


Ten-Year Experience with Endomyocardial Biopsy after Orthotopic Heart Transplantation: Comparison between Trans-Jugular and Trans-Femoral Approach
 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galeone, A.; Kirsch, M.; Barreda, E.; Fernandez, F.; Vaissier, E.; Pavie, A.; Leprince, P.; Varnous, S. Clinical outcome and quality of life of patients surviving 20 years or longer after heart transplantation. Transpl. Int. 2014, 27, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Lund, L.H.; Edwards, L.B.; Kucheryavaya, A.Y.; Benden, C.; Dipchand, A.I.; Goldfarb, S.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Yusen, R.D.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-second Official Adult Heart Transplantation Report–2015; Focus Theme: Early Graft Failure. J. Heart Lung Transplant. 2015, 34, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Lund, L.H.; Edwards, L.B.; Kucheryavaya, A.Y.; Benden, C.; Christie, J.D.; Dipchand, A.I.; Dobbels, F.; Goldfarb, S.B.; Levvey, B.J.; Meiser, B.; et al. The registry of the International Society for Heart and Lung Transplantation: Thirty-first official adult heart transplant report—2014; focus theme: Retransplantation. J. Heart Lung Transplant. 2014, 33, 996–1008. [Google Scholar] [CrossRef] [PubMed]
- Kent, G.; Sutton, D.C.; Sutton, G.C. Needle biopsy of the human ventricular myocardium. Q. Bull. Northwestern Univ. Med. Sch. 1956, 30, 213–214. [Google Scholar]
- Sakakibara, S.; Konno, S. Endomyocardial biopsy. JPN Heart J. 1962, 3, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Caves, P.K.; Stinson, E.B.; Graham, A.F.; Billingham, M.E.; Grehl, T.M.; Shumway, N.E. Percutaneous Transvenous Endomyocardial Biopsy. JAMA 1973, 225, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Marshall, H.; Allison, S. The femoral venous approach to endomyocardial biopsy: Comparison with internal jugular and transarterial approaches. Am. J. Cardiol. 1984, 53, 833–837. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Winters, G.L.; Fishbein, M.C.; Tazelaar, H.D.; Kobashigawa, J.; Abrams, J.; Andersen, C.B.; Angelini, A.; Berry, G.J.; Burke, M.M.; et al. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J. Heart Lung Transplant. 2005, 24, 1710–1720. [Google Scholar] [CrossRef]
