


Effectiveness of a Remote Monitoring-Based Home Training System for Preventing Frailty in Older Adults in Japan: A Preliminary Randomized Controlled Trial
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
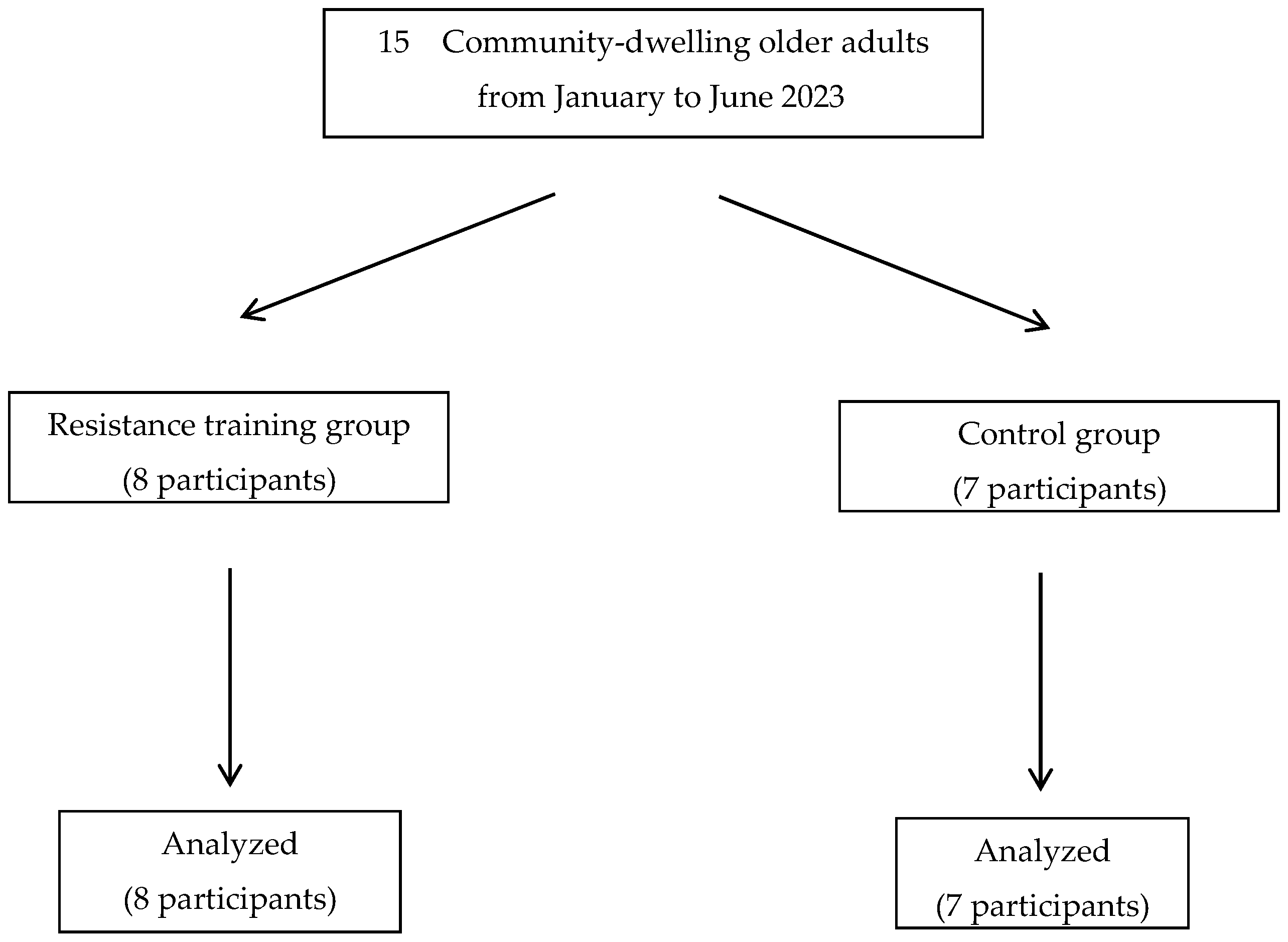
2.1. Participants
2.2. SUKUBARA®
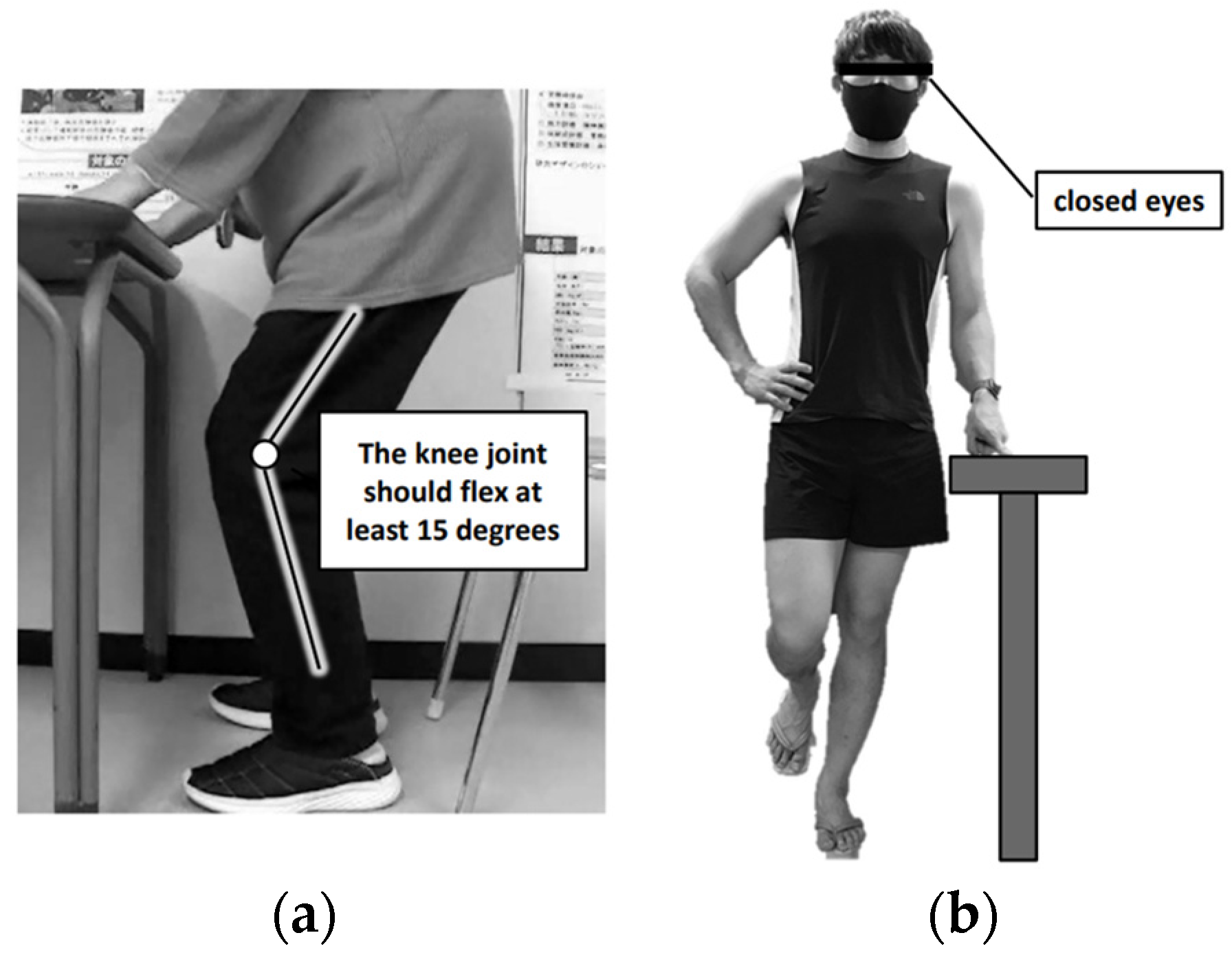
2.2.1. Exercise Protocols
2.2.2. Monitoring System Using YouTube Studio
2.3. Clinical Data and Laboratory Tests
2.4. Statistical Analysis
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Bandeen-Roche, K.; Xue, Q.-L.; Ferrucci, L.; Walston, J.; Guralnik, J.M.; Chaves, P.; Zeger, S.L.; Fried, L.P. Phenotype of frailty: Characterization in the women’s health and aging studies. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Xue, Q.L. The frailty syndrome: Definition and natural history. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.Y.; Bruyere, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef]
- Liu, P.; Hao, Q.; Hai, S.; Wang, H.; Cao, L.; Dong, B. Sarcopenia as a predictor of all-cause mortality among community-dwelling older people: A systematic review and meta-analysis. Maturitas 2017, 103, 16–22. [Google Scholar] [CrossRef]
- Borst, S.E. Interventions for sarcopenia and muscle weakness in older people. Age Ageing 2004, 33, 548–555. [Google Scholar] [CrossRef]
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance exercise for muscular strength in older adults: A meta-analysis. Ageing Res. Rev. 2010, 9, 226–237. [Google Scholar] [CrossRef]
- Peterson, M.D.; Sen, A.; Gordon, P.M. Influence of resistance exercise on lean body mass in aging adults: A meta-analysis. Med. Sci. Sports Exerc. 2011, 43, 249–258. [Google Scholar] [CrossRef]
- American College of Sports Medicine. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Weakley, J.; Schoenfeld, B.J.; Ljungberg, J.; Halson, S.L.; Phillips, S.M. Physiological responses and adaptations to lower load resistance training: Implications for health and performance. Sports Med. Open 2023, 9, 28. [Google Scholar] [CrossRef]
