
Assessment of Esophageal Shifts during Catheter Ablation of Atrial Fibrillation Using Intracardiac Ultrasound Integrated with 3-Dimensional Electroanatomical Mapping System

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Populations
2.2. Ablation Procedure and Mapping Protocol
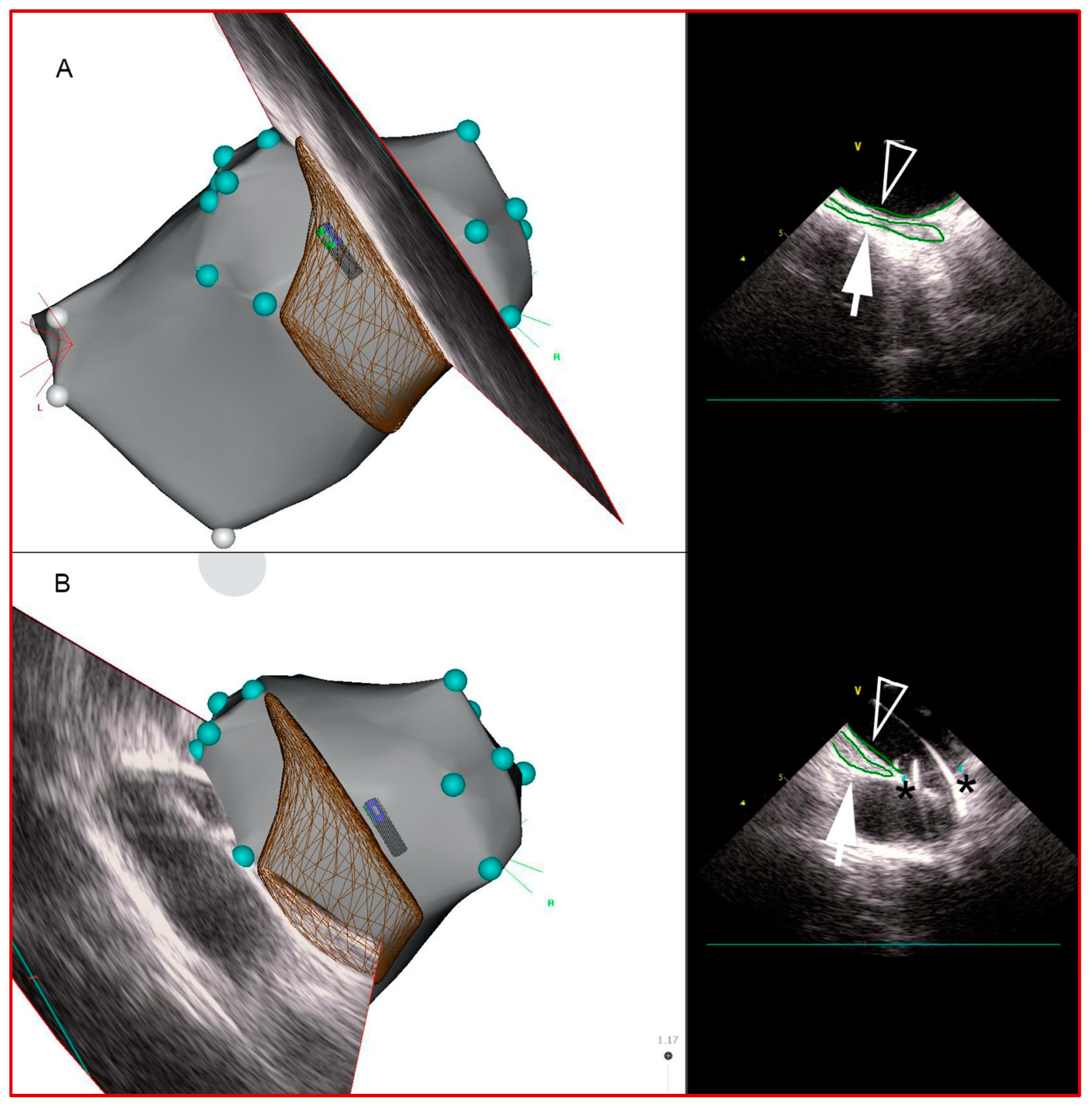
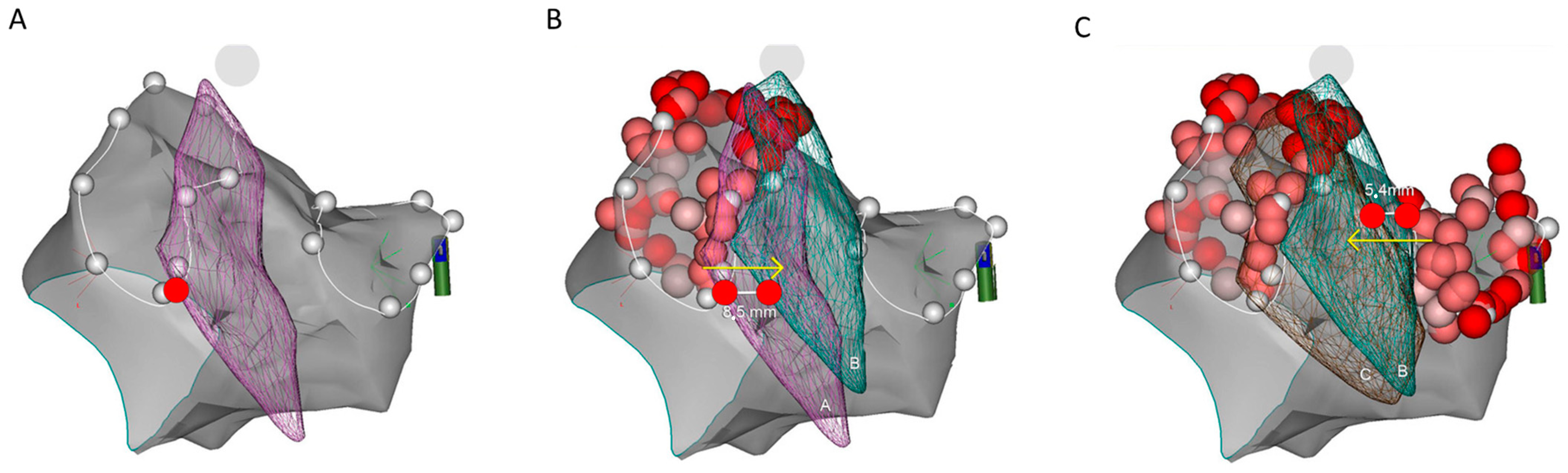
2.3. Esophageal Course Assessment and Data Analysis
2.4. Statistical Analysis
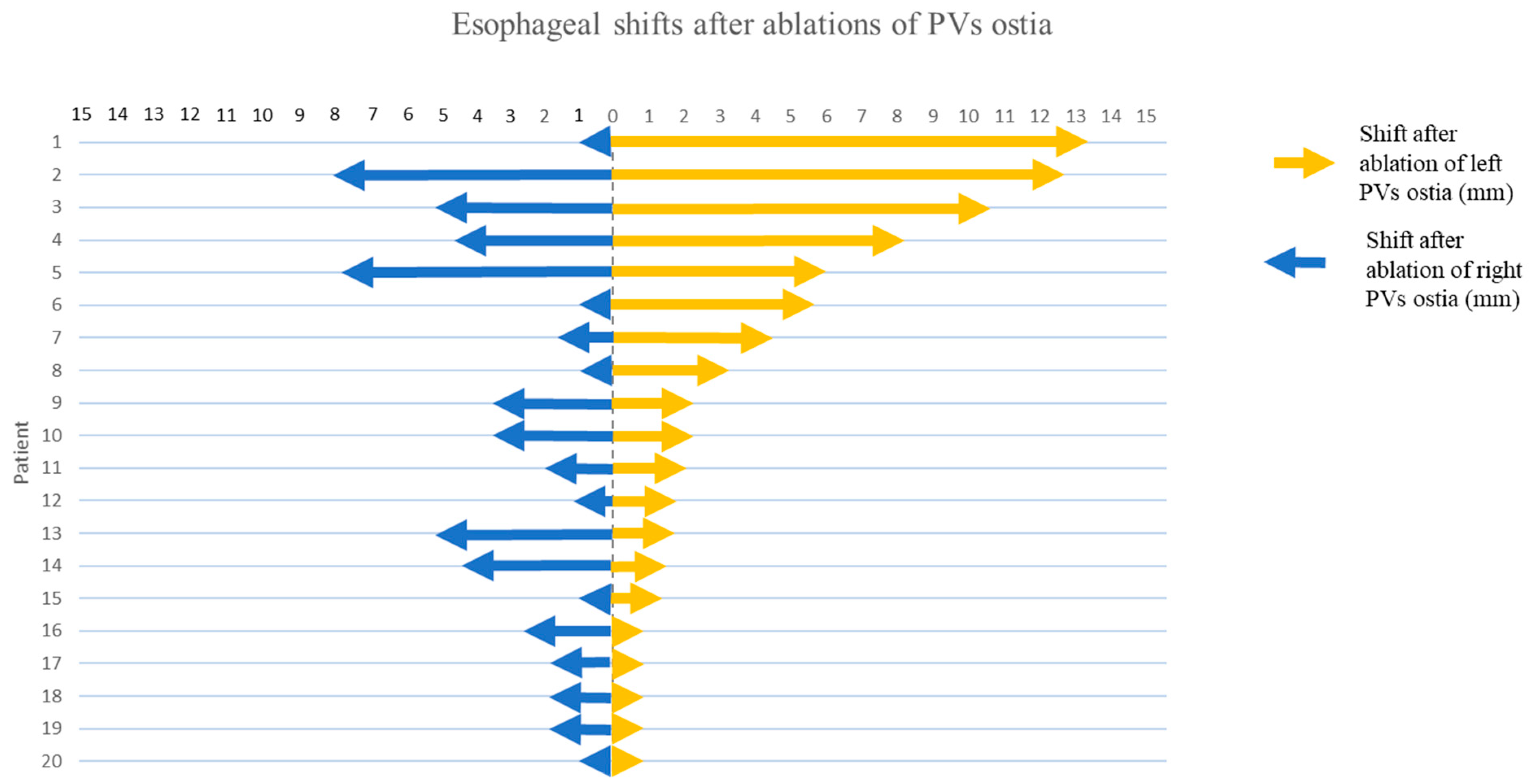
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed]
- Pappone, C.; Oral, H.; Santinelli, V.; Vicedomini, G.; Lang, C.C.; Manguso, F.; Torracca, L.; Benussi, S.; Alfieri, O.; Hong, R.; et al. Atrio-Esophageal Fistula as a Complication of Percutaneous Transcatheter Ablation of Atrial Fibrillation. Circulation 2004, 109, 2724–2726. [Google Scholar] [CrossRef] [PubMed]
- Cappato, R.; Calkins, H.; Chen, S.A.; Davies, W.; Iesaka, Y.; Kalman, J.; Kim, Y.H.; Klein, G.; Natale, A.; Packer, D.; et al. Prevalence and Causes of Fatal Outcome in Catheter Ablation of Atrial Fibrillation. J. Am. Coll. Cardiol. 2009, 53, 1798–1803. [Google Scholar] [CrossRef] [PubMed]
- Mönnig, G.; Wessling, J.; Juergens, K.U.; Milberg, P.; Ribbing, M.; Fischbach, R.; Wiekowski, J.; Breithardt, G.; Eckardt, L. Further evidence of a close anatomical relation between the oesophagus and pulmonary veins. Europace 2005, 7, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Orlov, M.V.; Hoffmeister, P.; Chaudhry, G.M.; Almasry, I.; Gijsbers, G.H.; Swack, T.; Haffajee, C.I. Three-dimensional rotational angiography of the left atrium and esophagus—A virtual computed tomography scan in the electrophysiology lab? Heart Rhythm 2007, 4, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Gavin, A.R.; Singleton, C.B.; McGavigan, A.D. Assessment of oesophageal position by direct visualization with luminal contrast compared with segmentation from pre-acquired computed tomography scan-implications for ablation strategy. Europace 2014, 16, 1304–1308. [Google Scholar] [CrossRef] [PubMed]
