
Surgical Mortality Risk Scores in Transcatheter Aortic Valve Implantation: Is Their Early Predictive Value Still Strong?

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
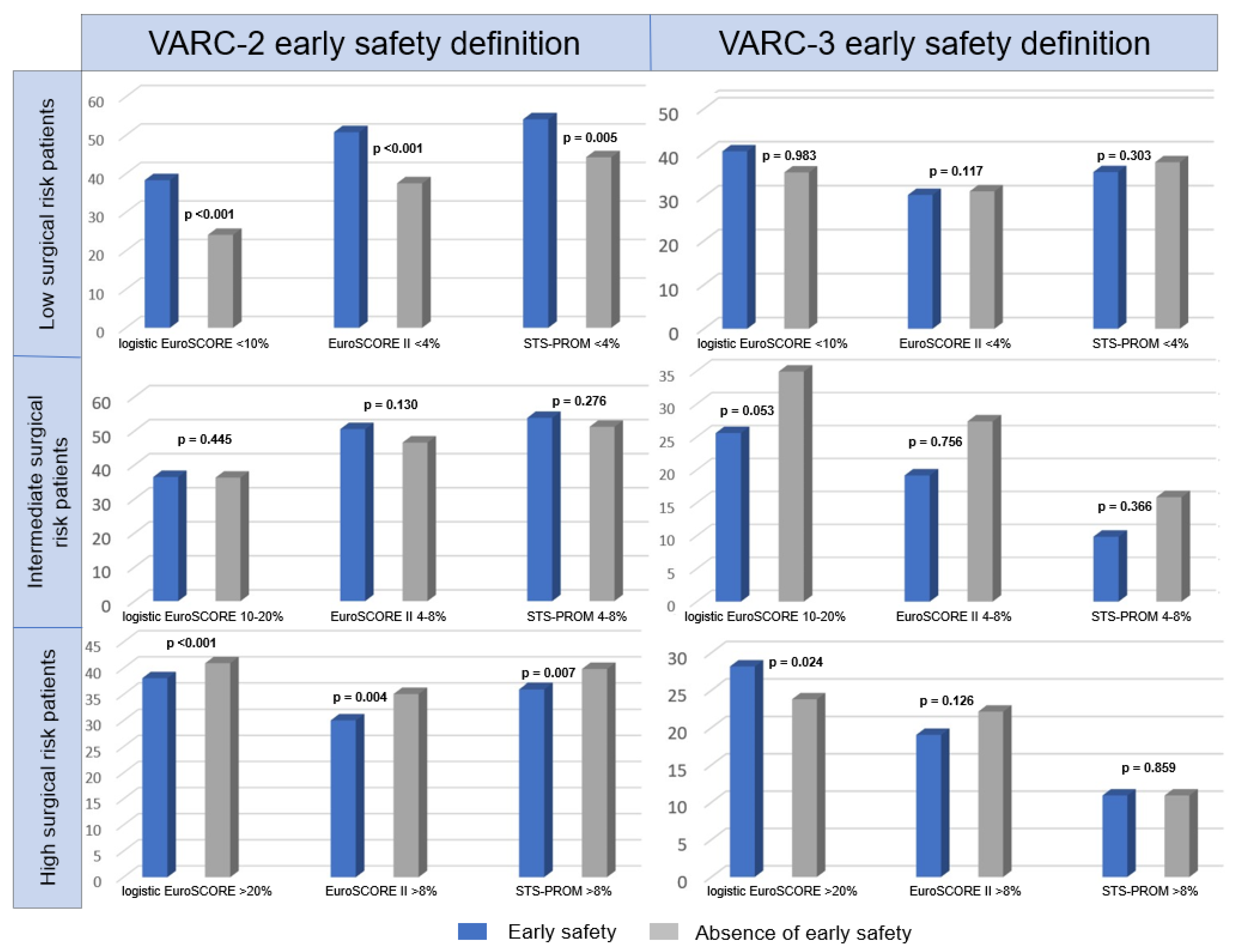
3.2. Surgical Mortality Risk Scores
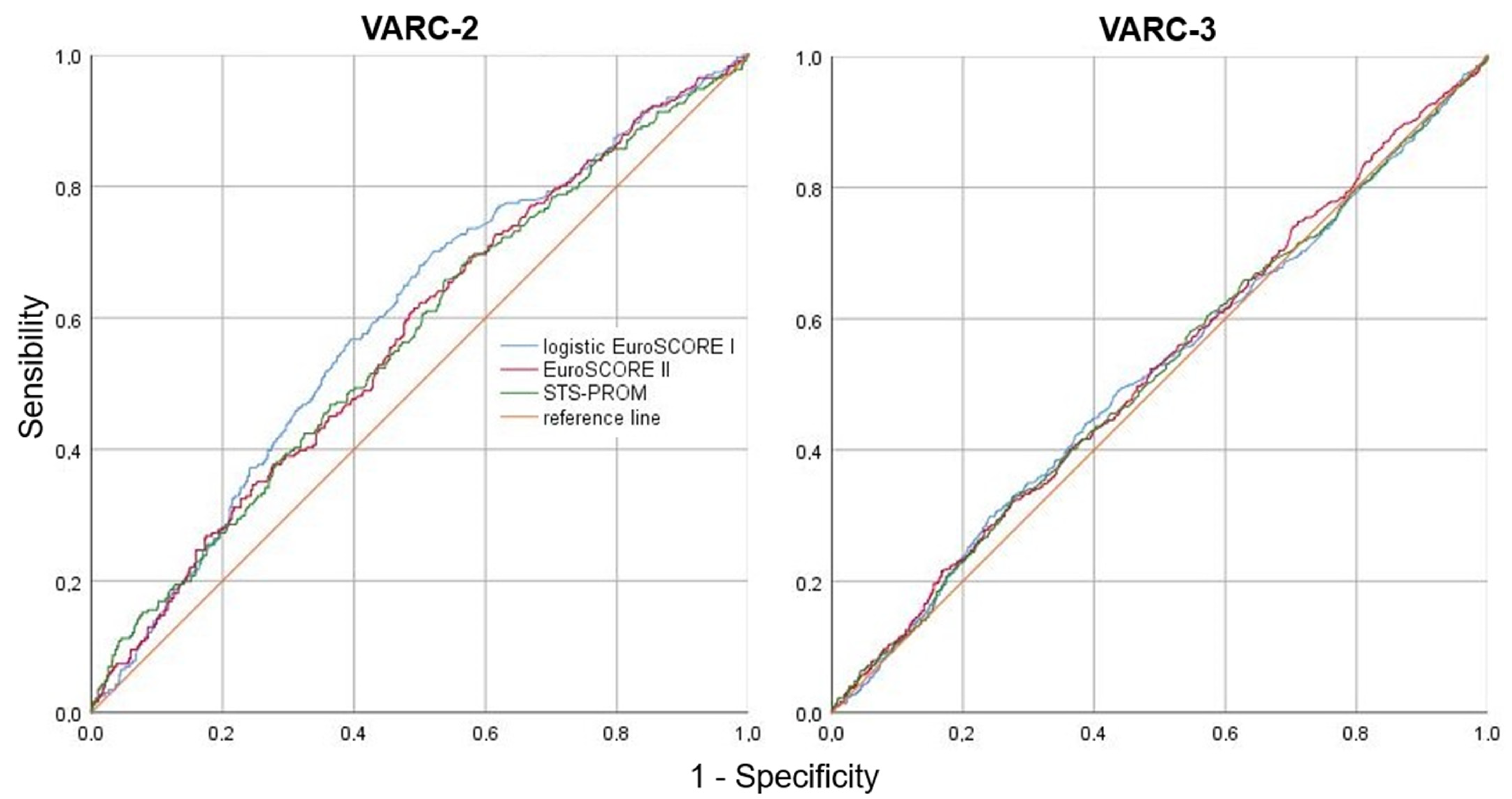
3.3. Absence of Early Safety and 1-Year Mortality Predictors
4. Discussion
4.1. Early Safety
4.2. Surgical Mortality Risk Scores and Absence of Early Safety
4.3. One-Year Mortality Predictors
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- D’Errigo, P.; Barbanti, M.; Ranucci, M.; Onorati, F.; Covello, R.D.; Rosato, S.; Tamburino, C.; Santini, F.; Santoro, G.; Seccareccia, F.; et al. Transcatheter aortic valve implantation versus surgical aortic valve replacement for severe aortic stenosis: Results from an intermediate risk propensity-matched population of the Italian OBSERVANT study. Int. J. Cardiol. 2013, 167, 1945–1952. [Google Scholar] [CrossRef] [PubMed]
- Thyregod, H.G.H.; Steinbrüchel, D.A.; Ihlemann, N.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Chang, Y.; Franzen, O.W.; Engstrøm, T.; Clemmensen, P.; et al. Transcatheter versus surgical aortic valve replacement in patients with severe aortic valve stenosis: 1-Year results from the all-comers NOTION randomized clinical trial. J. Am. Coll. Cardiol. 2015, 65, 2184–2194. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Nashef, S.A.M.; Sharples, L.D.; Roques, F.; Lockowandt, U. EuroSCORE II and the art and science of risk modelling. Eur. J. Cardio-Thorac. Surg. 2013, 43, 695–696. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease: Developed by the task force for the management of valvular heart disease of the european society of cardiology (ESC) and the European association for cardio-thoracic surgery (EACTS). Rev. Española Cardiol. 2022, 75, 524. [Google Scholar] [CrossRef]
- Nashef, S.A.; Roques, F.; Michel, P.; Gauducheau, E.; Lemeshow, S.; Salamon, R. European system for cardiac operative risk evaluation (EuroSCORE). Eur. J. Cardiothorac. Surg. 1999, 16, 9–13. [Google Scholar] [CrossRef]
- Roques, F.; Nashef, S.A.; Michel, P.; Gauducheau, E.; de Vincentiis, C.; Baudet, E.; Cortina, J.; David, M.; Faichney, A.; Gabrielle, F.; et al. Risk factors and outcome in European cardiac surgery: Analysis of the EuroSCORE multinational database of 19,030 patients. Eur. J. Cardio-Thorac. Surg. 1999, 15, 816–822, discussion 822–823. [Google Scholar] [CrossRef]
