Smart Wound Dressings for Diabetic Chronic Wounds


Abstract
:1. Background
2. Chronic Inflammation in Diabetic Wounds
3. Current Treatment and Challenges
4. Current Wound Dressings
4.1. Natural Polymers
4.1.1. Cellulose
4.1.2. Chitosan
4.1.3. Collagen and Gelatin
4.1.4. Hyaluronic Acid
4.2. Synthetic Polymers
4.2.1. Poly(lactide-co-glycolide)
4.2.2. Polyurethanes
4.2.3. Polyethylene Glycol
4.2.4. Polycaprolactone
4.3. Smart Polymers
4.4. Fiber Geometry and Scaffold Architecture
5. Biosensing in the Chronic Wound Environment
5.1. Biomarkers for Wound Healing
5.1.1. Biochemical Markers
5.1.2. Physical Biomarkers
5.2. Biochemical Sensors
5.2.1. Matrix Metalloproteinases
5.2.2. Uric Acid
5.2.3. pH
5.2.4. Bacterial
5.2.5. Nitric Oxide
5.2.6. Oxygen
5.3. Physical Sensors
5.3.1. Impedance
5.3.2. Temperature Sensors
5.3.3. Integrated Sensors
6. Sensor Clinical Outcomes
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2014.
- Reiber, G.; Lipsky, B.; Gibbons, G. The burden of diabetic foot ulcers. Am. J. Surg. 1998, 176, 5S–10S. [Google Scholar] [CrossRef]
- Dahiru, I.; Amaefule, K.; Okpe, I.; Ibrahim, A.; Muazu, S. An overview of diabetic foot disease. Niger. J. Basic Clin. Sci. 2016, 13, 1. [Google Scholar] [CrossRef]
- Siddiqui, A.R.; Bernstein, J.M. Chronic wound infection: Facts and controversies. Clin. Dermatol. 2010, 28, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Jeffcoate, W.J.; Harding, K.G. Diabetic foot ulcers. Lancet 2003, 361, 1545–1551. [Google Scholar] [CrossRef]
- Moxey, P.W.; Gogalniceanu, P.; Hinchliffe, R.J.; Loftus, I.M.; Jones, K.J.; Thompson, M.M.; Holt, P.J. Lower extremity amputations—A review of global variability in incidence. Diabet. Med. 2011, 28, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Health Statistics|NIDDK. Available online: https://www.niddk.nih.gov/health-information/health-statistics#category=diabetes (accessed on 17 May 2018).
- Davis, F.M.; Kimball, A.; Boniakowski, A.; Gallagher, K.; Gallagher, K. Dysfunctional Wound Healing in Diabetic Foot Ulcers: New Crossroads. Curr. Diabetes Rep. 2018, 18, 2. [Google Scholar] [CrossRef] [PubMed]
- Syeda, M.M.; Jing, X.; Mirza, R.H.; Yu, H.; Sellers, R.S.; Chi, Y. Prostaglandin transporter modulates wound healing in diabetes by regulating prostaglandin-induced angiogenesis. Am. J. Pathol. 2012, 181, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Mohd, J.; Shah, Y.; Omar, E.; Pai, D.R.; Sood, S. Cellular events and biomarkers of wound healing. Indian J. Plast. Surg. 2012, 45, 220. [Google Scholar]
- Greene, D.A.; Stevens, M.J.; Feldman, E.L. Diabetic neuropathy: Scope of the syndrome. Am. J. Med. 1999, 107, 2S–8S. [Google Scholar] [CrossRef]
- Alavi, A.; Sibbald, R.G.; Mayer, D.; Goodman, L.; Botros, M.; Armstrong, D.G.; Woo, K.; Boeni, T.; Ayello, E.A.; Kirsner, R.S. Diabetic foot ulcers: Part I. Pathophysiology and prevention. J. Am. Acad. Dermatol. 2014, 70, 1.e1–1.e18. [Google Scholar] [CrossRef] [PubMed]
- Mowat, A.G.; Baum, J. Chemotaxis of polymorphonuclear leukocytes from patients with diabetes mellitus. N. Engl. J. Med. 1971, 284, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Chin, G.A.; Diegelmann, R.F.; Schultz, G.S. Cellular and molecular regulation of wound healing. Basic Clin. Dermatol. 2005, 33, 17. [Google Scholar]
- Johnson, S.; Branthwaite, H.; Naemi, R.; Chockalingam, N. The effect of three different toe props on plantar pressure and patient comfort. J. Foot Ankle Res. 2012, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Birke, J.A.; Franks, B.D.; Foto, J.G. First ray joint limitation, pressure, and ulceration of the first metatarsal head in diabeties melitus. Foot Ankle Int. 1995, 15, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Jain, A. A new classification of diabetic foot complications: A simple and effective teaching tool. J. Diabet. Foot Complicat. 2012, 4, 1–5. [Google Scholar]
- Lipsky, B.A. A current approach to diabetic foot infections. Curr. Infect. Dis. Rep. 1999, 1, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Tentolouris, N.; Jude, E.B.; Smirnof, I.; Knowles, E.A.; Boulton, A.J. Methicillin-resistant Staphylococcus aureus: An increasing problem in a diabetic foot clinic. Diabet. Med. 1999, 16, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Berendt, A.R. Principles and practice of antibiotic therapy of diabetic foot infections. Diabetes Metab. Res. Rev. 2000, 16, S42–S46. [Google Scholar] [CrossRef]
