

Predictors of Health Satisfaction in Spanish Physically Active Older Adults: A Cross-Sectional Observational Study
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Variables and Measured Instruments
2.3.1. Physical Activity
2.3.2. Quality of Life
2.3.3. Sociodemographic Variables
2.4. Analysis of Data
3. Results
4. Discussion
4.1. Main Findings of This Study
4.2. How Can the Results Be Interpreted in the Perspective of Previous Studies?
4.3. Limitations
4.4. Contributions and Practical Implications
4.5. Future Line of Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spijker, J. Perspectivas alternativas sobre la medición del envejecimiento en España. Doc. Anal. Geogr. 2021, 67, 323–347. [Google Scholar]
- World Health Organization. Envejecimiento y salud 2021. Available online: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health (accessed on 21 February 2022).
- Fernández-Ballesteros, R. Un nuevo paradigma en el estudio del envejecimiento. In Envejecimiento activo. Contribuciones de la Psicología; Fernández-Ballesteros, R., Ed.; Psicología Pirámide: Madrid, Spain, 2009; Volume 13, pp. 214–216. [Google Scholar]
- Parra-Rizo, M.A. Diferencias de género en la percepción de salud en personas mayores de 60 años físicamente activas. Revista Española de Comunicación en Salud 2017, 8, 219–227. [Google Scholar] [CrossRef]
- Parra-Rizo, M.A. La alta práctica de actividad física es determinante en el mayor consumo de ocio por parte de mujeres y hombres mayores de 60 años: Envejecimiento activo y ocio. Anuario de Psicología 2020, 50, 127–134. [Google Scholar] [CrossRef]
- Parra-Rizo, M.A.; Vásquez-Gómez, J.; Álvarez, C.; Diaz-Martínez, X.; Troncoso, C.; Leiva-Ordóñez, A.M.; Zapata-Lamana, R.; Cigarroa, I. Predictors of the level of physical activity in physically active older people. Behav. Sci. 2022, 12, 331. [Google Scholar] [CrossRef]
- Duque-Fernández, L.M.; Ornelas-Contreras, M.; Benavides-Pando, E.V. Actividad física y su relación con el envejecimiento y la capacidad funcional: Una revisión de la literatura de investigación. Psicología y Salud 2020, 30, 45–57. Available online: https://link.gale.com/apps/doc/A628052332/IFME?u=anon~2611e09&sid=googleScholar&xid=b2c48aec (accessed on 21 February 2022). [CrossRef]
- Parra-Rizo, M.A. Componentes de influencia más valorados en la calidad de vida por las personas mayores de 60 años físicamente activas. Eur. J. Investig. Health Psychol. Educ. 2017, 7, 135–144. [Google Scholar] [CrossRef] [Green Version]
- Solórzano, R.W.V.; Vargas, A.R.R. La actividad física para el desarrollo la calidad de vida de adultos mayores con diabetes TIPO II. RECIMUNDO: Revista Científica de la Investigación y el Conocimiento 2019, 3, 362–386. [Google Scholar] [CrossRef]
- Schroeder, E.C.; Welk, G.J.; Franke, W.D.; Lee, D.C. Associations of Health Club Membership with Physical Activity and Cardiovascular Health. PLoS ONE 2017, 12, e0170471. [Google Scholar] [CrossRef]
- Balchin, R.; Linde, J.; Blackhurst, D.; Raugh, H.L.; Schönbächler, G. Sweating away depression? The impact of intensive exercise on depression. J. Affect Disord. Rep. 2016, 200, 218–221. [Google Scholar] [CrossRef]