- O’Brien, S.M.; Shahian, D.M.; Filardo, G.; Ferraris, V.A.; Haan, C.K.; Rich, J.B.; Normand, S.-L.T.; DeLong, E.R.; Shewan, C.M.; Dokholyan, R.S.; et al. The society of thoracic surgeons 2008 cardiac surgery risk models: Part 2—Isolated valve surgery. Ann Thorac. Surg. 2009, 88, S23–S42. [Google Scholar] [CrossRef]
- Shahian, D.M.; O’Brien, S.M.; Filardo, G.; Ferraris, V.A.; Haan, C.K.; Rich, J.B.; Normand, S.-L.T.; DeLong, E.R.; Shewan, C.M.; Dokholyan, R.S.; et al. The society of thoracic surgeons 2008 cardiac surgery risk models: Part 3—Valve plus coronary artery bypass grafting surgery. Ann. Thorac. Surg. 2009, 88, S43–S62. [Google Scholar] [CrossRef] [PubMed]
- Wendt, D.; Thielmann, M.; Kahlert, P.; Kastner, S.; Price, V.; Al-Rashid, F.; Patsalis, P.; Erbel, R.; Jakob, H. Comparison between different risk scoring algorithms on isolated conventional or transcatheter aortic valve replacement. Ann. Thorac. Surg. 2014, 97, 796–802. [Google Scholar] [CrossRef]
- Compagnone, M.; Moretti, C.; Marcelli, C.; Taglieri, N.; Ghetti, G.; Corsini, A.; Bruno, M.; Bruno, A.G.; Orzalkiewicz, M.; Marrozzini, C.; et al. Surgical risk scores applied to transcatheter aortic valve implantation: Friends or foes? Short-term and long-term outcomes from a single-center registry. J. Invasive Cardiol. 2019, 31, 7. [Google Scholar]
- Arangalage, D.; Cimadevilla, C.; Alkhoder, S.; Chiampan, A.; Himbert, D.; Brochet, E.; Iung, B.; Nataf, P.; Depoix, J.-P.; Vahanian, A.; et al. Agreement between the new EuroSCORE II, the logistic EuroSCORE and the society of thoracic surgeons score: Implications for transcatheter aortic valve implantation. Arch. Cardiovasc. Dis. 2014, 107, 353–360. [Google Scholar] [CrossRef]
- Leon, M.B.; Piazza, N.; Nikolsky, E.; Blackstone, E.H.; Cutlip, D.E.; Kappetein, A.P.; Krucoff, M.W.; Mack, M.; Mehran, R.; Miller, C.; et al. Standardized endpoint definitions for transcatheter aortic valve implantation clinical trials: A consensus report from the valve academic research consortium. Eur. Heart J. 2011, 32, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.-A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The valve academic research consortium-2 consensus document (VARC-2). Eur. J. Cardio-Thorac. Surg. 2012, 42, S45–S60. [Google Scholar] [CrossRef]
