
Encoder-Controlled Functional Electrical Stimulator for Bilateral Wrist Activities—Design and Evaluation


Abstract
:
1. Introduction
2. Materials
2.1. Electrical Stimulator
2.2. Encoder Circuit
2.3. Pedestal-Mounted Encoder Circuit
2.4. Device Firmware
2.5. FES-Encoder Software
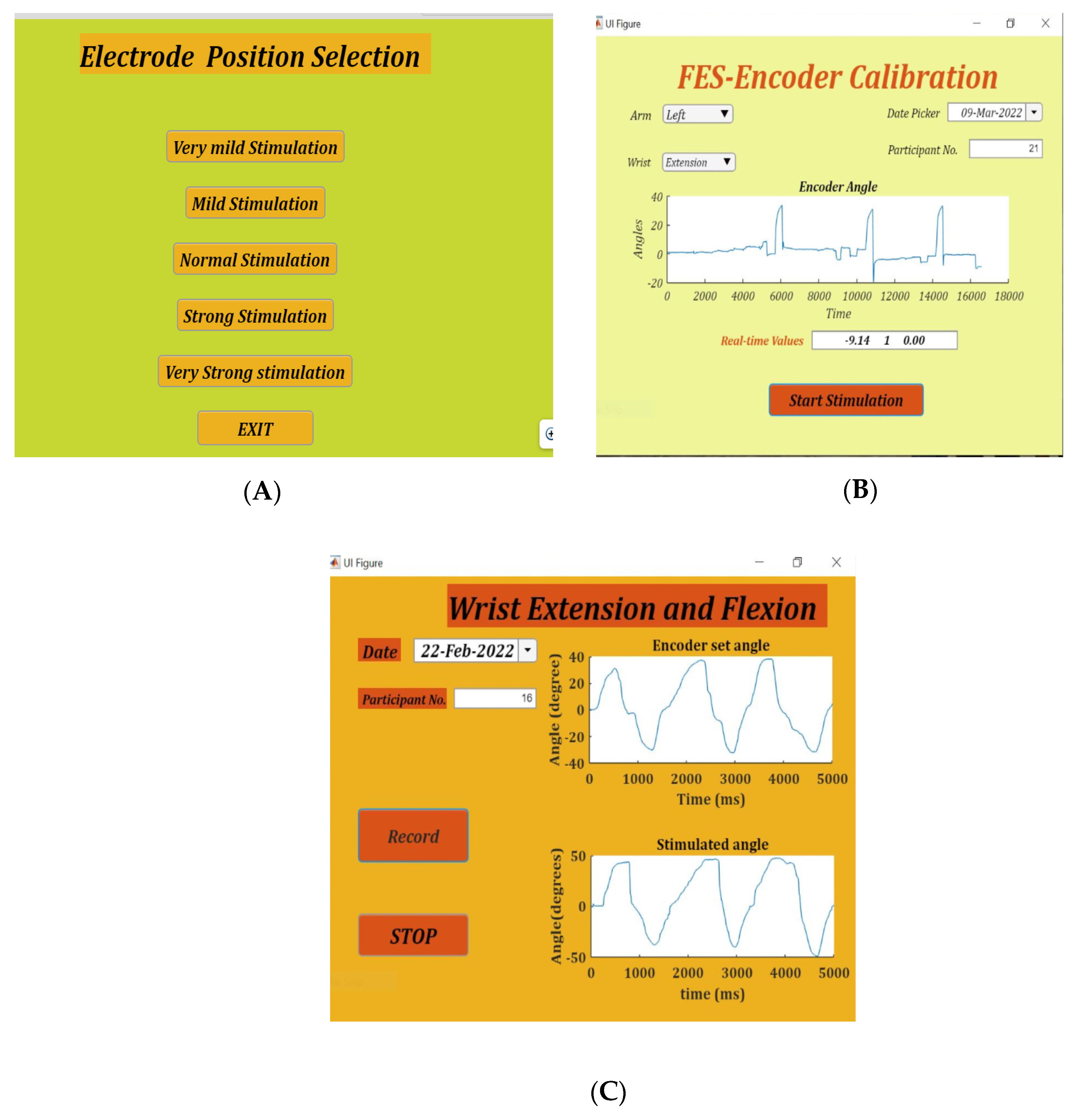
2.6. Placement Selection App
2.7. FES-Encoder Calibration App
2.8. Set/Stimulate and Record Angles App
3. Method
3.1. Participants
3.2. Placement Selection
3.3. FES-Encoder Calibration
3.4. Set/Stimulate and Record Angles