- Guillén, L.; Bueno, E.; Gutiérrez, M.; Guerra, J. Programa de actividad física y su incidencia en la depresión y bienestar subjetivo de adultos mayores. Retos 2018, 33, 14–19. [Google Scholar]
- Phillips, S.M.; Wójcicki, T.R.; McAuley, E. Physical activity and quality of life in older adults: An 18-month panel analysis. Qual. Life Res. 2013, 22, 1647–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almaguer, D.J.; Méndez, P.R.C.; Fonseca, R.S.S.; Almaguer, D.J.; Ramírez, G.H. Percepción de la calidad de vida en pacientes adultos mayores con diabetes mellitus tipo II. Medimay 2019, 26, 54–62. [Google Scholar]
- Mella, R.; González, L.; D’Appolonio, J.; Maldonado, I.; Fuenzalida, A.; Díaz, A.; Díaz, A. Factores Asociados al Bienestar Subjetivo en el Adulto Mayor. Psykhe 2004, 13, 79–89. [Google Scholar] [CrossRef] [Green Version]
- Herrera, E.; Pablos, A.; Chiva-Bartoll, O.; Pablos, C. Efectos de la Actividad Física en la Salud Percibida y Condición Física de los Adultos Mayores. J. Sport Health Res. 2017, 9, 27–40. [Google Scholar]
- Durán, D.M.; ValDerrama, L.J.O.; Rodríguez, A.F.U.; Linde, J.M.U. Integración social y habilidades funcionales en adultos mayores. Universitas Psychologica 2008, 7, 263–270. [Google Scholar]
- Fernández-Mayoralas, G.; Rojo-Pérez, F.; Martínez-Martín, P.; Prieto-Flores, M.E.; Rodríguez-Blázquez, C.; Martín-García, S.; Rojo-Abuín, J.M.; Forjaz, M.J. Active ageing and quality of life: Factors associated with participation in leisure activities among institutionalized older adults, with and without dementia. Aging Ment. Health 2015, 19, 1031–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, C.; Chang, Y.; Jeong, B.; Kang, S.; Ryu, J.; Kim, G. Effect of knee sleeves on coordination of lower-limb segments in healthy adults during level walking and one-leg hopping. PeerJ 2017, 5, e3340. [Google Scholar] [CrossRef] [Green Version]
- Petronila, L.; Aragón, S.; Calvo, B. Caídas en ancianos institucionalizados: Valoración del riesgo, factores relacionados y descripción. Gerokomos 2017, 28, 2–8. [Google Scholar]
- Béland, F.; Zunzunegui, M.V. La utilización de los servicios médicos y sociales por las personas mayores de Leganés. Revista multidisciplinar de gerontología 1995, 5, 309–324. [Google Scholar]
- Tijeras, E.; García, L.G.; Zegarra, S.P. Relación entre el apoyo social, la satisfacción de las necesidades psicológicas básicas y el bienestar en adultos mayores. Eur. J. Health Res. 2020, 6, 133–143. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Jean-Pierre, M.; Rolland, Y.; Schneider, S.M.; Topinková, E. Sarcopenia: European consensus on definition and diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinetti, M.E. Making prevention recommendations relevant for an aging population. Ann. Intern. Med. 2010, 153, 843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). IPAQ. International Physical Activity Questionnaire (Versión 2.0. Español). 2012. Available online: http://www.who.int/chp/steps/instrument/es/index/html (accessed on 23 September 2022).
