
Can Leucine Supplementation Improve Frailty Index Scores?

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
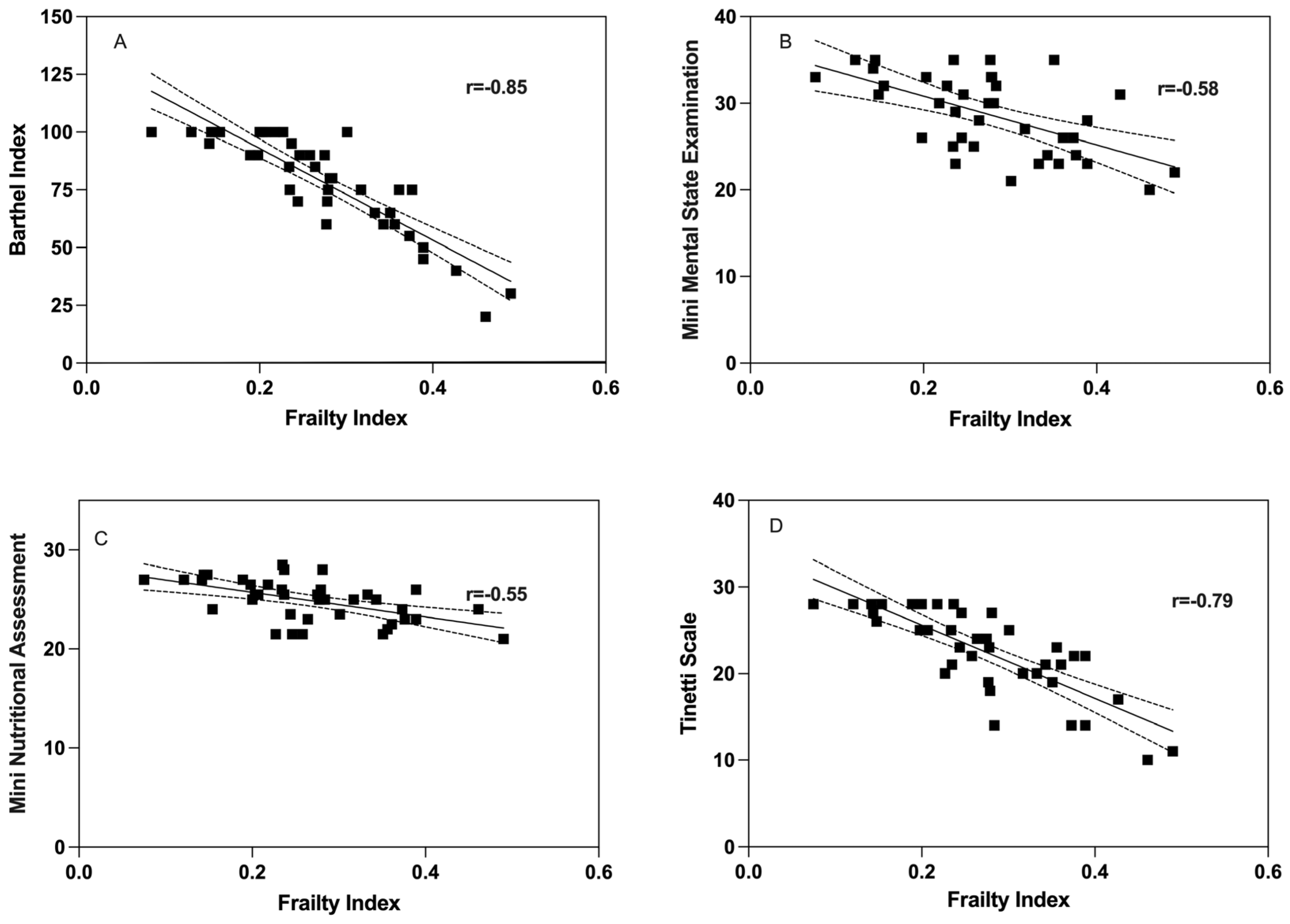
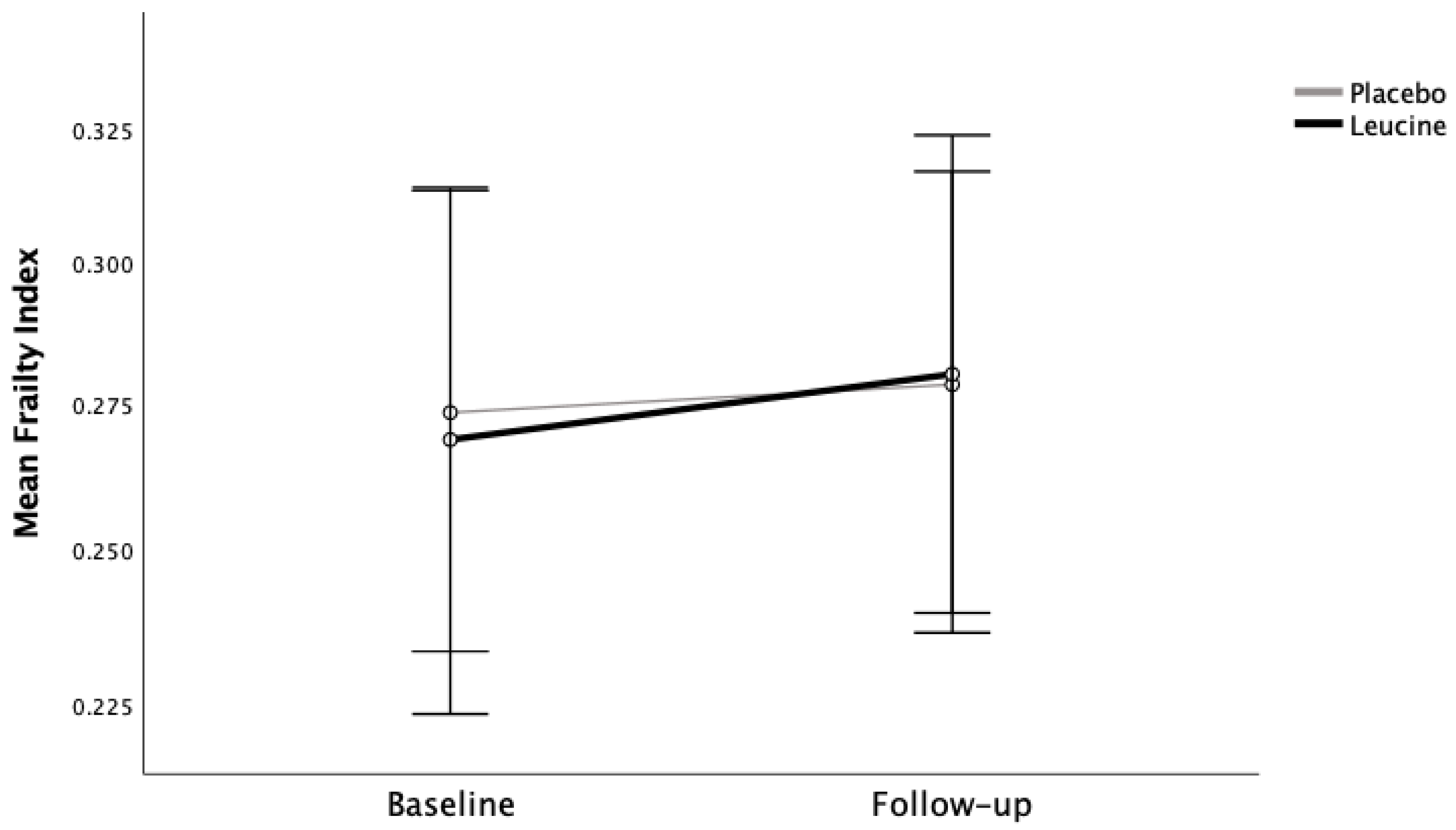
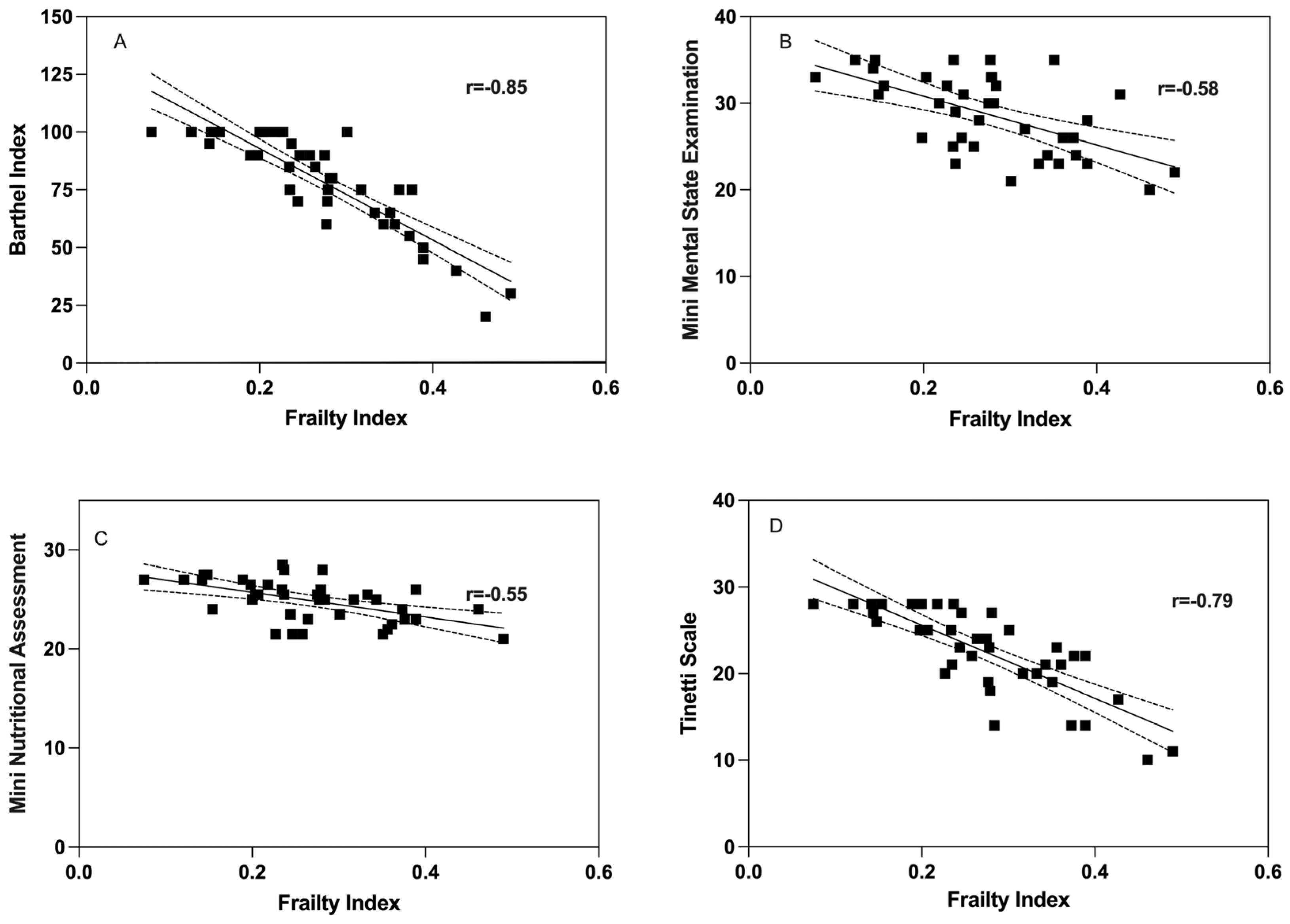
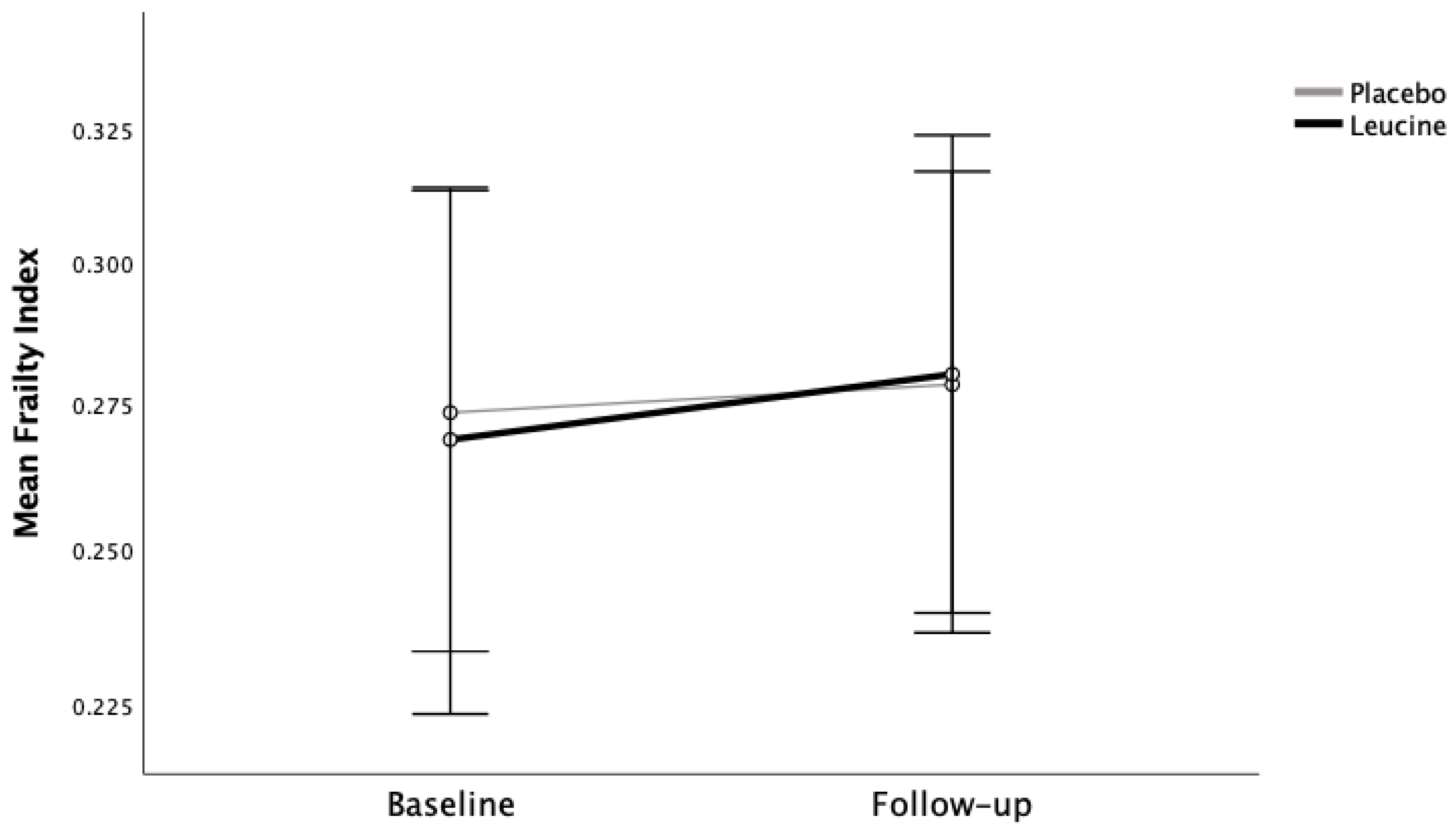
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European Consensus on Definition and Diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Rockwood, K.; Mitnitski, A. Frailty in Relation to the Accumulation of Deficits. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of Deficits as a Proxy Measure of Aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Brivio, P.; Paladini, M.S.; Racagni, G.; Riva, M.A.; Calabrese, F.; Molteni, R. From Healthy Aging to Frailty: In Search of the Underlying Mechanisms. Curr. Med. Chem. 2019, 26, 3685–3701. [Google Scholar] [CrossRef]
- Clegg, A.; Hassan-Smith, Z. Frailty and the Endocrine System. Lancet Diabetes Endocrinol. 2018, 6, 743–752. [Google Scholar] [CrossRef]
- Wilson, D.; Jackson, T.; Sapey, E.; Lord, J.M. Frailty and Sarcopenia: The Potential Role of an Aged Immune System. Ageing Res. Rev. 2017, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Calvani, R.; Marini, F.; Cesari, M.; Tosato, M.; Picca, A.; Anker, S.D.; von Haehling, S.; Miller, R.R.; Bernabei, R.; Landi, F.; et al. Biomarkers for Physical Frailty and Sarcopenia. Aging Clin. Exp. Res. 2017, 29, 29–34. [Google Scholar] [CrossRef]
- Ubaida-Mohien, C.; Lyashkov, A.; Gonzalez-Freire, M.; Tharakan, R.; Shardell, M.; Moaddel, R.; Semba, R.D.; Chia, C.W.; Gorospe, M.; Sen, R.; et al. Discovery Proteomics in Aging Human Skeletal Muscle Finds Change in Spliceosome, Immunity, Proteostasis and Mitochondria. Elife 2019, 8, e49874. [Google Scholar] [CrossRef]
