.1. Basic CNN Model
3.5.2. Proposed CNN Model
4. Experiments and Results
4.1. Hybrid Model
4.2. Performance Metrics
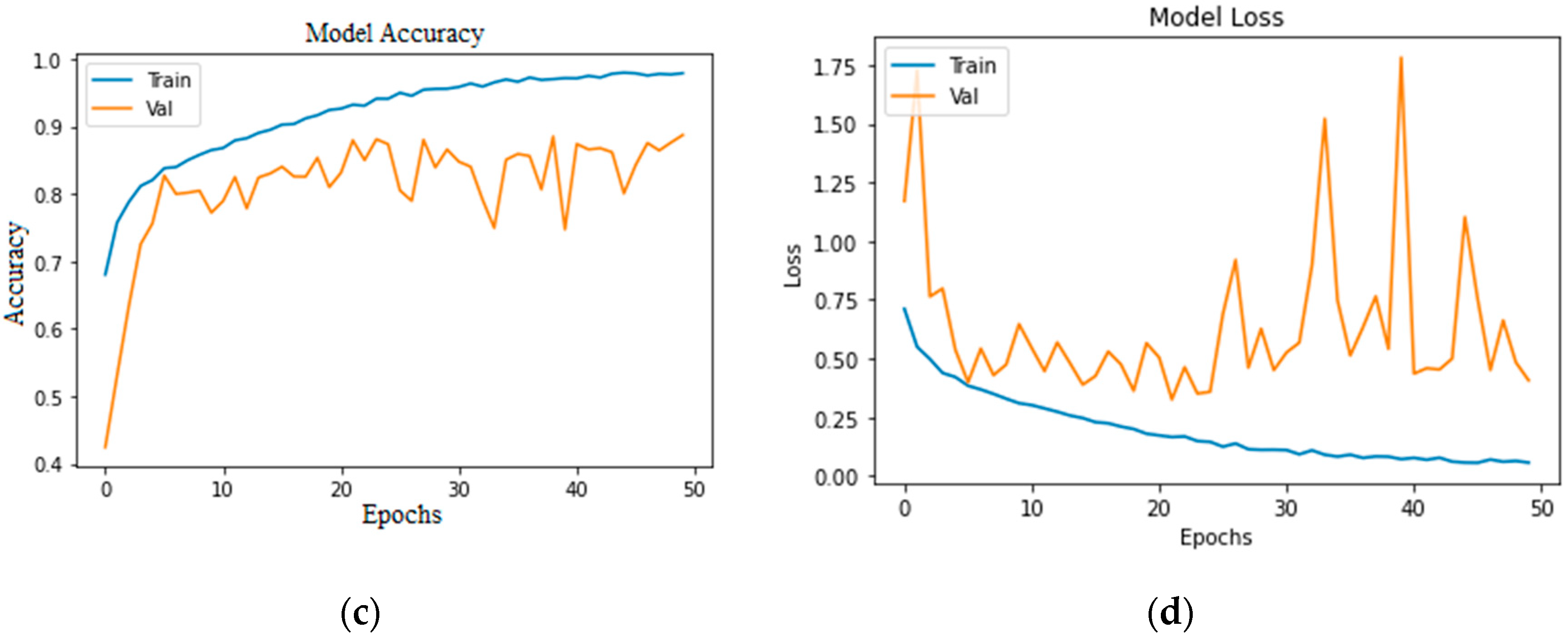
4.3. Accuracy and Loss
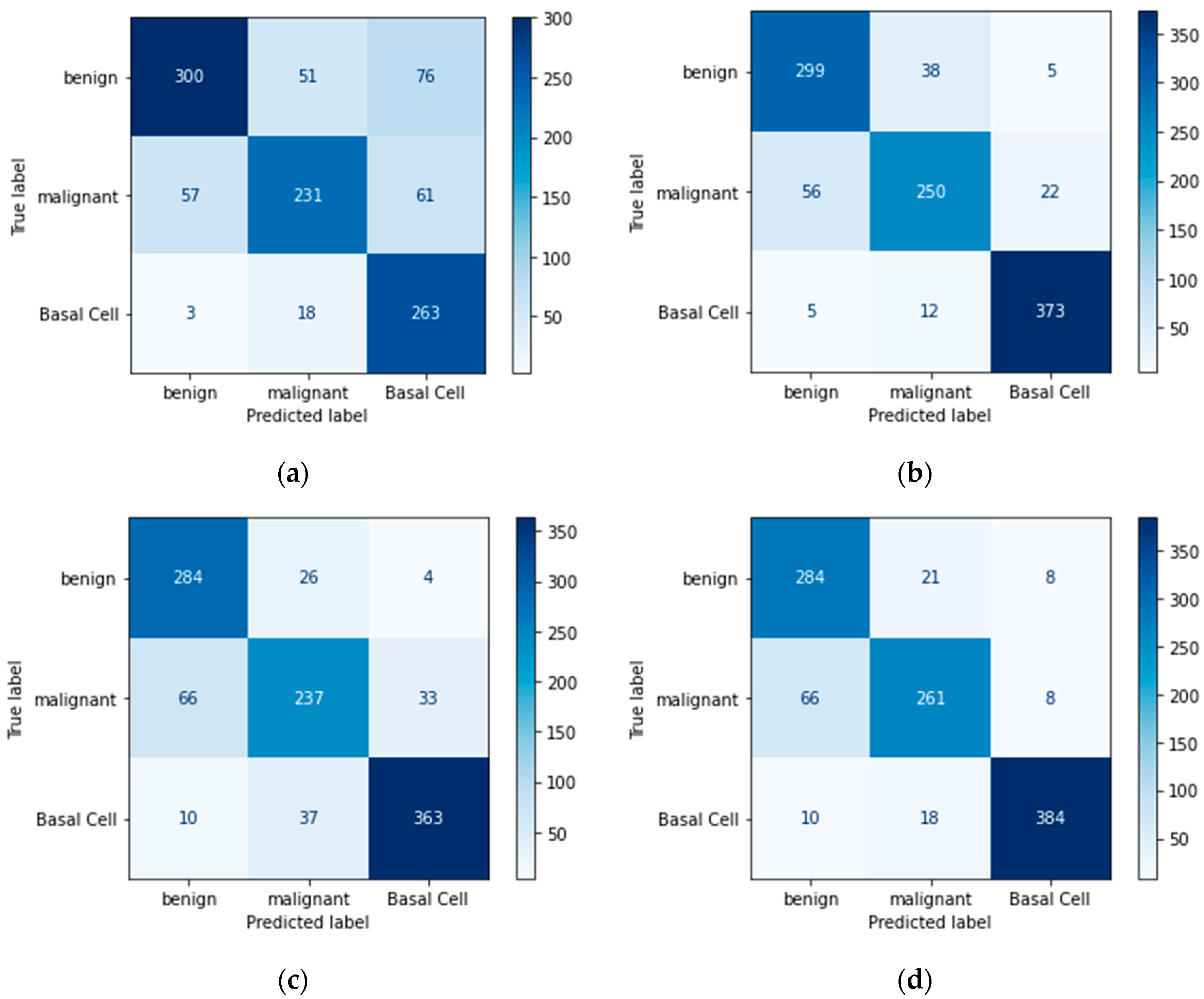
4.4. Confusion Matrix
4.5. Predictive Result
4.6. Comparison of Proposed Method
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Key Statistics for Melanoma Skin Cancer. Available online: https://www.cancer.org/cancer/melanoma-skin-cancer/about/key-statistics.html (accessed on 27 May 2023).
- World Cancer Research Fund. Skin Cancer Statistics. Available online: https://www.wcrf.org/cancer-trends/skin-cancer-statistics/ (accessed on 27 May 2023).
