
Effectiveness of Mechanical Horse-Riding Simulator-Based Interventions in Patients with Cerebral Palsy—A Systematic Review and Meta-Analysis

 ,
,  , and
, and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Register and Guidelines
2.2. Literature Search
2.3. Inclusion and Exclusion Criteria: Study Selection
2.4. Data Extraction
2.5. Variables
2.6. Quality Assessment
2.7. Statistical Analysis
2.8. Additional Analyses
3. Results
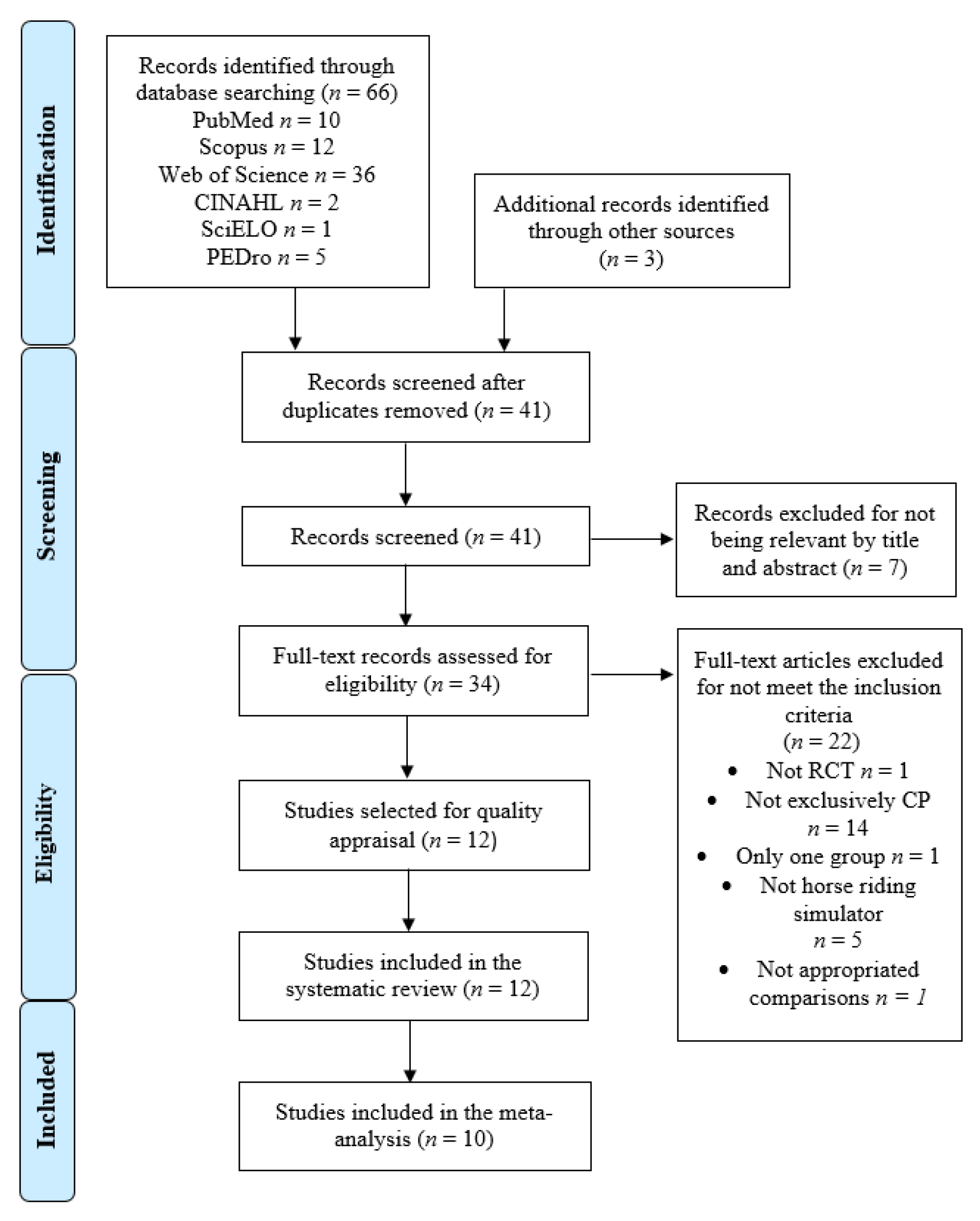
3.1. Study Selection
3.2. Characteristics of the Studies Included in the Review
3.3. Risk of Bias Assessment
3.4. Variables, Measurements and Synthesis
3.5. Quantitative Synthesis
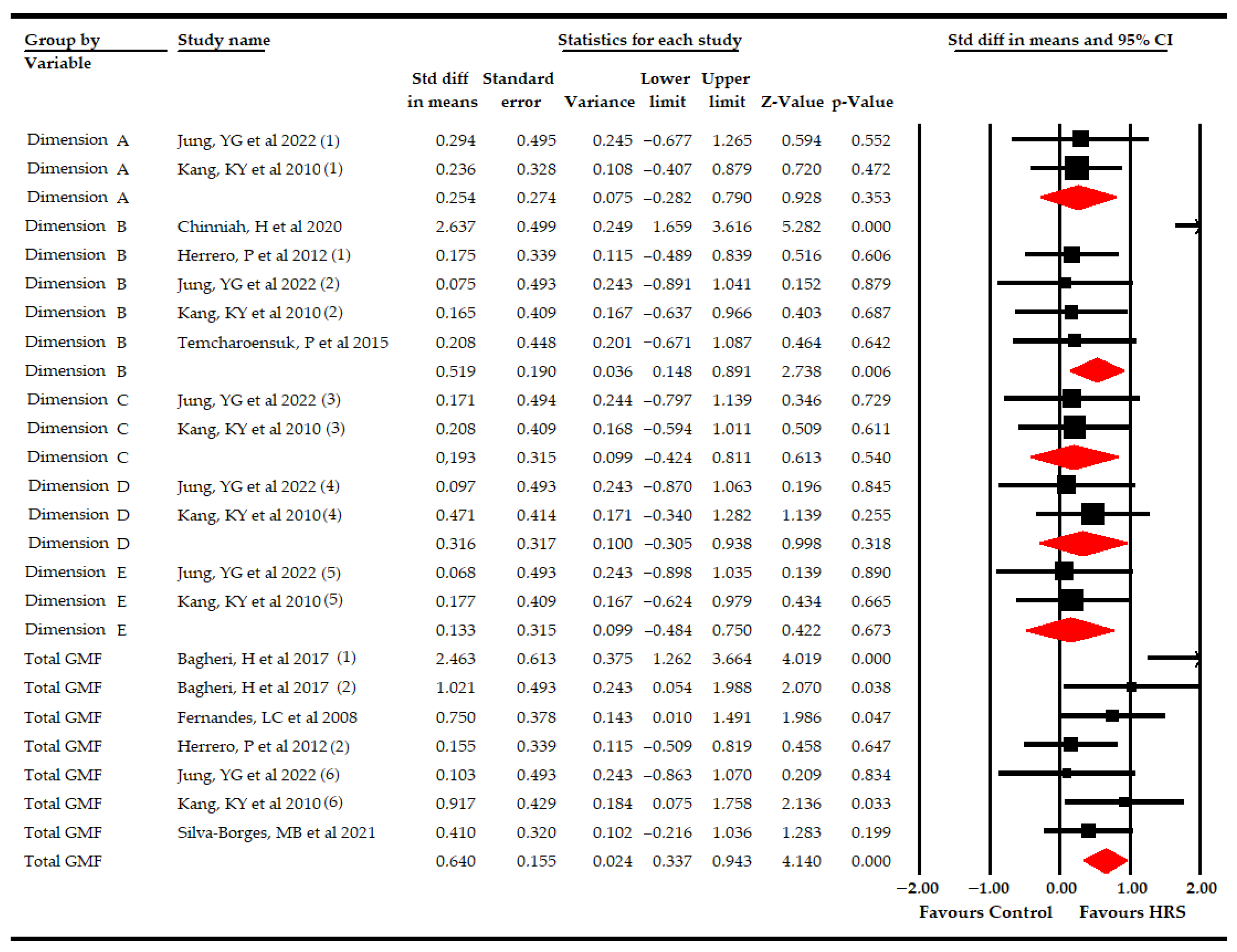
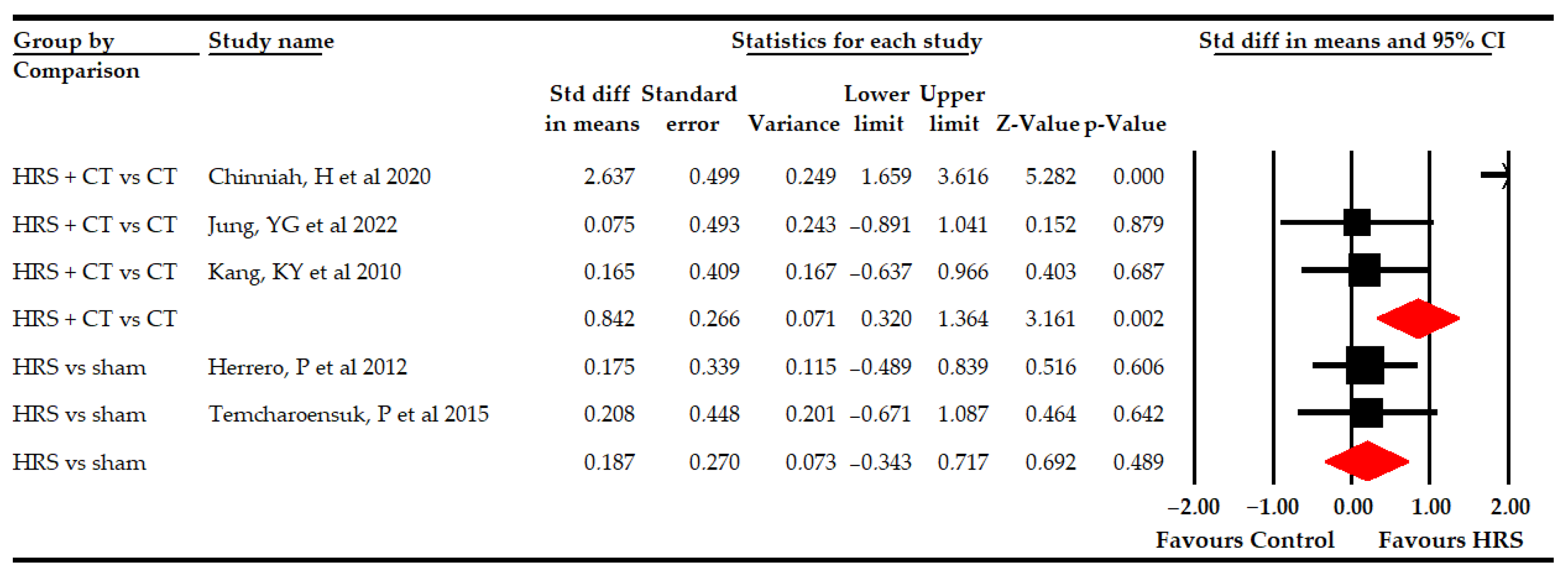
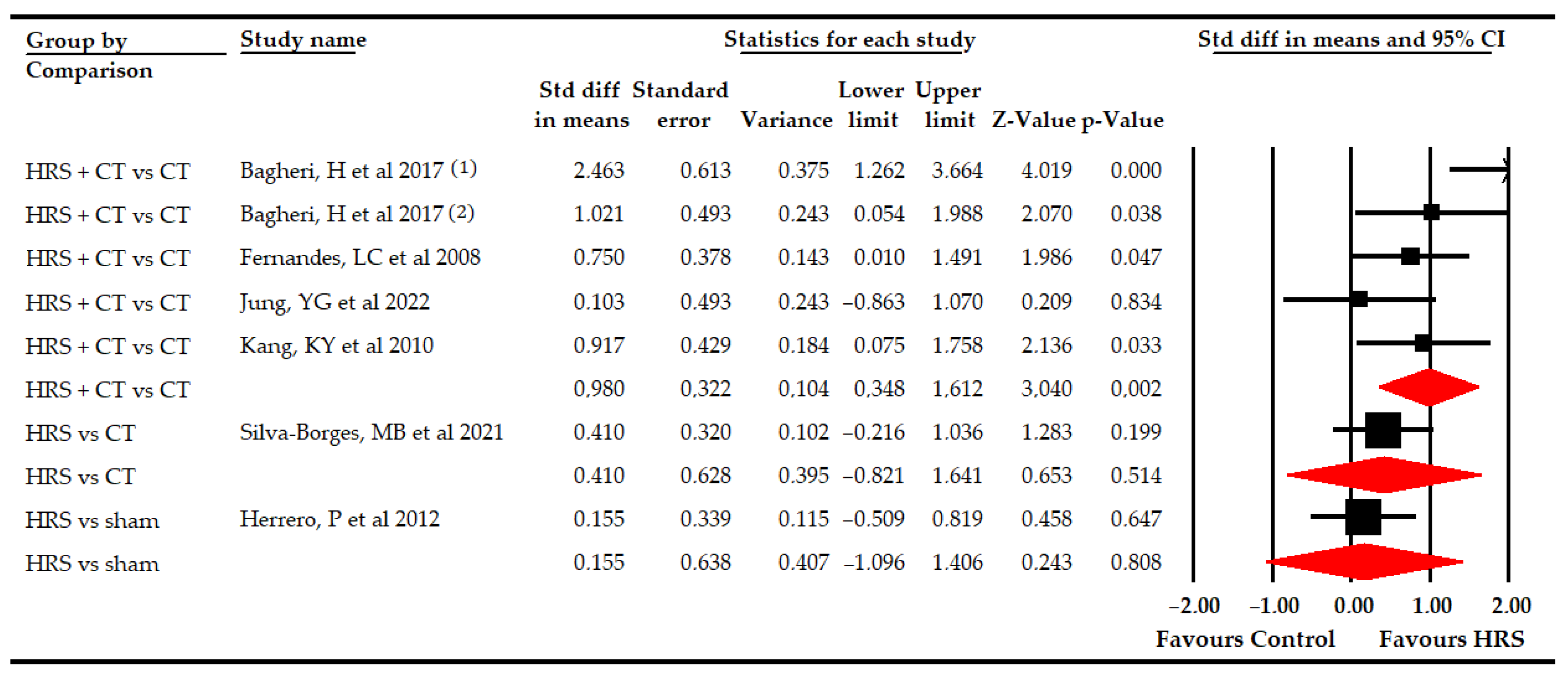
3.5.1. Gross Motor Function
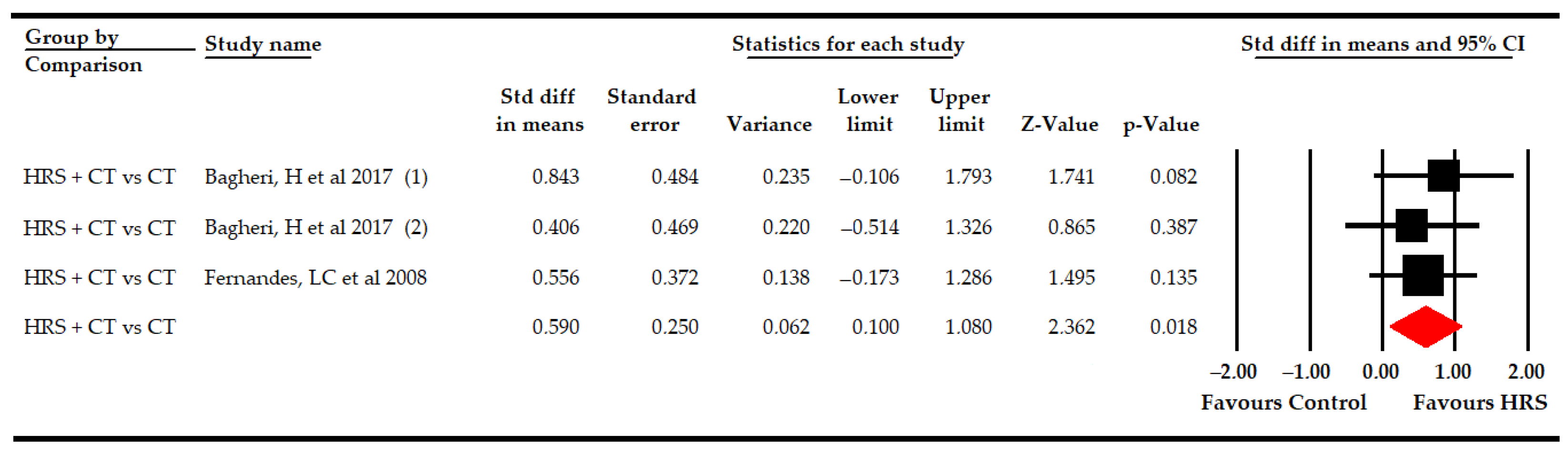
3.5.2. Functional Balance
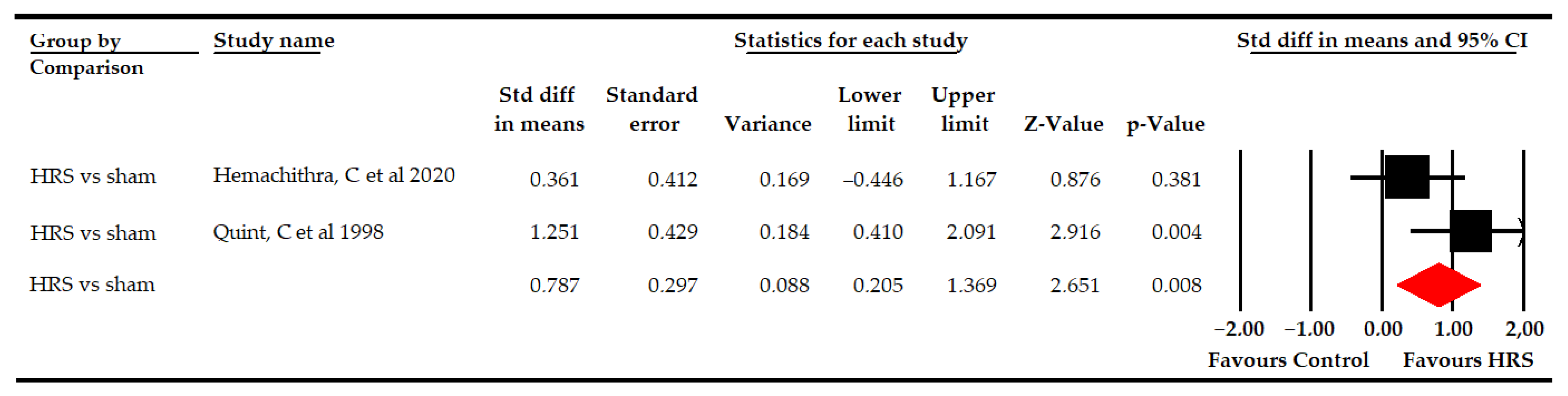
3.5.3. Abduction Pelvic Range of Motion
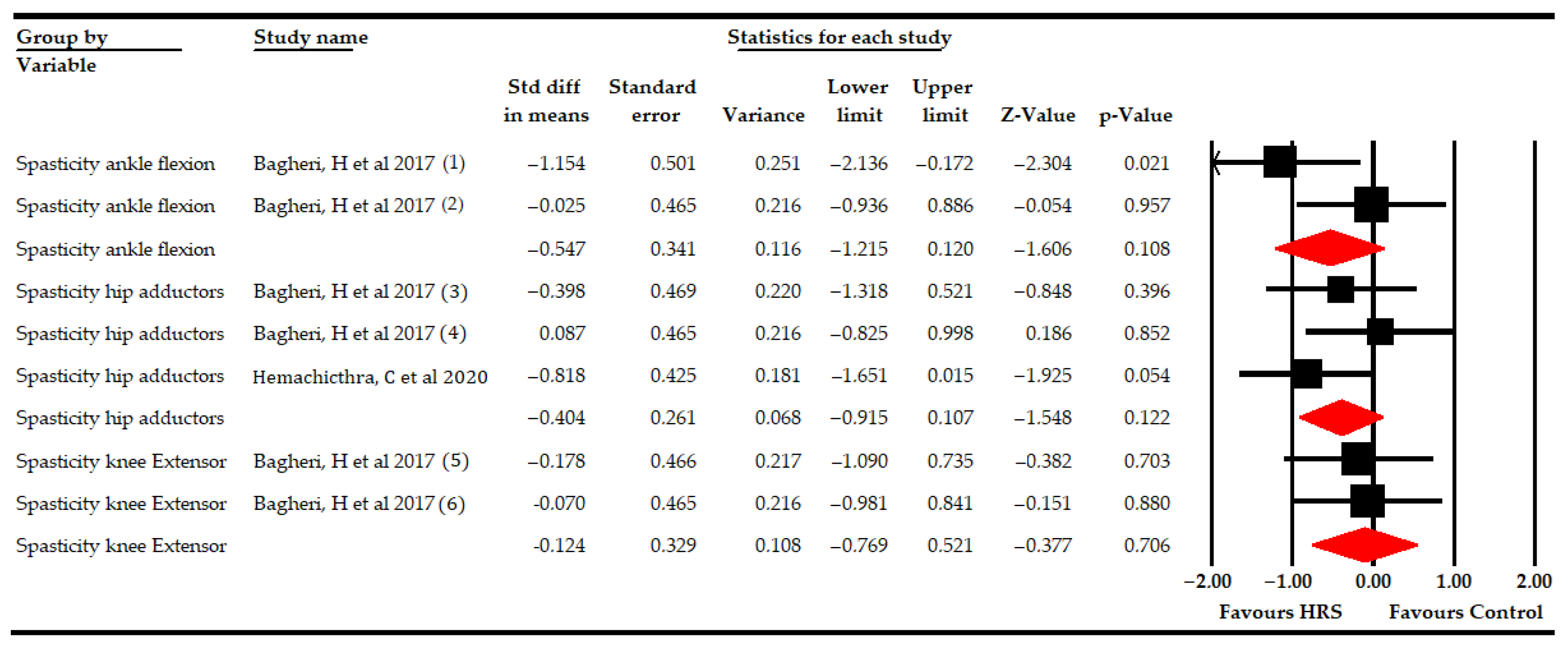
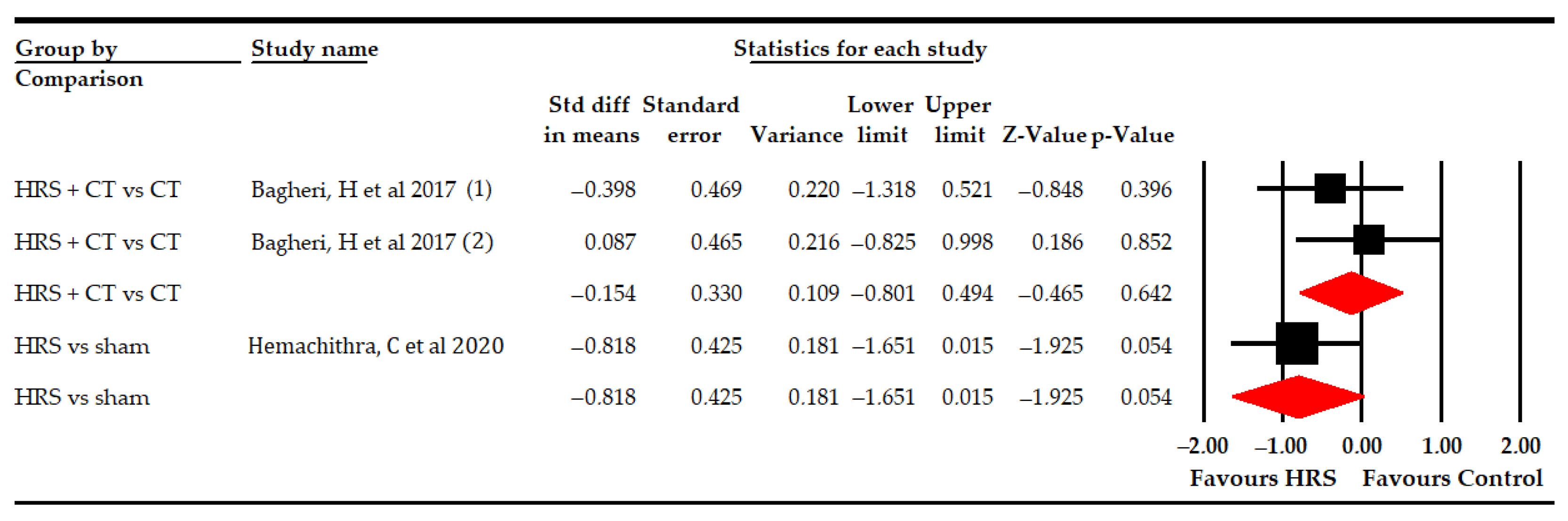
3.5.4. Spasticity
3.6. Qualitative Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HRS | Mechanical Horse-Riding Simulator |
| CP | Cerebral Palsy |
| PEDro | Physiotherapy Evidence Database |
| ROM | Range of Motion |
| SMD | Standardized Mean Difference |
| 95% CI | 95% Confidence Interval |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| AMSTAR | A Measurement Tool to Assess Systematic Reviews |
| WOS | Web of Science |
| GRADE | Grading of Recommendations Assessment, Development and Evaluation |
| MD | Mean Difference |
| MCID | Minimally Clinically Important Difference |
| I2 | Degree of Inconsistency |
| PT | Physiotherapy |
| GMFM | Gross Motor Function Measure |
| GMFCS | Gross Motor Function Classification System |
| PBS | Pediatric Balance Scale |
| MMAS | Modified Modified Ashworth Scale |
| MAS | Modified Ashworth Scale |
| AUQEI | Autoquestionnaire Qualité de Vie Enfant Image |
References
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.-P.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral palsy. Nat. Rev. Dis. Prim. 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, S.; Goldsmith, S.; Webb, A.; Ehlinger, V.; Hollung, S.J.; McConnell, K.; Arnaud, C.; Smithers-Sheedy, H.; Oskoui, M.; Khandaker, G.; et al. Global prevalence of cerebral palsy: A systematic analysis. Dev. Med. Child Neurol. 2022, 64, 1494–1506. [Google Scholar] [CrossRef] [PubMed]
- Oskoui, M.; Coutinho, F.; Dykeman, J.; Jetté, N.; Pringsheim, T. An update on the prevalence of cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2013, 55, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.J. Definition and classification of cerebral palsy. Dev. Med. Child Neurol. 2007, 47, 508. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. 2007, 49, 8–14. [Google Scholar]
- Zadnikar, M.; Kastrin, A. Effects of hippotherapy and therapeutic horseback riding on postural control or balance in children with cerebral palsy: A meta-analysis. Dev. Med. Child Neurol. 2011, 53, 684–691. [Google Scholar] [CrossRef]
- Burton, H.; Dixit, S.; Litkowski, P.; Wingert, J.R. Functional connectivity for somatosensory and motor cortex in spastic diplegia. Somatosens. Mot. Res. 2009, 26, 90–104. [Google Scholar] [CrossRef]
- Russo, R.N.; Skuza, P.P.; Sandelance, M.; Flett, P. Upper limb impairments, process skills, and outcome in children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2019, 61, 1080–1086. [Google Scholar] [CrossRef]
- Findlay, B.; Switzer, L.; Narayanan, U.; Chen, S.; Fehlings, D. Investigating the impact of pain, age, Gross Motor Function Classification System, and sex on health-related quality of life in children with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 292–297. [Google Scholar] [CrossRef]
- Viruega, H.; Gaillard, I.; Carr, J.; Greenwood, B.; Gaviria, M. Short- and Mid-Term Improvement of Postural Balance after a Neurorehabilitation Program via Hippotherapy in Patients with Sensorimotor Impairment after Cerebral Palsy: A Preliminary Kinetic Approach. Brain Sci. 2019, 9, 261. [Google Scholar] [CrossRef]
- Yun, G.; Huang, M.; Cao, J.; Hu, X. Selective motor control correlates with gross motor ability, functional balance and gait performance in ambulant children with bilateral spastic cerebral palsy. Gait Posture 2023, 99, 9–13. [Google Scholar] [CrossRef]