- Wilson, L.; Brooks, A.G.; Lau, D.H.; Dimitri, H.; Sharma, G.; Lim, H.S.; Alasady, M.; Young, G.D.; Sanders, P. Real-time CartoSound imaging of the esophagus: A comparison to computed tomography. Int. J. Cardiol. 2012, 157, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Piorkowski, C.; Hindricks, G.; Schreiber, D.; Tanner, H.; Weise, W.; Koch, A.; Gerds-Li, J.H.; Kottkamp, H. Electroanatomic reconstruction of the left atrium, pulmonary veins, and esophagus compared with the “true anatomy” on multislice computed tomography in patients undergoing catheter ablation of atrial fibrillation. Heart Rhythm 2006, 3, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Good, E.; Oral, H.; Lemola, K.; Han, J.; Tamirisa, K.; Igic, P.; Elmouchi, D.; Tschopp, D.; Reich, S.; Chugh, A.; et al. Movement of the Esophagus during Left Atrial Catheter Ablation for Atrial Fibrillation. J. Am. Coll. Cardiol. 2005, 46, 2107–2110. [Google Scholar] [CrossRef]
- Daoud, E.G.; Hummel, J.D.; Houmsse, M.; Hart, D.T.; Weiss, R.; Liu, Z.; Augostini, R.; Kalbfleisch, S.; Smith, M.C.; Mehta, R.; et al. Comparison of computed tomography imaging with intraprocedural contrast esophagram: Implications for catheter ablation of atrial fibrillation. Heart Rhythm 2008, 5, 975–980. [Google Scholar] [CrossRef]
- Sherzer, A.I.; Feigenblum, D.Y.; Kulkarni, S.; Pina, J.W.; Casey, J.L.; Salka, K.A.; Simons, G.R. Continuous Nonfluoroscopic Localization of the Esophagus During Radiofrequency Catheter Ablation of Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2007, 18, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Callans, D.J.; Marchlinski, F.E.; Stiffler, J.A.; Sadek, M.M.; Supple, G.E. 3D Intracardiac Echocardiography/CartoSoundTM Imaging of Esophagus Guided Left Atrial Posterior Wall Ablation for Atrial Fibrillation. J. Atr. Fibrillation 2014, 7, 1184. [Google Scholar] [PubMed]