- Crespo-Leiro, M.G.; Zuckermann, A.; Bara, C.; Mohacsi, P.; Schulz, U.; Boyle, A.; Ross, H.J.; Parameshwar, J.; Zakliczyński, M.; Fiocchi, R.; et al. Concordance among pathologists in the second Cardiac Allograft Rejection Gene Expression Observational Study (CARGO II). Transplantation 2012, 94, 1172–1177. [Google Scholar] [CrossRef]
- Seferovic, P.M.; Tsutsui, H.; McNamara, D.M.; Ristić, A.D.; Basso, C.; Bozkurt, B.; Cooper, L.T., Jr.; Filippatos, G.; Ide, T.; Inomata, T.; et al. Heart Failure Association of the ESC, Heart Failure Society of America and Japanese Heart Failure Society position statement on endomyocardial biopsy. Eur. J. Heart Fail. 2021, 23, 854–871. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Dipchand, A.; Starling, R.; Anderson, A.; Chan, M.; Desai, S.; Fedson, S.; Fisher, P.; Gonzales-Stawinski, G.; Martinelli, L.; et al. The International Society of Heart and Lung Transplantation guidelines for the care of heart transplant recipients. J Heart Lung Transplant. 2010, 29, 914–956. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.; Kindermann, I.; Kindermann, M.; Mahfoud, F.; Ukena, C.; Athanasiadis, A.; Hill, S.; Mahrholdt, H.; Voehringer, M.; Schieber, M.; et al. Comparative evaluation of left and right ventricular endomyocardial biopsy: Differences in complication rate and diagnostic performance. Circulation 2010, 122, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Holzmann, M.; Nicko, A.; Kühl, U.; Noutsias, M.; Poller, W.; Hoffmann, W.; Morguet, A.; Witzenbichler, B.; Tschöpe, C.; Schultheiss, H.P.; et al. Complication rate of right ventricular endomyocardial biopsy via the femoral approach: A retrospective and prospective study analyzing 3048 diagnostic procedures over an 11-year period. Circulation 2008, 118, 1722–1728. [Google Scholar] [CrossRef]
- Cooper, L.T.; Baughman, K.L.; Feldman, A.M.; Frustaci, A.; Jessup, M.; Kuhl, U.; Levine, G.N.; Narula, J.; Starling, R.C.; Towbin, J.; et al. The role of endomyocardial biopsy in the management of cardiovascular disease: A scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007, 116, 2216–2233. [Google Scholar] [CrossRef]
- Shah, Z.; Vuddanda, V.; Rali, A.S.; Pamulapati, H.; Masoomi, R.; Gupta, K. National trends and procedural complications from endomyocardial biopsy: Results from the National Inpatient Sample, 2007-2014. Cardiology 2018, 141, 125–131. [Google Scholar] [CrossRef]