- Hunt, M.; Everaert, L.; Brown, M.; Muraru, L.; Hatzidimitriadou, E.; Desloovere, K. Effectiveness of robotic exoskeletons for improving gait in children with cerebral palsy: A systematic review. Gait Posture 2022, 98, 343–354. [Google Scholar] [CrossRef]
- Llamas-Ramos, R.; Sánchez-González, J.L.; Llamas-Ramos, I. Robotic Systems for the Physiotherapy Treatment of Children with Cerebral Palsy: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5116. [Google Scholar] [CrossRef]
- Inamdar, K.; Molinini, R.M.; Panibatla, S.T.; Chow, J.C.; Dusing, S.C. Physical therapy interventions to improve sitting ability in children with or at-risk for cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2021, 63, 396–406. [Google Scholar] [CrossRef]
- Jones, M.W.; Morgan, E.; Shelton, J.E.; Thorogood, C. Cerebral Palsy: Introduction and Diagnosis (Part I). J. Pediatr. Health Care 2007, 21, 146–152. [Google Scholar] [CrossRef]
- Ploypetch, T.; Buasuk, C.; Pajareya, K. Participation restriction of children with cerebral palsy living in Thailand and influential factors: A cross-sectional study. Dev. Neurorehabil. 2022, 25, 392–399. [Google Scholar] [CrossRef]
- Wu, M.; Kim, J.; Gaebler-Spira, D.J.; Schmit, B.D.; Arora, P. Robotic Resistance Treadmill Training Improves Locomotor Function in Children With Cerebral Palsy: A Randomized Controlled Pilot Study. Arch. Phys. Med. Rehabil. 2017, 98, 2126–2133. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.C.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef]
- Yana, M.; Tutuola, F.; Westwater-Wood, S.; Kavlak, E. The efficacy of botulinum toxin A lower limb injections in addition to physiotherapy approaches in children with cerebral palsy: A systematic review. NeuroRehabilitation 2019, 44, 175–189. [Google Scholar] [CrossRef]
- Zanon, M.A.; Pacheco, R.L.; Latorraca, C.D.O.C.; Martimbianco, A.L.C.; Pachito, D.V.; Riera, R. Neurodevelopmental Treatment (Bobath) for Children With Cerebral Palsy: A Systematic Review. J. Child Neurol. 2019, 34, 679–686. [Google Scholar] [CrossRef]
- Martin, L.; Baker, R.; Harvey, A. A Systematic Review of Common Physiotherapy Interventions in School-Aged Children with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2010, 30, 294–312. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.; Niles, N.; Kysh, L.; Sargent, B. Effect of Motor Intervention for Infants and Toddlers With Cerebral Palsy: A Systematic Review and Meta-analysis. Pediatr. Phys. Ther. 2022, 34, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Salazar, A.P.; Pagnussat, A.S.; Pereira, G.A.; Scopel, G.; Lukrafka, J.L. Neuromuscular electrical stimulation to improve gross motor function in children with cerebral palsy: A meta-analysis. Braz. J. Phys. Ther. 2019, 23, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Montoro-Cárdenas, D.; Cortés-Pérez, I.; Ibancos-Losada, M.D.R.; Zagalaz-Anula, N.; Obrero-Gaitán, E.; Osuna-Pérez, M.C. Nintendo® Wii Therapy Improves Upper Extremity Motor Function in Children with Cerebral Palsy: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 12343. [Google Scholar] [CrossRef] [PubMed]
- Montoro-Cárdenas, D.; Cortés-Pérez, I.; Zagalaz-Anula, N.; Osuna-Pérez, M.C.; Obrero-Gaitán, E.; Lomas-Vega, R. Nintendo Wii Balance Board therapy for postural control in children with cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2021, 63, 1262–1275. [Google Scholar] [CrossRef]
- Conner, B.C.; Remec, N.M.; Lerner, Z.F. Is robotic gait training effective for individuals with cerebral palsy? A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2022, 36, 873–882. [Google Scholar] [CrossRef]
- De Guindos-Sanchez, L.; Lucena-Anton, D.; Moral-Munoz, J.A.; Salazar, A.; Carmona-Barrientos, I. The Effectiveness of Hippotherapy to Recover Gross Motor Function in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis. Children 2020, 7, 106. [Google Scholar] [CrossRef]
- Baek, I.H.; Kim, B.J. The effects of horse riding simulation training on stroke patients’ balance ability and abdominal muscle thickness changes. J. Phys. Ther. Sci. 2014, 26, 1293–1296. [Google Scholar] [CrossRef]
- Koca, T.T.; Ataseven, H. What is hippotherapy? The indications and effectiveness of hippotherapy. North. Clin. Istanb. 2015, 2, 247. [Google Scholar] [CrossRef]