- Dodds, R.; Sayer, A.A. Sarcopenia and Frailty: New Challenges for Clinical Practice. Clin. Med. 2016, 16, 455–458. [Google Scholar] [CrossRef]
- Billot, M.; Calvani, R.; Urtamo, A.; Sánchez-Sánchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, N.; et al. Preserving Mobility in Older Adults with Physical Frailty and Sarcopenia: Opportunities, Challenges, and Recommendations for Physical Activity Interventions. Clin. Interv. Aging 2020, 15, 1675–1690. [Google Scholar] [CrossRef]
- Keevil, V.L.; Romero-Ortuno, R. Ageing Well: A Review of Sarcopenia and Frailty. Proc. Nutr. Soc. 2015, 74, 337–347. [Google Scholar] [CrossRef]
- Mori, H.; Tokuda, Y. Differences and Overlap between Sarcopenia and Physical Frailty in Older Community-Dwelling Japanese. Asia Pac. J. Clin. Nutr. 2018, 28, 157–165. [Google Scholar]
- Cesari, M.; Gambassi, G.; Van Kan, G.A.; Vellas, B. The Frailty Phenotype and the Frailty Index: Different Instruments for Different Purposes. Age Ageing 2014, 43, 10–12. [Google Scholar] [CrossRef]
- Yu, Z.; Ruan, Q.; D’Onofrio, G.; Greco, A.; Yu, Z.; Ruan, Q.; D’Onofrio, G.; Greco, A. From Sarcopenia to Frailty: The Pathophysiological Basis and Potential Target Molecules of Intervention. Frailty Sarcopenia Onset Dev. Clin. Chall. 2017, 3, 55–69. [Google Scholar]
- Shaw, S.C.; Dennison, E.M.; Cooper, C. Epidemiology of Sarcopenia: Determinants Throughout the Lifecourse. Calcif. Tissue Int. 2017, 101, 229–247. [Google Scholar] [CrossRef] [PubMed]