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, 498–516. [Google Scholar] [CrossRef] [Green Version]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of high-intensity interval training (HIT) and continuous endurance training for VO 2max improvements: A systematic review and meta-analysis of controlled trials. Sport Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.D.; McHugh, G.A.; Quicke, J.G.; Dziedzic, K.S.; Healey, E.L. Comparison of realibility, construct validity and responsiveness of the IPAQ-SF and PASE in adults with osteoarthritis. Musculoskeletal Care 2021, 19, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ballesteros, R.; Zamarrón, M.D. Cubrecavi. Cuestionario breve sobre la calidad de vida; TEA Ediciones: Madrid, Spain, 2007. [Google Scholar]
- Luque-Reca, O.; Pulido-Martos, M.; López-Zafra, E.; Augusto-Landa, J.M. The importance of emotional intelligence and cognitive style in institutionalized older adults´quality of life. J. Gen. Psychol. 2018, 145, 120–133. [Google Scholar] [CrossRef]
- Cruz-Sánchez, E.; Moreno-Contreras, M.I.; Pino-Ortega, J.; Martínez-Santos, R. Actividad física durante el tiempo libre y su relación con algunos indicadores de salud mental en España. Salud Ment. 2011, 34, 45–52. [Google Scholar]
- Fematt, F. Definición y objetivos de la geriatría. El Residente 2010, 5, 49–54. [Google Scholar]