- Bermpeis, K.; Esposito, G.; Gallinoro, E.; Paolisso, P.; Bertolone, D.T.; Fabbricatore, D.; Mileva, N.; Munhoz, D.; Buckley, J.; Wyffels, E.; et al. Safety of Right and Left Ventricular Endomyocardial Biopsy in Heart Transplantation and Cardiomyopathy Patients. JACC Heart Fail. 2022, 10, 963–973. [Google Scholar] [CrossRef]
- Vilalta, A. Cost and Use Trends of Endomyocardial Biopsy in Heart Transplant Patients: A 4-Year Claims Data Analysis. Transplant. Proc. 2023, 55, 2186–2190. [Google Scholar] [CrossRef] [PubMed]
- Fiorelli, A.I.; Coelho, G.H.; Aiello, V.D.; Benvenuti, L.A.; Palazzo, J.F.; Santos Júnior, V.P.; Canizares, B.; Dias, R.R.; Stolf, N.A. Tricuspid valve injury after heart transplantation due to endomyocardial biopsy: An analysis of 3550 biopsies. Transplant. Proc. 2012, 44, 2479–2482. [Google Scholar] [CrossRef]
- Mielniczuk, L.; Haddad, H.; Davies, R.A.; Veinot, J.P. Tricuspid valve chordal tissue in endomyocardial biopsy specimens of patients with significant tricuspid regurgitation. J. Heart Lung Transplant. 2005, 24, 1586–1590. [Google Scholar] [CrossRef]
- Wong, R.C.; Abrahams, Z.; Hanna, M.; Pangrace, J.; Gonzalez-Stawinski, G.; Starling, R.; Taylor, D. Tricuspid regurgitation after cardiac transplantation: An old problem revisited. J. Heart Lung Transplant. 2008, 27, 247–252. [Google Scholar] [CrossRef]
- Chan, M.C.; Giannetti, N.; Kato, T.; Kornbluth, M.; Oyer, P.; Valantine, H.A.; Robbins, R.C.; Hunt, S.A. Severe tricuspid regurgitation after heart transplantation. J. Heart Lung Transplant. 2001, 20, 709–717. [Google Scholar] [CrossRef]
- Filsoufi, F.; Salzberg, S.P.; Anderson, C.A.; Couper, G.S.; Cohn, L.H.; Adams, D.H. Optimal surgical management of severe tricuspid regurgitation in cardiac transplant patients. J. Heart Lung Transplant. 2006, 25, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.; Cantarovich, M.; Cecere, R.; Giannetti, N. Tricuspid regurgitation after cardiac transplantation: How many biopsies are too many? J. Heart Lung Transplant. 2005, 24, S227–S231. [Google Scholar] [CrossRef]