- VARC-3 Writing Committee; Généreux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; et al. Valve academic research consortium 3: Updated endpoint definitions for aortic valve clinical research. Eur. Heart J. 2021, 42, 1825–1857. [Google Scholar] [CrossRef]
- van Ginkel, D.J.; Brouwer, J.; van Hemert, N.D.; Kraaijeveld, A.O.; Rensing, B.J.W.M.; Swaans, M.J.; Timmers, L.; Voskuil, M.; Stella, P.R.; Ten Berg, J.M. Major threats to early safety after transcatheter aortic valve implantation in a contemporary cohort of real-world patients. Neth. Heart J. 2021, 29, 632–642. [Google Scholar] [CrossRef]
- Fraccaro, C.; Testa, L.; Schiavo, A.; Brambilla, N.; Napodano, M.; Azzolina, D.; Bedogni, F.; Tarantini, G. Transcatheter aortic valve implantation in patients younger than 75 years: Guidelines-based patients selection and clinical outcome. Int. J. Cardiol. 2018, 272, 273–278. [Google Scholar] [CrossRef]
- Costa, G.; Saia, F.; Pilgrim, T.; Abdel-Wahab, M.; Garot, P.; Valvo, R.; Gandolfo, C.; Branca, L.; Latib, A.; Santos, I.A.; et al. Transcatheter aortic valve replacement with the latest-iteration self-expanding or balloon-expandable valves: The multicenter OPERA-TAVI registry. JACC Cardiovasc. Interv. 2022, 15, S1936879822017101. [Google Scholar] [CrossRef]
- Iacovelli, F.; Pignatelli, A.; Cafaro, A.; Stabile, E.; Salemme, L.; Cioppa, A.; Pucciarelli, A.; Spione, F.; Loizzi, F.; Cillis, E.D.; et al. Impact of contrast medium osmolality on the risk of acute kidney injury after transcatheter aortic valve implantation: Insights from the magna graecia TAVI registry. Int. J. Cardiol. 2021, 329, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Vontobel, J.; Possner, M.; Schütz, P.; Müller, B.; Taramasso, M.; Binder, R.K.; Haueis, S.; Attinger-Toller, A.; Maisano, F.; Nietlispach, F. Early safety outcome following transcatheter aortic valve implantation: Is the amount of contrast media used a matter of concern? Swiss Med. Wkly. 2015, 145, w14238. [Google Scholar] [CrossRef] [PubMed]