- Valenta, C.; Auner, B.G. The use of polymers for dermal and transdermal delivery. Eur. J. Pharm. Biopharm. 2004, 58, 279–289. [Google Scholar] [CrossRef] [PubMed]
- LaRiviere, C.A.; Goldin, A.B.; Avansino, J. Silver toxicity with the use of silver-impregnated dressing and wound vacuum-assisted closure in an immunocompromised patient. J. Am. Coll. Certif. Wound Spec. 2011, 3, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Falanga, V. Classifications for wound bed preparation and stimulation of chronic wounds: Editorial. Wound Repair Regen. 2000, 8, 347–352. [Google Scholar] [PubMed]
- Harding, K.G.; Jones, V.; Price, P. Topical Treatment: which dressing to choose. Diabetes Metab. Res. Rev. 2000, 16, S47–S50. [Google Scholar] [CrossRef]
- O’Meara, S.; Cullum, N.; Majid, M.; Sheldon, T. Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration. Health Technol. Assess. 2000, 4, 1–237. [Google Scholar] [PubMed]
- Mason, J.; O’Keeffe, C.; Hutchinson, A.; McIntosh, A.; Young, R.; Booth, A. A systematic review of foot ulcer in patients with Type 2 diabetes mellitus. II: Treatment. Diabet. Med. 1999, 16, 889–909. [Google Scholar] [CrossRef] [PubMed]
- Bradley, M.; Cullum, N.; Nelson, E.A.; Petticrew, M.; Sheldon, T.; Torgerson, D. Systematic reviews of wound care management: (2). Dressings and topical agents used in the healing of chronic wounds. Health Technol. Assess. 1999, 3, 1–35. [Google Scholar] [PubMed]
- Wu, L.; Norman, G.; Dumville, J.C.; O’Meara, S.; Bell-Syer, S.E. Dressings for treating foot ulcers in people with diabetes: An overview of systematic reviews. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Moura, L.I.F.; Dias, A.M.A.; Carvalho, E.; de Sousa, H.C. Recent advances on the development of wound dressings for diabetic foot ulcer treatment—A review. Acta Biomater. 2013, 9, 7093–7114. [Google Scholar] [CrossRef] [PubMed]
- Strauss, M.B. Surgical treatment of problem foot wounds in patients with diabetes. Clin. Orthop. Relat. Res. 2005, 439, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, L.; Nasiri, M.; Adarvishi, S. Literature review on the management of diabetic foot ulcer. World J. Diabetes 2015, 6, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Mulder, M. The selection of wound care products for wound bed preparation: Wound care. Prof. Nurs. Today 2011, 15, 30–36. [Google Scholar]
- Wittaya-Areekul, S.; Prahsarn, C. Development and in vitro evaluation of chitosan-polysaccharides composite wound dressings. Int. J. Pharm. 2006, 313, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Mano, J.F.; Silva, G.A.; Azevedo, H.S.; Malafaya, P.B.; Sousa, R.A.; Silva, S.S.; Boesel, L.F.; Oliveira, J.M.; Santos, T.C.; Marques, A.P.; et al. Natural origin biodegradable systems in tissue engineering and regenerative medicine: Present status and some moving trends. J. R. Soc. Interface 2007, 4, 999–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serafica, G.; Mormino, R.; Oster, G.A.; Lentz, K.E.; Koehler, K.P. Microbial Cellulose Wound Dressing for Treating Chronic Wounds. U.S. Patent 7704523B2, 30 April 2003. [Google Scholar]
- Brassolatti, P.; Kido, H.W.; Bossini, P.S.; Gabbai-Armelin, P.R.; Otterço, A.N.; Almeida-Lopes, L.; Zanardi, L.M.; Napolitano, M.A.; de Avó, L.R.D.S.; Forato, L.A.; et al. Bacterial cellulose membrane used as biological dressings on third-degree burns in rats. Biomed. Mater. Eng. 2018, 29, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Hussain, Z.; Thu, H.E.; Shuid, A.N.; Katas, H.; Hussain, F. Recent advances in polymer-based wound dressings for the treatment of diabetic foot ulcer: An overview of state-of-the-art. Curr. Drug Targets 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Naseri-Nosar, M.; Ziora, Z.M. Wound dressings from naturally-occurring polymers: A review on homopolysaccharide-based composites. Carbohydr. Polym. 2018, 189, 379–398. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Leong, K.-F.; Du, Z.; Chua, C.-K. The Design of Scaffolds for Use in Tissue Engineering. Part II. Rapid Prototyp. Tech. 2004. [Google Scholar] [CrossRef]
- Dai, T.; Tanaka, M.; Huang, Y.-Y.; Hamblin, M. Chitosan preparation for wounds and burns: Antimicrobial and wound healing effects. Expert Rev. Anti-Infect. Ther. 2012, 9, 857–879. [Google Scholar] [CrossRef] [PubMed]
- Pérez, R.A.; Won, J.E.; Knowles, J.C.; Kim, H.W. Naturally and synthetic smart composite biomaterials for tissue regeneration. Adv. Drug Deliv. Rev. 2013, 65, 471–496. [Google Scholar] [CrossRef] [PubMed]
