
Virtual Group Exercises and Psychological Status among Community-Dwelling Older Adults during the COVID-19 Pandemic—A Feasibility Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Population
2.2. Recruitment Procedure
2.3. Measures
2.3.1. Mental Health
2.3.2. Physical Activity
2.3.3. Social Participation
2.3.4. Social Network
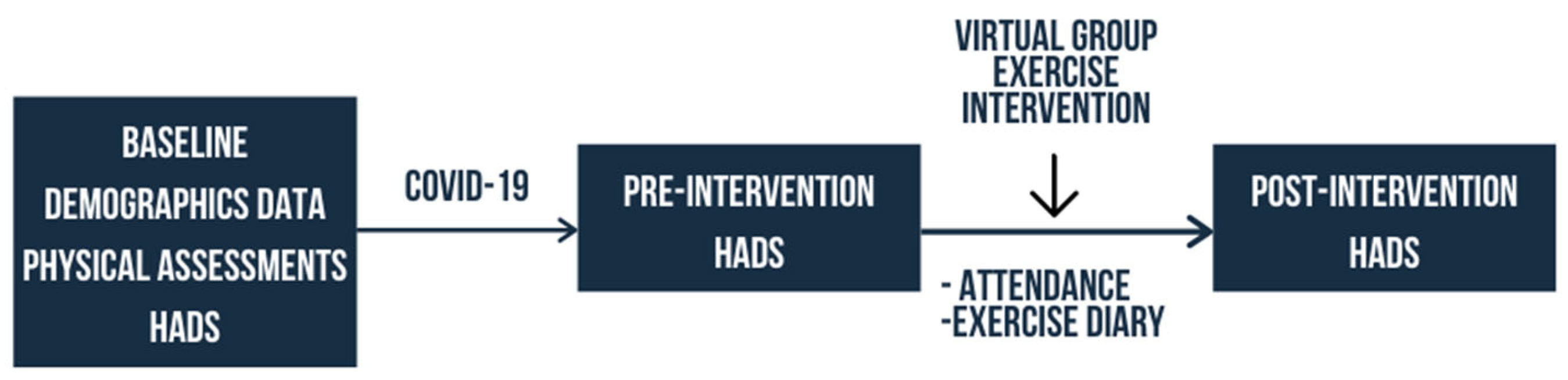
2.4. Intervention
Adherence
2.5. Data Analysis
3. Results
3.1. Recruitment
3.2. Groups Comparison
3.3. Adherence
3.3.1. Attendance
3.3.2. Exercise Diary
3.3.3. Technical Issues
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social Relationships and Mortality Risk: A Meta-analytic Review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 11 March 2021).
- Delmastro, M.; Zamariola, G. The Psychological Effect of COVID-19 and Lockdown on the Population: Evidence from Italy. re-searchsquare.com. 2020. [Google Scholar] [CrossRef]
- Pandey, D.; Bansal, S.; Goyal, S.; Garg, A.; Sethi, N.; Pothiyill, D.I.; Sreelakshmi, E.S.; Sayyad, M.G.; Sethi, R. Psychological impact of mass quarantine on population during pandemics—The COVID-19 Lock-Down (COLD) study. PLoS ONE 2020, 15, e0240501. [Google Scholar] [CrossRef]
- Sugaya, N.; Yamamoto, T.; Suzuki, N.; Uchiumi, C. A real-time survey on the psychological impact of mild lockdown for COVID-19 in the Japanese population. Sci. Data 2020, 7, 1–6. [Google Scholar] [CrossRef]
- García-Portilla, P.; de la Fuente Tomás, L.; Bobes-Bascarán, T.; Jiménez Treviño, L.; Zurrón Madera, P.; Suárez Álvarez, M.; Menéndez Miranda, I.; García Álvarez, L.; Sáiz Martínez, P.A.; Bobes, J. Are older adults also at higher psychological risk from COVID-19? Aging Mental Health 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rivan, N.M.; Yahya, H.; Shahar, S.; Singh, D.A.; Ibrahim, N.; Ludin, A.M.; Sakian, N.M.; Mahadzir, H.; Subramaniam, P.; Kamaruddin, M. The Impact of Poor Nutrient Intakes and Food Insecurity on the Psychological Distress among Community-Dwelling Middle-Aged and Older Adults during the COVID-19 Pandemic. Nutrure 2021, 13, 353. [Google Scholar] [CrossRef]
- Suzuki, Y.; Maeda, N.; Hirado, D.; Shirakawa, T.; Urabe, Y. Physical Activity Changes and Its Risk Factors among Community-Dwelling Japanese Older Adults during the COVID-19 Epidemic: Associations with Subjective Well-Being and Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 6591. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Bennell, K.; White, D.K.; Wei, J.; Wu, Z.; He, H.; Liu, S.; Luo, X.; Hu, S.; et al. Physical Distancing Measures and Walking Activity in Middle-aged and Older Residents in Changsha, China, During the COVID-19 Epidemic Period: Longitudinal Observational Study. J. Med Internet Res. 2020, 22, e21632. [Google Scholar] [CrossRef] [PubMed]
- AbdelBasset, W.K. Stay Home: Role of Physical Exercise Training in Elderly Individuals’ Ability to Face the COVID-19 Infection. J. Immunol. Res. 2020, 2020, 1–5. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.Y.; Ibrahim, R.; Hamid, T.A.; Mansor, E.I. Measuring Expectation for an Affordance Gap on a Smartphone User Interface and its Usage Among Older Adults. Hum. Technol. 2020, 16, 6–34. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Snaith, R.P. The Hospital Anxiety And Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- Chu, A.H.Y.; Moy, F.M. Reliability and Validity of the Malay International Physical Activity Questionnaire (IPAQ-M)Among a Malay Population in Malaysia. Asia Pac. J. Public Health 2012, 27, NP2381–NP2389. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Sepp, H.; Brage, S.; Becker, W.; Jakes, R.; Hennings, M.; Wareham, N.J. Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults. Public Health Nutr. 2006, 9, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, R.; Jordan, J.L.; Muller, S.; Nicholls, E.; Healey, E.L.; Van Der Windt, D.A. Measures of social function and participation in musculoskeletal populations: Impact on Participation and Autonomy (IPA), Keele Assessment of Participation (KAP), Participation Measure for Post-Acute Care (PM-PAC), Participation Objective, Participation S. Arthritis Rheum. 2011, 63, S325–S336. [Google Scholar] [CrossRef]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; Kruse, W.V.R.; Beck, J.C.; Stuck, A.E. Performance of an Abbreviated Version of the Lubben Social Network Scale Among Three European Community-Dwelling Older Adult Populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef] [Green Version]
- Meng, H.; Xu, Y.; Dai, J.; Zhang, Y.; Liu, B.; Yang, H. Analyze the psychological impact of COVID-19 among the elderly population in China and make corresponding suggestions. Psychiatry Res. 2020, 289, 112983. [Google Scholar] [CrossRef]
- Rababa, M.; Hayajneh, A.A.; Bani-Iss, W. Association of Death Anxiety with Spiritual Well-Being and Religious Coping in Older Adults During the COVID-19 Pandemic. J. Relig. Health 2021, 60, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Robb, C.E.; De Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of Social Isolation with Anxiety and Depression During the Early COVID-19 Pandemic: A Survey of Older Adults in London, UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef]
- Arigo, D.; Pagoto, S.; Carter-Harris, L.; E Lillie, S.; Nebeker, C. Using social media for health research: Methodological and ethical considerations for recruitment and intervention delivery. Digit. Health 2018, 4, 205520761877175. [Google Scholar] [CrossRef] [Green Version]
- Iribarren, S.J.; Ghazzawi, A.; Sheinfil, A.Z.; Frasca, T.; Brown, W.; López-Ríos, J.; Rael, C.T.; Balán, I.C.; Crespo, R.; Dolezal, C.; et al. Mixed-Method Evaluation of Social Media-Based Tools and Traditional Strategies to Recruit High-Risk and Hard-to-Reach Populations into an HIV Prevention Intervention Study. AIDS Behav. 2017, 22, 347–357. [Google Scholar] [CrossRef]
- Topolovec-Vranic, J.; Natarajan, K. The Use of Social Media in Recruitment for Medical Research Studies: A Scoping Review. J. Med Internet Res. 2016, 18, e286. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Patel, P.M.; O’Neal, J.L.; Heinrich, B.S. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: an intervention study. BMC Public Health 2014, 14, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Pfaff, J.J.; Alfonso, H.; Newton, R.U.; Sim, M.G.; Flicker, L.; Almeida, O.P. ACTIVEDEP: a randomised, controlled trial of a home-based exercise intervention to alleviate depression in middle-aged and older adults. Br. J. Sports Med. 2013, 48, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Schoene, D.; Valenzuela, T.; Toson, B.; Delbaere, K.; Severino, C.; Garcia, J.F.; Davies, T.A.; Russell, F.; Smith, S.T.; Lord, S.R. Interactive Cognitive-Motor Step Training Improves Cognitive Risk Factors of Falling in Older Adults – A Randomized Controlled Trial. PLoS ONE 2015, 10, e0145161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, H.; Makizako, H.; Doi, T. Effects of Combined Physical and Cognitive Exercises on Cognition and Mobility in Patients With Mild Cognitive Impairment: A Randomized Clinical Trial Prevalence of frailty in Japan: A systematic review and me-ta-analysis View project. J. Am. Med. Directors Assoc. 2017. [Google Scholar] [CrossRef]