- Mehmood, M.; Abbasi, S.H.; Aurangzeb, K.; Majeed, M.F.; Anwar, M.S.; Alhussein, M. A classifier model for prostate cancer diagnosis using CNNs and transfer learning with multi-parametric MRI. Front. Oncol. 2023, 13, 1225490. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Ullah, I.; Shabaz, M.; Omer, M.F.; Usman, M.T.; Guellil, M.S.; Koo, J. Visionary vigilance: Optimized YOLOV8 for fallen person detection with large-scale benchmark dataset. Image Vis. Comput. 2024, 26, 105195. [Google Scholar] [CrossRef]
- Dildar, M.; Akram, S.; Irfan, M.; Khan, H.U.; Ramzan, M.; Mahmood, A.R.; Alsaiari, S.A.; Saeed, A.H.M.; Alraddadi, M.O.; Mahnashi, M.H. Skin Cancer Detection: A Review Using Deep Learning Techniques. Int. J. Environ. Res. Public Health 2021, 18, 5479. [Google Scholar] [CrossRef]
- Goyal, M.; Knackstedt, T.; Yan, S.; Hassanpour, S. Artificial intelligence-based image classification methods for diagnosis of skin cancer: Challenges and opportunities. Comput. Biol. Med. 2020, 127, 104065. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, Z.; Ma, Y.-K.; Ullah, I.; Al Shloul, T.; Tufail, A.B.; Ghadi, Y.Y.; Khan, M.Z.; Mohamed, H.G. Automated Classification of Brain Tumors from Magnetic Resonance Imaging Using Deep Learning. Brain Sci. 2023, 13, 602. [Google Scholar] [CrossRef]
- Khan, H.U.; Ali, N.; Nazir, S.; Alabdulatif, A.; Arif, M. Multi-criterial based feature selection for health care system. Mob. Netw. Appl. 2023, 1–14. [Google Scholar] [CrossRef]
- Strzelecki, M.H.; Strąkowska, M.; Kozłowski, M.; Urbańczyk, T.; Wielowieyska-Szybińska, D.; Kociołek, M. Skin Lesion Detection Algorithms in Whole Body Images. Sensors 2021, 21, 6639. [Google Scholar] [CrossRef]
- Korotkov, K.; Quintana, J.; Campos, R.; Jesus-Silva, A.; Iglesias, P.; Puig, S.; Malvehy, J.; Garcia, R. An Improved Skin Lesion Matching Scheme in Total Body Photography. IEEE J. Biomed. Health Inform. 2019, 23, 586–598. [Google Scholar] [CrossRef]
- Birkenfeld, J.S.; Tucker-Schwartz, J.M.; Soenksen, L.R.; Avilés-Izquierdo, J.A.; Marti-Fuster, B. Computer-aided classification of suspicious pigmented lesions using wide-field images. Comput. Methods Programs Biomed. 2020, 195, 105631. [Google Scholar]
- Mahmoud, N.M.; Soliman, A.M. Early automated detection system for skin cancer diagnosis using artificial intelligent techniques. Sci. Rep. 2024, 14, 9749. [Google Scholar] [CrossRef]
- Winkler, J.K.; Kommoss, K.S.; Toberer, F.; Enk, A.; Maul, L.V.; Navarini, A.A.; Hudson, J.; Salerni, G.; Rosenberger, A.; Haenssle, H.A. Performance of an automated total body mapping algorithm to detect melanocytic lesions of clinical relevance. Eur. J. Cancer 2024, 202, 114026. [Google Scholar] [CrossRef] [PubMed]
- Hashmani, M.A.; Jameel, S.M.; Rizvi, S.S.H.; Shukla, S. An Adaptive Federated Machine Learning-Based Intelligent System for Skin Disease Detection: A Step toward an Intelligent Dermoscopy Device. Appl. Sci. 2021, 11, 2145. [Google Scholar] [CrossRef]
- Asif, A.; Ahmed, F.; Khan, J.A.; Allogmani, E.; El Rashidy, N.; Manzoor, S.; Anwar, M.S. Machine Learning based Diagnostic Paradigm in Viral and Non-viral Hepatocellular Carcinoma (November 2023). IEEE Access 2024, 12, 37557–37571. [Google Scholar] [CrossRef]
- Park, H.C.; Hong, I.P.; Poudel, S.; Choi, C. Data augmentation based on generative adversarial networks for endoscopic image classification. IEEE Access 2023, 11, 49216–49225. [Google Scholar] [CrossRef]