4. Results
4.1. Placement Selection
4.2. FES-Encoder Calibration
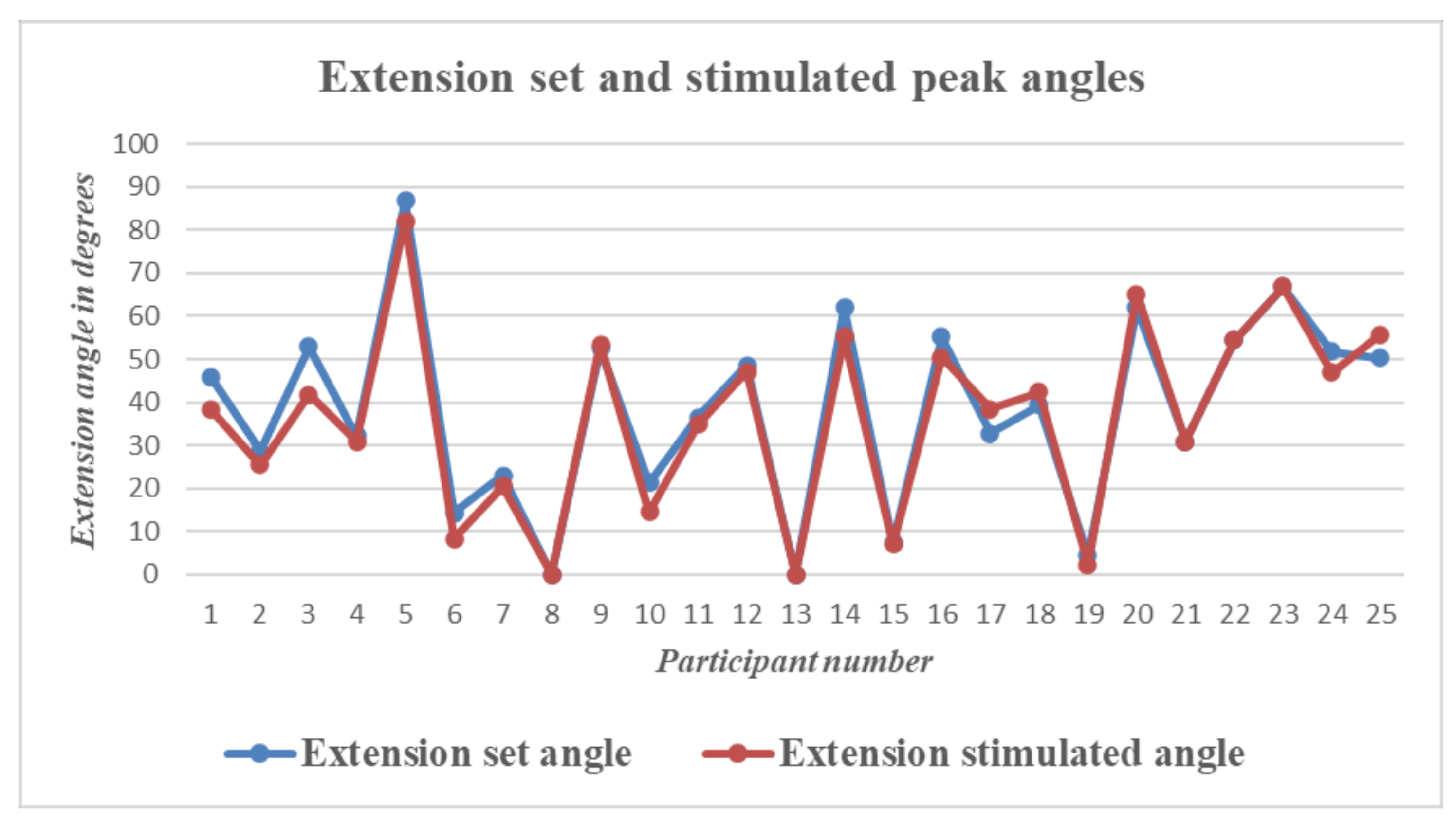
4.3. Set/Stimulate and Record
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Lancet: Latest Global Disease Estimates Reveal Perfect Storm of Rising Chronic Diseases and Public Health Failures Fuelling COVID-19 Pandemic|Institute for Health Metrics and Evaluation. Available online: https://www.healthdata.org/news-release/lancet-latest-global-disease-estimates-reveal-perfect-storm-rising-chronic-diseases-and (accessed on 5 April 2022).