- Al-Hijji, M.; El Sabbagh, A.; El Hajj, S.; AlKhouli, M.; El Sabawi, B.; Cabalka, A.; Miranda, W.R.; Holmes, D.R.; Rihal, C.S. Coronary Artery Fistulas: Indications, Techniques, Outcomes, and Complications of Transcatheter Fistula Closure. JACC Cardiovasc. Interv. 2021, 14, 1393–1406. [Google Scholar] [CrossRef]
- Saraiva, F.; Matos, V.; Goncalves, L.; Antunes, M.; Providencia, L.A. Complications of endomyocardial biopsy in heart transplant recipients: A retrospective study of 2117 consecutive procedures. Transplant. Proc. 2011, 43, 1908–1912. [Google Scholar] [CrossRef] [PubMed]
- Somers, J.M.; Verney, G.I. Coronary cameral fistulae following heart transplantation. Clin. Radiol. 1991, 44, 419–421. [Google Scholar] [CrossRef] [PubMed]
- Henzlova, M.J.; Nath, H.; Bucy, R.P.; Bourge, R.C.; Kirklin, J.K.; Rogers, W.J. Coronary artery to right ventricle fistula in heart transplant recipients: A complication of endomyocardial biopsy. J. Am. Coll. Cardiol. 1989, 14, 258–261. [Google Scholar] [CrossRef]
- Sandhu, J.S.; Utretsky, B.F.; Zerbe, T.R.; Goldsmith, A.S.; Reddy, P.S.; Kormos, R.L.; Griffith, B.P.; Hardesty, R.L. Coronary artery fistula in the heart transplant patient: A potential complication of endomyocardial biopsy. Circulation 1989, 79, 350–356. [Google Scholar] [CrossRef]
- Isogai, T.; Yasunaga, H.; Matsui, H.; Ueda, T.; Tanaka, H.; Horiguchi, H.; Fushimi, K. Hospital volume and cardiac complications of endomyocardial biopsy: A retrospective cohort study of 9508 adult patients using a nationwide inpatient database in Japan. Clin. Cardiol. 2015, 38, 164–170. [Google Scholar] [CrossRef]
- ACS Committee on Perioperative Care. Revised statement on recommendations for use of real-time ultrasound guidance for placement of central venous catheters. Bull. Am. Coll. Surg. 2011, 96, 36–37. [Google Scholar]
- Saugel, B.; Scheeren, T.W.L.; Teboul, J.L. Ultrasound-guided central venous catheter placement: A structured review and recommendations for clinical practice. Crit. Care 2017, 21, 225. [Google Scholar] [CrossRef] [PubMed]
- Cusi, V.; Vaida, F.; Wettersten, N.; Rodgers, N.; Tada, Y.; Gerding, B.; Urey, M.A.; Greenberg, B.; Adler, E.D.; Kim, P.J. Incidence of Acute Rejection Compared with Endomyocardial Biopsy Complications for Heart Transplant Patients in the Contemporary Era. Transplantation, 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Pergola, V.; Mattesi, G.; Cozza, E.; Pradegan, N.; Tessari, C.; Dellino, C.M.; Savo, M.T.; Amato, F.; Cecere, A.; Perazzolo Marra, M.; et al. New Non-Invasive Imaging Technologies in Cardiac Transplant Follow-Up: Acquired Evidence and Future Options. Diagnostics 2023, 13, 2818. [Google Scholar] [CrossRef] [PubMed]
