

Qualities of Older Adults’ Family and Friendship Relationships and Their Association with Life Satisfaction



Abstract
:1. Statement of Relevance
- Interacting types of social support and social strain by types of relationships;
- Unraveling the most significant relationships and controlling for demographics and self-rated health statuses;
- Revealing the importance of family, child, non-child relative, and friend relationships to the overall life satisfaction of older adults;
- Providing preliminary evidence to inform relationship support interventions responsive to older adults’ life situations to improve life satisfaction.
1.1. Older Adults’ Friendship Relationship Qualities: Their Association with Life Satisfaction
1.2. Family and Friendship Relationships in Life Satisfaction
1.3. Significance of Personal Factors, Health and Function, and Social Interaction Types
- How are older adults’ social demographics and personal and social interaction factors associated with their life satisfaction?
- How are social support and social strain in spousal/partner, child, relative, and friendship relationships associated with life satisfaction in older adults?
2. Methods
Sources of Data
3. Measures
3.1. Procedure
3.2. Analysis Strategy
4. Results
4.1. Sociodemographic, Health and Function, and Life Satisfaction
4.2. Relationships Types and Life Satisfaction
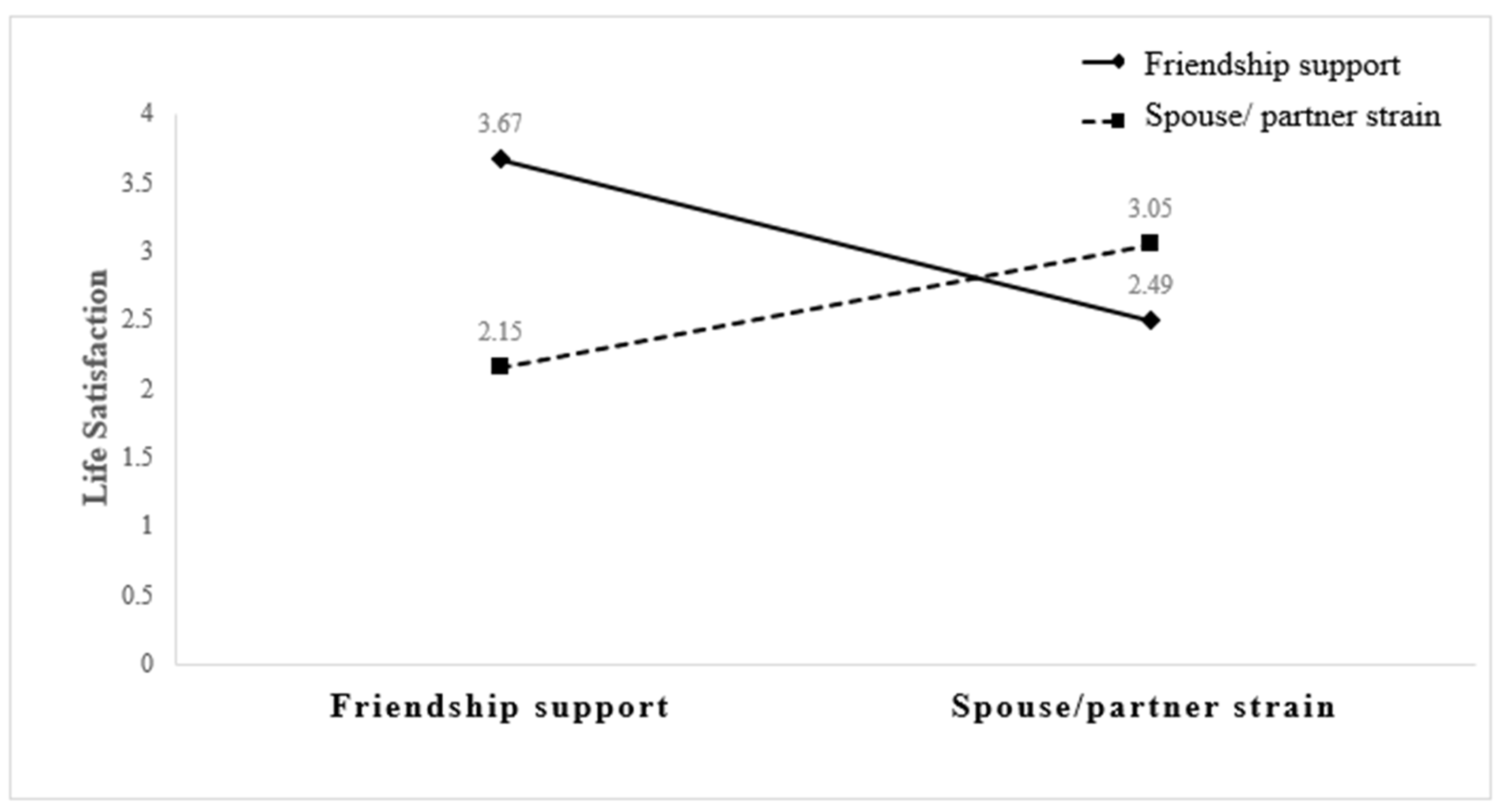
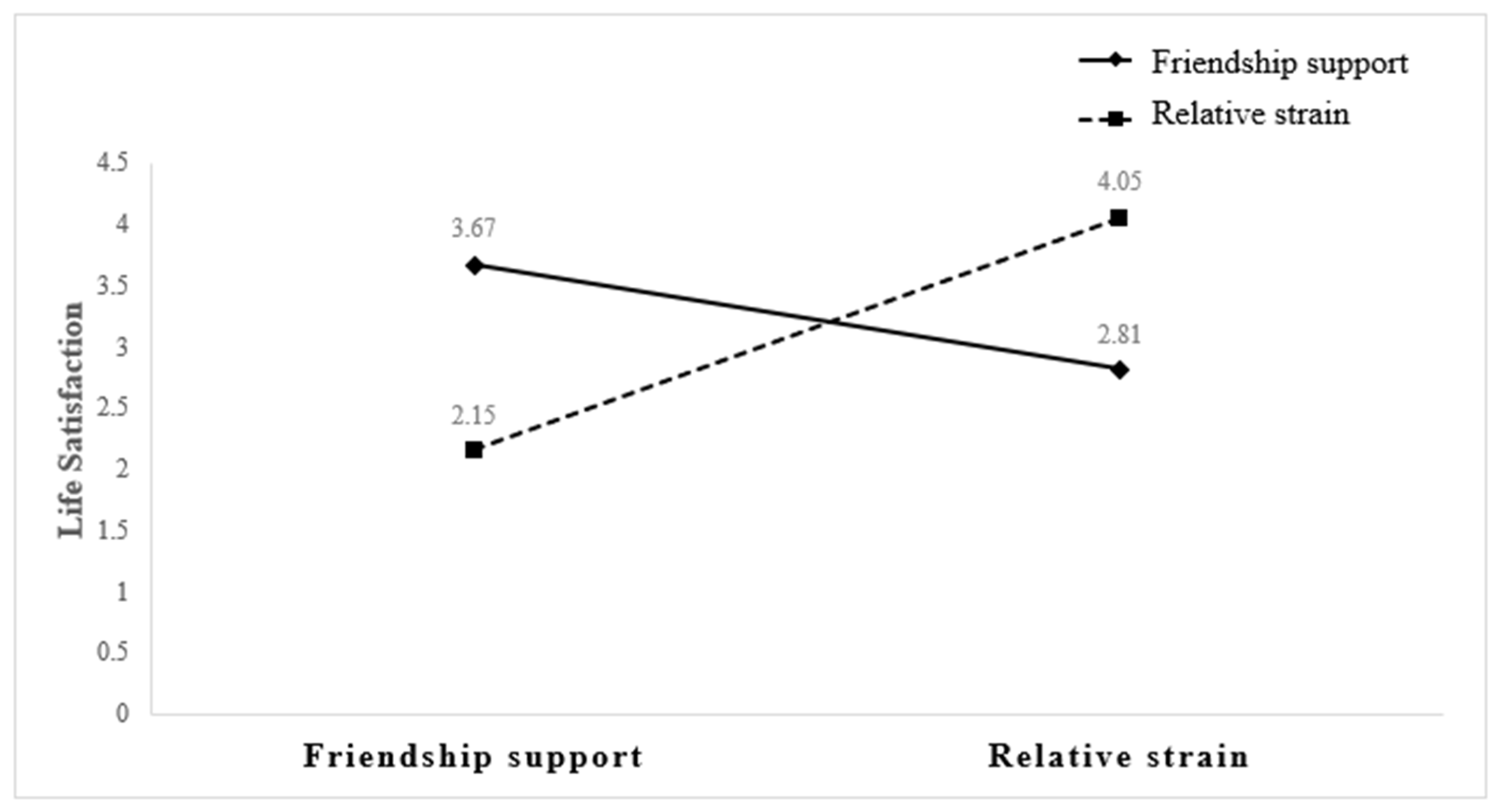
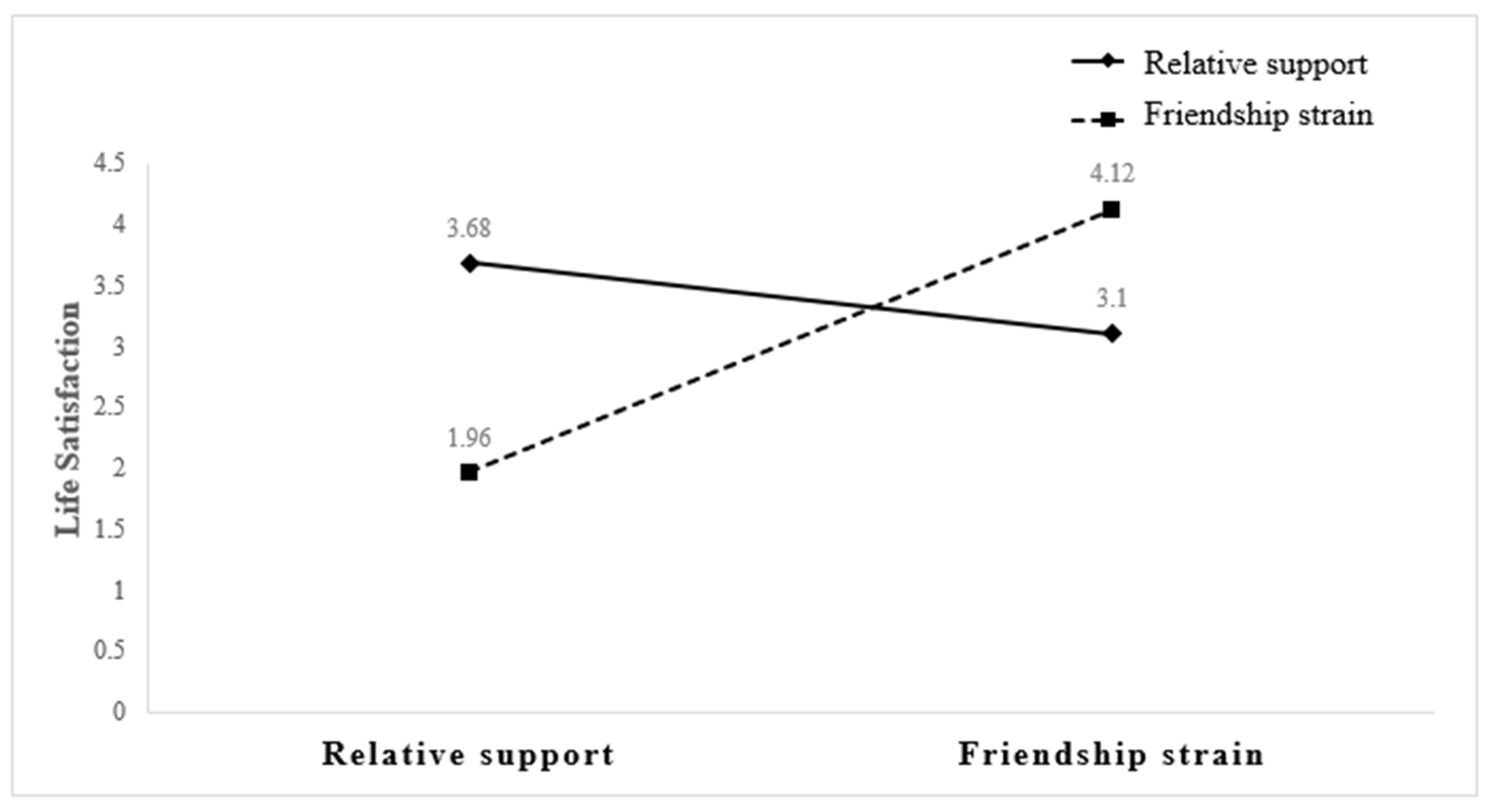
4.3. Combined Effects of Relationship Quality on Life Satisfaction
5. Discussion
5.1. Implications for Gerontologic Research and Practice
5.2. Limitations of this Study and Suggestions for Further Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lim, H.J.; Min, D.K.; Thorpe, L.; Lee, C.H. Multidimensional construct of life satisfaction in older adults in Korea: A six-year follow-up study. BMC Geriatr. 2016, 16, 197. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Janicki-Deverts, D.; Turner, R.B.; Doyle, W.J. Does hugging provide stress-buffering social support? A study of susceptibility to upper respiratory infection and illness. Psychol. Sci. 2015, 26, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Hornstein, E.A.; Eisenberger, N.I. Unpacking the buffering effect of social support figures: Social support attenuates fear acquisition. PLoS ONE 2017, 12, e0175891. [Google Scholar] [CrossRef] [PubMed]
- Fakoya, O.A.; McCorry, N.K.; Donnelly, M. Loneliness and social isolation interventions for older adults: A scoping review of reviews. BMC Public Health 2020, 20, 129. [Google Scholar] [CrossRef] [PubMed]
- Lue, B.; Chen, L.; Wu, S. Health, financial stresses, and life satisfaction affecting late-life depression among older adults: A nationwide, longitudinal survey in Taiwan. Arch. Gerontol. Geriatr. 2010, 50, S34–S38. [Google Scholar] [CrossRef] [PubMed]
- Amati, V.; Meggiolaro, S.; Rivellini, G.; Zaccarin, S. Social relations and life satisfaction: The role of friends. Genus 2018, 74, 7. [Google Scholar] [CrossRef] [PubMed]
- Carr, D.; Freedman, V.A.; Cornman, J.C.; Schwarz, N. Happy marriage, happy life? Marital quality and subjective Well-being in later life. J. Marriage Fam. 2014, 76, 930–948. [Google Scholar] [CrossRef]
- Fiori, K.L.; Smith, J.; Antonucci, T.C. Social network types among older adults: A multidimensional approach. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2007, 62, 322–330. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychol. Aging 2000, 15, 187–224. [Google Scholar] [CrossRef]
- Şener, A.; Oztop, H.; Doğan, N.; Guven, S. Family, close relatives, friends: Life satisfaction among older people. Educ. Gerontol. 2008, 34, 890–906. [Google Scholar] [CrossRef]
- Hansen, T.; Slagsvold, B. The age and subjective well-being paradox revisited: A multidimensional perspective. Nor. Epidemiol. 2012, 22, 187–195. [Google Scholar] [CrossRef]
- Wiesmann, U.; Hannich, H.J. A salutogenic analysis of the well-being paradox in older age. J. Happiness Stud. 2014, 15, 339–355. [Google Scholar] [CrossRef]