- Huang, C.; Yu, Y.; Qi, M. Skin Lesion Segmentation Based on Deep Learning. In Proceedings of the 2020 IEEE 20th International Conference on Communication Technology (ICCT), Nanning, China, 28–31 October 2020; pp. 1360–1364. [Google Scholar]
- Polat, K.; Koc, K.O. Detection of Skin Diseases from Dermoscopy Image Using the combination of Convolutional Neural Network and One-versus-All. J. Artif. Intell. Syst. 2020, 2, 80–97. [Google Scholar] [CrossRef]
- Shanthi, T.; Sabeenian, R.S.; Anand, R. Automatic diagnosis of skin diseases using convolution neural network. Microprocess. Microsyst. 2020, 76, 103074. [Google Scholar] [CrossRef]
- Shamshad, N.; Sarwr, D.; Almogren, A.; Saleem, K.; Munawar, A.; Rehman, A.U.; Bharany, S. Enhancing Brain Tumor Classification by a Comprehensive Study on Transfer Learning Techniques and Model Efficiency Using MRI Datasets. IEEE Access 2024, 12, 100407–100418. [Google Scholar] [CrossRef]
- Bajwa, M.N.; Muta, K.; Malik, M.I.; Siddiqui, S.A.; Braun, S.A.; Homey, B.; Dengel, A.; Ahmed, S. Computer-Aided Diagnosis of Skin Diseases Using Deep Neural Networks. Appl. Sci. 2020, 10, 2488. [Google Scholar] [CrossRef]
- Kaur, R.; Gholam Hosseini, H.; Sinha, R.; Lindén, M. Melanoma Classification Using a Novel Deep Convolutional Neural Network with Dermoscopic Images. Sensors 2022, 22, 1134. [Google Scholar] [CrossRef]
- Shahzad, M.; Tahir, M.A.; Alhussein, M.; Mobin, A.; Shams Malick, R.A.; Anwar, M.S. NeuPD—A neural network-based approach to predict antineoplastic drug response. Diagnostics 2023, 13, 2043. [Google Scholar] [CrossRef]
- Rasel, M.A.; Obaidellah, U.H.; Kareem, S.A. Convolutional Neural Network-Based Skin Lesion Classification with Variable Nonlinear Activation Functions. IEEE Access 2022, 10, 83398–83414. [Google Scholar] [CrossRef]
- Zhang, J.; Petitjean, C.; Ainouz, S. Kappa Loss for Skin Lesion Segmentation in Fully Convolutional Network. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; pp. 2001–2004. [Google Scholar]
- Jinnai, S.; Yamazaki, N.; Hirano, Y.; Sugawara, Y.; Ohe, Y.; Hamamoto, R. The Development of a Skin Cancer Classification System for Pigmented Skin Lesions Using Deep Learning. Biomolecules 2020, 10, 1123. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.Q.; Reiff-Marganiec, S. Targeted Ensemble Machine Classification Approach for Supporting IoT Enabled Skin Disease Detection. IEEE Access 2021, 9, 50244–50252. [Google Scholar] [CrossRef]
- Mahbod, A.; Schaefer, G.; Wang, C.; Ecker, R.; Ellinge, I. Skin Lesion Classification Using Hybrid Deep Neural Networks. In Proceedings of the ICASSP 2019–2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 1229–1233. [Google Scholar]
- Abbas, Q.; Ramzan, F.; Ghani, M.U. Acral melanoma detection using dermoscopic images and convolutional neural networks. Vis. Comput. Ind. Biomed. Art 2021, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, Z.; Ma, Y.-K.; Ullah, I.; Ghadi, Y.Y.; Khan, M.Z.; Khan, M.A.; Abdusalomov, A.; Alqahtani, F.; Shehata, A.M. Brain Tumor Classification from MRI Using Image Enhancement and Convolutional Neural Network Techniques. Brain Sci. 2023, 13, 1320. [Google Scholar] [CrossRef]
- Tufail, A.B.; Anwar, N.; Othman, M.T.; Ullah, I.; Khan, R.A.; Ma, Y.K.; Adhikari, D.; Rehman, A.U.; Shafiq, M.; Hamam, H. Early-stage Alzheimer’s disease categorization using PET neuroimaging modality and convolutional neural networks in the 2D and 3D domains. Sensors 2022, 22, 4609. [Google Scholar] [CrossRef]