- Hyun, C.; Kim, K.; Lee, S.; Ko, N.; Lee, I.-S.; Koh, S.-E. The Short-term Effects of Hippotherapy and Therapeutic Horseback Riding on Spasticity in Children With Cerebral Palsy: A Meta-analysis. Pediatr. Phys. Ther. 2022, 34, 172–178. [Google Scholar] [CrossRef]
- Santos de Assis, G.; Schlichting, T.; Rodrigues Mateus, B.; Gomes Lemos, A.; dos Santos, A.N. Physical therapy with hippotherapy compared to physical therapy alone in children with cerebral palsy: Systematic review and meta-analysis. Dev. Med. Child Neurol. 2022, 64, 156–161. [Google Scholar] [CrossRef]
- Menor-Rodríguez, M.J.; Sevilla Martín, M.; Sánchez-García, J.C.; Montiel-Troya, M.; Cortés-Martín, J.; Rodríguez-Blanque, R. Role and Effects of Hippotherapy in the Treatment of Children with Cerebral Palsy: A Systematic Review of the Literature. J. Clin. Med. 2021, 10, 2589. [Google Scholar] [CrossRef]
- Ren, C.; Liu, T.; Zhang, J. Horse-riding simulators in treatment of chronic low back pain: A meta-analysis. Int. J. Clin. Pract. 2021, 75, e14198. [Google Scholar] [CrossRef]
- Dewar, R.; Love, S.; Johnston, L.M. Exercise interventions improve postural control in children with cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2015, 57, 504–520. [Google Scholar] [CrossRef]
- Dominguez-Romero, J.G.; Molina-Aroca, A.; Moral-Munoz, J.A.; Luque-Moreno, C.; Lucena-Anton, D. Effectiveness of Mechanical Horse-Riding Simulators on Postural Balance in Neurological Rehabilitation: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 17, 165. [Google Scholar] [CrossRef]
- Chang, H.J.; Jung, Y.G.; Park, Y.S.; O, S.H.; Kim, D.H.; Kim, C.W. Virtual Reality-Incorporated Horse Riding Simulator to Improve Motor Function and Balance in Children with Cerebral Palsy: A Pilot Study. Sensors 2021, 21, 6394. [Google Scholar] [CrossRef]
- Bordeleau, M.; Stamenkovic, A.; Tardif, P.A.; Thomas, J. The Use of Virtual Reality in Back Pain Rehabilitation: A Systematic Review and Meta-Analysis. J. Pain 2022, 23, 175–195. [Google Scholar] [CrossRef]
- Hilliere, C.; Collado-Mateo, D.; Villafaina, S.; Duque-Fonseca, P.; Parraça, J.A. Benefits of Hippotherapy and Horse Riding Simulation Exercise on Healthy Older Adults: A Systematic Review. PMR 2018, 10, 1062–1072. [Google Scholar] [CrossRef]
- Heussen, N.; Häusler, M. Equine-Assisted Therapies for Children With Cerebral Palsy: A Meta-analysis. Pediatrics 2022, 150, e2021055229. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley Blackwell & Sons: Hoboken, NJ, USA, 2020. [Google Scholar]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef]
- Meader, N.; King, K.; Llewellyn, A.; Norman, G.; Brown, J.; Rodgers, M.; Moe-Byrne, T.; Higgins, J.P.; Sowden, A.; Stewart, G. A checklist designed to aid consistency and reproducibility of GRADE assessments: Development and pilot validation. Syst. Rev. 2014, 3, 82. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Software, version 3; Biostat Inc.: Englewood, NJ, USA, 2020. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 1–421. [Google Scholar] [CrossRef]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis, 2nd ed.; Russell Sage Foundation: New York, NY, USA, 2009. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. P T 2008, 33, 700–711. [Google Scholar]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Rücker, G.; Schwarzer, G. Beyond the forest plot: The drapery plot. Res. Synth. Methods 2020, 12, 13–19. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test measures of funnel plot asymmetry. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Shi, L.; Lin, L.; Omboni, S. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; ISBN 0781755646. [Google Scholar]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Statistical heterogeneity in systematic reviews of clinical trials: A critical appraisal of guidelines and practice. J. Health Serv. Res. Policy 2002, 7, 51–61. [Google Scholar] [CrossRef]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Bagheri, H.; Gholmreza, O.; Khaleel, R.F.; Mohammad, H.; Jalaie, S.; Diab, A.S. Evaluation of horse riding simulator with strengthening training program and conventional physiotherapy in treatment of children with spastic diplegic cerebral palsy. Diyala J. Med. 2017, 13, 103–112. [Google Scholar] [CrossRef]