- Stricker-Krongrad, A.H.; Alikhassy, Z.; Matsangos, N.; Sebastian, R.; Marti, G.; Lay, F.; Harmon, J.W. Efficacy of chitosan-based dressing for control of bleeding in excisional wounds. Eplasty 2018, 18, e14. [Google Scholar] [PubMed]
- Lin, W.C.; Lien, C.C.; Yeh, H.J.; Yu, C.M.; Hsu, S.H. Bacterial cellulose and bacterial cellulose-chitosan membranes for wound dressing applications. Carbohydr. Polym. 2013, 94, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, R.M.; Abdel-Mohsen, A.M.; Hrdina, R.; Burgert, L.; Fohlerova, Z.; Pavliňák, D.; Sayed, O.N.; Jancar, J. Wound dressing based on chitosan/hyaluronan/nonwoven fabrics: Preparation, characterization and medical applications. Int. J. Biol. Macromol. 2016, 89, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Arul, V.; Kartha, R.; Jayakumar, R. A therapeutic approach for diabetic wound healing using biotinylated GHK incorporated collagen matrices. Life Sci. 2007, 80, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Sell, S.A.; Wolfe, P.S.; Garg, K.; McCool, J.M.; Rodriguez, I.A.; Bowlin, G.L. The Use of Natural Polymers in Tissue Engineering: A Focus on Electrospun Extracellular Matrix Analogues. Polymers 2010, 2, 522–553. [Google Scholar] [CrossRef] [Green Version]
- Wiegand, C.; Elsner, P.; Hipler, U.-C.; Klemm, D. Protease and ROS activities influenced by a composite of bacterial cellulose and collagen type I in vitro. Cellulose 2006, 13, 689–696. [Google Scholar] [CrossRef]
- Singh, O.; Gupta, S.S.; Soni, M.; Moses, S.; Shukla, S.; Mathur, R.K. Collagen dressing versus conventional dressings in burn and chronic wounds: A retrospective study. J. Cutan. Aesthet. Surg. 2011, 4, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.-K.; Youn, H.-H.; Park, C.-S.; Song, K.-Y.; Park, J.-K. Reinforced bioartificial dermis constructed with collagen threads. Biotechnol. Bioprocess Eng. 2008, 13, 745–751. [Google Scholar] [CrossRef]
- Kanda, N.; Morimoto, N.; Ayvazyan, A.A.; Takemoto, S.; Kawai, K.; Nakamura, Y.; Sakamoto, Y.; Taira, T.; Suzuki, S. Evaluation of a novel collagen-gelatin scaffold for achieving the sustained release of basic fibroblast growth factor in a diabetic mouse model. J. Tissue Eng. Regen. Med. 2014, 8, 29–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campo, G.M.; Avenoso, A.; Campo, S.; D’Ascola, A.; Nastasi, G.; Calatroni, A. Molecular size hyaluronan differently modulates toll-like receptor-4 in LPS-induced inflammation in mouse chondrocytes. Biochimie 2010, 92, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Ghazi, K.; Deng-Pichon, U.; Warnet, J.M.; Rat, P. Hyaluronan fragments improve wound healing on in vitro cutaneous model through P2X7 purinoreceptor basal activation: Role of molecular weight. PLoS ONE 2012, 7, e48351. [Google Scholar] [CrossRef] [PubMed]
- Simman, R.; Mari, W.; Younes, S.; Wilson, M. Use of hyaluronic acid–based biological bilaminar matrix in wound bed preparation: A case series. Eplasty 2018, 18, e17. [Google Scholar] [PubMed]
- Zhong, S.P.; Zhang, Y.Z.; Lim, C.T. Tissue scaffolds for skin wound healing and dermal reconstruction. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2010, 2, 510–525. [Google Scholar] [CrossRef] [PubMed]
- Lü, J.M.; Wang, X.; Marin-Muller, C.; Wang, H.; Lin, P.H.; Yao, Q.; Chen, C. Current advances in researcn and clinical applications of PLGA-based nanotechnology. Expert Rev. Mol. Diagn. 2009, 9, 325–341. [Google Scholar] [CrossRef] [PubMed]
- Mir, M.; Ali, M.N.; Barakullah, A.; Gulzar, A.; Arshad, M.; Fatima, S.; Asad, M. Synthetic polymeric biomaterials for wound healing: A review. Prog. Biomater. 2018, 7, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.F.; Woodrow, K.A. Relationships between mechanical properties and drug release from electrospun fibers of PCL and PLGA blends. J. Mech. Behav. Biomed. Mater. 2017, 65, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Liu, Y.; Huang, W.; Mo, Y.; Lan, Y.; Guo, R.; Cheng, B. Neurotensin-loaded PLGA/CNC composite nanofiber membranes accelerate diabetic wound healing. Artif. Cells Nanomed. Biotechnol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Xu, J.; Wang, W.; Luo, H.; Liang, X.; Zhang, L.; Wang, H.; Wang, P.; Chang, J. Repair effect of diabetic ulcers with recombinant human epidermal growth factor loaded by sustained-release microspheres. Sci. China Ser. C Life Sci. 2008, 51, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Khil, M.