- Waller, S.M.; Whitall, J. Bilateral arm training: Why and who benefits? NeuroRehabilitation 2008, 23, 29–41. [Google Scholar] [CrossRef]
- Sethy, D.; Sahoo, S.; Kujur, E.S.; Bajpai, P. Stroke upper extremity rehabilitation: Effect of bilateral arm training. Int. J. Health Allied Sci. 2018, 7, 217. [Google Scholar]
- Chen, P.M.; Kwong, P.W.H.; Lai, C.K.Y.; Ng, S.S.M. Comparison of bilateral and unilateral upper limb training in people with stroke: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0216357. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Lee, J.H.; Koo, H.M.; Lee, S.M. Effectiveness of Bilateral Arm Training for Improving Extremity Function and Activities of Daily Living Performance in Hemiplegic Patients. J. Stroke Cerebrovasc. Dis. 2017, 26, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Sainburg, R.L.; Good, D.; Przybyla, A. Bilateral Synergy: A Framework for Post-Stroke Rehabilitation. J. Neurol. Transl. Neurosci. 2013, 1, 1025. [Google Scholar] [PubMed]
- Swinnen, S.P. Intermanual coordination: From behavioural principles to neural-network interactions. Nat. Rev. Neurosci. 2002, 3, 348–359. [Google Scholar] [CrossRef]
- Cohen, L. Synchronous bimanual movements performed by homologous and non-homologous muscles. Percept. Mot. Skills 1971, 32, 639–644. [Google Scholar] [CrossRef]
- Kelso, S.J.; Southard, D.L.; Goodman, D. On the Nature of Human Interlimb Coordination. Science 1979, 203, 1029–1031. [Google Scholar] [CrossRef]
- Stoykov, M.E.; Corcos, D.M. A review of bilateral training for upper extremity hemiparesis. Occup. Ther. Int. 2009, 16, 190–203. [Google Scholar] [CrossRef]
- van Delden, A.E.Q.; Peper, C.E.; Kwakkel, G.; Beek, P.J. A Systematic Review of Bilateral Upper Limb Training Devices for Poststroke Rehabilitation. Stroke Res. Treat. 2012, 2012, 17. [Google Scholar] [CrossRef]
- Brackenridge, J.; Bradnam, L.V.; Lennon, S.; Costi, J.J.; Hobbs, D.A. A Review of Rehabilitation Devices to Promote Upper Limb Function...: Ingenta Connect. Neurosci. Biomed. Eng. 2016, 4, 25–42. [Google Scholar] [CrossRef]
- Nudo, R.J. Recovery after brain injury: Mechanisms and principles. Front. Hum. Neurosci. 2013, 7, 887. [Google Scholar] [CrossRef] [PubMed]
- Kimberley, T.J.; Samargia, S.; Moore, L.G.; Shakya, J.K.; Lang, C.E. Comparison of amounts and types of practice during rehabilitation for traumatic brain injury and stroke. J. Rehabil. Res. Dev. 2010, 47, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.S.P.; Moreira, J.; Silva, C.; Mesquita, I.; Macedo, R.; Silva, A.; Santos, R. Usability of Functional Electrical Stimulation in Upper Limb Rehabilitation in Post-Stroke Patients: A Narrative Review. Sensors (Basel) 2022, 22, 1409. [Google Scholar] [CrossRef] [PubMed]
- Chae, J.; Bethoux, F.; Bohinc, T.; Dobos, L.; Davis, T.; Friedl, A. Neuromuscular stimulation for upper extremity motor and functional recovery in acute hemiplegia. Stroke 1998, 29, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Kimberley, T.J.; Lewis, S.M.; Auerbach, E.J.; Dorsey, L.L.; Lojovich, J.M.; Carey, J.R. Electrical stimulation driving functional improvements and cortical changes in subjects with stroke. Exp. Brain Res. 2004, 154, 450–460. [Google Scholar] [CrossRef]
- Powell, J.; Pandyan, A.D.; Granat, M.; Cameron, M.; Stott, D.J. Electrical stimulation of wrist extensors in poststroke hemiplegia. Stroke 1999, 30, 1384–1389. [Google Scholar] [CrossRef]
- Sharififar, S.; Shuster, J.J.; Bishop, M.D. Adding electrical stimulation during standard rehabilitation after stroke to improve motor function. A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2018, 61, 339–344. [Google Scholar] [CrossRef]