- Imayama, I.; Alfano, C.M.; Mason, C.E.; Wang, C.; Xiao, L.; Duggan, C.; Campbell, K.L.; Foster-Schubert, K.E.; McTiernan, A. Exercise Adherence, Cardiopulmonary Fitness, and Anthropometric Changes Improve Exercise Self-Efficacy and Health-Related Quality of Life. J. Phys. Act. Health 2013, 10, 676–689. [Google Scholar] [CrossRef] [Green Version]
- Aoyagi, Y.; Park, H.; Park, S.; Shephard, R.J. Habitual physical activity and health related quality of life in older adults: Interactions between the amount and intensity of activity (the Nakanojo Study). Qual. Life Res. 2013, 19, 333–338. [Google Scholar] [CrossRef]
- Garatachea, N.; Molinero, O.; Martínez-García, R.; Jiménez-Jiménez, R.; González-Gallego, J.; Márquez, S. Feelings of well being in elderly people: Relationship to physical activity and physical function. Arch. Gerontol. Geriatr. 2009, 48, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Limón, M.; del Carmen, M. Envejecimiento activo y mejora de la calidad de vida en adultos mayores Active aging and improvement the quality of life in older adults. Rev. Psicol. Educ. 2011, 6, 225–238. [Google Scholar]
- Zapata-Lamana, R.; Poblete-Valderrama, F.; Ledezma-Dames, A.; Pavón-León, P.; Leiva, A.M.; Fuentes-Álvarez, M.T.; Cigarroa, I.; Parra-Rizo, M.A. Health, functional ability, and environmental quality as predictors of life satisfaction in physically active older adults. Soc. Sci. 2022, 11, 265. [Google Scholar] [CrossRef]
- Lee, C.; Russell, A. Effects of physical activity on emotional well-being among older Australian women: Cross-sectional and longitudinal analyses. J. Psychosom. Res. 2003, 54, 155–160. [Google Scholar] [CrossRef]
- Valdez-Mora, I.; Alejo-Torres, M.; Meza-Calleja, A.; Ortega-Medellín, M. Aspectos subjetivos de la calidad de vida en personas mayores. Rev. Educ. Des. 2013, 27, 15–24. [Google Scholar]
- Yang, G.; Niu, K.; Fujita, K.; Hozawa, A.; Ohmori-Matsuda, K.; Kuriyama, S.; Nakaya, N.; Ebihara, S.; Okazaki, T.; Guo, H. Impact of physical activity and performance on medical care costs among the Japanese elderly. Geriatr. Gerontol. Int. 2011, 11, 157–165. [Google Scholar] [CrossRef]
- Barchielli, B.; Cricenti, C.; Gallè, F.; Sabella, E.A.; Liguori, F.; Da Molin, G.; Liguori, G.; Battista, G.; Giannini, A.M.; Ferracuti, S.; et al. Climate changes, natural resources depletion, COVID-19 pandemic, and Russian-Ukrainian War: What is the impact on habits change and mental health? Int. J. Environ. Res. Public Health 2022, 19, 11929. [Google Scholar] [CrossRef]
