
British Columbia’s Index of Multiple Deprivation for Community Health Service Areas


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Data Description
2.2.1. Data Dictionary
- Variables
- Descriptions
2.2.2. BCIMD Notes and Dimensions
- Data Notes
- Indicator dimensions
2.2.3. BCIMD CHSA 2016 Data (Column Names)
- CHSA2018_NUM
- CHSA18_NAM
- Ethno_Cultural_Composition_Quint
- Ethno_Cultural_Composition_Score
- Economic_Dependency_Quint
- Economic_dependency_Scores
- Residential_Instability_Quint
2.3. Data Analysis
3. Results
3.1. Data Products
3.2. Data Use
4. Discussion
4.1. Data Strengths
4.2. Data Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Source | Degrees of Freedom | Sum of Squares | Mean Square | F Value | Pr > F |
|---|---|---|---|---|---|
| Ethno-cultural composition | |||||
| Model | 6 | 273.4 | 45.6 | 61.5 | <0.0001 |
| Error | 206 | 152.6 | 0.7 | ||
| Corrected Total | 212 | 426.0 | |||
| Residential instability | |||||
| Model | 6 | 75.4 | 12.6 | 7.4 | <0.0001 |
| Error | 206 | 350.6 | 1.7 | ||
| Corrected Total | 212 | 426.0 | |||
| Economic dependency | |||||
| Model | 6 | 71.6 | 11.9 | 6.9 | <0.0001 |
| Error | 206 | 354.4 | 1.7 | ||
| Corrected Total | 212 | 426.0 | |||
| Situational vulnerability | |||||
| Model | 6 | 109.9 | 18.3 | 11.9 | <0.0001 |
| Error | 206 | 316.1 | 1.5 | ||
| Corrected Total | 212 | 426.0 | |||

References
- Zhang, L.R.; Rasali, D. Life expectancy ranking of Canadians among the populations in selected OECD countries and its disparities among British Columbians. Arch. Public Health 2015, 73, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zandy, M.; Zhang, L.R.; Kao, D.; Rajabali, F.; Turcotte, K.; Zheng, A.; Oakey, M.; Smolina, K.; Pike, I.; Rasali, D. Area-based socioeconomic disparities in mortality due to unintentional injury and youth suicide in British Columbia, 2009–2013. Health Promot. Chronic Dis. Prev. Can. 2019, 39, 35–44. [Google Scholar] [CrossRef]
- Rasali, D.; Zhang, L.R.; Guram, K.; Gustin, S.; Hay, D.I. Priority Health Equity Indicators for British Columbia: Selected Indicators Report; Provincial Health Services Authority: Vancouver, BC, Canada, 2016. [Google Scholar]
- Centers for Disease Control and Prevention. Health Disparities. Available online: https://www.cdc.gov/healthyyouth/disparities/index.htm (accessed on 15 January 2022).
- Chang, W.-C. The meaning and goals of equity in health. J. Epidemiol. Community Health 2002, 56, 488–491. [Google Scholar] [CrossRef]
- Carter-Pokras, O. What is a “health disparity”? Public Health Rep. 2002, 117, 426–434. [Google Scholar] [CrossRef]
- Townsend, P. Deprivation. J. Soc. Pol. 1987, 16, 125–146. [Google Scholar] [CrossRef]
- Pampalon, R.; Raymond, G. A deprivation index for Health and Welfare Planning in Québec. Chronic Dis. Can. 2000, 21, 104–113. [Google Scholar] [PubMed]
- Pampalon, R.; Gamache, P.; Hamel, D. The Québec Index of Material and Social Deprivation: Methodological Follow-Up, 1991 through 2006. INSPQ. Available online: https://www.inspq.qc.ca/pdf/publications/1258_QcIndexDeprivation1991-2006.pdf (accessed on 15 January 2022).