- Vermes, E.; Pantaléon, C.; Auvet, A.; Cazeneuve, N.; Machet, M.C.; Delhommais, A.; Bourguignon, T.; Aupart, M.; Brunereau, L. Cardiovascular magnetic resonance in heart transplant patients: Diagnostic value of quantitative tissue markers: T2 mapping and extracellular volume fraction, for acute rejection diagnosis. J. Cardiovasc. Magn. Reson. 2018, 20, 59. [Google Scholar] [CrossRef] [PubMed]
- Anthony, C.; Imran, M.; Pouliopoulos, J.; Emmanuel, S.; Iliff, J.; Liu, Z.; Moffat, K.; Qiu, M.R.; McLean, C.A.; Stehning, C.; et al. Cardiovascular Magnetic Resonance for Rejection Surveillance After Cardiac Transplantation. Circulation 2022, 145, 1811–1824. [Google Scholar] [CrossRef]
- Brunetti, G.; Barile, B.; Nicchia, G.P.; Onorati, F.; Luciani, G.B.; Galeone, A. The ST2/IL-33 Pathway in Adult and Paediatric Heart Disease and Transplantation. Biomedicines 2023, 11, 1676. [Google Scholar] [CrossRef] [PubMed]
- Galeone, A.; Salem, J.E.; Lebreton, G.; Coutance, G.; Nguyen, L.; Hulot, J.S.; Atassi, F.; Bega, M.; Leprince, P.; Varnous, S. Suppression of tumorigenicity-2 (ST2) is a promising biomarker in heart transplantation. Clin. Transplant. 2022, 36, e14616. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Figal, D.A.; Garrido, I.P.; Blanco, R.; Minguela, A.; Lax, A.; Ordoñez-Llanos, J.; Bayes-Genis, A.; Valdés, M.; Moore, S.A.; Januzzi, J.L. Soluble ST2 is a marker for acute cardiac allograft rejection. Ann. Thorac. Surg. 2011, 92, 2118–2124. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L.; Horne, B.D.; Moore, S.A.; Galenko, O.; Snow, G.L.; Brunisholz, K.D.; Muhlestein, J.B.; Alharethi, R.; Carlquist, J.F.; Budge, D.; et al. Interleukin receptor family member ST2 concentrations in patients following heart transplantation. Biomarkers 2013, 18, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Coutance, G.; Desiré, E.; Duong Van Huyen, J.-P. A Review of Biomarkers of Cardiac Allograft Rejection: Toward an Integrated Diagnosis of Rejection. Biomolecules 2022, 12, 1135. [Google Scholar] [CrossRef]
