
How do Paraspinal Muscles Contract during the Schroth Exercise Treatment in Patients with Adolescent Idiopathic Scoliosis (AIS)?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment Procedure
2.2.1. Before Exercise
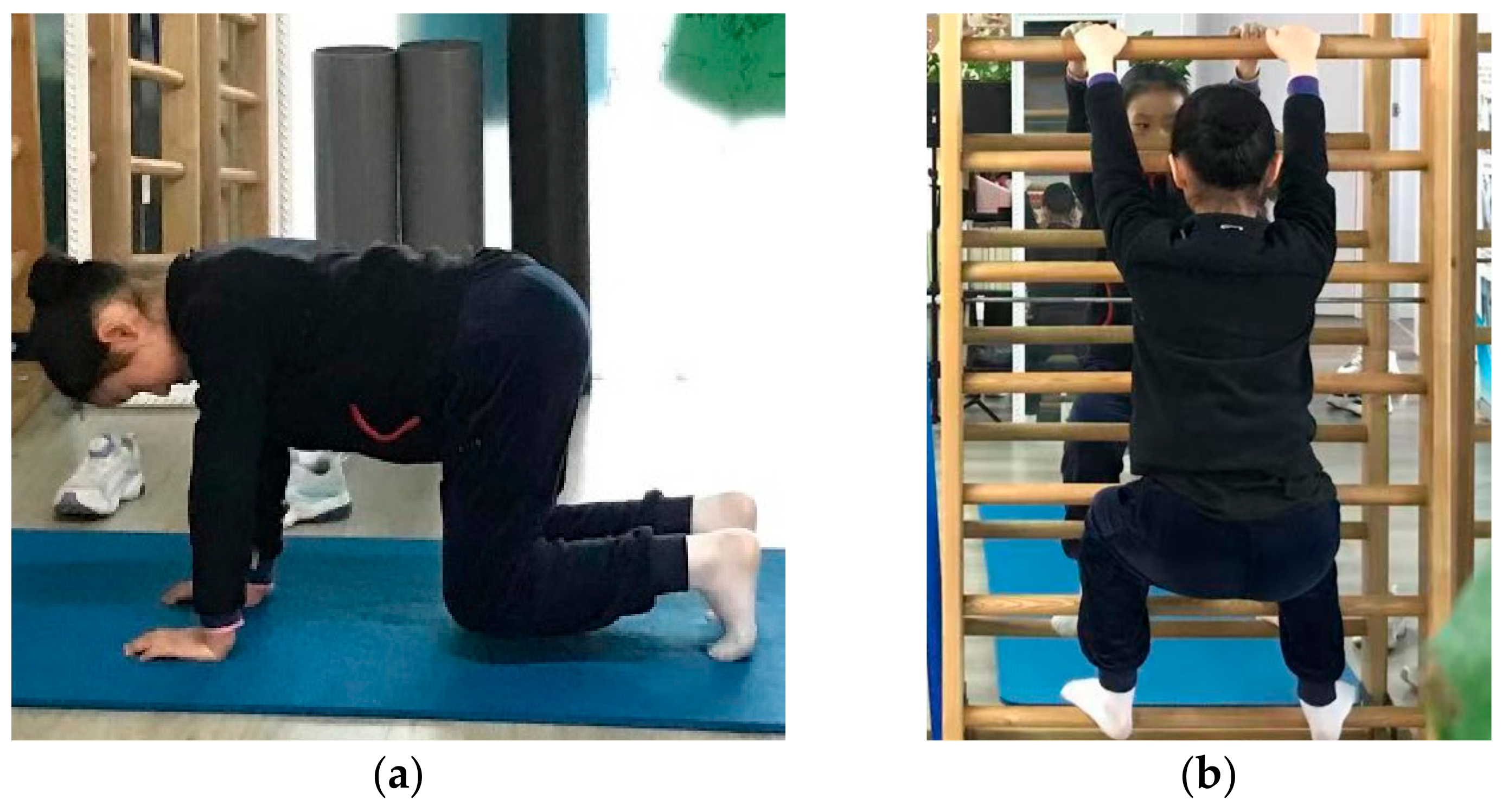
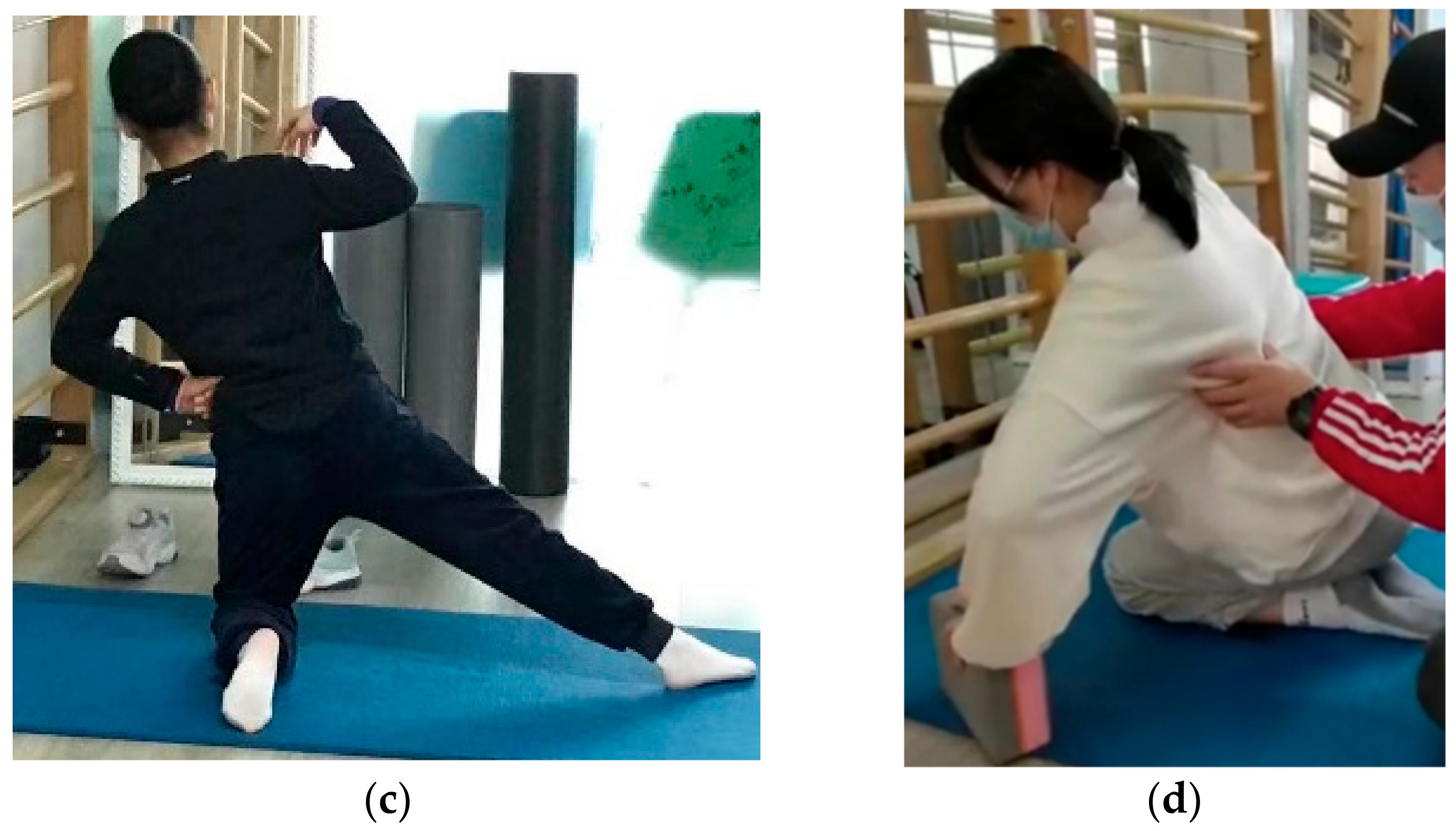
2.2.2. During Exercise
2.2.3. After Exercise
2.3. Data and Statistical Analysis
3. Results
3.1. Participants
3.2. The PMSI and RMS of sEMG Activity of Paraspinal Muscles
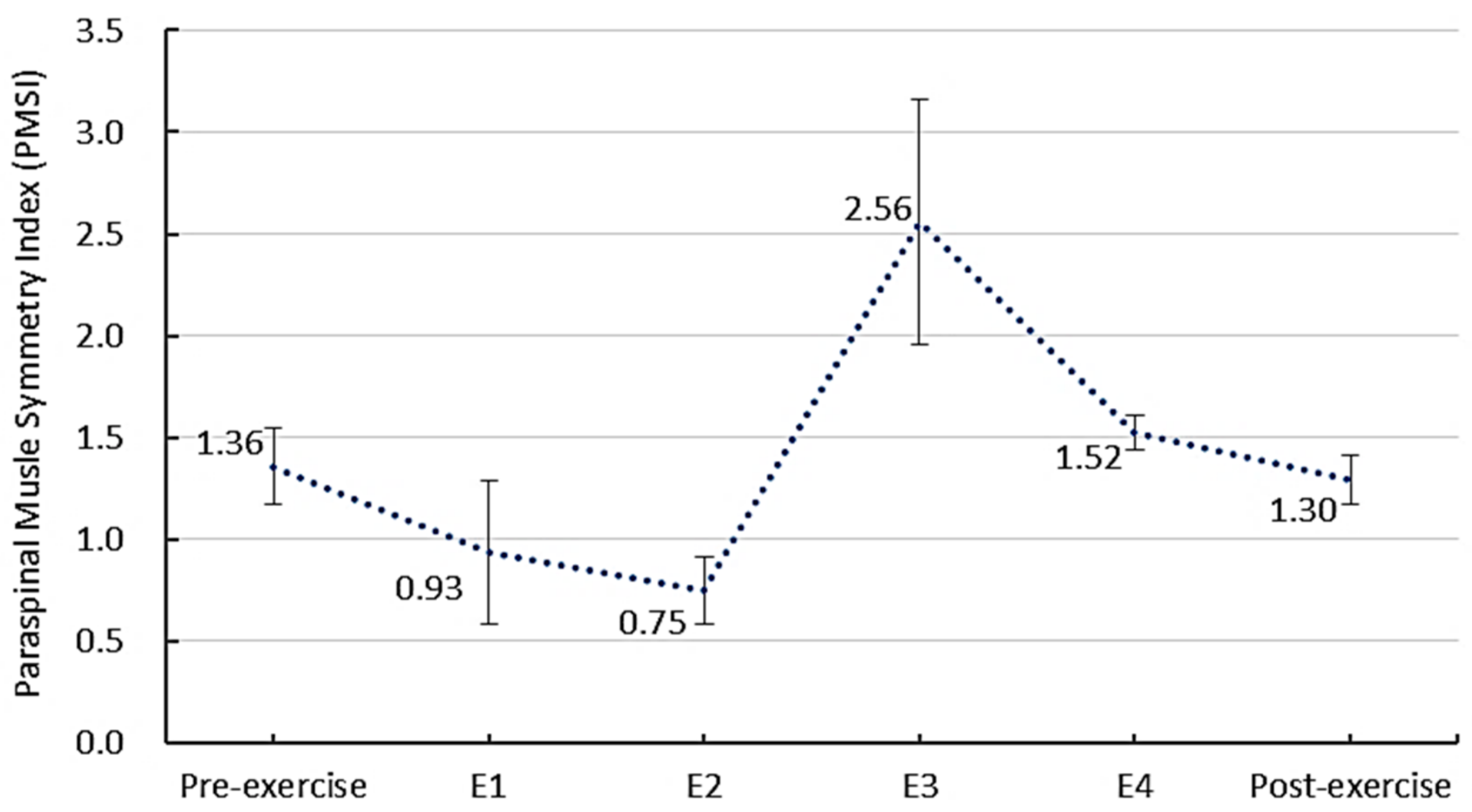
3.2.1. The PMSI before, during and after the Schroth Exercise
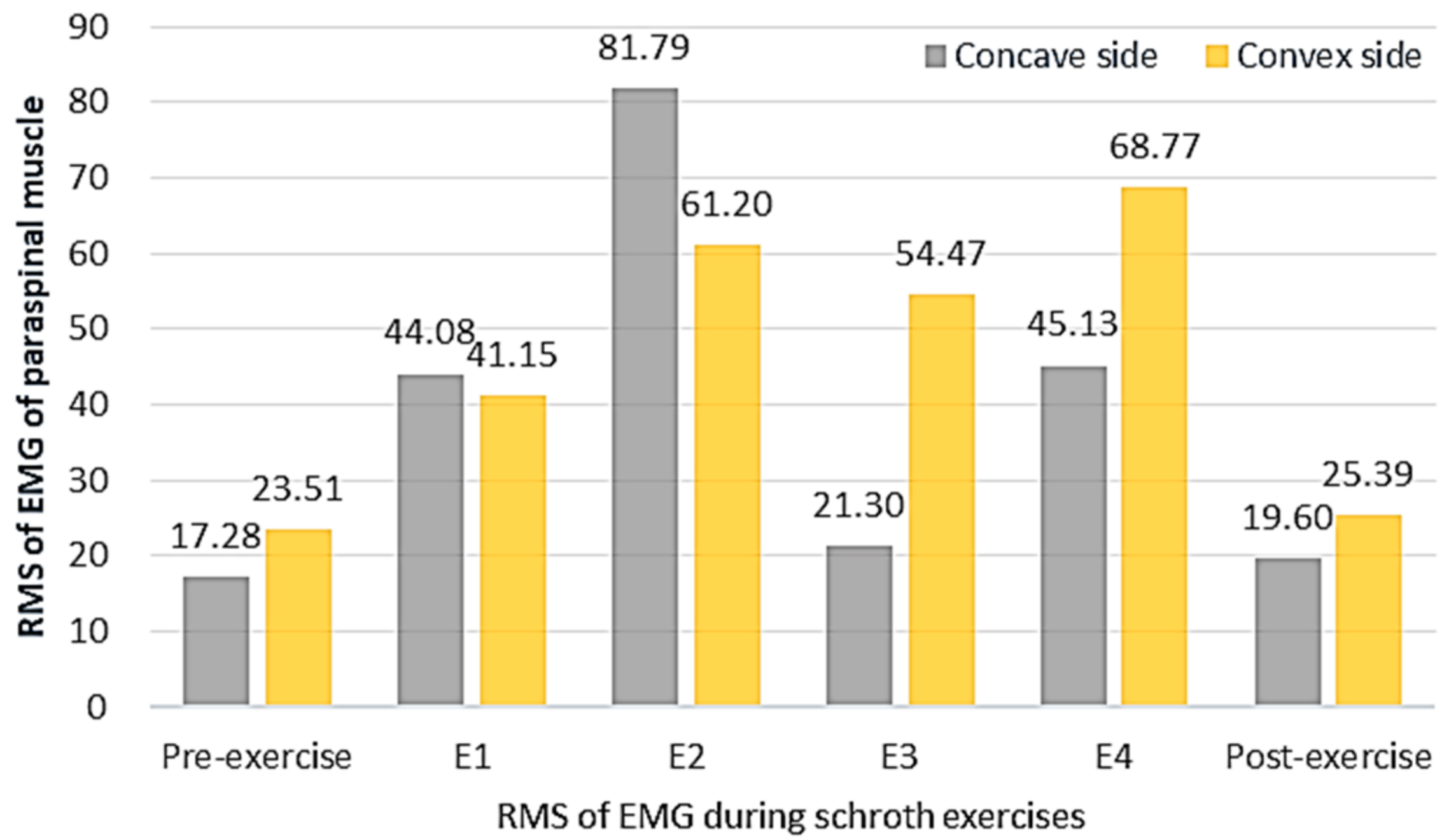
3.2.2. The RMS of sEMG Activity before, during and after the Schroth Exercise
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, H.; Guo, C.; Tang, M.; Liu, S.; Li, J.; Guo, Q.; Chen, L.; Zhu, Y.; Zhao, S. Prevalence of scoliosis among primary and middle school students in Mainland China: A systematic review and meta-analysis. Spine 2015, 40, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Dang, Y.; Wu, X.; Yang, Y.; Reinhardt, J.D.; He, C.; Wong, M. Epidemiological study of adolescent idiopathic scoliosis in Eastern China. J. Rehabil. Med. 2017, 49, 512–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avikainen, V.J.; Rezasoltani, A.; Kauhanen, H.A. Asymmetry of paraspinal EMG-time characteristics in idiopathic scoliosis. J. Spinal Disord. 