- Picca, A.; Coelho-Junior, H.J.; Calvani, R.; Marzetti, E.; Vetrano, D.L. Biomarkers Shared by Frailty and Sarcopenia in Older Adults: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2022, 73, 101530. [Google Scholar] [CrossRef]
- Davies, B.; García, F.; Ara, I.; Artalejo, F.R.; Rodriguez-Mañas, L.; Walter, S. Relationship Between Sarcopenia and Frailty in the Toledo Study of Healthy Aging: A Population Based Cross-Sectional Study. J. Am. Med. Dir. Assoc. 2018, 19, 282–286. [Google Scholar] [CrossRef]
- Davies, B.; Walter, S.; Rodríguez-Laso, A.; Carnicero Carreño, J.A.; García-García, F.J.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Differential Association of Frailty and Sarcopenia with Mortality and Disability: Insight Supporting Clinical Subtypes of Frailty. J. Am. Med. Dir. Assoc. 2022, 23, 1712–1716.e3. [Google Scholar] [CrossRef]
- Kimball, S.R.; Jefferson, L.S. Signaling Pathways and Molecular Mechanisms through Which Branched-Chain Amino Acids Mediate Translational Control of Protein Synthesis. J. Nutr. 2006, 136, 227–231. [Google Scholar] [CrossRef]
- Le Couteur, D.G.; Solon-Biet, S.M.; Cogger, V.C.; Ribeiro, R.; de Cabo, R.; Raubenheimer, D.; Cooney, G.J.; Simpson, S.J. Branched Chain Amino Acids, Aging and Age-Related Health. Ageing Res. Rev. 2020, 64, 101198. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhou, Q.; Yang, R.; Hu, C.; Huang, Z.; Zheng, C.; Liang, Q.; Gong, R.; Zhu, X.; Gong, H.; et al. Serum Branched-Chain Amino Acids Are Associated with Leukocyte Telomere Length and Frailty Based on Residents from Guangxi Longevity County. Sci. Rep. 2020, 10, 10252. [Google Scholar] [CrossRef] [PubMed]