- Phlips, T.; Taghji, P.; El Haddad, M.; Wolf, M.; Knecht, S.; Vandekerckhove, Y.; Tavernier, R.; Duytschaever, M. Improving procedural and one-year outcome after contact force-guided pulmonary vein isolation: The role of interlesion distance, ablation index, and contact force variability in the ‘CLOSE’-protocol. Europace 2018, 20, f419–f427. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2017, 14, e275–e444. [Google Scholar] [CrossRef] [PubMed]
- Winship, D.H.; De Andrade, S.R.V.; Zboralske, F.F. Influence of bolus temperature on human esophageal motor function. J. Clin. Investig. 1970, 49, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Paterson, W.G. Esophageal Peristalsis. GI Motility Online. 2006. Available online: http://www.nature.com/gimo/contents/pt1/full/gimo13.html (accessed on 16 May 2006).
- Maenosono, R.; Oketani, N.; Ishida, S.; Iriki, Y.; Ichiki, H.; Okui, H.; Ninomiya, Y.; Hamasaki, S.; Namino, F.; Matsushita, M.; et al. Effectiveness of esophagus detection by three-dimensional electroanatomical mapping to avoid esophageal injury during ablation of atrial fibrillation. J. Cardiol. 2012, 60, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Summerton, S.L. Radiographic Evaluation of Esophageal Function. Gastrointest. Endosc. Clin. N. Am. 2005, 15, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R.K.; Chaudhury, A. Physiology of Normal Esophageal Motility. J. Clin. Gastroenterol. 2008, 42, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Kettering, K.; Yim, D.-H.; Benz, A.; Gramley, F. Catheter ablation of paroxysmal atrial fibrillation: Circumferential pulmonary vein ablation: Success rates with and without exclusion of areas adjacent to the esophagus. Clin. Res. Cardiol. Off J. Ger. Card. Soc. 2017, 106, 743–751. [Google Scholar] [CrossRef]
- Ye, Y.; Chen, S.Q.; Lu, Y.F.; Jiang, R.H.; Liu, Q.; Sheng, X.; Zhang, Z.; Sun, Y.X.; Zhang, P.; Yu, L.; et al. PV isolation guided by esophageal visualization with a tailored ablation strategy for the avoidance of esophageal thermal injury: A randomized trial. J. Interv. Card. Electrophysiol. 2020, 58, 219–227. [Google Scholar] [CrossRef]