1999, 12, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Cheung, J.; Veldhuizen, A.G.; Halbertsma, J.; Maurits, N.M.; Sluiter, W.J.; Cool, J.C.; Horn, J.V. The Relation Between Electromyography and Growth Velocity of the Spine in the Evaluation of Curve Progression in Idiopathic Scoliosis. Spine 2004, 29, 1011–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannion, A.; Meier, M.; Grob, D.; Muntener, M. Paraspinal muscle fibre type alterations associated with scoliosis: An old problem revisited with new evidence. Eur. Spine J. 1998, 7, 289–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, H.R. Imbalance of electromyographic activity and physical rehabilitation of patients with idiopathic scoliosis. Eur. Spine J. 1993, 1, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Yang, S.; Chen, C.; Luo, K.; Chen, Y.; Wang, D.; Tan, J.; Dai, Q.; Zhang, C.; Wu, W. Assessment of the association between paraspinal muscle degeneration and quality of life in patients with degenerative lumbar scoliosis. Exp. Ther. Med. 2020, 20, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, A.B.; Dyer, L.; Böni, T.; Held, U.; Brunner, F. Paraspinal muscle activity during symmetrical and asymmetrical weight training in idiopathic scoliosis. J. Sport Rehabil. 2010, 19, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Chwala, W.; Koziana, A.; Kasperczyk, T.; Walaszek, R.; Plaszewski, M. Electromyographic assessment of functional symmetry of paraspinal muscles during static exercises in adolescents with idiopathic scoliosis. Biomed Res. Int. 2014, 2014, 573276. [Google Scholar] [CrossRef] [PubMed]
- Strasse, W.; Stadnik, A.; Beraldo, L.M.; Oliveira, K.D. Analysis of the electromyography and symmetrography technologies in the treatment of scoliosis. In Proceedings of the Global Medical Engineering Physics Exchanges/Pan American Health Care Exchanges, Porto, Portugal, 19–24 March 2018; pp. 1–5. [Google Scholar]
- Tsai, Y.-T.; Leong, C.-P.; Huang, Y.-C.; Kuo, S.-H.; Wang, H.-C.; Yeh, H.-C.; Lau, Y.-C. The electromyographic responses of paraspinal muscles during isokinetic exercise in adolescents with idiopathic scoliosis with a Cobb’s angle less than fifty degrees. Chang. Gung Med. J. 2010, 33, 540–550. [Google Scholar] [PubMed]
- Lehnert-Schroth, C. Three-Dimensional Treatment for Scoliosis: A Physiotherapeutic Method for Deformities of the Spine; The Martindale Press: Palo Alto, CA, USA, 2007. [Google Scholar]