- Watanabe, Y.; Tanimoto, M.; Ohgane, A.; Sanada, K.; Miyachi, M.; Ishii, N. Increased muscle size and strength from slow-movement, low-intensity resistance exercise and tonic force generation. J. Aging Phys. Act. 2013, 21, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Madarame, H.; Ogasawara, R.; Nakazato, K.; Ishii, N. Effect of very low-intensity resistance training with slow movement on muscle size and strength in healthy older adults. Clin. Physiol. Funct. Imaging 2014, 34, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Van Roie, E.; Delecluse, C.; Coudyzer, W.; Boonen, S.; Bautmans, I. Strength training at high versus low external resistance in older adults: Effects on muscle volume, muscle strength, and force-velocity characteristics. Exp. Gerontol. 2013, 48, 1351–1361. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Yamada, Y.; Yoshida, T.; Yokoyama, K.; Miyake, M.; Yamagata, E.; Yamada, M.; Yoshinaka, Y.; Kimura, M.; for Kyoto-Kameoka Study Group. Comprehensive geriatric intervention in community-dwelling older adults: A cluster-randomized controlled trial. J. Cachexia Sarcopenia Muscle 2020, 11, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Koda, M.; Shimizu, Y.; Tsubaki, T.; Hada, Y. Verification of the effects of a YouTube based home based (self-managed intervention) training system developed for frailty prevention—A pilot study. J. Allied Health, 2022; in press. [Google Scholar]
- Lacroix, A.; Hortobágyi, T.; Beurskens, R.; Granacher, U. Effects of supervised vs. unsupervised training programs on balance and muscle strength in older adults: A systematic review and meta-analysis. Sports Med. 2017, 47, 2341–2361. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, CD012424. [Google Scholar] [CrossRef]
- Suzuki, Y.; Yatoh, S.; Suzuki, H.; Tanabe, Y.; Shimizu, Y.; Hada, Y.; Shimano, H. Age-dependent changes in dynamic standing-balance ability evaluated quantitatively using a stabilometer. J. Phys. Ther. Sci. 2018, 30, 86–91. [Google Scholar] [CrossRef]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between dual-energy X-ray absorptiometry and bioelectrical impedance analyses for accuracy in measuring whole body muscle mass and appendicular skeletal muscle mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef]
- Yi, Y.; Baek, J.Y.; Lee, E.; Jung, H.-W.; Jang, I.-Y. A comparative study of high-frequency bioelectrical impedance analysis and dual-energy X-ray absorptiometry for estimating body composition. Life 2022, 12, 994. [Google Scholar] [CrossRef]