- Schilling, O. Development of life satisfaction in old age: Another view on the “Paradox”. Soc. Indic. Res. 2006, 75, 241–271. [Google Scholar] [CrossRef]
- Cranford, J.A. Stress-buffering or stress-exacerbation? Social support and social undermining as moderators of the relationship between perceived stress and depressive symptoms among married people. Pers. Relatsh. 2004, 11, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Szinovacz, M.E. Positive, negative, and ambivalent interactions with family and friends: Associations with well-being. J. Marriage Fam. 2016, 78, 660–679. [Google Scholar] [CrossRef]
- Thompson, M.G.; Heller, K. Facets of support related to well-being: Quantitative social isolation and perceived family support in a sample of elderly women. Psychol. Aging 1990, 5, 535–544. [Google Scholar] [CrossRef]
- Yeung, G.T.Y.; Fung, H.H. Social support and life satisfaction among Hong Kong Chinese older adults: Family first? Eur. J. Ageing 2007, 4, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Tomini, F.; Tomini, S.M.; Groot, W. Understanding the value of social networks in life satisfaction of elderly people: A comparative study of 16 European countries using SHARE data. BMC Geriatr. 2016, 16, 203. [Google Scholar] [CrossRef]
- O’Connor, B.P. Family and friend relationships among older and younger adults: Interaction motivation, mood, and quality. Int. J. Aging Hum. Dev. 1995, 40, 9–29. [Google Scholar] [CrossRef]
- Huxhold, O.; Miche, M.; Schüz, B. Benefits of having friends in older ages: Differential effects of informal social activities on well-being in middle-aged and older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2014, 69, 366–375. [Google Scholar] [CrossRef]
- Jensen, J.F.; Rauer, A.J. Turning inward versus outward: Relationship work in young adults and romantic functioning. Pers. Relatsh. 2014, 21, 451–467. [Google Scholar] [CrossRef]
- Umberson, D.; Chen, M.D.; House, J.S.; Hopkins, K.; Slaten, E. The effect of social relationships on psychological well-being: Are men and women really so different? Am. Sociol. Rev. 1996, 61, 837–857. [Google Scholar] [CrossRef]