-S.; Cha, D.-I.; Kim, H.-Y.; Kim, I.-S.; Bhattarai, N. Electrospun nanofibrous polyurethane membrane as wound dressing. J. Biomed. Mater. Res. 2003, 67, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Barrett, S. Mepilex® Ag: An antimicrobial, absorbent. Br. J. Nurs. 2009, 18, S28–S36. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.Y.; Cobain, E.; Huard, J.; Huang, L. Thermosensitive hydrogel PEG-PLGA-PEG enhances engraftment of muscle-derived stem cells and promotes healing in diabetic wound. Mol. Ther. 2007, 15, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, D.H.; Osman, M.A.; El-Gizawy, S.A.; Hawthorne, S.J.; Faheem, A.M.; McCarron, P.A. Effect of poly(ethylene glycol) on insulin stability and cutaneous cell proliferation in vitro following cytoplasmic delivery of insulin-loaded nanoparticulate carriers—A potential topical wound management approach. Eur. J. Pharm. Sci. 2018, 114, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Shahverdi, S.; Hajimiri, M.; Esfandiari, M.A.; Larijani, B.; Atyabi, F.; Rajabiani, A.; Dehpour, A.R.; Gharehaghaji, A.A.; Dinarvand, R. Fabrication and structure analysis of poly(lactide-co-glycolic acid)/silk fibroin hybrid scaffold for wound dressing applications. Int. J. Pharm. 2014, 473, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Lu, M.; Zhu, G.; Gao, H.; Xie, L.; Zhang, X.; Ye, C.; Wang, Y.; Sun, C.; Li, X. Acceleration of diabetic-wound healing with PEGylated rhaFGF in healing-impaired streptozocin diabetic rats. Wound Repair Regen. 2011, 19, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Tan, B.H. Towards the development of polycaprolactone based amphiphilic block copolymers: Molecular design, self-assembly and biomedical applications. Mater. Sci. Eng. C 2015, 45, 620–634. [Google Scholar] [CrossRef] [PubMed]
- Kakkar, P.; Verma, S.; Manjubala, I.; Madhan, B. Development of keratin-chitosan-gelatin composite scaffold for soft tissue engineering. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 45, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Reshmi, C.R.; Suja, P.S.; Manaf, O.; Sanu, P.P.; Sujith, A. Nanochitosan enriched poly ε-caprolactone electrospun wound dressing membranes: A fine tuning of physicochemical properties, hemocompatibility and curcumin release profile. Int. J. Biol. Macromol. 2018, 108, 1261–1272. [Google Scholar]
- Wang, X.; You, C.; Hu, X.; Zheng, Y.; Li, Q.; Feng, Z.; Sun, H.; Gao, C.; Han, C. The roles of knitted mesh-reinforced collagen-chitosan hybrid scaffold in the one-step repair of full-thickness skin defects in rats. Acta Biomater. 2013, 9, 7822–7832. [Google Scholar] [CrossRef] [PubMed]
- Harkins, A.L.; Duri, S.; Kloth, L.C.; Tran, C.D. Chitosan-cellulose composite for wound dressing material. Part 2. Antimicrobial activity, blood absorption ability, and biocompatibility. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 1199–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, R.D.; Berry, M.G.; Navsaria, H.A. Hyaluronic acid: The scientific and clinical evidence. J. Plast. Reconstr. Aesthet. Surg. 2007, 60, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.; Martino, M.M.; Hubbell, J.A. Biomimetic materials in tissue engineering. Mater. Today 2010, 13, 14–22. [Google Scholar] [CrossRef]
- Liao, Y.-H.; Jones, S.A.; Forbes, B.; Martin, G.P.; Brown, M.B. Hyaluronan: Pharmaceutical Characterization and Drug Delivery. Drug Deliv. 2005, 12, 327–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koetting, M.C.; Peters, J.T.; Steichen, S.D.; Peppas, N.A. Stimulus-responsive hydrogels: Theory, modern advances, and applications. Mater. Sci. Eng. R Rep. 2015, 93, 1–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dissemond, J.; Witthoff, M.; Brauns, T.C.; Haberer, D.; Goos, M. pH values in chronic wounds. Evaluation during modern wound therapy. Hautarzt 2003, 54, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Cheng, S.-X.; Zhang, X.-Z.; Zhuo, R.-X. Thermo-sensitive polymeric micelles based on poly(N-isopropylacrylamide) as drug carriers. Prog. Polym. Sci. 2009, 34, 893–910. [Google Scholar] [CrossRef]
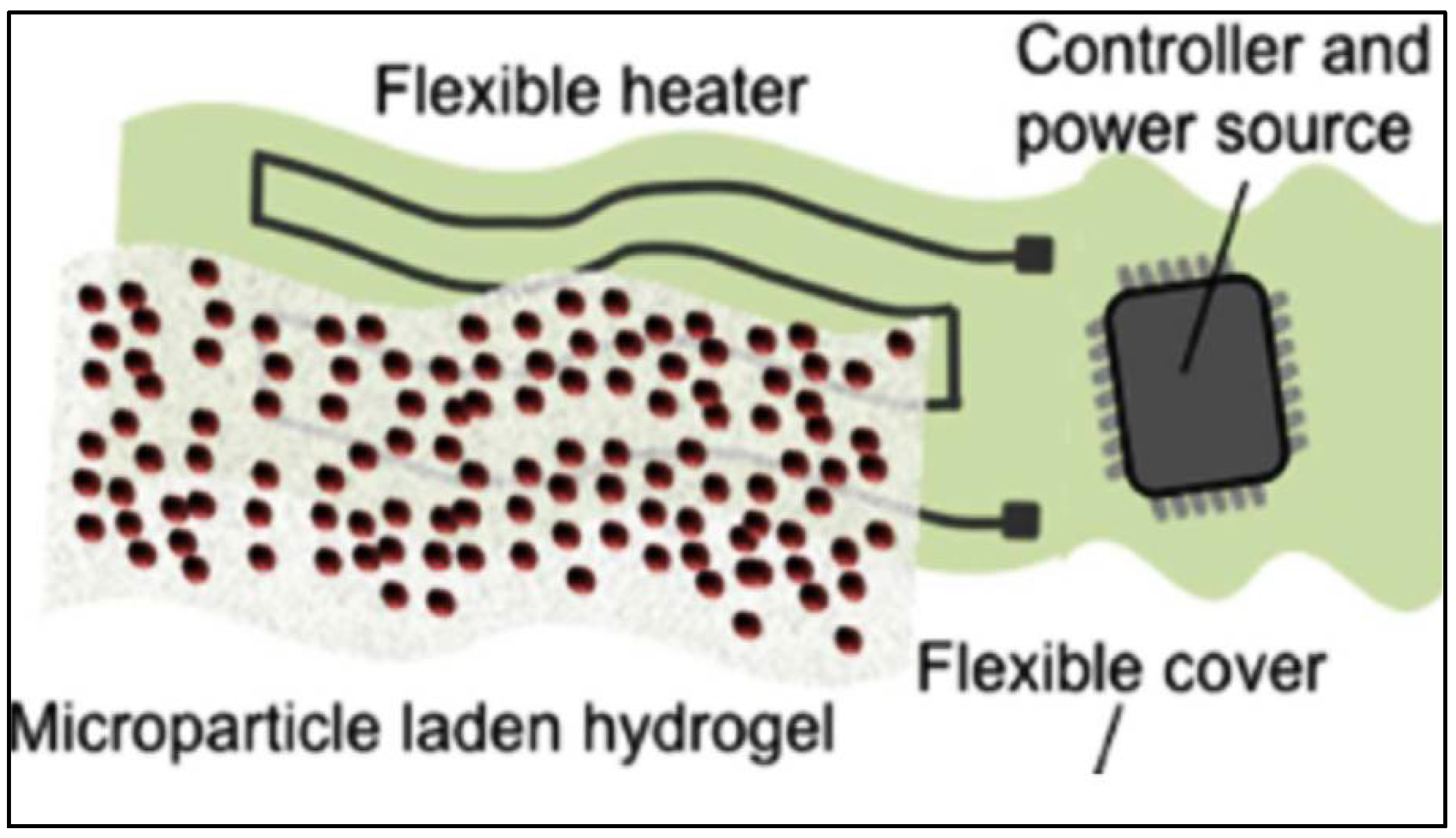