- Ghosh, H.; Rahat, I.S.; Mohanty, S.N.; Ravindra, J.V.R.; Sobu, A. A Study on the Application of Machine Learning and Deep Learning Techniques for Skin Cancer Detection. World Acad. Sci. Eng. Technol. Int. J. Comput. Syst. Eng. 2024, 18, 51–59. [Google Scholar]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classes | Training Samples 100% | Augmented Training Samples 100% | Total Training Samples 80% | Validation Samples 20% | Test Samples |
|---|---|---|---|---|---|
| MAL | 1197 | 3591 | 2873 | 718 | 300 |
| BEN | 1440 | 4320 | 3456 | 864 | 360 |
| BCC | 1125 | 3375 | 2700 | 675 | 400 |
| Total | 3762 | 11,286 | 9029 | 2257 | 1060 |
| Classes | Training Samples 100% | Augmented Training Samples 100% | Total Training Samples 80% | Validation Samples 20% | Test Samples |
|---|---|---|---|---|---|
| MAL | 1125 | 3375 | 2700 | 675 | 300 |
| BEN | 1125 | 3375 | 2700 | 675 | 360 |
| BCC | 1125 | 3375 | 2700 | 675 | 400 |
| Total | 3375 | 10,125 | 8100 | 2025 | 1060 |
| Hyperparameters | Grid Search | Best Parameter |
|---|---|---|
| Regularization | 0.1, 1, 10, 100 | 0.1 |
| Gamma | 0.0001, 0.001, 0.1, 1 | 0.0001 |
| Kernel | rbf, poly | poly |
| Hyperparameters | Hyperparameters Values |
|---|---|
| Mini Batch-Size | 32 |
| Learning Rate | 0.001 |
| Epochs | 50, 100 |
| Regularization Parameter | 0.00001 |
| Optimization Function | Adam |
| Loss Function | Categorical Cross Entropy |
| Approach | Proposed CNN Model |
|---|---|
| Imbalanced class without augmentation | 0.7490 |
| Imbalanced class with augmentation | 0.8698 |
| Balanced class without augmentation | 0.8339 |
| Balanced class with augmentation | 0.8764 |
| Approach | Basic CNN Model | Proposed CNN Model | SVM | Random Forest |
|---|---|---|---|---|
| Imbalanced class without augmentation | 0.5594 | 0.8179 | 0.7783 | 0.8113 |
| Imbalanced class with augmentation | 0.8471 | 0.8669 | 0.8424 | 0.8462 |
| Balanced class without augmentation | 0.7962 | 0.7339 | 0.7924 | 0.8113 |
| Balanced class with augmentation | 0.7952 | 0.8688 | 0.8226 | 0.8424 |
| Estimators | Accuracy |
|---|---|
| 100 | 0.8160 |
| 200 | 0.8169 |
| 300 | 0.8141 |
| 400 | 0.8216 |
| 500 | 0.8198 |
| Approach | BEN | MAL | BCC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | REC | F-Score | PRE | REC | F-Score | PRE | REC | F-Score | |
| Imbalanced class without augmentation | 0.68 | 0.51 | 0.58 | 1.0 | 0.07 | 0.13 | 0.50 | 0.97 | 0.66 |
| Imbalanced class with augmentation | 0.86 | 0.80 | 0.83 | 0.75 | 0.80 | 0.77 | 0.92 | 0.93 | 0.92 |
| Balanced class without augmentation | 0.85 | 0.76 | 0.80 | 0.66 | 0.77 | 0.71 | 0.87 | 0.85 | 0.86 |
| Balanced class with augmentation | 0.80 | 0.81 | 0.80 | 0.65 | 0.79 | 0.71 | 0.94 | 0.79 | 0.86 |
| Approach | BEN | MAL | BCC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | REC | F-Score | PRE | REC | F-Score | PRE | REC | F-Score | |
| Imbalanced class without augmentation—50 Epochs | 0.78 | 0.82 | 0.80 | 0.74 | 0.80 | 0.77 | 0.92 | 0.83 | 0.88 |
| Imbalanced class with augmentation—50 Epochs | 0.87 | 0.84 | 0.86 | 0.77 | 0.84 | 0.80 | 0.95 | 0.91 | 0.93 |
| Balanced class without augmentation—50 Epochs | 0.73 | 0.79 | 0.76 | 0.62 | 0.88 | 0.72 | 0.95 | 0.57 | 0.71 |
| Balanced class with augmentation—50 Epochs | 0.86 | 0.86 | 0.86 | 0.79 | 0.81 | 0.80 | 0.94 | 0.93 | 0.93 |
| Imbalanced class without augmentation—100 Epochs | 0.70 | 0.83 | 0.76 | 0.66 | 0.77 | 0.71 | 0.93 | 0.66 | 0.77 |
| Imbalanced class with augmentation—100 Epochs | 0.87 | 0.83 | 0.85 | 0.76 | 0.83 | 0.80 | 0.96 | 0.93 | 0.94 |
| Balanced class without augmentation—100 Epochs | 0.90 | 0.79 | 0.84 | 0.71 | 0.79 | 0.75 | 0.89 | 0.91 | 0.90 |
| Balanced class with augmentation—100 Epochs | 0.91 | 0.79 | 0.84 | 0.78 | 0.87 | 0.82 | 0.93 | 0.96 | 0.95 |