- Waite, L.; Das, A. Families, social life, and well-being at older ages. Demography 2010, 47 (Suppl. S1), S87–S109. [Google Scholar] [CrossRef] [PubMed]
- Cantor, M. Family and community—Changing roles in an aging society. Gerontologist 1991, 31, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Warner, D.F.; Adams, S.A.; Anderson, R.K. The good, the bad, and the indifferent: Physical disability, social role configurations, and changes in loneliness among married and unmarried older adults. J. Aging Health 2019, 31, 1423–1453. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, L.; Isaacowitz, D.; Charles, S. Taking time seriously. A theory of socioemotional selectivity. Am. Psychol. 1999, 54, 165–181. [Google Scholar] [CrossRef] [PubMed]
- Birditt, K.S.; Hartnett, C.S.; Fingerman, K.L.; Zarit, S.H.; Antonucci, T.C. Extending the intergenerational stake hypothesis: Evidence of an intra-individual stake and implications for well-being. J. Marriage Fam. 2015, 77, 877–888. [Google Scholar] [CrossRef] [PubMed]
- DeWall, C.N. (Ed.) The Oxford Handbook of Social Exclusion; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Chen, Y.; Feeley, T.H. Social support, social strain, loneliness, and well-being among older adults: An analysis of the Health and Retirement Study. J. Soc. Pers. Relatsh. 2014, 31, 141–161. [Google Scholar] [CrossRef]
- Warner, D.F.; Adams, S.A. Widening the social context of disablement among married older adults: Considering the role of nonmarital relationships for loneliness. Soc. Sci. Res. 2012, 41, 1529–1545. [Google Scholar] [CrossRef]
- Proulx, C.M.; Helms, H.M.; Milardo, R.M.; Payne, C.C. Relational support from friends and wives’ family relationships: The role of husbands’ interference. J. Soc. Pers. Relatsh. 2009, 26, 195–210. [Google Scholar] [CrossRef]
- Tang, F.; Jang, H.; Rauktis, M.B.; Musa, D.; Beach, S. The race paradox in subjective wellbeing among older Americans. Ageing Soc. 2019, 39, 568–589. [Google Scholar] [CrossRef]