- Bai, G.H.; Tsai, M.C.; Tsai, H.W.; Chang, C.C.; Hou, W.H. Effects of Branched-Chain Amino Acid-Rich Supplementation on EWGSOP2 Criteria for Sarcopenia in Older Adults: A Systematic Review and Meta-Analysis. Eur. J. Nutr. 2022, 61, 637–651. [Google Scholar] [CrossRef]
- Gielen, E.; Beckwée, D.; Delaere, A.; De Breucker, S.; Vandewoude, M.; Bautmans, I.; Bautmans, I.; Beaudart, C.; Beckwée, D.; Beyer, I.; et al. Nutritional Interventions to Improve Muscle Mass, Muscle Strength, and Physical Performance in Older People: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutr. Rev. 2021, 79, 121–147. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Arnau, F.M.; Fonfría-vivas, R.; Cauli, O. Beneficial Effects of Leucine Supplementation on Criteria for Sarcopenia: A Systematic Review. Nutrients 2019, 11, 2504. [Google Scholar] [CrossRef]
- Martínez-Arnau, F.M.; Fonfría-Vivas, R.; Buigues, C.; Castillo, Y.; Molina, P.; Hoogland, A.J.; van Doesburg, F.; Pruimboom, L.; Fernández-Garrido, J.; Cauli, O. Effects of Leucine Administration in Sarcopenia: A Randomized and Placebo-Controlled Clinical Trial. Nutrients 2020, 12, 932. [Google Scholar] [CrossRef]
- Theou, O.; Jayanama, K.; Fernández-Garrido, J.; Buigues, C.; Pruimboom, L.; Hoogland, A.J.; Navarro-Martínez, R.; Rockwood, K.; Cauli, O. Can a Prebiotic Formulation Reduce Frailty Levels in Older People? J. Frailty Aging 2019, 8, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A Standard Procedure for Creating a Frailty Index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef]