- Bagherifard, S.; Tamayol, A.; Mostafalu, P.; Akbari, M.; Comotto, M.; Annabi, N.; Ghaderi, M.; Sonkusale, S.; Dokmeci, M.R.; Khademhosseini, A. Dermal patch with integrated flexible heater for on demand drug delivery. Adv. Healthc. Mater. 2016, 5, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Tamayol, A.; Akbari, M.; Zilberman, Y.; Comotto, M.; Lesha, E.; Serex, L.; Bagherifard, S.; Chen, Y.; Fu, G.; Ameri, S.K.; et al. Flexible pH-sensing hydrogel fibers for epidermal applications. Adv. Heal. Mater. 2016, 5, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.; Yilgor, I.; Yilgor, E.; Erman, B. Electrospinning of polyurethane fibers. Polymer 2002, 43, 3303–3309. [Google Scholar] [CrossRef]
- Lendlein, A.; Langer, R. Biodegradable, elastic shape-memory polymers for potential biomedical applications. Science 2002, 296, 1673–1676. [Google Scholar] [CrossRef] [PubMed]
- Deitzel, J.; Kleinmeyer, J.; Harris, D.; Tan, N.B. The effect of processing variables on the morphology of electrospun nanofibers and textiles. Polymer 2001, 42, 261–272. [Google Scholar] [CrossRef]
- Gilmore, J.; Yin, F.; Burg, K.J.L. Evaluation of permeability and fluid wicking in woven fiber bone scaffolds. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Xia, T.; Zhi, W.; Wei, L.; Weng, J.; Zhang, C.; Li, X. Promotion of skin regeneration in diabetic rats by electrospun core-sheath fibers loaded with basic fibroblast growth factor. Biomaterials 2011, 32, 4243–4254. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, A.T.A.; Young, A. Smart dressings for the prevention of infection in pediatric burns patients. Expert Rev. Anti. Infect. Ther. 2010, 8, 1063–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLister, A.; McHugh, J.; Cundell, J.; Davis, J. New developments in smart bandage technologies for wound diagnostics. Adv. Mater. 2016, 28, 5732–5737. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Moore, M. Bioelectrical impedance assessment of wound healing. J. Diabetes Sci. Technol. 2012, 6, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Touhami, A. Biosensors and nanobiosensors: Design and applications. In Nanomedicine; One Center Press: Cheshire, UK, 2014; pp. 374–400. [Google Scholar]
- Boykin, J.V., Jr. Wound nitric oxide bioactivity: A promising diagnostic indicator for diabetic foot ulcer management. J. Wound Ostomy Cont. Nurs. 2010, 37, 33–34. [Google Scholar] [CrossRef] [PubMed]
- Biela, A.; Watkinson, M.; Meier, U.C.; Baker, D.; Giovannoni, G.; Becer, C.R.; Krause, S. Disposable MMP-9 sensor based on the degradation of peptide cross-linked hydrogel films using electrochemical impedance spectroscopy. Biosens. Bioelectron. 2015, 68, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Utz, E.R.; Elster, E.A.; Tadaki, D.K.; Gage, F.; Perdue, P.W.; Forsberg, J.A.; Stojadinovic, A.; Hawksworth, J.S.; Brown, T.S. Metalloproteinase expression is associated with traumatic wound failure. J. Surg. Res. 2010, 159, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Young, L. Identifying infection in chronic wounds. Wound Pract. Res. 2012, 20, 38–44. [Google Scholar]
- Privetta, B.J.; Shinb, J.H.; Schoenfisch, M.H. Tutorial Review: Electrochemical Nitric Oxide Sensors for Physiological Measurements. Chem. Soc. Rev. 2010, 14, 384–399. [Google Scholar]
- Kassal, P.; Kim, J.; Kumar, R.; de Araujo, W.R.; Steinberg, I.M.; Steinberg, M.D.; Wang, J. Smart bandage with wireless connectivity for uric acid biosensing as an indicator of wound status. Electrochem. Commun. 2015, 56, 6–10. [Google Scholar] [CrossRef]
- Ferber, R.; Webber, T.; Everett, B.; Groenland, M. Validation of plantar pressure measurements for a novel in-shoe plantar sensory replacement unit. J. Diabetes Sci. Technol. 2013, 7, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Houghton, V.J.; Bower, V.M.; Chant, D.C. Is an increase in skin temperature predictive of neuropathic foot ulceration in people with diabetes? A systematic review and meta-analysis. J. Foot Ankle Res. 2013, 6, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocchitta, G.; Spanu, A.; Babudieri, S.; Latte, G.; Madeddu, G.; Galleri, G.; Nuvoli, S.; Bagella, P.; Demartis, M.I.; Fiore, V.; et al. Enzyme biosensors for biomedical applications: Strategies for safeguarding analytical performances in biological fluids. Sensors 2016, 16, 780. [Google Scholar] [CrossRef] [PubMed]
- Thiha, A.; Ibrahim, F. A colorimetric Enzyme-Linked Immunosorbent Assay (ELISA) detection platform for a point-of-care dengue detection system on a lab-on-compact-disc. Sensors 2015, 15, 11431–11441. [Google Scholar] [CrossRef] [PubMed]