- Barlow, M.A.; Liu, S.Y.; Wrosch, C. Chronic illness and loneliness in older adulthood: The role of self-protective control strategies. Health Psychol. 2015, 34, 870. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Ma, J.; Ren, Z.; Zhou, G.; Gong, P.; Liu, M.; Yang, X.; Xiong, W.; Wang, Q.; Liu, H.; et al. Association between activities of daily living disability and depression symptoms of middle-aged and older Chinese adults and their spouses: A community based study. J. Affect. Disord. 2019, 242, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Canada, B.; Stephan, Y.; Sutin, A.R.; Terracciano, A. Personality and falls among older adults: Evidence from a longitudinal cohort. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 75, 1905–1910. [Google Scholar] [CrossRef]
- Saklofske, D.H.; Austin, E.J.; Rohr, B.A.; Andrews, J.J. Personality, emotional intelligence and exercise. J. Health Psychol. 2007, 12, 937–948. [Google Scholar] [CrossRef] [PubMed]
- McCrae, R.R.; Costa, P.T., Jr.; Ostendorf, F.; Angleitner, A.; Hřebíčková, M.; Avia, M.D.; Sanz, J.; Sánchez-Bernardos, M.L.; Kusdil, M.E.; Woodfield, R.; et al. Nature over nurture: Temperament, personality, and life span development. J. Personal. Soc. Psychol. 2000, 78, 173. [Google Scholar] [CrossRef]
- Debast, I.; van Alphen, S.P.; Rossi, G.; Tummers, J.H.; Bolwerk, N.; Derksen, J.J.; Rosowsky, E. Personality traits and personality disorders in late middle and old age: Dothey remain stable? A literature review. Clin. Gerontol. 2014, 37, 253–271. [Google Scholar] [CrossRef]
- Choi, Y.J. Age-friendly features in home and community and the self-reported health and functional limitation of older adults: The role of supportive environments. J. Urban Health 2020, 97, 471–485. [Google Scholar] [CrossRef] [PubMed]
- Nieboer, A.P.; Cramm, J.M. Age-friendly communities matter for older people’s well-being. J. Happiness Stud. 2018, 19, 2405–2420. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Commission to Foster Social Connection. 2023. Available online: https://www.who.int/activities/creating-age-friendly-cities-and-communities (accessed on 9 March 2024).