- Sanchez, J.; Woods, C.; Zagrodzky, J.; Nazari, J.; Singleton, M.J.; Schricker, A.; Ruppert, A.; Brumback, B.; Jenny, B.; Athill, C.; et al. Atrioesophageal Fistula Rates Before and After Adoption of Active Esophageal Cooling During Atrial Fibrillation Ablation. JACC Clin. Electrophysiol. 2023, 9, 2558–2570. [Google Scholar] [CrossRef]
- Leung, L.W.; Bajpai, A.; Zuberi, Z.; Li, A.; Norman, M.; Kaba, R.A.; Akhtar, Z.; Evranos, B.; Gonna, H.; Harding, I.; et al. Randomized comparison of oesophageal protection with a temperature control device: Results of the IMPACT study. Europace 2021, 23, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.; Nazari, J.; Zagrodzky, J.; Brumback, B.; Sherman, J.; Zagrodzky, W.; Bailey, S.; Kulstad, E.; Metzl, M. Improved 1-year outcomes after active cooling during left atrial radiofrequency ablation. J. Interv. Card. Electrophysiol. 2023, 66, 1621–1629. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.; Sherman, J.; Ro, A.; Fisher, W.G.; Nazari, J.; Metzl, M. Procedural time reduction associated with active esophageal cooling during pulmonary vein isolation. J. Interv. Card. Electrophysiol. 2022, 65, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Osorio, J.; Nair, D.; Aguinaga, L.; Arabia, L.; Alcivar, D.; Al-Ahmad, A.; Tomassoni, G.; Kahaly, O.; Mehta, R.; et al. EsophAguS Deviation During RadiofrequencY Ablation of Atrial Fibrillation: The EASY AF Trial. JACC Clin. Electrophysiol. 2024, 10, 68–78. [Google Scholar] [CrossRef]
- Aupperle, H.; Doll, N.; Walther, T.; Kornherr, P.; Ullmann, C.; Schoon, H.A.; Mohr, F.W. Ablation of atrial fibrillation and esophageal injury: Effects of energy source and ablation technique. J. Thorac. Cardiovasc. Surg. 2005, 130, 1549–1554. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Patient Characteristics | |
|---|---|