- Schreiber, S.; Parent, E.C.; Hedden, D.M.; Moreau, M.; Hill, D.; Lou, E. Effect of Schroth exercises on curve characteristics and clinical outcomes in adolescent idiopathic scoliosis: Protocol for a multicentre randomised controlled trial. J. Physiother. 2017, 60, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiber, S. Schroth Exercises for Adolescent Idiopathic Scoliosis—Reliability, A Randomized Controlled Trial and Clinical Significance. Ph.D. Thesis, University of Alberta, Edmonton, AB, Canada, 2015. [Google Scholar]
- Weiss, H.; Weiss, G.; Petermann, F. Incidence of curvature progression in idiopathic scoliosis patients treated with scoliosis in-patient rehabilitation (SIR): An age- and sex-matched cotrolled study. Pediatr. Rehabil. 2003, 6, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Fusco, C.; Minozzi, S.; Atanasio, S.; Zaina, F.; Romano, M. Exercises reduce the progression rate of adolescent idiopathic scoliosis: Results of a comprehensive systematic review of the literature. Disabil. Rehabil. 2008, 30, 772–785. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.-R. Scoliosis-related pain in adults: Treatment influences. Eur. J. Phys. Med. Rehabil. 1993, 3, 91–94. [Google Scholar]
- Otman, S.; Kose, N.; Yakut, Y. The efficacy of Schroth’s 3-dimensional exercise therapy in the treatment of AIS in Turkey. Saudi Med. J. 2005, 26, 1429–1435. [Google Scholar] [PubMed]