- Vega-Cabello, V.; Caballero, F.F.; Rodriguez-Artalejo, F.; Lopez-Garcia, E.; Struijk, E.A. Leucine Intake and Risk of Impaired Physical Function and Frailty in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 78, 241–249. [Google Scholar] [CrossRef]
- de Vries, N.M.; Staal, J.B.; van Ravensberg, C.D.; Hobbelen, J.S.M.; Olde Rikkert, M.G.M.; Nijhuis-van der Sanden, M.W.G. Outcome Instruments to Measure Frailty: A Systematic Review. Ageing Res. Rev. 2011, 10, 104–114. [Google Scholar] [CrossRef]
- Pridham, G.; Rockwood, K.; Rutenberg, A. Strategies for Handling Missing Data That Improve Frailty Index Estimation and Predictive Power: Lessons from the NHANES Dataset. Geroscience 2022, 44, 897–923. [Google Scholar] [CrossRef]
- Jones, D.; Song, X.; Mitnitski, A.; Rockwood, K. Evaluation of a Frailty Index Based on a Comprehensive Geriatric Assessment in a Population Based Study of Elderly Canadians. Aging Clin. Exp. Res. 2005, 17, 465–471. [Google Scholar] [CrossRef]
- Lee, H.; Lee, E.; Jang, I.Y. Frailty and Comprehensive Geriatric Assessment. J. Korean Med. Sci. 2020, 35, e16. [Google Scholar] [CrossRef]
- Badrasawi, M.; Shahar, S.; Zahara, A.M.; Nor Fadilah, R.; Singh, D.K.A. Efficacy of L-Carnitine Supplementation on Frailty Status and Its Biomarkers, Nutritional Status, and Physical and Cognitive Function among Prefrail Older Adults: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial. Clin. Interv. Aging 2016, 11, 1675–1686. [Google Scholar] [CrossRef]
- Dirks, M.L.; Tieland, M.; Verdijk, L.B.; Losen, M.; Nilwik, R.; Mensink, M.; de Groot, L.; van Loon, L.J.C. Protein Supplementation Augments Muscle Fiber Hypertrophy but Does Not Modulate Satellite Cell Content during Prolonged Resistance-Type Exercise Training in Frail Elderly. J. Am. Med. Dir. Assoc. 2017, 18, 608–615. [Google Scholar] [CrossRef]