- Fitzsimons, S.; Evans, J.; Parameshwar, J.; Pettit, S.J. Utility of Troponin Assays for Exclusion of Acute Cellular Rejection after Heart Transplantation: A Systematic Review. J. Heart Lung Transplant. 2018, 37, 631–638. [Google Scholar] [CrossRef]
- Agbor-Enoh, S.; Shah, P.; Tunc, I.; Hsu, S.; Russell, S.; Feller, E.; Shah, K.; Rodrigo, M.E.; Najjar, S.S.; Kong, H.; et al. Cell-Free DNA to Detect Heart Allograft Acute Rejection. Circulation 2021, 143, 1184–1197. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.; Hall, S.; Shah, P.; Fine, B.; Halloran, P.; Jackson, A.M.; Khush, K.K.; Margulies, K.B.; Sani, M.M.; Patel, J.K.; et al. The evolving use of biomarkers in heart transplantation: Consensus of an expert panel. Am. J. Transplant. 2023, 23, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Velleca, A.; Shullo, M.A.; Dhital, K.; Azeka, E.; Colvin, M.; DePasquale, E.; Farrero, M.; García-Guereta, L.; Jamero, G.; Khush, K.; et al. The International Society for Heart and Lung Transplantation (ISHLT) guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2023, 42, e1–e141. [Google Scholar] [CrossRef] [PubMed]
- Deng, M.C.; Eisen, H.J.; Mehra, M.R.; Billingham, M.; Marboe, C.C.; Berry, G.; Kobashigawa, J.; Johnson, F.L.; Starling, R.C.; Murali, S.; et al. Noninvasive Discrimination of Rejection in Cardiac Allograft Recipients Using Gene Expression Profiling. Am. J. Transplant. 2006, 6, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Pham, M.X.; Teuteberg, J.J.; Kfoury, A.G.; Starling, R.C.; Deng, M.C.; Cappola, T.P.; Kao, A.; Anderson, A.S.; Cotts, W.G.; Ewald, G.A.; et al. Gene-Expression Profiling for Rejection Surveillance after Cardiac Transplantation. N. Engl. J. Med. 2010, 362, 1890–1900. [Google Scholar] [CrossRef]
- Kobashigawa, J.; Patel, J.; Azarbal, B.; Kittleson, M.; Chang, D.; Czer, L.; Daun, T.; Luu, M.; Trento, A.; Cheng, R.; et al. Randomized Pilot Trial of Gene Expression Profiling versus Heart Biopsy in the First Year after Heart Transplant: Early Invasive Monitoring Attenuation through Gene Expression Trial. Circ. Heart Fail. 2015, 8, 557–564. [Google Scholar] [CrossRef]
- Crespo-Leiro, M.G.; Stypmann, J.; Schulz, U.; Zuckermann, A.; Mohacsi, P.; Bara, C.; Ross, H.; Parameshwar, J.; Zakliczyński, M.; Fiocchi, R.; et al. Clinical Usefulness of Gene-Expression Profile to Rule out Acute Rejection after Heart Transplantation: CARGO II. Eur. Heart J. 2016, 37, 2591–2601. [Google Scholar] [CrossRef] [PubMed]