- Matern, R.; Mendelson, M.; Oliphant, M. Developing a Deprivation Index: The Research Process; Caledon Institute of Social Policy: Ottawa, ON, Canada, 2009; 26p, ISBN 1-55382-419-9. [Google Scholar]
- Canadian Institute for Health Information. Pursuit of Health Equity: Defining Stratifers for Measuring Health Inequity—A Focus on Age, Sex, Gender, Income, Education and Geographic Location; CIHI: Ottawa, ON, Canada, 2018. [Google Scholar]
- Bell, N.; Hayes, M.V. The Vancouver Area Neighbourhood Deprivation Index (Vandix): A census-based tool for assessing small-area variations in health status. Can. J. Public Health 2012, 103, S28–S32. [Google Scholar] [CrossRef] [PubMed]
- Chateau, D.; Metge, C.; Prior, H.; Soodeen, R.-A. Learning from the census: The Socio-economic Factor Index (SEFI) and health outcomes in Manitoba. Can. J. Public Health 2012, 103, S23–S27. [Google Scholar] [CrossRef] [PubMed]
- Matheson, F.I.; Dunn, J.R.; Smith, K.L.W.; Moineddin, R.; Glazier, R.H. Development of the Canadian Marginalization Index: A new tool for the study of inequality. Can. J. Public Health 2012, 103, S12–S16. [Google Scholar] [CrossRef] [PubMed]
- Pampalon, R.; Hamel, D.; Gamache, P.; Philibert, M.D.; Raymond, G.; Simpson, A. An area-based material and social deprivation index for public health in Quebec and Canada. Can. J. Public Health 2012, 103, S17–S22. [Google Scholar] [CrossRef] [PubMed]
- Poirier, M.J.P.; Wilson, M.G. Rapid Synthesis: Identifying How Area-Based Socio-Economic Indicators Are Measured in Canada. McMaster Heal Forum. 2019. Available online: https://www.mcmasterforum.org/docs/default-source/product-documents/rapid-responses/identifying-how-area-based-socio-economic-indicators-are-measured-in-canada.pdf?sfvrsn=2 (accessed on 15 January 2022).
- Statistics Canada. The Canadian Index of Multiple Deprivation—User Guide. Stat Canada Cat No 45-20-0001. 2019. Available online: https://www150.statcan.gc.ca/n1/pub/45-20-0001/452000012019002-eng.htm (accessed on 1 November 2021).
- Provincial Health Services Authority. Towards Reducing Health Inequities; Provincial Health Services Authority, Population and Public Health Program: Vancouver, BC, Canada, 2011. [Google Scholar]
- Provincial Health Services Authority. Promoting Health Equity—Choosing Appropriate Indicators: Literature Scan; Provincial Health Services Authority, Population and Public Health Program: Vancouver, BC, Canada, 2013. [Google Scholar]
- Provincial Health Services Authority. Development of Priority Health Equity Indicators for British Columbia: Process & Outcome Report; Provincial Health Services Authority, Population and Public Health Program: Vancouver, BC, Canada, 2014. [Google Scholar]
- Posser, B.; Krueger, H.; Zhang, L.R.; Li, C. Development of Area-Based Socio-Economic Deprivation Index Using Censusplus 2011. In Proceedings of the Public Health Association of BC Annual Conference, Vancouver, BC, Canada, 11–12 December 2016. [Google Scholar]
- Varas, K. Breaking New Ground in Health Analytics: B.C. Health Boundaries and Geocoded Data; BC Ministry of Health: Victoria, BC, Canada, 2019.
- Provincial Health Services Authority. Community Health Service Area profiles. Available online: http://communityhealth.phsa.ca/chsahealthprofiles (accessed on 1 November 2021).
- Relova, S.; Roth, D.; Smolina, K.; Rasali, D.; McKee, G.; Janjua, N.; Sandhu, J. Examining vaccine coverage inequity across Community Health Service Areas (CHSA) using British Columbia’s Index of Multiple Deprivation. In Proceedings of the Canadian Alliance for Regional Risk Factor Surveillance, Ottawa, ON, Canada, 5 October 2021; Available online: https://static1.squarespace.com/static/556a42d3e4b09b4e298ee5b1/t/61c1106d23e03c0f2ad410e7/1640042665089/2021_CARRFS_Proceedings_Report.pdf (accessed on 15 January 2022).