- Yatsynovich, Y.; Khattak, H.; Ali, M.; Schwartz, B.; Pak, S.; Chen, T. Comparison of transcatheter aortic valve replacement risk score against currently accepted surgical risk models as predictors of 30-day mortality in transcatheter aortic valve replacement. J. Interv. Cardiol. 2017, 30, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Beohar, N.; Whisenant, B.; Kirtane, A.J.; Leon, M.B.; Tuzcu, E.M.; Makkar, R.; Svensson, L.G.; Miller, D.C.; Smith, C.R.; Pichard, A.D.; et al. The relative performance characteristics of the logistic European system for cardiac operative risk evaluation score and the society of thoracic surgeons score in the placement of aortic transcatheter valves trial. J. Thorac. Cardiovasc. Surg. 2014, 148, 2830.e1–2837.e1. [Google Scholar] [CrossRef] [PubMed]
- Vanhuyse, F.; Maureira, P.; Folliguet, T.; Villemot, J.P. Predictive value of five risk scores to predict outcomes after aortic valve replacement in octogenarians. J. Heart Valve Dis. 2013, 22, 517–523. [Google Scholar]
- Balan, P.; Zhao, Y.; Johnson, S.; Dhoble, A.; Estrera, A.; Smalling, R.; Nguyen, T.C. The society of thoracic surgery risk score as a predictor of 30-day mortality in transcatheter vs. surgical aortic valve replacement: A single-center experience and its implications for the development of a TAVR risk-prediction model. J. Invasive Cardiol. 2017, 29, 109–114. [Google Scholar]
- Ishizu, K.; Shirai, S.; Isotani, A.; Hayashi, M.; Kawaguchi, T.; Taniguchi, T.; Ando, K.; Yashima, F.; Tada, N.; Yamawaki, M.; et al. Long-term prognostic value of the society of thoracic surgery risk score in patients undergoing transcatheter aortic valve implantation (from the OCEAN-TAVI registry). Am. J. Cardiol. 2021, 149, 86–94. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | All | VARC-2 Early Safety | p | VARC-3 Early Safety | p | ||
|---|---|---|---|---|---|---|---|
| Yes (n = 1515) | No (n = 248) | Yes (n = 1050) | No (n = 713) | ||||
| Patient characteristics | |||||||
| Age (years) | 80.94 ± 5.73 | 80.95 ± 5.63 | 80.90 ± 6.34 | 0.361 | 80.76 ± 5.62 | 81.21 ± 5.90 | 0.030 |
| Female | 982 (55.70%) | 836 (55.18%) | 146 (58.87%) | 0.310 | 587 (55.90%) | 395 (55.40%) | 0.872 |
| Body Surface Area (m2) | 1.75 ± 0.17 | 1.76 ± 0.17 | 1.73 ± 0.19 | 0.018 | 1.76 ± 0.17 | 1.75 ± 0.17 | 0.100 |
| Mortality risk scores | |||||||