- Hurt, R.T.; Ebbert, J.O.; Croghan, I.; Nanda, S.; Schroeder, D.R.; Teigen, L.M.; Velapati, S.R.; Mundi, M.S. The comparison of segmental multifrequency bioelectrical impedance analysis and dual-energy X-ray absorptiometry for estimating fat free mass and percentage body fat in an ambulatory population. J. Parenter. Enteral. Nutr. 2021, 45, 1231–1238. [Google Scholar] [CrossRef]
- Saeterbakken, A.H.; Stien, N.; Pedersen, H.; Andersen, V. Core muscle activation in three lower extremity exercises with different stability requirements. J. Strength Cond. Res. 2022, 36, 304–309. [Google Scholar] [CrossRef]
- Erskine, R.M.; Jones, D.A.; Williams, A.G.; Stewart, C.E.; Degens, H. Inter-individual variability in the adaptation of human muscle specific tension to progressive resistance training. Eur. J. Appl. Physiol. 2010, 110, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Erskine, R.M.; Fletcher, G.; Folland, J.P. The contribution of muscle hypertrophy to strength changes following resistance training. Eur. J. Appl. Physiol. 2014, 114, 1239–1249. [Google Scholar] [CrossRef]
- Baz-Valle, E.; Fontes-Villalba, M.; Santos-Concejero, J. Total number of sets as a training volume quantification method for muscle hypertrophy: A systematic review. J. Strength Cond. Res. 2021, 35, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Onishi, T.; Ogawa, Y.; Yamauchi, J.; Kawada, S. Effects of motor imagery combined with action observation training on the lateral specificity of muscle strength in healthy subjects. Biomed. Res. 2019, 40, 107–113. [Google Scholar] [CrossRef]
- Van Het Reve, E.; Silveira, P.; Daniel, F.; Casati, F.; de Bruin, E.D. Tablet-based strength-balance training to motivate and improve adherence to exercise in independently living older people: Part 2 of a phase II preclinical exploratory trial. J. Med. Internet Res. 2014, 16, e159. [Google Scholar] [CrossRef]
- Braith, R.W.; Graves, J.E.; Pollock, M.L.; Leggett, S.L.; Carpenter, D.M.; Colvin, A.B. Comparison of 2 vs 3 days/week of variable resistance training during 10- and 18-week programs. Int. J. Sports Med. 1989, 10, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Izuma, K.; Saito, D.N.; Sadato, N. Processing of the incentive for social approval in the ventral striatum during charitable donation. J. Cogn. Neurosci. 2010, 22, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Bereczkei, T.; Birkas, B.; Kerekes, Z. Public charity offer as a proximate factor of evolved reputation-building strategy: An experimental analysis of a real-life situation. Evol. Hum. Behav. 2007, 28, 277–284. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| RT n = 8 | CO n = 7 | p | |