- Chinniah, H.; Natarajan, M.; Ramanathan, R.; Ambrose, J.W.F. Effects of horse riding simulator on sitting motor function in children with spastic cerebral palsy. Physiother. Res. Int. 2020, 25, e1870. [Google Scholar] [CrossRef]
- Silva e Borges, M.B.; Werneck, M.J.; da Silva, M.L.; Gandolfi, L.; Pratesi, R. Therapeutic effects of a horse riding simulator in children with cerebral palsy. Arq. Neuropsiquiatr. 2011, 69, 799–804. [Google Scholar] [CrossRef]
- Temcharoensuk, P.; Lekskulchai, R.; Akamanon, C.; Ritruechai, P.; Sutcharitpongsa, S. Effect of horseback riding versus a dynamic and static horse riding simulator on sitting ability of children with cerebral palsy: A randomized controlled trial. J. Phys. Ther. Sci. 2015, 27, 273–277. [Google Scholar] [CrossRef]
- Choi, H.-J.; Kim, K.-J.; Nam, K.-W. The effects of a horseback riding simulation exercise on the spinal alignment of children with cerebral palsy. J. Korean Phys. Ther. 2014, 26, 209–215. [Google Scholar]
- Choi, H.-J.; Nam, K.-W. The effect of horseback riding simulator on static balance of cerebral palsy. J. Korean Phys. Ther. 2014, 26, 269–273. [Google Scholar]
- Fernandes, L.C.; Chitra, J.; Metgud, D.; Khatri, S.M. Effectiveness of artificial horse riding on postural control in spastic diplegics− rct. IJPOT 2008, 2, 36–40. [Google Scholar]
- Hemachithra, C.; Meena, N.; Ramanathan, R.; Felix, A.J.W. Immediate effect of horse riding simulator on adductor spasticity in children with cerebral palsy: A randomized controlled trial. Physiother. Res. Int. 2020, 25, e1809. [Google Scholar] [CrossRef] [PubMed]
- Herrero, P.; Gómez-Trullén, E.M.; Asensio, Á.; García, E.; Casas, R.; Monserrat, E.; Pandyan, A. Study of the therapeutic effects of a hippotherapy simulator in children with cerebral palsy: A stratified single-blind randomized controlled trial. Clin. Rehabil. 2012, 26, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.G.; Chang, H.J.; Jo, E.S.; Kim, D.H. The Effect of a Horse-Riding Simulator with Virtual Reality on Gross Motor Function and Body Composition of Children with Cerebral Palsy: Preliminary Study. Sensors 2022, 22, 2903. [Google Scholar] [CrossRef]
- Kang, K.-Y.; Song, B.-H. Effects of horseback riding simulation machine training on gross motor function for the children with cerebral palsy. J. Korea Contents Assoc. 2010, 10, 268–284. [Google Scholar] [CrossRef]
- Quint, C.; Toomey, M. Powered saddle and pelvic mobility: An investigation into the effects on pelvic mobility of children with cerebral palsy of a powered saddle which imitates the movements of a walking horse. Physiotherapy 1998, 84, 376–384. [Google Scholar] [CrossRef]
- Collado-Mateo, D.; Lavín-Pérez, A.M.; Fuentes García, J.P.; García-Gordillo, M.Á.; Villafaina, S. Effects of Equine-Assisted Therapies or Horse-Riding Simulators on Chronic Pain: A Systematic Review and Meta-Analysis. Medicina 2020, 56, 444. [Google Scholar] [CrossRef]
- Ruggeri, A.; Dancel, A.; Johnson, R.; Sargent, B. The effect of motor and physical activity intervention on motor outcomes of children with autism spectrum disorder: A systematic review. Autism 2020, 24, 544–568. [Google Scholar] [CrossRef]
- Storm, F.A.; Petrarca, M.; Beretta, E.; Strazzer, S.; Piccinini, L.; Maghini, C.; Panzeri, D.; Corbetta, C.; Morganti, R.; Reni, G.; et al. Minimum Clinically Important Difference of Gross Motor Function and Gait Endurance in Children with Motor Impairment: A Comparison of Distribution-Based Approaches. Biomed. Res. Int. 2020, 2020, 2794036. [Google Scholar] [CrossRef]
- Chen, C.; Shen, I.; Chen, C.; Wu, C.; Liu, W.-Y.; Chung, C. Validity, responsiveness, minimal detectable change, and minimal clinically important change of Pediatric Balance Scale in children with cerebral palsy. Res. Dev. Disabil. 2013, 34, 916–922. [Google Scholar] [CrossRef]
- Van Criekinge, T.; Saeys, W.; Vereeck, L.; De Hertogh, W.; Truijen, S. Are unstable support surfaces superior to stable support surfaces during trunk rehabilitation after stroke? A systematic review. Disabil. Rehabil. 2018, 40, 1981–1988. [Google Scholar] [CrossRef]
- Marshall, P.W.; Murphy, B.A. Core stability exercises on and off a Swiss ball. Arch. Phys. Med. Rehabil. 2005, 86, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Bertoncelli, C.M.; Altamura, P.; Bertoncelli, D.; Rampal, V.; Vieira, E.R.; Solla, F. PredictMed: A Machine Learning Model for Identifying Risk Factors of Neuromuscular Hip Dysplasia: A Multicenter Descriptive Study. Neuropediatrics 2021, 52, 343–350. [Google Scholar] [CrossRef]