- Spector, P.E. Do not cross me: Optimizing the use of cross-sectional designs. J. Bus. Psychol. 2019, 34, 125–137. [Google Scholar] [CrossRef]
- Health and Retirement Study. 2014 RAND HRS Fat File Public Use Data Set; Produced and Distributed by the University of Michigan with Funding from the National Institute on Aging (grant number NIA U01AG009740); University of Michigan: Ann Arbor, MI, USA, 2020. [Google Scholar]
- Hapfelmeier, A.; Hothorn, T.; Ulm, K. Recursive partitioning on incomplete data using surrogate decisions and multiple imputation. Comput. Stat. Data Anal. 2012, 56, 1552–1565. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Vexler, A.; Whitcomb, B.W.; Liu, A. The limitations due to exposure detection limits for regression models. Am. J. Epidemiol. 2006, 163, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, L.; McKee, K.J. Correlates of social and emotional loneliness in older people: Evidence from an English community study. Aging Ment. Health 2014, 18, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; White, I.R.; Anzures-Cabrera, J. Meta-analysis of skewed data: Combining results reported on log-transformed or raw scales. Stat. Med. 2008, 27, 6072–6092. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N. Detecting multicollinearity in regression analysis. Am. J. Appl. Math. Stat. 2020, 8, 39–42. [Google Scholar] [CrossRef]
- Komalasari, R.; Mpofu, E.; Prybutok, G.; Ingman, S.R. Subjective Aging Difficulties among Older Adults with Subjective Cognitive Decline. J. Appl. Gerontol. 2023, 42, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Waite, L. Bad marriage, broken heart? Age and gender differences in the link between marital quality and cardiovascular risks among older adults. J. Health Soc. Behav. 2014, 55, 403–423. [Google Scholar] [CrossRef] [PubMed]
- Felmlee, D.; Muraco, A. Gender and friendship norms among older adults. Res. Aging 2009, 31, 318–344. [Google Scholar] [CrossRef] [PubMed]
- Schneider, F.W.; Gruman, J.A.; Coutts, L.A. Applied Social Psychology: Understanding and Addressing Social and Practical Problems, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Lendon, J.P.; Silverstein, M.; Giarrusso, R. Ambivalence in older parent–adult child relationships: Mixed feelings, mixed measures. J. Marriage Fam. 2014, 76, 272–284. [Google Scholar] [CrossRef]
- Wellman, B.; Wortley, S. Different strokes from different folks: Community ties and social support. Am. J. Sociol. 1990, 96, 558–588. [Google Scholar] [CrossRef]
- Weissman, J.D.; Russell, D. Relationships between living arrangements and health status among older adults in the United States, 2009–2014: Findings from the National Health Interview Survey. J. Appl. Gerontol. 2018, 37, 7–25. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (Percentage/%) | Mean (Standard Deviation) |
|---|---|---|
| Life satisfaction | 4.93 (1.52) | |
| Social interaction quality | ||
| Spouse/partner support | 3.41 (0.67) | |
| Spouse/partner strain | 3.01 (0.69) | |
| Child support | 3.22 (0.73) | |
| Child strain | 3.27 (0.64) | |