| Logistic EuroSCORE (%) | 16.21 ± 12.41 | 15.78 ± 12.23 | 18.92 ± 13.23 | <0.001 | 16.02 ± 12.40 | 16.51 ± 12.43 | 0.334 |
| <10 | 617/1695 (36.40%) | 561/1463 (38.35%) | 56/232 (24.14%) | <0.001 | 376/1031 (36.47%) | 241/664 (36.29%) | 0.983 |
| 10–20 | 652/1695 (38.47%) | 557/1463 (38.07%) | 95/232 (40.95%) | 0.445 | 416/1031 (40.35%) | 236/664 (35.54%) | 0.053 |
| ≥20 | 426/1695 (25.13%) | 345/1463 (23.58%) | 81/232 (34.91%) | <0.001 | 239/1031 (23.18%) | 187/664 (28.16%) | 0.024 |
| EuroSCORE II (%) | 5.91 ± 5.83 | 5.72 ± 5.59 | 7.05 ± 7.02 | <0.001 | 5.70 ± 5.39 | 6.21 ± 6.42 | 0.097 |
| <4 | 856/1749 (48.94%) | 764/1504 (50.80%) | 92/245 (37.55%) | <0.001 | 528/1045 (50.53%) | 328/704 (46.59%) | 0.117 |
| 4–8 | 538/1749 (30.76%) | 452/1504 (30.05%) | 86/245 (35.10%) | 0.130 | 318/1045 (30.43%) | 220/704 (31.25%) | 0.756 |
| ≥8 | 355/1749 (20.30%) | 288/1504 (19.15%) | 67/245 (27.35%) | 0.004 | 199/1045 (19.04%) | 156/704 (22.16%) | 0.126 |
| STS-PROM (%) | 4.73 ± 3.56 | 4.57 ± 3.10 | 5.71 ± 5.49 | <0.001 | 4.60 ± 3.07 | 4.93 ± 4.16 | 0.177 |
| <4 | 923/1749 (52.78%) | 814/1503 (54.16%) | 109/246 (44.31%) | 0.005 | 562/1044 (53.83%) | 361/705 (51.21%) | 0.303 |
| 4–8 | 639/1749 (36.53%) | 541/1503 (35.99%) | 98/246 (39.84%) | 0.276 | 372/1044 (35.63%) | 267/705 (37.87%) | 0.366 |
| ≥8 | 187/1749 (10.69%) | 148/1503 (9.85%) | 39/246 (15.85%) | 0.007 | 110/1044 (10.54%) | 77/705 (10.92%) | 0.859 |
| Procedural details | |||||||
| Valve-in-valve | 79 (4.48%) | 60 (3.96%) | 19 (7.66%) | 0.014 | 48 (4.57%) | 31 (4.35%) | 0.916 |
| Predilation | 828/1751 (47.29%) | 712/1505 (47.31%) | 116/246 (47.15%) | 0.981 | 475/1043 (45.54%) | 353/708 (49.86%) | 0.084 |
| Valve substitute | |||||||
| Balloon-expandable | 578 (32.79%) | 511 (33.73%) | 67 (27.02%) | 0.044 | 396 (37.71%) | 182 (25.53%) | <0.001 |
| Self-expanding | 1097 (62.22%) | 935 (61.72%) | 162 (65.32%) | 0.310 | 601 (57.24%) | 496 (69.56%) | <0.001 |
| Others | 88 (4.99%) | 69 (4.55%) | 19 (7.66%) | 0.054 | 53 (5.05%) | 35 (4.91%) | 0.984 |
| Valve size ≤ 26 mm | 1079 (61.20%) | 934 (61.65%) | 145 (58.47%) | 0.377 | 685 (65.24%) | 394 (55.26%) | <0.001 |
| Postdilation | 449/1755 (25.58%) | 361/1508 (23.94%) | 88/247 (35.63%) | <0.001 | 222/1047 (21.20%) | 227/708 (32.06%) | <0.001 |