- Milne, S.D.; Connolly, P.; al Hamad, H.; Seoudi, I. Development of wearable sensors for tailored patient wound care. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS), Chicago, IL, USA, 26–30 August 2014; pp. 618–621. [Google Scholar]
- Sharp, D.; Forsythe, S.; Davis, J. Carbon Fibre Composites: Integrated Electrochemical Sensors for Wound Management. J. Biochem. 2007, 44, 1–22. [Google Scholar] [CrossRef] [PubMed]
- RoyChoudhury, S.; Umasankar, Y.; Bhansali, S. A wearable electrochemical sensor to monitor progression of wound healing. ECS Trans. 2017, 80, 1345–1353. [Google Scholar] [CrossRef]
- Staneva, D.; Betcheva, R.; Chovelon, J.M. Fluorescent benzo[de]anthracen-7-one pH-sensor in aqueous solution and immobilized on viscose fabrics. J. Photochem. Photobiol. A Chem. 2006, 183, 159–164. [Google Scholar] [CrossRef]
- McLister, A.; Davis, J. Molecular wiring in smart dressings: Opening a new route to monitoring wound pH. Healthcare 2015, 3, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, V.; Takahata, K. A hydrogel-based passive wireless sensor using a flex-circuit inductive transducer. Sens. Actuators A Phys. 2009, 155, 58–65. [Google Scholar] [CrossRef]
- Whelan, J. Smart bandages diagnose wound infection. Drug Discov. Today 2002, 7, 9–10. [Google Scholar] [CrossRef]
- DeLouise, L.A. Smart bandage—A hydrogel supported optical microcavity sensor. NSTI Nanotechnol. Conf. Trade Show 2005, 1, 51–54. [Google Scholar]
- Thet, N.T.; Alves, D.R.; Bean, J.E.; Booth, S.; Nzakizwanayo, J.; Young, A.E.R.; Jones, B.V.; Jenkins, A.T.A. Prototype development of the intelligent hydrogel wound dressing and its efficacy in the detection of model pathogenic wound biofilms. ACS Appl. Mater. Interfaces 2016, 8, 14909–14919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, S.; Cheng, R.; Wang, X.; Xue, T.; Liu, Y.; Nel, A.; Huang, Y.; Duan, X. Real-time electrical detection of nitric oxide in biological systems with sub-nanomolar sensitivity. Nat. Commun. 2013, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mostafalu, P.; Lenk, W.; Dokmeci, M.R.; Ziaie, B.; Khademhosseini, A.; Sonkusale, S.R. Wireless flexible smart bandage for continuous monitoring of wound oxygenation. IEEE Trans. Biomed. Circuits Syst. 2015, 9, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Farrow, M.J.; Hunter, I.S.; Connolly, P. Developing a real time sensing system to monitor bacteria in wound dressings. Biosensors 2012, 2, 171–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Wang, S.; Keum, H.; Ghaffari, R.; Kim, Y.S.; Tao, H.; Panilaitis, B.; Li, M.; Kang, Z.; Omenetto, F.; et al. Thin, flexible sensors and actuators as ‘instrumented’ surgical sutures for targeted wound monitoring and therapy. Small 2012, 8, 3263–3268. [Google Scholar] [CrossRef] [PubMed]
- Matzeu, G.; Losacco, M.; Parducci, E.; Pucci, A.; Dini, V.; Romanelli, M.; Di Francesco, F. Skin temperature monitoring by a wireless sensor. In Proceedings of the IECON 2011 37th Annual Conference of the IEEE Industrial Electronics Society, Melbourne, Australia, 7–10 November 2011; pp. 3533–3535. [Google Scholar]
- Mehmood, N.; Hariz, A.; Templeton, S.; Voelcker, N.H. A flexible and low power telemetric sensing and monitoring system for chronic wound diagnostics. Biomed. Eng. Online 2015, 14, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Farooqui, M.F.; Shamim, A. Low cost inkjet Printed smart bandage for wireless monitoring of chronic wounds. Sci. Rep. 2016, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Swisher, S.L.; Lin, M.C.; Liao, A.; Leeflang, E.J.; Khan, Y.; Pavinatto, F.J.; Mann, K.; Naujokas, A.; Young, D.; Roy, S.; et al. Impedance sensing device enables early detection of pressure ulcers in vivo. Nat. Commun. 2015, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ostadabbas, S.; Saeed, A.; Nourani, M.; Pompeo, M. Sensor architectural tradeoff for diabetic foot ulcer monitoring. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS), San Diego, CA, USA, 28 August–1 September 2012; pp. 6687–6690. [Google Scholar]
- Knapton, S. Smart bandages which tell doctor how wound is healing to begin trials. The Telegraph, 16 April 2017. [Google Scholar]
- Corbucci, G.G.; Lettieri, B.; Damonti, V.; Palombari, R.; Arienti, G.; Palmerini, C.A. Nitric oxide in ischemic and reperfused human muscle. Clin. Chim. Acta 2002, 318, 79–82. [Google Scholar] [CrossRef]