|---|---|---|---|
| Age (years) | 67 (65, 70) | 72 (66, 73) | 0.407 |
| Female, n (%) | 2 (25) | 3 (43) | 0.480 |
| Height (m) | 1.65 (1.62, 1.71) | 1.67 (1.58, 1.74) | 0.953 |
| Body weight (kg) | 61.6 ± 9.6 | 66.5 ± 7.0 | 0.290 |
| Body mass index (kg/m2) | 22.3 ± 2.4 | 24.3 ± 1.3 | 0.079 |
| Currently working, n (%) | 2 (33) | 1 (20) | 0.613 |
| Currently driving, n (%) | 7 (88) | 7 (100) | 0.694 |
| Fall history, n (%) | 0 (0) | 0 (0) | 1.000 |
| Body composition | |||
| Fat-free mass (kg) | 25.8 ± 5.0 | 27.1 ± 5.7 | 0.652 |
| Body fat mass (kg) | 14.7 ± 3.3 | 17.3 ± 4.6 | 0.225 |
| Muscle strength | |||
| Grip strength (kgf) | 37 (31, 47) | 37 (29, 46) | 0.602 |
| Knee extension strength (Nm/kg) | 1.54 ± 0.45 | 1.62 ± 0.26 | 0.685 |
| Balance capability | |||
| Index of postural stability | 1.86 (1.76, 2.01) | 1.62 (1.57, 1.67) | 0.073 |
| Modified index of postural stability | 0.46 (0.22, 0.60) | 0.43 (0.32, 0.59) | 1.000 |
| One-leg standing time with eyes open (s) | 95 (52, 120) | 99 (90, 116) | 0.720 |
| One-leg standing time with eyes closed (s) | 4 (3, 6) | 4 (3, 6) | 0.694 |
| Cognitive function | |||
| MMSE (points) | 30 (30, 30) | 30 (29, 30) | 0.613 |
| Physical activity | |||
| Steps (steps/day) * | 7279 ± 1878 | 8640 ± 3952 | 0.346 |
| MVPA time (min/day) * | 14.0 (11.6, 21.0) | 23.7 (15.4, 34.7) | 0.247 |
| Group | Baseline | 12 Weeks | p for Time | Change between Baseline and 12 Weeks | p for Group | p for Group × Time | |
|---|---|---|---|---|---|---|---|
| Body composition | |||||||
| Body weight (kg) | RT | 61.6 ± 9.6 | 61.6 ± 9.2 | 0.995 | −0.02 ± 1.4 | 0.251 | 0.894 |
| CO | 66.5 ± 7.0 | 65.6 ± 7.3 | 0.851 | −0.9 ± 1.3 | |||
| Fat-free mass (kg) | RT | 25.8 ± 5.0 | 26.3 ± 4.9 | 0.843 | 0.5 ± 0.5 | 0.028 | 0.866 |
| CO | 27.1 ± 5.7 | 26.9 ± 5.5 | 0.964 | −0.1 ± 0.5 | |||
| Body fat mass (kg) | RT | 14.7 ± 3.3 | 13.9 ± 3.0 | 0.663 | −0.9 ± 0.6 | 0.254 | 0.928 |
| CO | 17.3 ± 4.6 | 16.7 ± 4.7 | 0.777 | −0.6 ± 0.9 | |||
| Muscle strength | |||||||
| Grip strength (kgf) | RT | 37.3 ± 9.5 | 37.1 ± 9.5 | 0.977 | −0.1 ± 2.5 | 0.398 | 0.651 |