- Wang, K.; Law, C.K.; Zhao, J.; Hui, A.Y.; Yip, B.H.; Yeoh, E.K.; Chung, R.Y. Measuring health-related social deprivation in small areas: Development of an index and examination of its association with cancer mortality. Int. J. Equity Health 2021, 20, 216. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, M.Q.; Althouse, A.D.; Sabik, L.; Arnold, R.; Chu, E.; Smith, T.J.; Smith, K.; White, D.; Schenker, Y. The Association between Area Deprivation Index and Patient-Reported Outcomes in Patients with Advanced Cancer. Health Equity 2021, 5, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Jang, B.N.; Youn, H.M.; Lee, D.W.; Joo, J.H.; Park, E.C. Association between community deprivation and practising health behaviours among South Korean adults: A survey-based cross-sectional study. BMJ Open 2021, 11, e047244. [Google Scholar] [CrossRef] [PubMed]
- Frazer, J.S.; Frazer, G.R. GP prescribing in Northern Ireland by deprivation index: Retrospective analysis. Fam. Med. Community Health 2020, 8, e000376. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.E.; Crear-Perry, J.; Green, C.; Felker-Kantor, E.; Theall, K. Privilege and deprivation in Detroit: Infant mortality and the Index of Concentration at the Extremes. Int. J. Epidemiol. 2019, 48, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.J.; Chen, Y.; Serrano-Lomelin, J.; Talbot, J.; Yasui, Y. Higher levels of social and material deprivation are associated with higher rates of influenza-like illness-related emergency department visits: Edmonton, Alberta, 2004–2014. Public Health 2020, 189, 117–122. [Google Scholar] [CrossRef] [PubMed]