| Fluoroscopy time (min) | 23.94 ± 15.97 | 22.60 ± 12.72 | 32.61 ± 27.86 | <0.001 | 22.42 ± 13.03 | 26.42 ± 19.61 | 0.018 |
| Radiation dose (mGy) | 1151.20 ± 866.71 | 1103.30 ± 756.78 | 1490.40 ± 1378.69 | 0.007 | 1099.49 ± 778.35 | 1237.11 ± 991.67 | 0.037 |
| Procedural time (min) | 93.35 ± 31.54 | 91.13 ± 29.51 | 104.79 ± 38.95 | 0.026 | 91.31 ± 28.88 | 95.31 ± 33.93 | 0.398 |
| LOCM | 1312/1747 (75.10%) | 1124/1503 (74.78%) | 188/244 (77.05%) | 0.497 | 751/1044 (71.93%) | 561/703 (79.80%) | <0.001 |
| CM volume (mL) | 149.85 ± 72.43 | 145.15 ± 65.77 | 178.82 ± 99.93 | <0.001 | 144.17 ± 65.92 | 158.25 ± 80.44 | <0.001 |
| Other complications and outcomes | |||||||
| Permanent pacemaker implantation | 210/1538 (13.65%) | 170/1330 (12.78%) | 40/208 (19.23%) | 0.016 | 0/907 (0.00%) | 210/631 (33.28%) | <0.001 |
| New-onset LBBB | 518 (29.38%) | 445 (29.37%) | 73 (29.43%) | 0.956 | 311 (29.62%) | 207 (29.03%) | 0.832 |
| New-onset atrial fibrillation | 140/1425 (9.82%) | 105/1235 (8.50%) | 35/190 (18.42%) | <0.001 | 67/855 (7.84%) | 73/570 (12.81%) | 0.003 |
| Post-TAVI hospital length of stay (days) | 5.64 ± 4.21 | 5.27 ± 3.77 | 8.48 ± 5.94 | <0.001 | 4.67 ± 2.63 | 7.17 ± 5.78 | <0.001 |
| 1-year mortality | 64 (3.63%) | 46 (3.04%) | 18 (7.26%) | 0.002 | 29 (2.76%) | 35 (4.91%) | 0.025 |
| AUC (DeLong Standard Error) | 95% CI | Asymptotic Significance | CL | Slope | Cutoff | Youden Index | Sensitivity (%) | Specificity (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Absence of early safety (VARC-2) | |||||||||
| Logistic EuroSCORE (%) | 0.595 ± 0.020 | 0.571–0.618 | <0.001 | 0.00 | 1.000 | 11.36 ± 0.03 | 0.177 | 70 | 48 |
| EuroSCORE II (%) | 0.578 ± 0.019 | 0.554–0.601 | <0.001 | −0.00 | 1.000 | 3.97 ± 0.03 | 0.139 | 63 | 51 |
| STS-PROM (%) | 0.575 ± 0.020 | 0.552–0.598 | <0.001 | 0.00 | 1.000 | 3.53 ± 0.03 | 0.125 | 66 | 46 |
| Absence of early safety (VARC-3) | |||||||||
| Logistic EuroSCORE (%) | 0.514 ± 0.014 | 0.490–0.538 | 0.334 | −0.00 | 1.000 | 19.41 ± 0.02 | 0.057 | 30 | 76 |
| EuroSCORE II (%) | 0.523 ± 0.014 | 0.499–0.547 | 0.097 | 0.00 | 1.000 | 4.02 ± 0.02 | 0.046 | 53 | 51 |
| STS-PROM (%) | 0.519 ± 0.014 | 0.495–0.543 | 0.177 | 0.00 | 1.000 | 5.21 ± 0.02 | 0.058 | 33 | 75 |
| 1-year mortality | |||||||||