- Roschel, H.; Hayashi, A.P.; Fernandes, A.L.; Jambassi-Filho, J.C.; Hevia-Larraín, V.; de Capitani, M.; Santana, D.A.; Gonçalves, L.S.; de Sá-Pinto, A.L.; Lima, F.R.; et al. Supplement-Based Nutritional Strategies to Tackle Frailty: A Multifactorial, Double-Blind, Randomized Placebo-Controlled Trial. Clin. Nutr. 2021, 40, 4849–4858. [Google Scholar] [CrossRef]
- Amasene, M.; Medrano, M.; Echeverria, I.; Urquiza, M.; Rodriguez-Larrad, A.; Diez, A.; Labayen, I.; Ariadna, B.B. Malnutrition and Poor Physical Function Are Associated with Higher Comorbidity Index in Hospitalized Older Adults. Front. Nutr. 2022, 9, 920485. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Nagai, Y.; Kawanabe, S.; Hishida, Y.; Hiraki, K.; Sone, M.; Tanaka, Y. Effects of Resistance Training Using Elastic Bands on Muscle Strength with or without a Leucine Supplement for 48 Weeks in Elderly Patients with Type 2 Diabetes. Endocr. J. 2021, 68, 291–298. [Google Scholar] [CrossRef]
- Oktaviana, J.; Zanker, J.; Vogrin, S.; Duque, G. The Effect of Protein Supplements on Functional Frailty in Older Persons: A Systematic Review and Meta-Analysis. Arch. Gerontol. Geriatr. 2020, 86, 103938. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Category | Placebo | Leucine | p-Value |
|---|---|---|---|
| N | 23 | 18 | |
| Age (mean ± SD) | 78.3 ± 8.7 | 78.1 ± 9.6 | 0.935 |
| N (%) females | 14 (60.9) | 13 (72.2) | 0.520 |
| Mini Mental State Examination (MMSE) | 27.8 ± 5.0 | 29.5 ± 3.9 | 0.255 |