| Relative support | 2.82 (0.86) | |
| Relative strain | 3.43 (0.62) | |
| Friend support | 2.91 (0.76) | |
| Friend strain | 3.61 (0.51) | |
| Age | 67.9(9.3) | |
| 50–64 | 435 (36.9%) | |
| 65–74 | 401 (34.0%) | |
| 75–84 | 288 (24.4%) | |
| 85+ | 54 (4.6%) | |
| Gender | ||
| Female | 645 (54.8%) | |
| Male | 533 (45.2%) | |
| Education | 12.63 (2.88) | |
| Subjective social status | 6.32 (1.76) | |
| Self-reported general health status | ||
| Good | 718 (61.0) | |
| Poor | 460 (39.0) | |
| Physical health | ||
| Activities of daily living | 0.45 (0.95) | |
| Instrumental activities of daily living | 0.30 (0.77) | |
| Depressive symptoms | 1.73 (2.06) | |
| Physical activity | ||
| Vigorous activity | 3.26 (1.30) | |
| Moderate activity | 2.66 (1.61) | |
| Mild activity | 2.24 (1.64) | |
| Personality traits | ||
| Extraversion | 3.13 (0.58) | |
| Openness to experience | 2.85 (0.57) | |
| Neuroticism | 2.08 (0.63) | |
| Agreeableness | 3.50 (0.50) |
| Variables | B | SE B | Standardized β |
|---|---|---|---|
| Age | 0.16 | 0.05 | 0.09 ** |
| Gender | 0.12 | 0.09 | 0.04 |
| Education | −0.05 | 0.02 | −0.09 ** |
| Subjective social status | 0.15 | 0.02 | 0.17 ** |
| Self-reported general health status | 0.20 | 0.09 | 0.07 † |
| Physical health | |||
| Activities of daily living | −0.91 | 0.24 | −0.12 ** |
| Instrumental activities of daily living | −0.09 | 0.27 | −0.01 |
| Depressive symptoms | −0.63 | 0.16 | −0.13 ** |
| Physical activity | |||
| Vigorous activity | 0.02 | 0.04 | 0.02 |
| Moderate activity | 0.03 | 0.03 | 0.02 |
| Mild activity | 0.02 | 0.04 | 0.01 |
| Personality traits | |||
| Extraversion | 0.26 | 0.09 | 0.10 * |
| Openness to experience | −0.09 | 0.09 | −0.03 |
| Neuroticism | −0.12 | 0.07 | −0.05 |
| Agreeableness | 0.15 | 0.10 | 0.05 |
| Social interaction quality | |||
| Spouse/partner support | 0.32 | 0.07 | 0.14 ** |
| Spouse/partner strain | 0.18 | 0.07 | 0.08 † |
| Child support | 0.13 | 0.07 | 0.06 † |
| Child strain | −0.06 | 0.08 | −0.03 |
| Relative support | 0.01 | 0.05 | 0.01 |
| Relative strain | 0.07 | 0.08 | 0.03 |
| Friendship support | 0.05 | 0.06 | 0.03 |
| Friendship strain | −0.14 | 0.09 | −0.05 |
| Relationship | B | SE | Beta | R2 | ΔR2 | ΔF |
|---|---|---|---|---|---|---|
| Spouse/Partner | ||||||
| Step 1 | ||||||
| Spouse/partner support | 0.62 | 0.06 | 0.28 ** | 0.10 | 0.10 | 67.89 ** |
| Child strain | 0.29 | 0.07 | 0.12 ** | |||
| Step 2 | ||||||
| Spouse/partner support * Child strain | 0.10 | 0.09 | .00 | 0.10 | 0.00 | 0.01 |
| Step 1 | ||||||
| Spouse/partner support | 0.62 | 0.06 | 0.27 ** | 0.11 | 0.11 | 69.39 ** |
| Relative strain | 0.32 | 0.07 | 0.13 ** | |||
| Step 2 | ||||||
| Spouse/partner support * Relative strain | 0.10 | 0.09 | 0.03 | 0.11 | 0.00 | 1.31 |
| Step 1 | ||||||
| Spouse/partner support | 0.66 | 0.06 | 0.29 ** | 0.10 | 0.10 | 62.76 ** |
| Friendship strain | 0.26 | 0.08 | 0.09 * | |||
| Step 2 | ||||||
| Spouse/partner support * Friendship strain | 0.14 | 0.12 | 0.03 | 0.10 | 0.00 | 1.29 |
| Child | ||||||
| Step 1 | ||||||
| Child support | 0.39 | 0.06 | 0.19 ** | 0.11 | 0.11 | 71.54 ** |