- Bylund, P.; Jansson, E.; Dahlberg, E.; Eriksson, E. Muscle fiber types in thoracic erector spinae muscles. Fiber types in idiopathic and other forms of scoliosis. Clin. Orthop. Relat. Res. 1987, 214, 222–228. [Google Scholar] [CrossRef]
- He, C.; To, K.T.; Chan, C.K.; Wong, M.S. Significance of recumbent curvature in prediction of in-orthosis correction for adolescent idiopathic scoliosis. Prosthet. Orthot. Int. 2019, 43, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Mattei, T.A. Do not miss it: Paraspinal muscle atrophy in the concave side of the curve in patients with adult degenerative scoliosis. Spine J. 2013, 13, 987–988. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.H.; Ren, L.J.; Cheng, L.K.; Zheng, Y.P. Mapping of Back Muscle Stiffness along Spine during Standing and Lying in Young Adults: A Pilot Study on Spinal Stiffness Quantification with Ultrasound Imaging. Sensors 2020, 20, 7317. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Description |
|---|---|
| Age | 15.2 ± 3.3 years |
| Gender | 9 females |
| Body Mass Index (BMI) | 18.56 ± 1.66 |
| Cobb Angle | 31.56° ± 8.29° |
| Curve Type | C curve |
| Apex | T7~L2 |
| Risser Sign | 0~5 |
| RMSconcave (μV) | RMSconvex (μV) | PMSI | p Values | |
|---|---|---|---|---|
| Pre-exercise | 17.28 ± 6.18 | 23.51 ± 6.55 | 1.36 ± 0.19 * | <0.01 |
| E 1 | 44.08 ± 14.58 | 41.15 ± 20.49 | 0.93 ± 0.35 | 0.08 |
| E 2 | 81.79 ± 24.01 | 61.20 ± 44.59 | 0.75 ± 0.16 | 0.06 |