- Schreml, S.; Meier, R.J.; Weiß, K.T.; Cattani, J.; Flittner, D.; Gehmert, S.; Wolfbeis, O.S.; Landthaler, M.; Babilas, P. A sprayable luminescent pH sensor and its use for wound imaging in vivo. Exp. Dermatol. 2012, 21, 951–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, A.; Lin, M.C.; Ritz, L.C.; Swisher, S.L.; Ni, D.; Mann, K.; Khan, Y.; Roy, S.; Harrison, M.R.; Arias, A.C.; et al. Impedance sensing device for monitoring ulcer healing in human patients. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS), Milan, Italy, 25–29 August 2015; pp. 5130–5133. [Google Scholar]
- Milne, S.D.; Seoudi, I.; Al Hamad, H.; Talal, T.K.; Anoop, A.A.; Allahverdi, N.; Zakaria, Z.; Menzies, R.; Connolly, P. A wearable wound moisture sensor as an indicator for wound dressing change: An observational study of wound moisture and status. Int. Wound J. 2016, 13, 1309–1314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kekonen, A.; Eriksson, J.-E.; Bergelin, M.; Ylänen, H.; Viik, J. A quantitative method for monitoring wound healing. Int. J. Bioelectromagn. 2015, 17, 36–41. [Google Scholar]
- Hattori, Y.; Falgout, L.; Lee, W.; Jung, S.Y.; Poon, E.; Lee, J.W.; Na, I.; Geisler, A.; Sadhwani, D.; Zhang, Y.; et al. Multifunctional skin-like electronics for quantitative, clinical monitoring of cutaneous wound healing. Adv. Healthc. Mater. 2014, 3, 1597–1607. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wagner-Meggitt | University of Texas | PEDIS | |
|---|---|---|---|
| Grade 0 | Pain only, no open ulcer | Pre-ulceration | |
| Grade 1 | Superficial ulcer | Superficial wound | Skin intact, no infection or loss of sensation |
| Grade 2 | Deep ulcer | Wound penetrating to tendon or capsule | Superficial ulcer with infection at the surface and loss of sensation |
| Grade 3 | Deep ulceration with osteomyelitis | Wound penetrating to bone or joint | Ulcer reaching the fascia, muscle, and tendon, fasciitis and septic arthritis likely |
| Grade 4 | Localized Gangrene | Ulcer depth reaching the bone or joint, SIRS | |
| Grade 5 | Extensive Gangrene, Amputation likely | ||
| References | [13,16,17] | [18] | [19] |
| Polymer | Advantages | Disadvantages | Reference |
|---|---|---|---|
| Cellulose | 1. Readily available with low cost 2. Fiber and foam materials 3. Creates a gel-like material, forming a moist environment 4. Releases GFs to stimulate fibroblast proliferation | 1. Requires additional antimicrobial substances 2. Resorption in tissues does not occur, which could cause further tissue damage or become overwhelmed by excess exudate | [36] |
| Chitosan | 1. Fabricated in a gelatin of film-like material 2. Antimicrobial and hemostatic properties 3. Functional derivatives allowing for modified and versatile effects 4. Ability to deliver drugs | 1. Extensive swelling in water 2. Unable to dissolve in organic solvents because of its rigid crystalline structure | [38,43,44,45,70,71] |
| Collagen and Gelatin | 1. Promotes tissue granulation and angiogenesis 2. Inhibits bacterial growth and prolonged inflammatory response 3. Gelatin derivative forming a hydrogel material | 1. May not be absorptive in gelatin form, especially for wounds with excessive exudate 2. Might require secondary dressing | [22,38,46,48] |
| Hyaluronic Acid | 1. Lubricative and water absorptive 2. Bi-products promote epithelial cell migration 3. Improves collagen deposition and angiogenesis4. Popular drug delivery system and vehicle for growth factors | 1. Only MMWHA enhances wound repair | [52,72,73,74] |
| Poly(lactide-co-glycolide) | 1. FDA approved for drug delivery, suture applications 2. Ratio of lactide to glycolide units can modify release of drugs and growth factors 3. Cytocompatible and stimulates fibroblast adhesion, spreading, and proliferation 4. Fabricated into various shapes | 1. Requires additional antimicrobial substances 2. Properties fail to match ECM or collagen | [38,56,57,58,59] |
| Polyurethanes | 1. Semipermeable membrane that prevents bacteria from entering 2. Provides a moist environment 3. Delivers bioactive substances for fighting infection 4. Drainage properties that decrease the risk of swelling | 1. Need composite dressings in order to provide contact layer and waterproof properties 2. Wound healing effects are only associated with nanofiber structure | [57,61,62] |