| Partner strain | 0.52 | 0.06 | 0.23 ** | |||
| Step 2 | ||||||
| Child support * Spouse/partner strain | −0.01 | 0.08 | 0.00 | 0.11 | 0.00 | 0.02 |
| Step 1 | ||||||
| Child support | 0.42 | 0.06 | 0.20 ** | 0.07 | 0.07 | 46.78 ** |
| Relative strain | 0.34 | 0.07 | 0.14 ** | |||
| Step 2 | ||||||
| Child support * Relative strain | 0.03 | 0.09 | 0.01 | 0.07 | 0.00 | 0.15 |
| Step 1 | ||||||
| Child support | 0.47 | 0.06 | 0.23 ** | 0.06 | 0.06 | 39.85 ** |
| Friendship strain | 0.26 | 0.09 | 0.09 * | |||
| Step 2 | ||||||
| Child support * Friendship strain | 0.07 | 0.10 | 0.02 | 0.06 | 0.00 | 0.49 |
| Relative | ||||||
| Step 1 | ||||||
| Relative support | 0.19 | 0.05 | 0.11 ** | 0.09 | 0.09 | 55.29 ** |
| Spouse/partner strain | 0.58 | 0.06 | 0.26 ** | |||
| Step 2 | ||||||
| Relative support * Spouse/partner strain | −0.10 | 0.07 | −0.04 | 0.09 | 0.00 | 1.80 |
| Step 1 | ||||||
| Relative support | 0.19 | 0.05 | 0.11 ** | 0.04 | 0.04 | 25.57 ** |
| Child strain | 0.38 | 0.07 | 0.16 ** | |||
| Step 2 | ||||||
| Relative supsrain | 0.08 | 0.08 | 0.03 | 0.04 | 0.00 | 1.13 |
| Step 1 | ||||||
| Relative support | 0.22 | 0.05 | 0.13 ** | 0.03 | 0.03 | 18.18 ** |
| Friendship strain | 0.33 | 0.09 | 0.11 ** | |||
| Step 2 | ||||||
| Relative support * Friendship strain | 0.26 | 0.10 | 0.07 † | 0.04 | 0.01 | 6.06 † |
| Friendship | ||||||
| Step 1 | ||||||
| Friendship support | 0.28 | 0.06 | 0.14 ** | 0.10 | 0.10 | 61.38 ** |
| Spouse/partner strain | 0.58 | 0.06 | 0.26 ** | |||
| Step 2 | ||||||
| Friendship support*spouse/partner strain | 0.20 | 0.08 | 0.07 * | 0.10 | 0.01 | 6.95 * |
| Step 1 | ||||||
| Friend support | 0.29 | 0.06 | 0.15 ** | 0.05 | 0.05 | 32.07 ** |
| Child strain | 0.39 | 0.07 | 0.16 ** | |||
| Step 2 | ||||||
| Friendship support * child strain | 0.14 | 0.08 | 0.05 | 0.05 | 0.00 | 2.86 |
| Step 1 | ||||||
| Friendship support | 0.29 | 0.06 | 0.15 ** | 0.06 | 0.06 | 34.70 ** |
| Relative strain | 0.42 | 0.07 | 0.17 ** | |||
| Step 2 | ||||||
| Friendship support * Relative strain | 0.17 | 0.08 | 0.06 † | 0.06 | 0.00 | 4.25 † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mpofu, E.; Zhan, R.-F.; Yin, C.; Brock, K. Qualities of Older Adults’ Family and Friendship Relationships and Their Association with Life Satisfaction. Geriatrics 2024, 9, 49. https://doi.org/10.3390/geriatrics9020049
Mpofu E, Zhan R-F, Yin C, Brock K. Qualities of Older Adults’ Family and Friendship Relationships and Their Association with Life Satisfaction. Geriatrics. 2024; 9(2):49. https://doi.org/10.3390/geriatrics9020049
Chicago/Turabian StyleMpofu, Elias, Rong-Fang Zhan, Cheng Yin, and Kaye Brock. 2024. "Qualities of Older Adults’ Family and Friendship Relationships and Their Association with Life Satisfaction" Geriatrics 9, no. 2: 49. https://doi.org/10.3390/geriatrics9020049
APA StyleMpofu, E., Zhan, R.-F., Yin, C., & Brock, K. (2024). Qualities of Older Adults’ Family and Friendship Relationships and Their Association with Life Satisfaction. Geriatrics, 9(2), 49. https://doi.org/10.3390/geriatrics9020049