| Number of complications | 0.646 ± 0.040 | 0.624–0.669 | <0.001 | −0.00 | 1.000 | 1 ± 0.062 | 0.395 | 53 | 86 |
| Predictors | Absence of Early Safety (VARC-2) | Absence of Early Safety (VARC-3) | 1-Year Mortality | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariable OR (95% CI) | p | Multivariable OR (95% CI) | p | Univariable OR (95% CI) | p | Multivariable OR (95% CI) | p | Univariable OR (95% CI) | p | Multivariable OR (95% CI) | p | |
| Body Surface Area | 0.333 (0.150–0.738) | 0.007 | 0.626 (0.359–1.094) | 0.100 | ||||||||
| PAD | 1.499 (1.122–2.002) | 0.006 | 1.477 (0.749–2.915) | 0.260 | 1.094 (0.882–1.358) | 0.415 | ||||||
| Pulmonary arterial systolic pressure | 1.014 (1.004–1.024) | 0.006 | 1.003 (0.996–1.011) | 0.402 | ||||||||
| Logistic EuroSCORE | 1.018 (1.008–1.027) | <0.001 | 1.003 (0.995–1.011) | 0.433 | 1.028 (1.013–1.043) | <0.001 | ||||||
| EuroSCORE II | 1.032 (1.012–1.052) | <0.001 | 1.012 (0.946–1.082) | 0.734 | 1.015 (0.999–1.032) | 0.074 | 1.066 (1.039–1.093) | <0.001 | 1.060 (1.013–1.108) | 0.011 | ||
| STS-PROM | 1.072 (1.038–1.108) | <0.001 | 1.077 (0.958–1.212) | 0.214 | 1.026 (0.999–1.054) | 0.062 | 1.087 (1.041–1.134) | <0.001 | 1.055 (0.969–1.148) | 0.217 | ||
| Valve-in-valve | 2.012 (1.179–3.433) | 0.010 | 0.356 (0.043–2.948) | 0.338 | 0.949 (0.598–1.506) | 0.824 | ||||||
| Self-expanding prosthesis | 1.169 (0.882–1.548) | 0.278 | 1.708 (1.397–2.088) | <0.001 | 0.978 (0.615–1.555) | 0.925 | 0.225 (0.129–0.3919 | <0.001 | 0.270 (0.143–0.509) | <0.001 | ||
| Postdilation | 1.758 (1.321–2.341) | <0.001 | 1.962 (1.042–3.695) | 0.037 | 1.754 (1.412–2.178) | <0.001 | 1.284 (0.803–2.052) | 0.296 | ||||
| Fluoroscopy time (min) | 1.031 (1.020–1.042) | <0.001 | 1.014 (0.995–1.033) | 0.160 | 1.017 (1.008–1.026) | <0.001 | 1.010 (0.994–1.026) | 0.212 | ||||
| Radiation dose (mGy) | 1.000 (1.000–1.001) | <0.001 | 1.000 (0.999–1.000) | 0.121 | 1.000 (1.000–1.000) | 0.025 | 1.000 (0.999–1.000) | 0.877 | ||||
| Procedural time (min) | 1.013 (1.002–1.023) | 0.016 | 1.004 (0.996–1.012) | 0.333 | ||||||||
| LOCM | 1.132 (0.822–1.559) | 0.448 | 1.541 (1.227–1.937) | <0.001 | 2.876 (1.582–5.228) | 0.001 | ||||||
| CM volume | 1.005 (1.004–1.007) | <0.001 | 1.003 (1.001–1.004) | <0.001 | 1.004 (1.001–1.006) | 0.013 | 1.002 (0.999–1.006) | 0.230 | ||||