| Poly(ethylene glycol) | 1. Hydrophilic, flexible and compatible qualities 2. Surface modifier allowing for better grip in the contact layer 3. Growth factors have higher affinity for PEG | 1. Adhesiveness might damage granulation tissue 2. Does not incorporate antibiotics and other drugs so composite materials are needed | [38,57,64] |
| Polycaprolactone | 1. FDA approved for suture applications 2. Fibrous structure similar to ECM architecture 3. Water retention capacities used to capture wound exudate 4. Resistant to many solvents allowing for slow and controlled degradation | 1. Lack of antimicrobial properties | [67,68,69] |
| Biochemical Biomarkers | ||
| Wound Biomarker | Significance in Chronic Wounds vs. Acute Wounds | Reference |
| Cytokines (IL-1, IL-6, TNF-α) | Elevated levels of Cytokine | [11,90] |
| Nitric Oxide | Decreased levels of NO | [89,93] |
| Matrix Metalloproteinase | Increased protease activity | [11,91] |
| Oxygen | Higher probability for ischemia due to decreased oxygen levels | [9] |
| Bacteria | Bacteria concentration levels are higher indicating extent of infection. | [9,92] |
| Wound pH | Remains more alkalotic for extended period of time | [86] |
| Uric Acid | Decreased levels due to bacteria | [94] |
| Reactive Oxygen Species | Increased levels due to oxidative stress | [11] |
| Gene Expression | Increase in bacterial housekeeping genes; decrease in ulcer housekeeping genes. | [11] |
| Growth Factors | Decreased level (i.e., PDGF) | [11] |
| Physical Biomarkers | ||
| Wound Biomarker | Significance in Chronic Wounds vs. Acute Wounds | Reference |
| Bioelectrical Impedance | Phase angle, resistance, and reactance are all decreased | [87] |
| Pressure | Increased pressure | [95] |
| Temperature | Increased temperature | [96] |
| Sensor | Sensitivity/Range | Biomarker | Method | Reference |
|---|---|---|---|---|
| ELISA MMP Sensor | 0.1–100 mg/mL | MMP-9 | Electrochemical | [99] |
| Disposable MMP-9 Sensor | 200 mg/mL | MMP-9 | Electrochemical Impedance Spectroscopy | [90] |
| Smart Bandage UA Sensor | 100 µM of UA | Uric Acid | Electrochemical | [94] |
| Carbon fiber sensor | 0–500 µM | Uric Acid | Electrochemical | [100] |
| Wearable enzymatic sensor | 0.14 µ/M-cm2 Range: 14 µM | Uric Acid | Electrochemical | [101] |
| Poly-tryptophan Carbon Fiber pH Sensor | pH of 3–8 (±0.1) | pH | Voltammetry | [103] |
| Flexible Hydrogel pH sensor | pH of 5–8 (±0.2) | pH | Fluorescent Spectroscopy/Image processing | [79] |
| Hydrogel pH sensor | pH of 1–8 | pH | Electrical (LC circuit) and Chemical | [104] |
| Smart Bandage | Gram-Negative Bacteria, shift in wavelength by 3–4 nm | Gram-negative,-positive, E. coli, Lipid A | Electrochemical/Optical Microcavity | [105,106] |
| Intelligent Hydrogel Dressing | Contrast of approximately 20,000 and 35,000 fluorescence/a.u. of S. aureus and P aeruginosa, respectively compared to HEPES | Bacteria (S. aureus, P. aeruginosa, E. coli, E. faecalis) | Electrochemical/Fluorescent Spectroscopy | [107] |
| Hemin-Functionalized FET NO Sensor | 0.3 nm of NO | Nitric Oxide | Bio-electrical | [108] |
| Oxygen Bandage Sensor | 0.4–0.6 mA | Oxygen | Bio-electrical | [109] |
| Screen Printed Impedance Sensor | 5 × 107 CFU/mL of S. aureus | S. aureus | Electrical | [110] |
| Flexible Pt thermistor | 2.7 Ω/°C | Temperature | Electrical | [111] |
| Wireless thermistor | 17 Ω/°C at 35 °C | Temperature | Electrical | [112] |
| Flexible Low Power Sensor | 0.2 °C temperature difference, 0.5 mmHg pressure, 3.0% RH | Moisture, Temperature, Pressure | Electrical | [113] |
| Inkjet Printed Smart Bandage | ±2.3% capacitance, 8% quality factor, ±2.6% resistance | Blood, pH, Resistance | Electrical (Capacitance and Resistance) | [114] |
| Flexible Sensor Array | 100–50 KΩ at 100–1 MHz | Impedance | Electrical | [115] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gianino, E.; Miller, C.; Gilmore, J. Smart Wound Dressings for Diabetic Chronic Wounds. Bioengineering 2018, 5, 51. https://doi.org/10.3390/bioengineering5030051
Gianino E, Miller C, Gilmore J. Smart Wound Dressings for Diabetic Chronic Wounds. Bioengineering. 2018; 5(3):51. https://doi.org/10.3390/bioengineering5030051
Chicago/Turabian StyleGianino, Elizabeth, Craig Miller, and Jordon Gilmore. 2018. "Smart Wound Dressings for Diabetic Chronic Wounds" Bioengineering 5, no. 3: 51. https://doi.org/10.3390/bioengineering5030051
APA StyleGianino, E., Miller, C., & Gilmore, J. (2018). Smart Wound Dressings for Diabetic Chronic Wounds. Bioengineering, 5(3), 51. https://doi.org/10.3390/bioengineering5030051