- Mat Rosly, M.; Mat Rosly, H.; Hasnan, N.; Davis, G.M.; Husain, R. Exergaming boxing versus heavy-bag boxing: Are these equipotent for individuals with spinal cord injury? Eur. J. Phys. Rehabil. Med. 2017, 53, 527–534. [Google Scholar] [CrossRef]
- Chen, M.-H.; Huang, L.-L.; Lee, C.-F.; Hsieh, C.-L.; Lin, Y.-C.; Liu, H.; Chen, M.-I.; Lu, W.-S. A controlled pilot trial of two commercial video games for rehabilitation of arm function after stroke. Clin. Rehabil. 2015, 29, 674–682. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | Search Strategies |
|---|---|
| PubMed Medline | (Horse riding simulator[tiab] OR horse-riding simulator[tiab] OR horse simulator[tiab] OR simulator horse[tiab] OR horse virtual[tiab] OR simulator equine[tiab] OR virtual reality horse simulator[tiab]) AND (cerebral palsy[mh] OR cerebral palsy[tiab] OR infantile cerebral palsy[tiab]) |
| SCOPUS | (TITLE-ABS-KEY (“cerebral palsy”) AND TITLE-ABS-KEY (“Horse riding simulator” OR “horse simulator” OR “simulator horse” OR “simulator equine”)) |
| Web of Science | TOPIC: (*cerebral palsy*) AND TOPIC: (*Horse riding simulator* OR *horse simulator* OR *simulator horse* OR *simulator equine*) |
| CINAHL Complete | AB (cerebral palsy) AND AB (Horse riding simulator OR horse simulator OR simulator horse OR simulator equine) |
| PEDro | Cerebral palsy AND horse riding simulator |
| SciELO | Cerebral palsy AND horse riding simulator |
| Study | Pathology | Experimental Intervention | Control Intervention | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CP Type | GMFCS | N | Ne | Age | F:M | Intervention | Nc | Age | F:M | Intervention | |
| Bagheri, H et al., 2017 (Iraq) [63] Setting: Medical Rehabilitation and Rheumatology Center, Baghdad, Iraq Funding: No | Spastic diplegic CP | II–III | 30 | 11 | 4–13 years old | 4:7 | HRS plus strengthening training 8 weeks, 3 sessions per week, 75 min per session (15 min HRS plus 60 min of abdomen, back and lower limb strengthening exercises) | 8 | 4–13 years old | 3:5 | Conventional therapy. 8 weeks, 3 sessions per week, 60 min per session. |
| 11 | 4–13 years old | 5:6 | HRS plus conventional therapy 8 weeks, 3 sessions per week, 75 min per session (15 min HRS plus 60 min of conventional therapy) | ||||||||
| Chinniah, H et al., 2020 (India) [64] Setting: Deparment of Physical Medicine and Rehabilitation, Annamalai Nagar, Tamil Nadul Funding: No | Spastic diplegic CP | I–III | 30 | 15 | 2–3 years old | 10:5 | HRS plus conventional therapy 12 weeks, 3 days per week for 45 min per session (15 min of HRS plus 30 min of conventional therapy) | 15 | 2–3 years old | 7:8 | Conventional therapy 12 weeks, 3 days per week, for 30 min per session. |
| Choi, HJ et al., 2014a (South Korea) [65] Setting: Suncheon Pyungwha Hospital Funding: No | Spastic diplegic CP | I–IV | 30 | 15 | 8.8 ± 3.1 years old | 4:11 | Neurodevelopmental treatment plus HRS 10 weeks, 4 sessions per week, 45 min per session (30 min Neurodevelopmental treatment plus 15 min HRS) | 15 | 9.3 ± 3.8 | 5:10 | Neurodevelopmental treatment 10 weeks, 4 sessions per week, 30 min per session |
| Choi, HJ and Nam, KW 2014b (South Korea) [66] Setting: Suncheon Pyungwha Hospital Funding: No | Spastic diplegic CP | I–IV | 30 | 15 | 8.8 ± 3.14 years old | 4:11 | Neurodevelopmental treatment plus HRS 10 weeks, 4 sessions per week, 45 min per session (30 min Neurodevelopmental treatment plus 15 min HRS) | 15 | 9.27 ± 3.8 years old | 5:10 | Neurodevelopmental treatment 10 weeks, 4 sessions per week, 30 min per session |
| Fernandes, LC et al., 2018 (India) [67] Setting: K.L.E.S Hospital and MRC, Belgaum, Karnataka Funding: No | Spastic diplegic CP | I–III | 30 | 15 | 6.9 ± 1.9 years old | 8:7 | HRS plus Conventional therapy 6 weeks, 3 sessions per week, 60 min per session (30 min conventional therapy plus 30 min HRS) | 15 | 7.5 ± 2 years old | 7:8 | Conventional therapy 6 weeks, 3 sessions per week, 60 min per session |