- Wu, F.C.; Lin, Y.T.; Kuo, T.S.; Luh, J.J.; Lai, J.S. Clinical effects of combined bilateral arm training with functional electrical stimulation in patients with stroke. IEEE Int. Conf. Rehabil. Robot. 2011, 2011, 5975367. [Google Scholar]
- Cauraugh, J.H.; Kim, S.B.; Duley, A. Coupled bilateral movements and active neuromuscular stimulation: Intralimb transfer evidence during bimanual aiming. Neurosci. Lett. 2005, 382, 39–44. [Google Scholar]
- Knutson, J.S.; Hisel, T.Z.; Harley, M.Y.; Chae, J. A Novel Functional Electrical Stimulation Treatment for Recovery of Hand Function in Hemiplegia: 12-Week Pilot Study. Neurorehabil. Neural Repair 2009, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.; Idica, J.; Amitoj, B.; Cauraugh, J.H. Motor recovery patterns in arm muscles: Coupled bilateral training and neuromuscular stimulation. J. Neuroeng. Rehabil. 2014, 11, 57. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Yu, Z.; Mao, M. Contralaterally controlled functional electrical stimulation improves wrist dorsiflexion and upper limb function in patients with early-phase stroke: A randomized controlled trial. Ann. Phys. Rehabil. Med. 2018, 61, e36. [Google Scholar] [CrossRef]
- Chan, M.K.; Tong, R.K.; Chung, K.Y. Bilateral Upper Limb Training With Functional Electric Stimulation in Patients with Chronic Stroke. Neurorehabilit. Neural Repair 2009, 23, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, T.; Sakaino, S.; Tsuji, T. Bilateral control using functional electrical stimulation. In Proceedings of the IECON 2015-41st Annual Conference of the IEEE Industrial Electronics Society, Yokohama, Japan, 9–12 November 2015; pp. 2336–2341. [Google Scholar]
- Gandhi, D.B.C.; Sterba, A.; Khatter, H.; Pandian, J.D. Mirror Therapy in Stroke Rehabilitation: Current Perspectives. Ther. Clin. Risk Manag. 2020, 16, 75. [Google Scholar]
- Samuelkamaleshkumar, S.; Reethajanetsureka, S.; Pauljebaraj, P.; Benshamir, B.; Padankatti, S.M.; David, J.A. Mirror Therapy Enhances Motor Performance in the Paretic Upper Limb After Stroke: A Pilot Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2014, 95, 2000–2005. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Lee, S.; Kim, D.; Lee, K.; Kim, Y. Effects of mirror therapy combined with motor tasks on upper extremity function and activities daily living of stroke patients. J. Phys. Ther. Sci. 2016, 28, 1–5. [Google Scholar] [CrossRef]
- Kim, H.; Lee, G.; Song, C. Effect of Functional Electrical Stimulation with Mirror Therapy on Upper Extremity Motor Function in Poststroke Patients. J. Stroke Cerebrovasc. Dis. 2014, 23, 655–661. [Google Scholar] [CrossRef]
- Lin, K.; Huang, P.; Chen, Y.; Wu, C.; Huang, W. Combining Afferent Stimulation and Mirror Therapy for Rehabilitating Motor Function, Motor Control, Ambulation, and Daily Functions After Stroke. Neurorehabil. Neural Repair 2014, 28, 153–162. [Google Scholar] [CrossRef]
- Mathieson, S.; Parsons, J.; Kaplan, M. Combining functional electrical stimulation with mirror therapy for the upper limb in people with stroke. Crit. Rev. Phys. Rehabil. Med. 2014, 26, 113–129. [Google Scholar] [CrossRef]
- Gera, S.; Gangadharan, N.; Navin, B.P.; Tharion, G.; Chalagiri, P.H.; Thomas, R.; Devasahayam, S. Electrical Stimulation and assessment of the induced force in the Denervated Muscle. TENCON 2019 - 2019 IEEE Region 10 Conference (TENCON), Kochi, India, 17–20 October 2019; pp. 2046–2050. [Google Scholar] [CrossRef]
- Nehrujee, A.; Andrew, H.; Patricia, A.; Samuelkamaleshkumar, S.; Prakash, H.; Sujatha, S.; Balasubramanian, S. A Plug-and-Train Robot (PLUTO) for Hand Rehabilitation: Design and Preliminary Evaluation. IEEE Access 2021, 9, 134957–134971. [Google Scholar] [CrossRef]