- Baez, M.; Far, I.K.; Ibarra, F.; Ferron, M.; Didino, D.; Casati, F. Effects of online group exercises for older adults on physical, psychological and social wellbeing: a randomized pilot trial. PeerJ 2017, 5, e3150. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; E Miyawaki, C. What Types of Physical Function Predict Program Adherence in Older Adults? Rehabilitation Nurs. 2020, 45, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Vallerand, J.R.; Rhodes, R.E.; Walker, G.J.; Courneya, K.S. Feasibility and preliminary efficacy of an exercise telephone counseling intervention for hematologic cancer survivors: a phase II randomized controlled trial. J. Cancer Surviv. 2018, 12, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Farrance, C.; Tsofliou, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banbury, A.; Chamberlain, D.; Nancarrow, S.; Dart, J.; Gray, L.; Parkinson, L. Can videoconferencing affect older people’s engagement and perception of their social support in long-term conditions management: a social network analysis from the Telehealth Literacy Project. Health Soc. Care Community 2016, 25, 938–950. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.P.; Ho, Y.Y.; Chin, A.-V.; Saedon, N.; Abidin, I.Z.; Chee, K.H.; Khor, H.M.; Goh, C.H.; Hairi, N.N.; Othman, S.; et al. Ethnic differences in lifetime cumulative incidence of syncope: the Malaysian elders longitudinal research (MELoR) study. Clin. Auton. Res. 2019, 30, 121–128. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± Standard Deviation | p-Value | ||||
|---|---|---|---|---|---|---|
| Group A (n = 21) (14 or >14 sessions) | Group B (n = 22) (<14 sessions) | |||||
| Age (years) | 65.1 ± 4.81 | 61.8 ± 5.15 | Df = 41 t = 2.16 p = 0.037 | |||
| Years of education | 15.79 ± 2.42 | 14.48 ± 2.92 | Df = 38 t = 1.54 p = 0.132 | |||
| Attendance to online sessions | 12.43 ± 2.16 | 4.36 ± 4.44 | Df = 41 t = 11.4 p < 0.001 | |||
| Variable | Sub-variable | Group A | Group B | |||
| n | % | n | % | |||
| Gender | Male Female | 4 17 | 19 81 | 6 15 | 28.6 71.4 | p = 0.717 |
| Ethnicity | Malay Chinese Indian Others | 3 17 0 1 | 14.3 81 0 4.8 | 2 15 5 0 | 9.1 68.2 22.7 0 | p = 0.542 |
| Marital status | Single Married Widowed Partner Divorced | 1 19 1 0 | 4.8 90.5 4.8 0 | 3 15 2 2 | 13.6 68.2 9.1 9.1 | p = 0.155 |
| Dwelling | Independent Spouse Children Parent | 0 17 3 1 | 0 81 14.3 4.8 | 7 11 4 0 | 31.8 50 18.2 0 | p = 0.070 |
| Health condition (self-rated) | Poor Fair Good Very Good | 0 2 14 5 | 0 9.5 66.7 23.8 | 2 6 12 2 | 9.1 27.3 54.5 9.1 | p = 0.085 |
| Health compared to others | Poor Fair Good Very Good Excellent | 0 0 11 9 1 | 0 0 52.4 42.9 4.8 | 1 9 7 4 1 | 4.5 40.9 31.8 18.2 4.5 | p = 0.002 |
| Variables | All | Group A (n = 21) (14 or > 14 sessions) | Group B (n = 22) (<14 sessions) |
|---|---|---|---|
| Number of returned diaries | 26 | 18 | 8 |
| Total exercises sessions attended | 666 | 464 | 202 |
| Total exercise attended per person | 25.6 | 25.8 | 25.3 |
| Total virtual group exercises | 441 | 345 | 96 |
| Total virtual group exercises per person | 10.3 | 19.2 | 12 |
| Total individual home exercises | 225 | 119 | 106 |
| Total individual home exercises per person | 8.7 | 6.6 | 13.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, A.; Chong, M.C.; Khoo, S.; Wong, L.P.; Chung, I.; Tan, M.P. Virtual Group Exercises and Psychological Status among Community-Dwelling Older Adults during the COVID-19 Pandemic—A Feasibility Study. Geriatrics 2021, 6, 31. https://doi.org/10.3390/geriatrics6010031
Ibrahim A, Chong MC, Khoo S, Wong LP, Chung I, Tan MP. Virtual Group Exercises and Psychological Status among Community-Dwelling Older Adults during the COVID-19 Pandemic—A Feasibility Study. Geriatrics. 2021; 6(1):31. https://doi.org/10.3390/geriatrics6010031
Chicago/Turabian StyleIbrahim, Amirah, Mei Chan Chong, Selina Khoo, Li Ping Wong, Ivy Chung, and Maw Pin Tan. 2021. "Virtual Group Exercises and Psychological Status among Community-Dwelling Older Adults during the COVID-19 Pandemic—A Feasibility Study" Geriatrics 6, no. 1: 31. https://doi.org/10.3390/geriatrics6010031
APA StyleIbrahim, A., Chong, M. C., Khoo, S., Wong, L. P., Chung, I., & Tan, M. P. (2021). Virtual Group Exercises and Psychological Status among Community-Dwelling Older Adults during the COVID-19 Pandemic—A Feasibility Study. Geriatrics, 6(1), 31. https://doi.org/10.3390/geriatrics6010031