| Mini Nutritional Assessment (MNA) | 25.4 ± 2.0 | 24.1 ± 2.0 | 0.041 * |
| Ability to perform daily activities (Barthel index) | 78.0 ± 21.5 | 79.7 ± 21.3 | 0.805 |
| Tinetti mobility test (TMT) | 23.1 ± 4.8 | 21.9 ± 5.2 | 0.472 |
| Comorbidities (Charlson Index) | 5.34 ± 2.0 | 5.0 ± 1.7 | 0.576 |
| Baseline Frailty Group N (%) | |||
| 0–0.2 | 5 (21.7%) | 4 (22.2%) | 0.721 |
| 0.2–0.3 | 9 (39.1%) | 9 (50.0%) | |
| 0.3+ | 9 (39.1%) | 5 (27.8%) | |
| Follow-up Frailty Group N (%) | |||
| 0–0.2 | 5 (21.7%) | 3 (16.7%) | 0.808 |
| 0.2–0.3 | 8 (34.8%) | 9 (44.4%) | |
| 0.3+ | 10 (43.5%) | 7 (38.9%) | |
| Frailty Index Difference (mean ± SD) | 0.005 ± 0.45 | 0.01 ± 0.38 | 0.316 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buigues, C.; Theou, O.; Fonfría-Vivas, R.; Martínez-Arnau, F.M.; Rockwood, K.; Cauli, O. Can Leucine Supplementation Improve Frailty Index Scores? Geriatrics 2023, 8, 102. https://doi.org/10.3390/geriatrics8050102
Buigues C, Theou O, Fonfría-Vivas R, Martínez-Arnau FM, Rockwood K, Cauli O. Can Leucine Supplementation Improve Frailty Index Scores? Geriatrics. 2023; 8(5):102. https://doi.org/10.3390/geriatrics8050102
Chicago/Turabian StyleBuigues, Cristina, Olga Theou, Rosa Fonfría-Vivas, Francisco M. Martínez-Arnau, Kenneth Rockwood, and Omar Cauli. 2023. "Can Leucine Supplementation Improve Frailty Index Scores?" Geriatrics 8, no. 5: 102. https://doi.org/10.3390/geriatrics8050102
APA StyleBuigues, C., Theou, O., Fonfría-Vivas, R., Martínez-Arnau, F. M., Rockwood, K., & Cauli, O. (2023). Can Leucine Supplementation Improve Frailty Index Scores? Geriatrics, 8(5), 102. https://doi.org/10.3390/geriatrics8050102