| CO | 34.6 ± 7.5 | 37.4 ± 7.5 | 0.561 | 1.0 ± 2.3 | |||
| Knee extension strength (Nm/kg) | RT | 1.54 ± 0.54 | 1.74 ± 0.33 | 0.226 | 0.20 ± 0.22 | 0.041 | 0.459 |
| CO | 1.62 ± 0.26 | 1.65 ± 0.17 | 0.897 | 0.02 ± 0.13 |
| Group | Baseline | 12 Weeks | p for Time | Change between Baseline and 12 Weeks | p for Group | |
|---|---|---|---|---|---|---|
| Balance capability | ||||||
| Index of postural stability | RT | 1.86 (1.76, 2.01) | 1.91 (1.76, 2.06) | 0.799 | 0.06 (−0.11, 0.14) | 0.897 |
| CO | 1.62 (1.57, 1.67) | 1.55 (1.47, 1.78) | 0.917 | 0.01 (−0.13, 0.16) | ||
| Modified index of postural stability | RT | 0.46 (0.22, 0.60) | 0.39 (0.14, 0.61) | 0.779 | 0.04 (−0.05, 0.09) | 0.365 |
| CO | 0.43 (0.32, 0.59) | 0.31 (0.18, 0.40) | 0.116 | −0.18 (−0.22, −0.01) | ||
| One-leg standing time with eyes open (s) | RT | 95 (52, 120) | 116 (53, 120) | 0.720 | 0 (−3, 2) | 0.120 |
| CO | 99 (90, 116) | 74 (30, 120) | 0.080 | −25 (−50, 0) | ||
| One-leg standing time with eyes closed (s) | RT | 4 (3, 5) | 7 (6, 11) | 0.018 | 3 (1, 7) | 0.726 |
| CO | 4 (3, 6) | 6 (4, 8) | 0.034 | 2 (1, 4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, Y.; Shimizu, Y.; Soma, Y.; Matsuda, T.; Hada, Y.; Koda, M. Effectiveness of a Remote Monitoring-Based Home Training System for Preventing Frailty in Older Adults in Japan: A Preliminary Randomized Controlled Trial. Geriatrics 2024, 9, 20. https://doi.org/10.3390/geriatrics9010020
Suzuki Y, Shimizu Y, Soma Y, Matsuda T, Hada Y, Koda M. Effectiveness of a Remote Monitoring-Based Home Training System for Preventing Frailty in Older Adults in Japan: A Preliminary Randomized Controlled Trial. Geriatrics. 2024; 9(1):20. https://doi.org/10.3390/geriatrics9010020
Chicago/Turabian StyleSuzuki, Yasuhiro, Yukiyo Shimizu, Yuichiro Soma, Takaaki Matsuda, Yasushi Hada, and Masao Koda. 2024. "Effectiveness of a Remote Monitoring-Based Home Training System for Preventing Frailty in Older Adults in Japan: A Preliminary Randomized Controlled Trial" Geriatrics 9, no. 1: 20. https://doi.org/10.3390/geriatrics9010020
APA StyleSuzuki, Y., Shimizu, Y., Soma, Y., Matsuda, T., Hada, Y., & Koda, M. (2024). Effectiveness of a Remote Monitoring-Based Home Training System for Preventing Frailty in Older Adults in Japan: A Preliminary Randomized Controlled Trial. Geriatrics, 9(1), 20. https://doi.org/10.3390/geriatrics9010020