| Hemachithra, C et al., 2020 (India) [68] Setting: Physical Medicine and Rehabilitation, Rajah Muthiah Medical College Hospital, Annamalai University Funding: No | Spastic diplegic CP | I–III | 24 | 12 | 2–4 years old | 6:6 | HRS One session, 30 min per session | 12 | 2–4 years old | 6:6 | Sham One session, 30 min per session |
| Herrero, P et al., 2012 (Spain) [69] Setting: Schools run by the Department of Education of the Government of Aragon, Spain. Funding: Aragon Government: PM059/2007 | Spastic diplegic CP | I–IV | 38 | 19 | 9.95 ± 0.6 years old | 5:14 | HRS 10 weeks, 1 session per week, 15 min per session | 19 | 9.05 ± 0.7 years old | 9:10 | Sham 10 weeks, 1 session per week, 15 min per session |
| Jung, YG et al., 2022 (South Korea) [70] Setting: Samsung Changwon Hospital Funding: No | Spastic diplegic CP | I–IV | 17 | 10 | 9.33 ± 2.1 years old | 3:7 | HRS plus Conventional therapy 8 weeks, 2 sessions per week, 30 min per session | 7 | 9.08 ± 2.4 years old | 3:4 | Conventional therapy plus home bases aerobic exercise 8 weeks, 2 sessions per week |
| Kang, KY et al., 2010 (South Korea) [71] Setting: NR Funding: No | Spastic diplegic CP | III–IV | 24 | 12 | 10.5 ± 2.9 years old | 6:6 | HRS plus Conventional therapy 12 weeks, 3 sessions per week, 45 min per session (30 min conventional therapy plus 15 min HRS) | 12 | 9.08 ± 2.1 years old | 5:7 | Conventional therapy 12 weeks, 3 sessions per week, 30 min per session |
| Quint, C et al., 1998 (USA) [72] Setting: The Lord Mayor Treloar School. Alton, Illinois. Funding: No | Spastic diplegic CP | NR | 30 | 15 | 9–16 years old | NR | HRS 4 weeks, 10 times during the school day, 10 min per session | 15 | 9–16 years old | NR | Sham 4 weeks, 10 times during the school day, 10 min per session |
| Silva-Borges, MB et al., 2011 (Brazil) [73] Setting: The Clinic of Physiotherapy and Laboratory of Biomechanics of the Catholic University of Brasilia Funding: No | Spastic diplegic CP | I–V | 40 | 20 | 5.65 ± 2.48 years old | 12:8 | HRS 6 weeks, 2 sessions per week, 40 min per session | 20 | 5.77 ± 2.3 years old | 11:9 | Conventional therapy 6 weeks, 2 sessions per week, 40 min per session |
| Temcharoensuk, P et al., 2015 (Thailand) [74] Setting: Rehabilitation Centre, Mahidol Funding: No | Spastic diplegic CP | I–III | 20 | 10 | 10.1 ± 1.7 years old | 6:4 | HRS 30 min per session | 10 | 10.4 ± 1.5 years old | 5:5 | Sham 30 min per session |
| Study | Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias | |
|---|---|---|---|---|---|---|---|
| Random Sequence Generation | Allocation Concealment | Blinding of Participants | Blinding of Assessors | Incomplete Outcome Data | Selective Reporting | Anything Else, Ideally Pre-Specified | |
| Bagheri, H et al., 2017 [63] | − | − | + | + | − | ? | − |
| Chinniah, H et al., 2020 [64] | − | − | + | + | − | ? | − |
| Choi, HJ et al., 2014a [65] | − | + | + | + | − | ? | − |
| Choi, HJ and Nam, KW 2014b [66] | − | + | + | + | − | ? | − |
| Fernandes, LC et al., 2018 [67] | − | + | + | + | − | − | ? |
| Hemachithra, C et al., 2020 [68] | − | − | + | − | − | ? | − |
| Herrero, P et al., 2012 [69] | − | − | + | − | − | − | − |
| Jung, YG et al., 2022 [70] | ? | ? | + | + | − | − | ? |
| Kang, KY et al., 2010 [71] | − | + | + | + | − | − | ? |
| Quint, C et al., 1998 [72] | − | − | + | − | − | − | ? |
| Silva−Borges, MB et al., 2011 [73] | − | + | + | − | − | − | ? |
| Temcharoensuk, P et al., 2015 [74] | − | + | + | − | − | − | ? |
| Study | Outcomes | ||
|---|---|---|---|
| Variable | Test | Qualitative Findings | |
| Bagheri, H et al., 2017 [63] | GMF (Total) | GMFM-66 | Statistically significant differences in HRS plus strength training and HRS plus conventional therapy groups (p = 0.021 and p = 0.001 respectively), but not in conventional therapy alone (p = 0.156) |
| Functional balance | PBS | No statistically significant differences in all groups (p > 0.05) | |
| Adductors spasticity | MMAS | No significant differences were found between groups and within groups (p > 0.05) | |
| Knee flexors spasticity | MMAS | No significant differences were found in each group (p < 0.05) | |
| Ankle plantar flexors spasticity | MMAS | Statistically significant differences in HRS plus strength training group in right ankle plantar flexors strength (p = 0.05) | |