- Lu, Y.; Niti, M.; Yap, K.B.; Tan, C.T.Y.; Zin, M.S.; Feng, L.; Boon, T.; Gribson, C.; Khoo, S.A.; Chan, S.M.; et al. Assessment of Sarcopenia Among Community-Dwelling At-Risk Frail Adults Aged 65 Years and Older Who Received Multidomain Lifestyle Interventions: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e1913346. [Google Scholar] [CrossRef] [Green Version]
- Otero, A.; Zunzunegui, M.V.; Rodríguez-Laso, A.; Aguilar, M.D.; Lázaro, P. Volumen y tendencias de la dependencia asociada al envejecimiento en la población española. Rev. Esp. Salud Publica 2004, 78, 201–213. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Satisfaction with Health | ||||||
|---|---|---|---|---|---|---|
| Scale | High | Low | t | p | ||
| n | M (SD) | n | M (SD) | |||
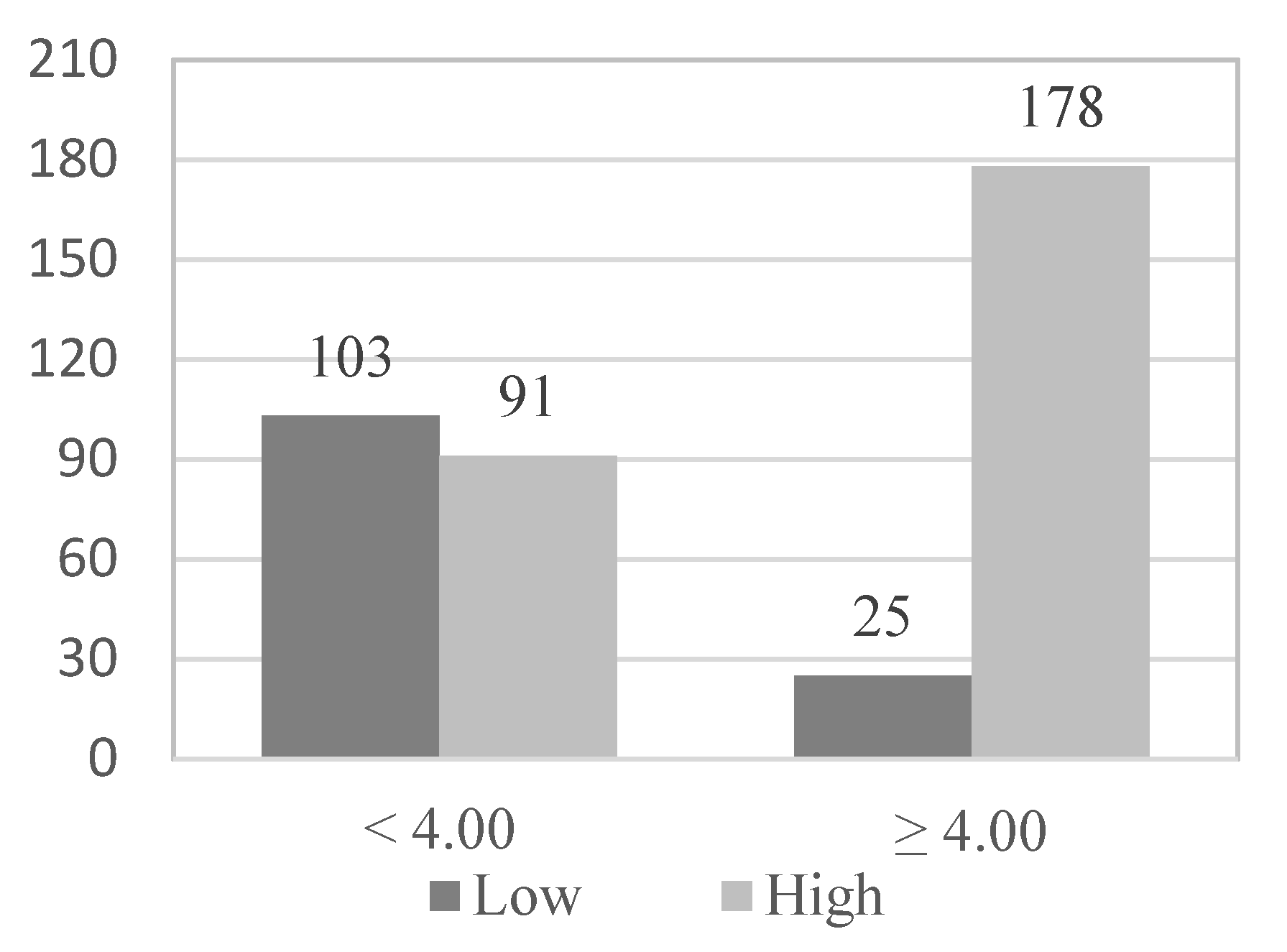
| Functional skills | 269 | 3.80 (0.34) | 128 | 3.45 (0.50) | 7.358 | 0.000 * |
| Satisfaction with Health | ||||||
|---|---|---|---|---|---|---|
| High | Low | Total | ||||
| n | % | n | % | n | % | |
| Gender | ||||||
| Male | 95 | 35.3 | 45 | 35.2 | 140 | 35.3 |
| Female | 174 | 64.7 | 83 | 64.8 | 257 | 64.7 |
| Age | ||||||
| <70 years old | 185 | 68.8 | 83 | 64.8 | 268 | 67.5 |
| ≥70 years old | 84 | 31.2 | 45 | 35.2 | 129 | 32.5 |
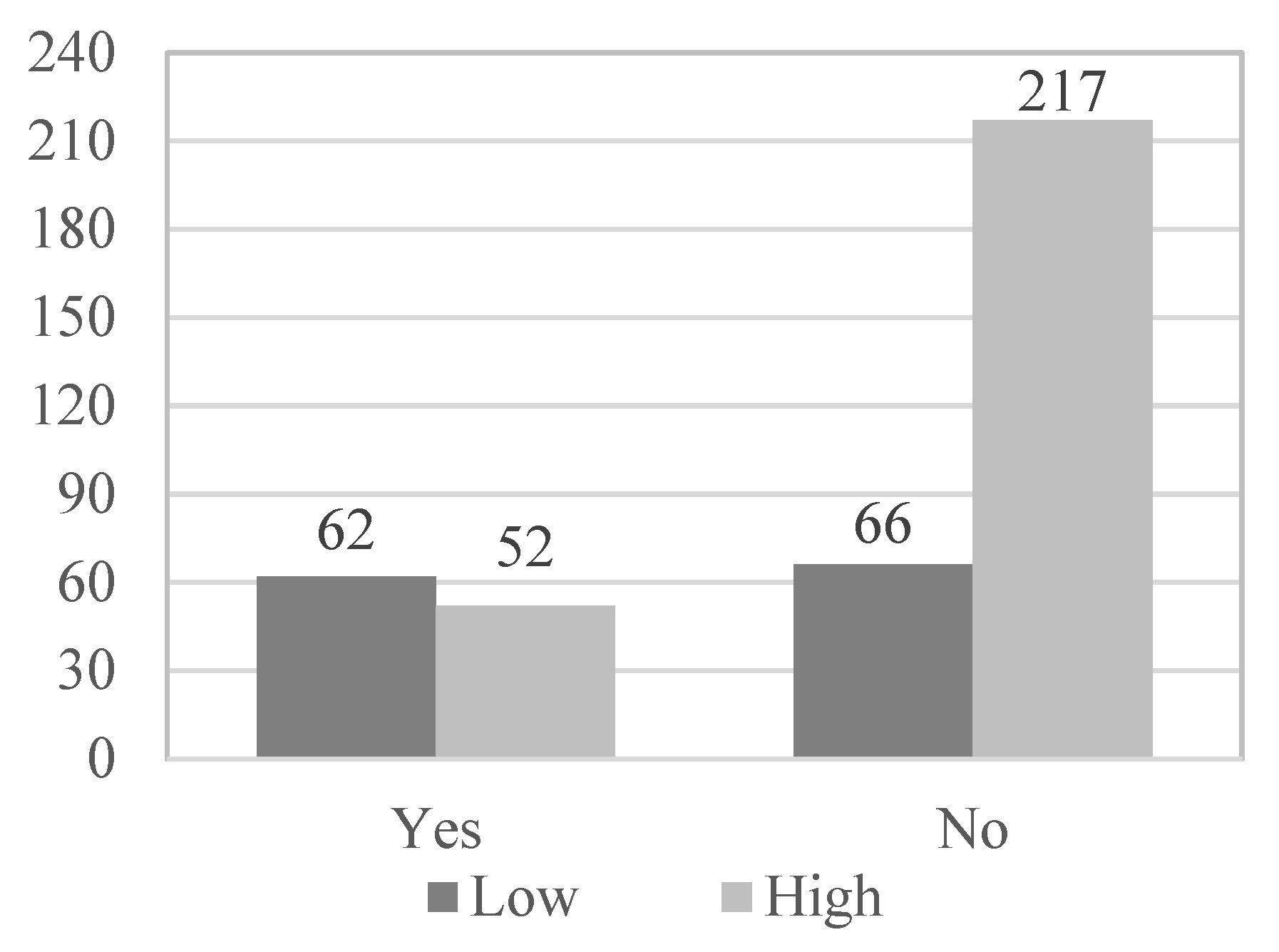
| Physical illnesses | ||||||
| Yes | 52 | 19.3 | 62 | 48.4 | 114 | 28.7 |
| No | 217 | 80.7 | 66 | 51.6 | 283 | 71.3 |