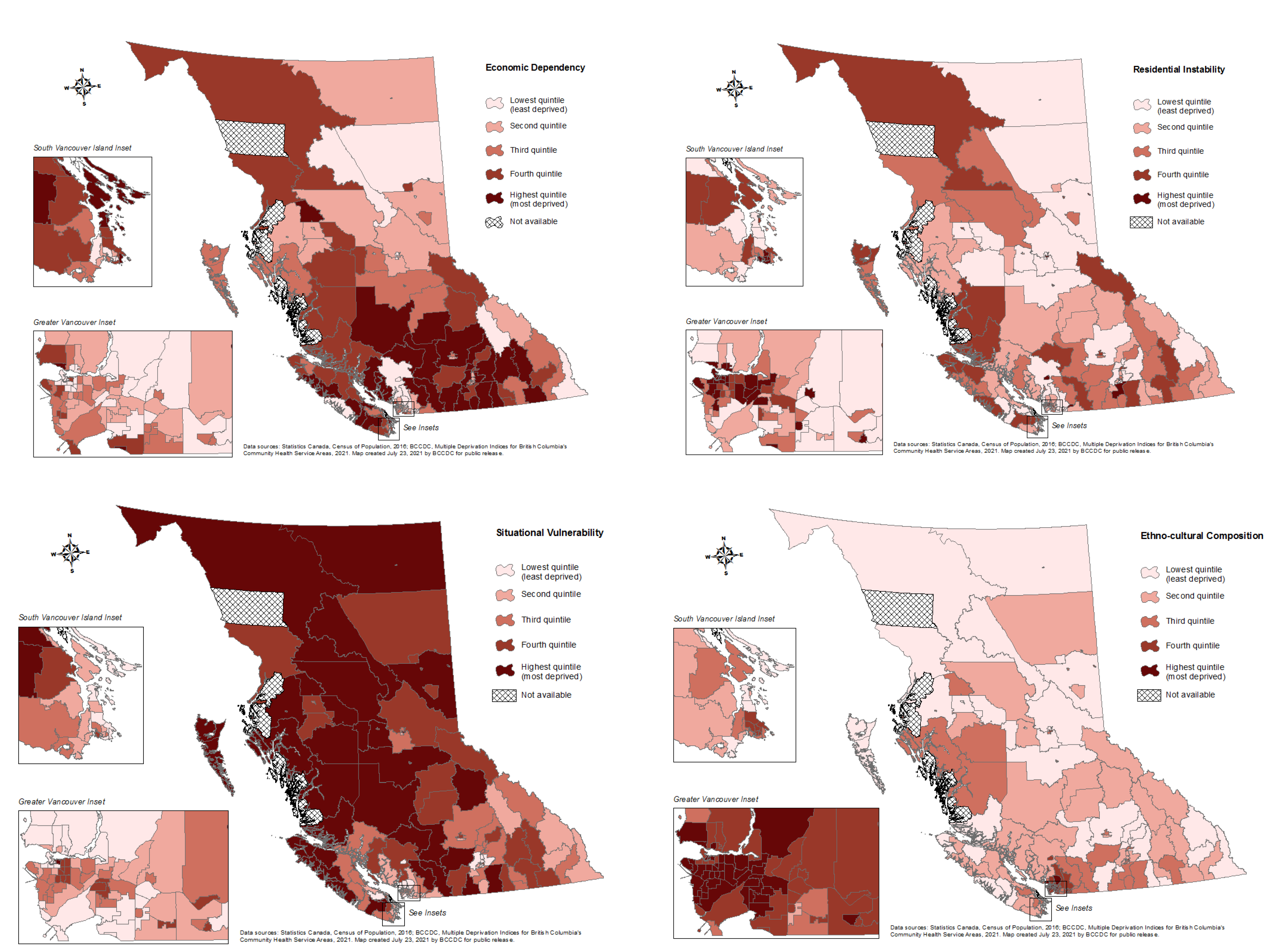
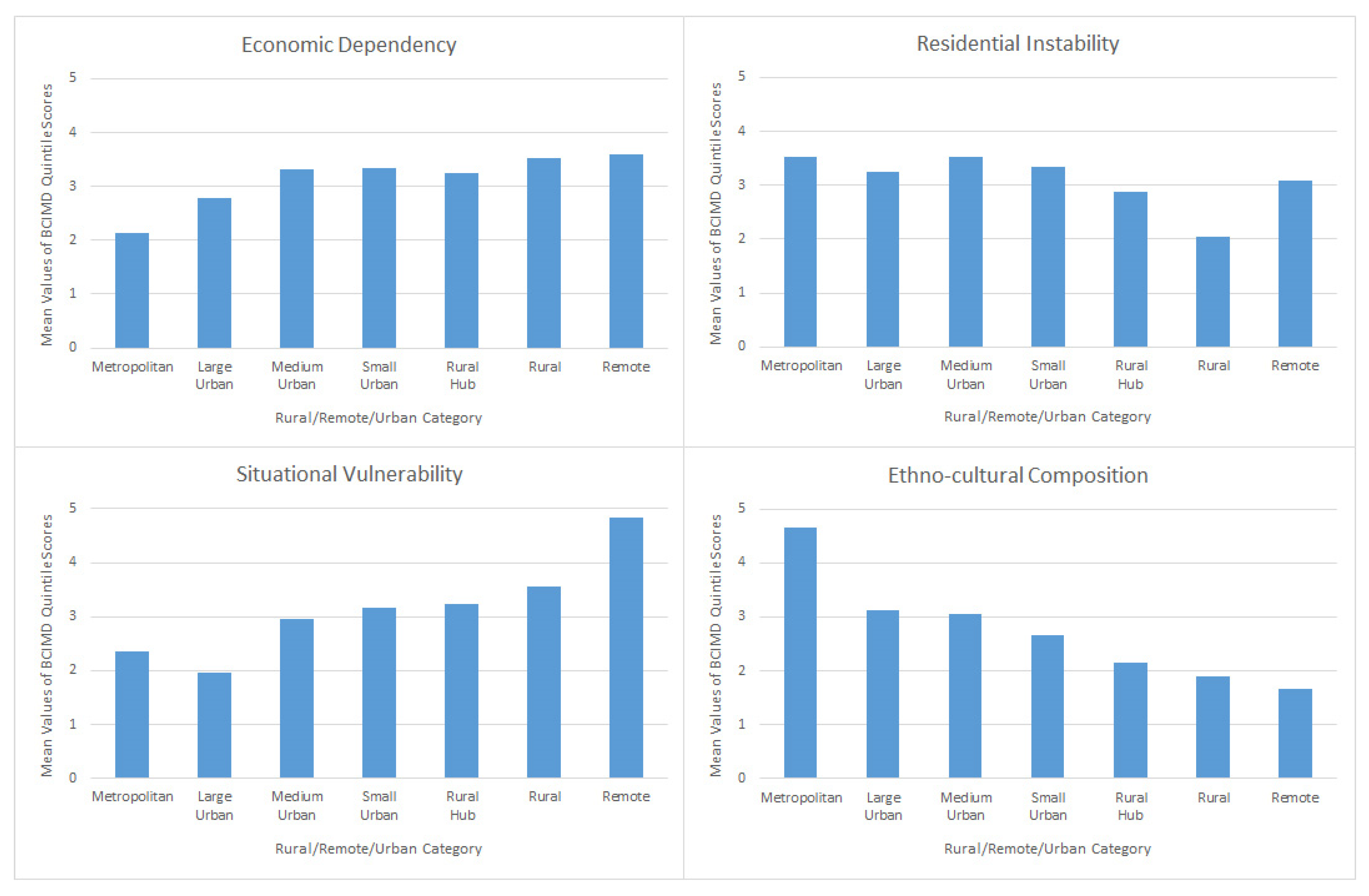
| Dimension of Deprivation | Ethno-Cultural Composition | Situational Vulnerability | Economic Dependency | Residential Instability |
|---|---|---|---|---|
| Concept captured at a British Columbia-level | Diverse community composition of immigrant populations | Socio-demographic conditions in housing and education, and other relevant demographic characteristics | Participation in the labor force, or a dependence on other income sources besides employment income | Transient nature of neighborhood inhabitants, considering housing and familial factors |
| Indicators included | Proportion of population who self-identify as visible minority, the proportion of population that is foreign-born, the proportion of population with no knowledge of either official language (linguistic isolation), and the proportion of population who are recent immigrants (arrived in five years prior to Census) | Proportion of population that identifies as Aboriginal, the proportion of population aged 25–64 without a high school diploma, the proportion of dwellings needing major repairs, the proportion of population that is low-income, and the proportion of single-parent families. | Proportion