| Number of complications | 1.956 (1.578–2.425) | <0.001 | ||||||||||
| New-onset LBBB | 0.434 (0.219–0.852) | 0.017 | 0.513 (0.242–1.088) | 0.082 | ||||||||
| New-onset atrial fibrillation | 2.430 (1.600–3.690) | <0.001 | 3.220 (1.536–6.750) | 0.002 | 1.727 (1.217–2.452) | 0.002 | 1.338 (0.728–2.457) | 0.348 | 2.654 (1.329–5.299) | 0.006 | 2.558 (1.213–5.392) | 0.014 |
| Absence of early safety (VARC-2) | 2.499 (1.424–4.386) | 0.001 | 2.263 (1.021–5.018) | 0.044 | ||||||||
| Absence of early safety (VARC-3) | 1.817 (1.101–3.001) | 0.020 | 1.638 (0.793–3.383) | 0.182 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iacovelli, F.; Loizzi, F.; Cafaro, A.; Burattini, O.; Salemme, L.; Cioppa, A.; Rizzo, F.; Palmitessa, C.; D’Alessandro, M.; De Feo, D.; et al. Surgical Mortality Risk Scores in Transcatheter Aortic Valve Implantation: Is Their Early Predictive Value Still Strong? J. Cardiovasc. Dev. Dis. 2023, 10, 244. https://doi.org/10.3390/jcdd10060244
Iacovelli F, Loizzi F, Cafaro A, Burattini O, Salemme L, Cioppa A, Rizzo F, Palmitessa C, D’Alessandro M, De Feo D, et al. Surgical Mortality Risk Scores in Transcatheter Aortic Valve Implantation: Is Their Early Predictive Value Still Strong? Journal of Cardiovascular Development and Disease. 2023; 10(6):244. https://doi.org/10.3390/jcdd10060244
Chicago/Turabian StyleIacovelli, Fortunato, Francesco Loizzi, Alessandro Cafaro, Osvaldo Burattini, Luigi Salemme, Angelo Cioppa, Francesco Rizzo, Chiara Palmitessa, Maurizio D’Alessandro, Daniele De Feo, and et al. 2023. "Surgical Mortality Risk Scores in Transcatheter Aortic Valve Implantation: Is Their Early Predictive Value Still Strong?" Journal of Cardiovascular Development and Disease 10, no. 6: 244. https://doi.org/10.3390/jcdd10060244
APA StyleIacovelli, F., Loizzi, F., Cafaro, A., Burattini, O., Salemme, L., Cioppa, A., Rizzo, F., Palmitessa, C., D’Alessandro, M., De Feo, D., Pucciarelli, A., De Cillis, E., Pestrichella, V., Contegiacomo, G., Tesorio, T., & Bortone, A. S. (2023). Surgical Mortality Risk Scores in Transcatheter Aortic Valve Implantation: Is Their Early Predictive Value Still Strong? Journal of Cardiovascular Development and Disease, 10(6), 244. https://doi.org/10.3390/jcdd10060244