| Chinniah, H et al., 2020 [64] | GMF (B Dimension) | GMFM-88 | Both groups reported significant improvements (p < 0.001, respectively). The experimental groups show higher mean values than the control group. Statistically significant differences were found between groups (p = 0.028). Interaction analysis showed more improvement in the experimental group than the control group in each comparison (week assessment). |
| Choi, HJ et al., 2014a [65] | Posturographic spinal posture | ABW Mapper | Statistically significant differences in interaction between groups and periods in trunk imbalance, pelvic torsion and pelvic tilt (p < 0.05). |
| Choi, HJ and Nam, KW 2014b [66] | Posturographic static balance | Pedoscan sensor | No significant differences in interaction between the group and period (p > 0.05). Statistically significant differences between groups in ML sway (p < 0.05) No significant differences between groups and within groups in AP sway (p > 0.05). |
| Fernandes, LC et al., 2018 [67] | Functional balance | PBS | Statistically significant differences in both groups (p < 0.0001 respectively). No statistically significant differences were found between groups in the post-intervention assessment (p = 0.4516) |
| GMF (Total) | GMFM-66 | Statistically significant differences in both groups (p < 0.0001 respectively). No statistically significant differences were found between groups in the post-intervention assessment (p = 0.4516) | |
| Hemachithra, C et al., 2020 [68] | Adductors spasticity | MAS | Statistically significant differences in the experimental group (p < 0.001). Statistically significant differences between groups (p < 0.001) |
| Hip ROM | Goniometry | Statistically significant differences in the experimental group (p < 0.001). Statistically significant differences between groups (p < 0.001) | |
| Herrero, P et al., 2012 [69] | GMF (Total and B dimension) | GMFM-66 | Both groups improved, although the HRS group reported greater scores than the control group in sitting and total GMFM |
| Jung, YG et al., 2022 [70] | GMF (Total and A, B, C, D and E dimensions) | GMFM-88 | For A, B and C dimensions, no statistically significant differences between groups and within groups (p > 0.05). For the D dimension, statistically significant differences were found in HRS (p = 0.03) but not between groups (p = 0.06). For the E dimension, statistically significant differences were found in HRS (p =0.03) but not between groups (p = 0.19). For GMFM total score, statistically significant differences in the HRS group (p < 0.01) and between groups favors HRS (p < 0.01) |
| Kang, KY et al., 2010 [71] | GMF (Total and A, B, C, D and E dimensions) | GMFM-88 | Statistically significant differences in A and B dimensions in the control group (p = 0.04 and p = 0.019, respectively). Statistically significant differences in all items in the HRS group (p < 0.05). Significant differences between groups favor HRS in the C, D and E dimensions (p = 0.04, p = 0.047 and p = 0.049, respectively). |
| Quint, C et al., 1998 [72] | Pelvic ROM | Goniometry | Both groups improved, although the experimental group reported a greater pelvic ROM after the intervention. |
| Silva-Borges, MB et al., 2011 [73] | Postural control (AP and ML) | F-mat sensor platform and F-scan system. | Statistically significant differences between groups favor the experimental group (p < 0.0001) in AP and ML displacement. |
| Satisfaction | AUQEI | Scores were higher on the “physiotherapy” item in the HRS group, finding statistically significant differences (p = 0.0026). No child was unhappy with the use of the simulator, while 25% of children belonging to the CT group were unhappy with the therapy. | |
| GMF (Sitting ability | GMFCS | Statistically significant differences in the HRS group (p = 0.0110). No between groups | |
| Temcharoensuk, P et al., 2015 [74] | GMF | GMFM-66 | No statistically significant differences in both groups (p > 0.05). No statistically significant differences between groups (p > 0.05) |
| Seated trunk control | SATco | Statistically significant differences in all groups. HR group reported more items with significant differences. The “Reactive control” item was statistically significant among the three groups (p < 0.05). Statistically significant differences were found in “reactive control” in the HR group vs. the SHS group comparison (p = 0.004). | |