| E 3 | 21.30 ± 15.72 | 54.47 ± 5.37 | 2.56 ± 0.60 * | <0.01 |
| E 4 | 45.13 ± 21.19 | 68.77 ± 16.51 | 1.52 ± 0.09 * | <0.01 |
| Post-exercise | 19.60 ± 6.17 | 25.39 ± 5.34 | 1.30 ± 0.12 * | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, C.; Yang, J.-T.; Zheng, Q.; Mei, Z.; Ma, C.Z.-H. How do Paraspinal Muscles Contract during the Schroth Exercise Treatment in Patients with Adolescent Idiopathic Scoliosis (AIS)? Bioengineering 2022, 9, 234. https://doi.org/10.3390/bioengineering9060234
He C, Yang J-T, Zheng Q, Mei Z, Ma CZ-H. How do Paraspinal Muscles Contract during the Schroth Exercise Treatment in Patients with Adolescent Idiopathic Scoliosis (AIS)? Bioengineering. 2022; 9(6):234. https://doi.org/10.3390/bioengineering9060234
Chicago/Turabian StyleHe, Chen, Jian-Tao Yang, Qian Zheng, Zhao Mei, and Christina Zong-Hao Ma. 2022. "How do Paraspinal Muscles Contract during the Schroth Exercise Treatment in Patients with Adolescent Idiopathic Scoliosis (AIS)?" Bioengineering 9, no. 6: 234. https://doi.org/10.3390/bioengineering9060234
APA StyleHe, C., Yang, J.-T., Zheng, Q., Mei, Z., & Ma, C. Z.-H. (2022). How do Paraspinal Muscles Contract during the Schroth Exercise Treatment in Patients with Adolescent Idiopathic Scoliosis (AIS)? Bioengineering, 9(6), 234. https://doi.org/10.3390/bioengineering9060234