| Approach | BEN | MAL | BCC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | REC | F-Score | PRE | REC | F-Score | PRE | REC | F-Score | |
| Imbalanced class without augmentation | 0.73 | 0.82 | 0.77 | 0.70 | 0.66 | 0.68 | 0.89 | 0.82 | 0.86 |
| Imbalanced class with augmentation | 0.80 | 0.86 | 0.83 | 0.78 | 0.71 | 0.74 | 0.93 | 0.93 | 0.93 |
| Balanced class without augmentation | 0.75 | 0.83 | 0.79 | 0.72 | 0.68 | 0.70 | 0.89 | 0.84 | 0.87 |
| Balanced class with augmentation | 0.79 | 0.83 | 0.81 | 0.73 | 0.69 | 0.71 | 0.92 | 0.92 | 0.92 |
| Approach | BEN | MAL | BCC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | REC | F-Score | PRE | REC | F-Score | PRE | REC | F-Score | |
| Imbalanced class without augmentation | 0.85 | 0.78 | 0.81 | 0.70 | 0.76 | 0.73 | 0.87 | 0.88 | 0.87 |
| Imbalanced class with augmentation | 0.86 | 0.77 | 0.81 | 0.73 | 0.80 | 0.76 | 0.92 | 0.95 | 0.94 |
| Balanced class without augmentation | 0.85 | 0.78 | 0.81 | 0.70 | 0.76 | 0.73 | 0.87 | 0.88 | 0.87 |
| Balanced class with augmentation | 0.88 | 0.75 | 0.81 | 0.72 | 0.81 | 0.76 | 0.91 | 0.95 | 0.93 |
| Actual Labels | |||
|---|---|---|---|
| Positive (1) | Negative (0) | ||
| Predicted Labels | Positive (1) | TP | FP |
| Negative (0) | FN | TN | |
| Paper No/Authors | Model | Dataset | Result |
|---|---|---|---|
| [18] Kemal et al. | CNN | HAM10000 | Accuracy: 77% to 92.9% |
| [19] Shanthi et al. | AlexNet | DermNet (acne, keratosis, eczema herpeticum) | Accuracy: 85.7%, 92.3%, 93.3%, and 92.8% for acne, keratosis, eczema herpeticum, and utricaria, respectively |
| [21] Bajwa et al. | ResNet-152, DenseNet-161, SE-ResNeXt-101, and NASNet | DermNet and ISIC | Accuracy: DermNet: 98% ISIC: 99% |
| [22] Kaur et al. | DCNN | ISIC, PH2(for testing) (Melanoma and Benign) | Accuracy: 81.41% to 90.42% |
| [24] Rasel et al. | CNN | PH2 and ISIC | Accuracy: 97.50% |
| [25] Zhang et al. | U-Net | SCD, ISIC | N/A |
| [26] Jinnai et al. | FRCNN | 5846 clinical images collected from patients | Accuracy: 86.2% |
| [27] Yu et al. | VGG16, Inception, Xception, MobileNet, ResNet50 and DenseNet161 | HAM10000 | Accuracy: DensNet: 86.5%, ResNet: 83.7%, MobileNet: 82.4%, Inception: 82.8%. Overall evaluation: 98.48% |
| [28] Mahbod et al. | AlexNet, VGG-16, ResNet-18, SVM classifier | ISIC | Accuracy: melanoma: 83.83% Seborrheic keratosis: 97.55% |
| [29] Abbas et al. | CNN | Acral Melanoma vs. Benign | Accuracy: 91.03% |
| Proposed Method | CNN | ISIC | Accuracy: 87.64% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malik, S.G.; Jamil, S.S.; Aziz, A.; Ullah, S.; Ullah, I.; Abohashrh, M. High-Precision Skin Disease Diagnosis through Deep Learning on Dermoscopic Images. Bioengineering 2024, 11, 867. https://doi.org/10.3390/bioengineering11090867
Malik SG, Jamil SS, Aziz A, Ullah S, Ullah I, Abohashrh M. High-Precision Skin Disease Diagnosis through Deep Learning on Dermoscopic Images. Bioengineering. 2024; 11(9):867. https://doi.org/10.3390/bioengineering11090867
Chicago/Turabian StyleMalik, Sadia Ghani, Syed Shahryar Jamil, Abdul Aziz, Sana Ullah, Inam Ullah, and Mohammed Abohashrh. 2024. "High-Precision Skin Disease Diagnosis through Deep Learning on Dermoscopic Images" Bioengineering 11, no. 9: 867. https://doi.org/10.3390/bioengineering11090867
APA StyleMalik, S. G., Jamil, S. S., Aziz, A., Ullah, S., Ullah, I., & Abohashrh, M. (2024). High-Precision Skin Disease Diagnosis through Deep Learning on Dermoscopic Images. Bioengineering, 11(9), 867. https://doi.org/10.3390/bioengineering11090867