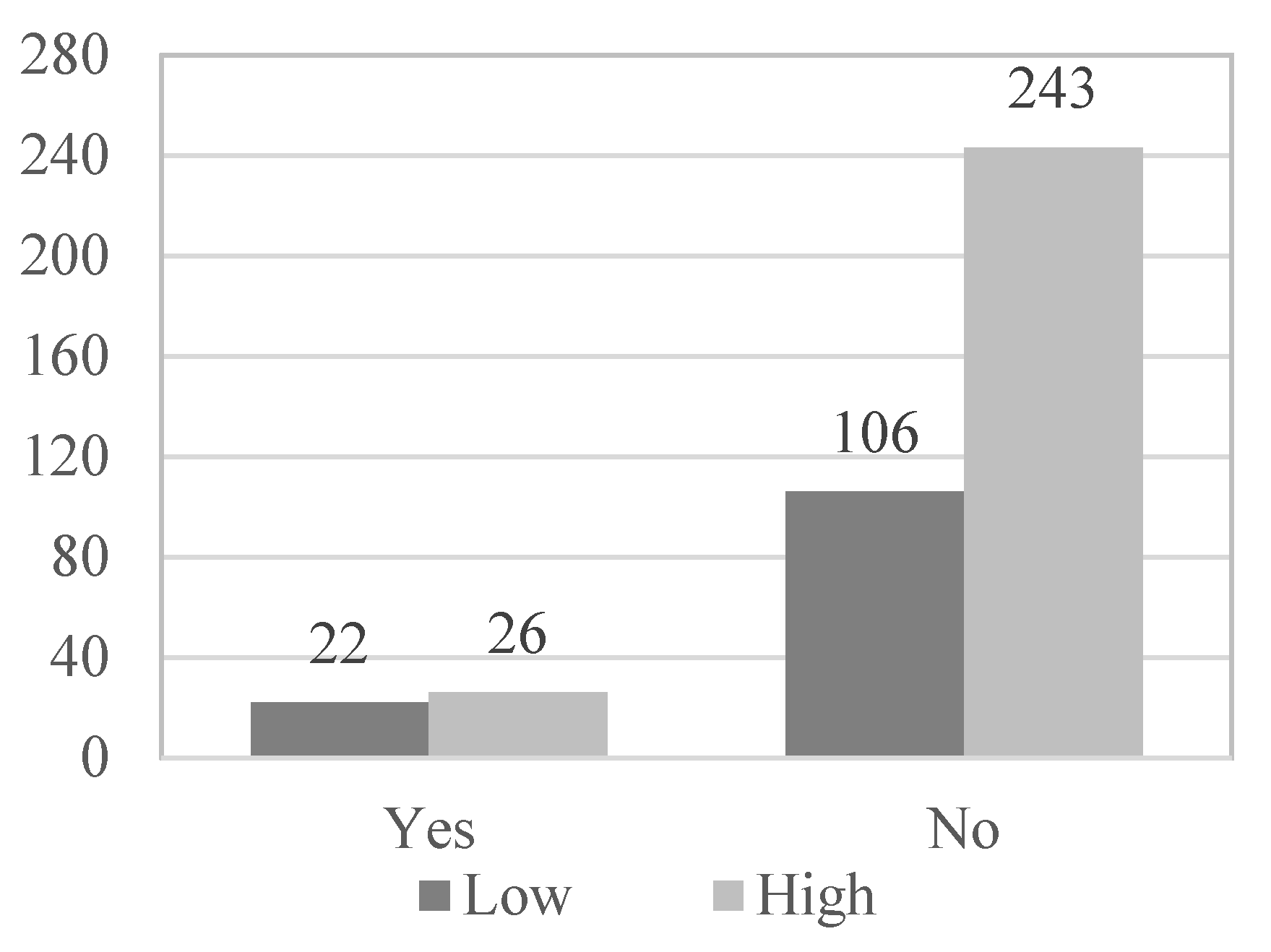
| Psychological problems | ||||||
| Yes | 26 | 9.7 | 22 | 17.2 | 48 | 12.1 |
| No | 243 | 90.3 | 106 | 82.8 | 349 | 87.9 |
| Physical activity | ||||||
| Low | 27 | 10.0 | 22 | 17.2 | 49 | 12.3 |
| Moderate | 103 | 38.3 | 62 | 48.4 | 165 | 41.6 |
| High | 139 | 51.7 | 44 | 34.4 | 183 | 46.1 |
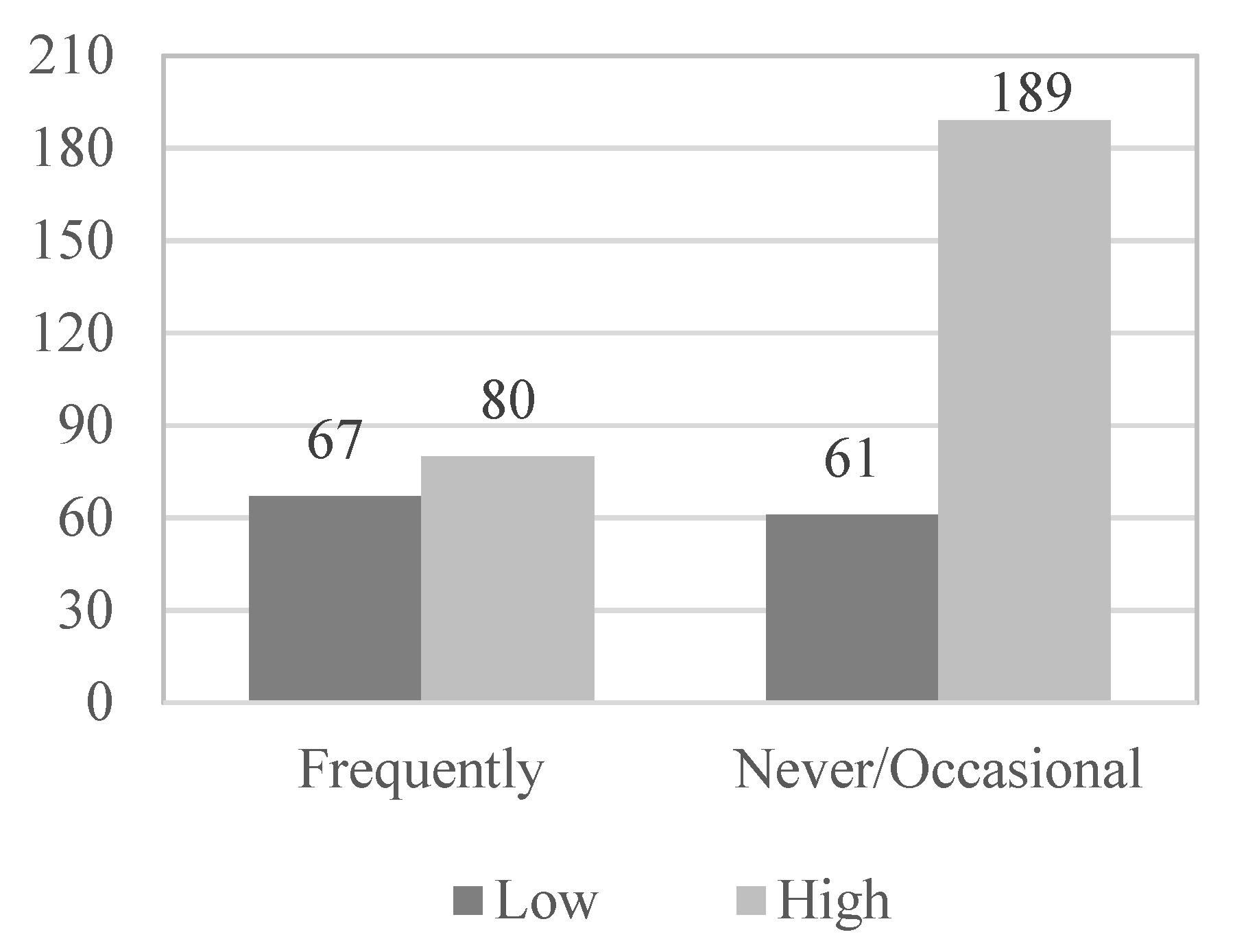
| Use of socio-health services | ||||||
| Never | 17 | 6.3 | 7 | 5.5 | 24 | 6.1 |
| Occasionally | 172 | 63.9 | 54 | 42.2 | 226 | 56.9 |
| Frequently | 80 | 29.8 | 67 | 52.3 | 147 | 37.0 |
| Satisfaction with socio-health services | ||||||
| Wholly dissatisfied | 5 | 1.9 | 7 | 5.5 | 12 | 3.0 |
| Moderately dissatisfied | 52 | 19.3 | 33 | 25.8 | 85 | 21.4 |
| Moderately satisfied | 161 | 59.9 | 50 | 39.1 | 211 | 53.2 |
| Very satisfied | 51 | 18.9 | 38 | 29.6 | 89 | 22.4 |
| B | E.T. | Wald | p | Exp(B) | IC 95 for Exp(B) | |
|---|---|---|---|---|---|---|
| Physical illness | 1.174 | 0.269 | 19.004 | 0.000 * | 3.234 | 1.908–5.481 |
| Psychological problem | 0.723 | 0.368 | 3.861 | 0.049 * | 2.061 | 1.002–4.241 |
| Functional skills | 1.983 | 0.276 | 51.763 | 0.000 * | 7.263 | 4.232–12.466 |
| Use of social and health services | 0.578 | 0.257 | 5.045 | 0.025 * | 1.783 | 1.076–2.952 |
| Level P.A. | 0.380 | 0.262 | 2.112 | 0.146 | 1.463 | 0.876–2.442 |