- Mortimer, J.T.; Bhadra, N. Chapter 4.2 Peripheral Nerve and Muscle Stimulation. In Neuroprosthetics Theory and Practice; World Scientific: London, UK, 2004; pp. 638–682. [Google Scholar]
- Gobbo, M.; Maffiuletti, N.A.; Orizio, C.; Minetto, M.A. Muscle motor point identification is essential for optimizing neuromuscular electrical stimulation use. J. Neuroeng. Rehabil. 2014, 11, 17. [Google Scholar] [CrossRef] [PubMed]
- Lyons, G.M.; Leane, G.E.; Clarke-Moloney, M.; O’Brien, J.V.; Grace, P.A. An investigation of the effect of electrode size and electrode location on comfort during stimulation of the gastrocnemius muscle. Med. Eng. Phys. 2004, 26, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Flodin, J.; Juthberg, R.; Ackermann, P.W. Effects of electrode size and placement on comfort and efficiency during low-intensity neuromuscular electrical stimulation of quadriceps, hamstrings and gluteal muscles. BMC Sports Sci. Med. Rehabil. 2022, 14, 11. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, F.V.A.; Vieira, A.; Carregaro, R.L.; Bottaro, M.; Maffiuletti, N.A.; Durigan, J.L.Q. Skinfold thickness affects the isometric knee extension torque evoked byNeuromuscular Electrical Stimulation. Brazilian J. Phys. Ther. 2015, 19, 466. [Google Scholar] [CrossRef]
- Keller, T.; Kuhn, A. Skin properties and the influence on electrode design for transcutaneous (surface) electrical stimulation. IFMBE Proc. 2009, 25, 492–495. [Google Scholar]
- Petrofsky, J. The effect of the subcutaneous fat on the transfer of current through skin and into muscle. Med. Eng. Phys. 2008, 30, 1168–1176. [Google Scholar] [CrossRef]
- Solomons, C.D.; Shanmugasundaram, V. Forearm and wrist band for Functional Electrical Stimulation. In Proceedings of the 2019 Innovations in Power and Advanced Computing Technologies, Vellore, India, 22–23 March 2019. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Angle | Amplitude | Pulse Width |
|---|---|---|---|
| 1. | −0.7000 | 18 | 80 |
| 2. | −0.4300 | 18 | 100 |
| 3. | 1.9540 | 15 | 120 |
| 4. | 2.8925 | 20 | 80 |
| 5. | 3.0520 | 18 | 120 |
| 6. | 3.4545 | 15 | 80 |
| 7. | 4.3500 | 15 | 140 |
| 8. | 4.5335 | 24 | 80 |
| 9. | 4.9555 | 20 | 100 |
| 10. | 10.6625 | 15 | 170 |
| 11. | 11.7900 | 15 | 100 |
| 12. | 30.0085 | 18 | 140 |
| 13. | 30.0725 | 15 | 200 |
| 14. | 32.7865 | 24 | 100 |
| 15. | 35.9210 | 28 | 80 |
| 16. | 41.6605 | 20 | 120 |
| Flexion (Angle in Degrees) | Extension (Angle in Degrees) | Time (in MS) | ||||||
|---|---|---|---|---|---|---|---|---|
| Error | Error | Lag | ||||||
| Mean | 2.3668 | Mean | 1.908 | Mean | 1016.4 | |||
| Std. deviation | 5.38 | Std. deviation | 3.95 | Std. deviation | 492.09 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solomons, C.D.; Shanmugasundaram, V.; Balasubramanian, S. Encoder-Controlled Functional Electrical Stimulator for Bilateral Wrist Activities—Design and Evaluation. Bioengineering 2022, 9, 501. https://doi.org/10.3390/bioengineering9100501
Solomons CD, Shanmugasundaram V, Balasubramanian S. Encoder-Controlled Functional Electrical Stimulator for Bilateral Wrist Activities—Design and Evaluation. Bioengineering. 2022; 9(10):501. https://doi.org/10.3390/bioengineering9100501
Chicago/Turabian StyleSolomons, Cassandra D., Vivekanandan Shanmugasundaram, and Sivakumar Balasubramanian. 2022. "Encoder-Controlled Functional Electrical Stimulator for Bilateral Wrist Activities—Design and Evaluation" Bioengineering 9, no. 10: 501. https://doi.org/10.3390/bioengineering9100501
APA StyleSolomons, C. D., Shanmugasundaram, V., & Balasubramanian, S. (2022). Encoder-Controlled Functional Electrical Stimulator for Bilateral Wrist Activities—Design and Evaluation. Bioengineering, 9(10), 501. https://doi.org/10.3390/bioengineering9100501