| Number of patients | 20 |
| Age (years) | 61.0 (51.8–66.0) |
| Male | 17 (85%) |
| Body mass index (kg/m2) | 27.7 (24.8–31.7) |
| Atrial fibrillation type (%): | |
| Paroxysmal | 75% |
| Persistent | 25% |
| Concomitant CTI dependent atrial flutter (%) | 35% |
| Antiarrhythmic drugs (%): | |
| Beta blockers | 50% |
| Propafenone | 15% |
| Sotalol | 10% |
| Amiodarone | 35% |
| LAVI * | 45 mL/m2 * (43–50) |
| Procedural time (“skin to skin”) | 223.68 min (187.5–255) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pernat, A.; Zavrtanik, M.; Robles, A.G.; Romano, S.; Sciarra, L.; Antolič, B. Assessment of Esophageal Shifts during Catheter Ablation of Atrial Fibrillation Using Intracardiac Ultrasound Integrated with 3-Dimensional Electroanatomical Mapping System. J. Cardiovasc. Dev. Dis. 2024, 11, 110. https://doi.org/10.3390/jcdd11040110
Pernat A, Zavrtanik M, Robles AG, Romano S, Sciarra L, Antolič B. Assessment of Esophageal Shifts during Catheter Ablation of Atrial Fibrillation Using Intracardiac Ultrasound Integrated with 3-Dimensional Electroanatomical Mapping System. Journal of Cardiovascular Development and Disease. 2024; 11(4):110. https://doi.org/10.3390/jcdd11040110
Chicago/Turabian StylePernat, Andrej, Mark Zavrtanik, Antonio Gianluca Robles, Silvio Romano, Luigi Sciarra, and Bor Antolič. 2024. "Assessment of Esophageal Shifts during Catheter Ablation of Atrial Fibrillation Using Intracardiac Ultrasound Integrated with 3-Dimensional Electroanatomical Mapping System" Journal of Cardiovascular Development and Disease 11, no. 4: 110. https://doi.org/10.3390/jcdd11040110
APA StylePernat, A., Zavrtanik, M., Robles, A. G., Romano, S., Sciarra, L., & Antolič, B. (2024). Assessment of Esophageal Shifts during Catheter Ablation of Atrial Fibrillation Using Intracardiac Ultrasound Integrated with 3-Dimensional Electroanatomical Mapping System. Journal of Cardiovascular Development and Disease, 11(4), 110. https://doi.org/10.3390/jcdd11040110