| Constant | −1.991 | 0.433 | 21.140 | 0.000 * | 0.136 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agustí, A.I.; Guillem-Saiz, J.; González-Moreno, J.; Cantero-García, M.; Cigarroa, I.; Parra-Rizo, M.A. Predictors of Health Satisfaction in Spanish Physically Active Older Adults: A Cross-Sectional Observational Study. Geriatrics 2023, 8, 27. https://doi.org/10.3390/geriatrics8010027
Agustí AI, Guillem-Saiz J, González-Moreno J, Cantero-García M, Cigarroa I, Parra-Rizo MA. Predictors of Health Satisfaction in Spanish Physically Active Older Adults: A Cross-Sectional Observational Study. Geriatrics. 2023; 8(1):27. https://doi.org/10.3390/geriatrics8010027
Chicago/Turabian StyleAgustí, Ana Isabel, Javier Guillem-Saiz, Jesús González-Moreno, María Cantero-García, Igor Cigarroa, and María Antonia Parra-Rizo. 2023. "Predictors of Health Satisfaction in Spanish Physically Active Older Adults: A Cross-Sectional Observational Study" Geriatrics 8, no. 1: 27. https://doi.org/10.3390/geriatrics8010027
APA StyleAgustí, A. I., Guillem-Saiz, J., González-Moreno, J., Cantero-García, M., Cigarroa, I., & Parra-Rizo, M. A. (2023). Predictors of Health Satisfaction in Spanish Physically Active Older Adults: A Cross-Sectional Observational Study. Geriatrics, 8(1), 27. https://doi.org/10.3390/geriatrics8010027