of population participating in labor force (aged 15 and older) 1, the proportion of population aged 65 and older, the ratio of employment to population 1, and the dependency ratio (population aged 0–14 and aged 65 and older divided by population aged 15–64) | Proportion of dwellings that are apartment buildings, the proportion of persons living alone, the proportion of dwellings that are owned 1, and the proportion of the population who moved within the past five years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Relova, S.; Joffres, Y.; Rasali, D.; Zhang, L.R.; McKee, G.; Janjua, N. British Columbia’s Index of Multiple Deprivation for Community Health Service Areas. Data 2022, 7, 24. https://doi.org/10.3390/data7020024
Relova S, Joffres Y, Rasali D, Zhang LR, McKee G, Janjua N. British Columbia’s Index of Multiple Deprivation for Community Health Service Areas. Data. 2022; 7(2):24. https://doi.org/10.3390/data7020024
Chicago/Turabian StyleRelova, Sharon, Yayuk Joffres, Drona Rasali, Li Rita Zhang, Geoffrey McKee, and Naveed Janjua. 2022. "British Columbia’s Index of Multiple Deprivation for Community Health Service Areas" Data 7, no. 2: 24. https://doi.org/10.3390/data7020024
APA StyleRelova, S., Joffres, Y., Rasali, D., Zhang, L. R., McKee, G., & Janjua, N. (2022). British Columbia’s Index of Multiple Deprivation for Community Health Service Areas. Data, 7(2), 24. https://doi.org/10.3390/data7020024