| Findings Summary | Quality Evidence (Grade) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect Size | Heterogeneity | Publication Bias | ||||||||||||||||
| K | N | Ns | SMD | 95% CI | p | Q (df) | I2 (p) | Egger p | Trim and Fill | Risk of Bias | Incons | Indirect | Imprec | Publ. Bias | Quality | |||
| Adj SMD | % Var | |||||||||||||||||
| GMF (A dimension) | HRS + PT vs. PT | 2 | 41 | 20.5 | 0.25 | −0.28–0.79 | 0.353 | 0.01 (1) | 0% (0.92) | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low |
| GMF (B dimension) | Overall | 5 | 129 | 25.8 | 0.52 | 0.15–0.9 | 0.006 | 9.65 (4) | 41% (0.04) | 0.07 | 0.6 | 15% | Mod. | Mod. | No | Yes | Yes | Very low |
| HRS + PT vs. PT | 3 | 71 | 23.6 | 0.84 | 0.32–1.36 | 0.002 | 3.5 (2) | 42% (0.17) | 0.62 | 0.84 | 0% | Mod. | Mod. | No | Yes | No | Low | |
| HRS vs. sham | 2 | 58 | 29 | 0.19 | −0.34–0.72 | 0.49 | 0.004 (1) | 0% (0.94) | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low | |
| GMF (C dimension) | HRS + PT vs. PT | 2 | 41 | 20.5 | 0.19 | −0.42–0.81 | 0.54 | 0.09 (1) | 0% (0.76) | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low |
| GMF (D dimension) | HRS + PT vs. PT | 2 | 41 | 20.5 | 0.32 | −0.31–0.94 | 0.32 | 0.338 (1) | 2% (0.56) | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low |
| GMF (E dimension) | HRS + PT vs. PT | 2 | 41 | 20.5 | 0.13 | −0.48–0.75 | 0.67 | 0.04 (1) | 0% (0.84) | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low |
| GMF (Total) | Overall | 7 | 187 | 26.7 | 0.64 | 0.34–0.94 | <0.001 | 6.72 (6) | 10.7% (0.35) | 0.13 | 0.64 | 0% | Mod. | Low | No | Yes | No | Mod. |
| HRS + PT vs. PT | 5 | 109 | 21.4 | 0.98 | 0.35–1.62 | 0.002 | 4.85 (4) | 17.6% (0.31) | 0.08 | 1.11 | 13% | Mod. | Low | No | Yes | Yes | Low | |
| HRS vs. PT | 1 | 40 | 40 | 0.41 | −0.82–1.64 | 0.52 | 0 (0) | 0% | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low | |
| HRS vs. sham | 1 | 38 | 38 | 0.15 | −1.01–1.4 | 0.8 | 0 (0) | 0% | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low | |
| Funct. balance | HRS + PT vs. PT | 3 | 68 | 22.7 | 0.6 | 0.1–1.08 | 0.018 | 0.43 (2) | 0% (0.8) | 0.81 | 0.6 | 0% | Mod. | No | No | Yes | No | Low |
| Abduction pelvic ROM | HRS vs. sham | 2 | 54 | 27 | 0.79 | 0.21–1.37 | 0.008 | 2.24 (1) | 37% (0.13) | NP | NP | NP | Mod. | Mod. | No | Yes | Prob. | Very low |
| Spasticity hip add | Overall | 3 | 62 | 20.7 | −0.4 | −0.92–0.11 | 0.122 | 2.06 (2) | 3.05 (0.36) | 0.19 | −0.81 | 100% | Mod. | No | No | Yes | Yes | Low |
| HRS + PT vs. PT | 2 | 38 | 19 | −0.15 | −0.8–0.5 | 0.642 | 0.53 (1) | 0% (0.46) | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low | |
| HRS vs. sham | 1 | 24 | 24 | −0.82 | −1.65–0.02 | 0.054 | 0 (0) | 0% | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low | |
| Spasticity ankle flex | HRS + PT vs. PT | 2 | 38 | 19 | −0.55 | −1.22–0.12 | 0.11 | 0.03 (1) | 0% (0.86) | NP | NP | NP | Mod. | No | No | Yes | Prob. | Very low |
| Spasticity knee ext | HRS + PT vs. PT | 2 | 38 | 19 | −0.12 | −0.77–0.52 | 0.71 | 2.73 (1) | 57% (0.09) | NP | NP | NP | Mod. | Large | No | Yes | Prob. | Very low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obrero-Gaitán, E.; Montoro-Cárdenas, D.; Cortés-Pérez, I.; Osuna-Pérez, M.C. Effectiveness of Mechanical Horse-Riding Simulator-Based Interventions in Patients with Cerebral Palsy—A Systematic Review and Meta-Analysis. Bioengineering 2022, 9, 790. https://doi.org/10.3390/bioengineering9120790
Obrero-Gaitán E, Montoro-Cárdenas D, Cortés-Pérez I, Osuna-Pérez MC. Effectiveness of Mechanical Horse-Riding Simulator-Based Interventions in Patients with Cerebral Palsy—A Systematic Review and Meta-Analysis. Bioengineering. 2022; 9(12):790. https://doi.org/10.3390/bioengineering9120790
Chicago/Turabian StyleObrero-Gaitán, Esteban, Desirée Montoro-Cárdenas, Irene Cortés-Pérez, and María Catalina Osuna-Pérez. 2022. "Effectiveness of Mechanical Horse-Riding Simulator-Based Interventions in Patients with Cerebral Palsy—A Systematic Review and Meta-Analysis" Bioengineering 9, no. 12: 790. https://doi.org/10.3390/bioengineering9120790
APA StyleObrero-Gaitán, E., Montoro-Cárdenas, D., Cortés-Pérez, I., & Osuna-Pérez, M. C. (2022). Effectiveness of Mechanical Horse-Riding Simulator-Based Interventions in Patients with Cerebral Palsy—A Systematic Review and Meta-Analysis. Bioengineering, 9(12), 790. https://doi.org/10.3390/bioengineering9120790