- Novák, J.; Macháčková, T.; Krejčí, J.; Bienertová-Vašků, J.; Slabý, O. MicroRNAs as Theranostic Markers in Cardiac Allograft Transplantation: From Murine Models to Clinical Practice. Theranostics 2021, 11, 6058–6073. [Google Scholar] [CrossRef] [PubMed]
- Grankvist, R.; Chireh, A.; Sandell, M.; Mukarram, A.K.; Jaff, N.; Berggren, I.; Persson, H.; Linde, C.; Arnberg, F.; Lundberg, J.; et al. Myocardial micro-biopsy procedure for molecular characterization with increased precision and reduced trauma. Sci. Rep. 2020, 10, 8029. [Google Scholar] [CrossRef]
- Halloran, P.F.; Potena, L.; Van Huyen, J.D.; Bruneval, P.; Leone, O.; Kim, D.H.; Jouven, X.; Reeve, J.; Loupy, A. Building a tissue-based molecular diagnostic system in heart transplant rejection: The heart Molecular Microscope Diagnostic (MMDx) System. J. Heart Lung Transplant. 2017, 36, 1192–1200. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Heart Recipients (n = 212) |
|---|---|
| Male sex, n (%) | 158 (75%) |
| Age at time of HT, years | 57 (49–65) |
| Dilated cardiomyopathy, n (%) | 86 (41%) |
| Ischemic cardiomyopathy, n (%) | 85 (40%) |
| Valvular cardiomyopathy, n (%) | 11 (5%) |
| Myocarditis, n (%) | 9 (4%) |
| Peri-partum cardiomyopathy | 5 (2%) |
| Hypertrophic cardiomyopathy, n (%) | 3 (1%) |
| Radiation- or chemotherapy-induced cardiomyopathy | 3 (1%) |
| Arrhythmogenic right ventricular dysplasia | 3 (1%) |
| Other cardiomyopathies | 7 (3%) |
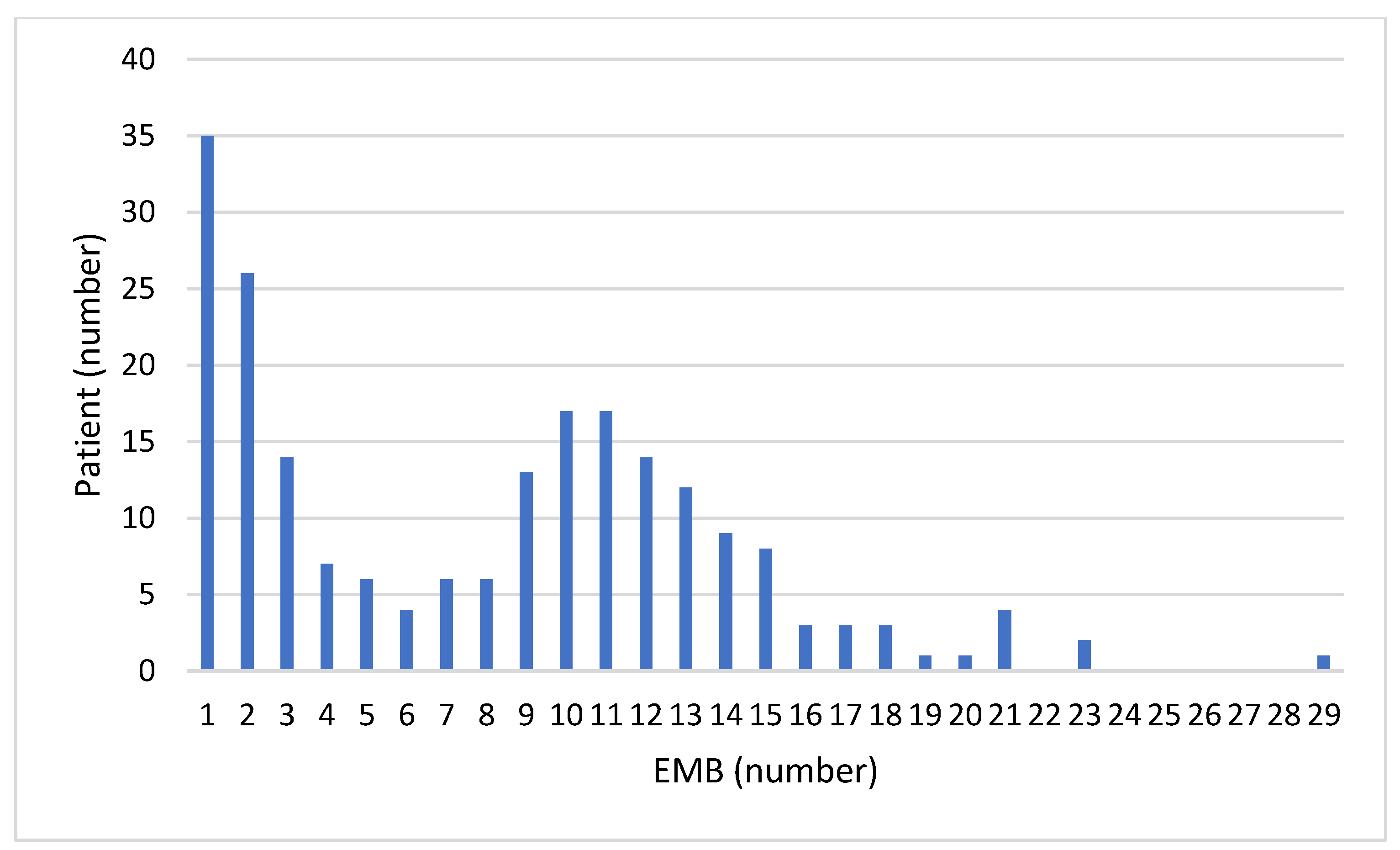
| Endomyocardial biopsy, n (interquartile range) | 9 (2–12) |
| Characteristics | Total EMBs (n = 1698) | Trans-Jugular EMBs (n = 927) | Trans-Femoral EMBs (n = 771) | p |
|---|---|---|---|---|
| Male sex, n (%) | 1309 (77%) | 744 (80%) | 565 (73%) | <0.001 |
| Age at time of EMB, years | 57 (49–63) | 57 (50–64) | 56 (47–63) | 0.003 |
| Time from HT, years | 0.4 (0.1–0.9) | 0.2 (0.1–0.5) | 0.7 (0.3–2.8) | <0.001 |
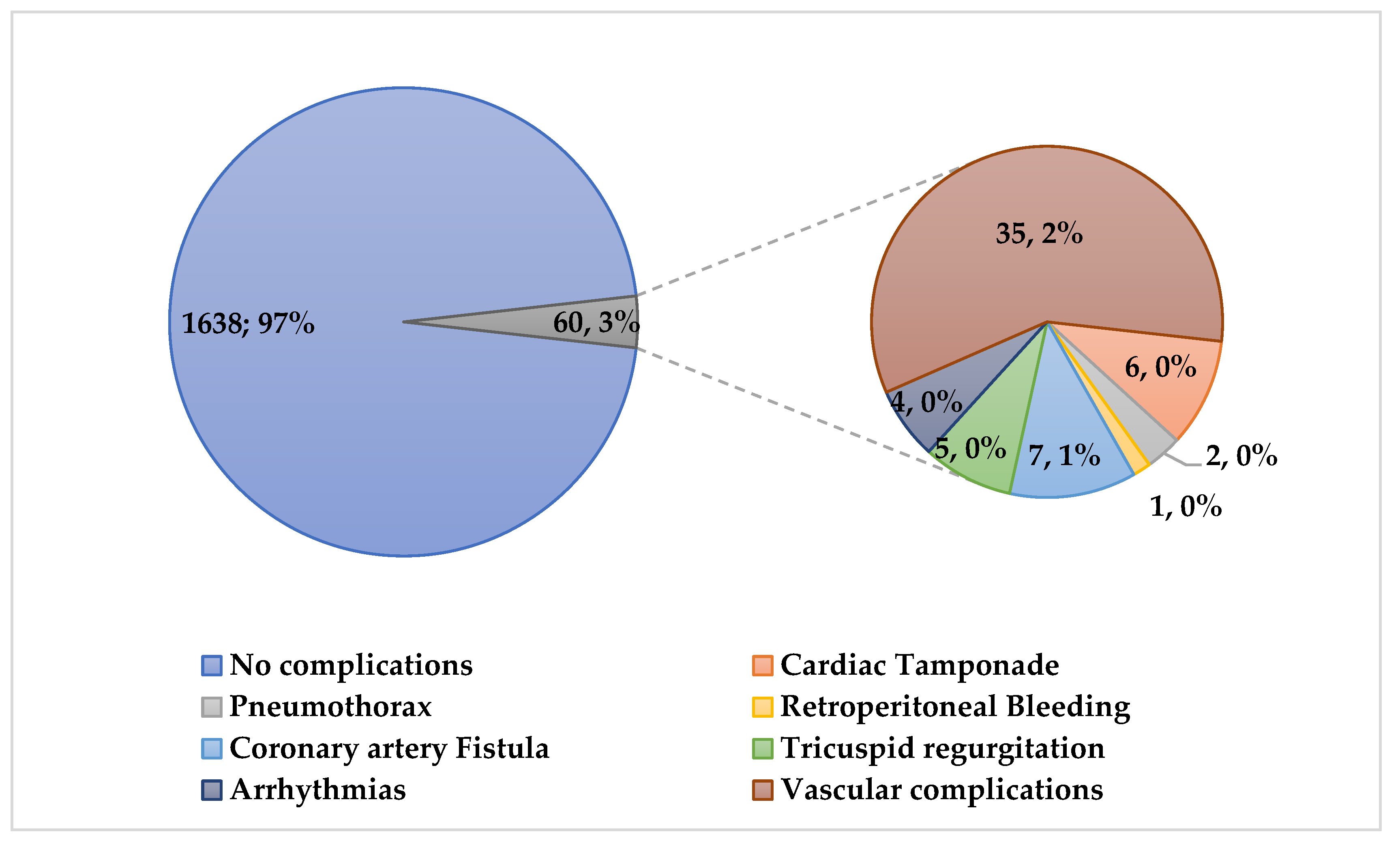
| Total Complications, n (%) | 60 (3.5%) | 38 (4%) | 22 (3%) | 0.16 |
| Major complications, n (%) | 9 (0.5%) | 6 (1%) | 3 (0.4%) | 0.65 |
| Cardiac tamponade n (%) | 6 (0.4%) | 4 (0.4%) | 2 (0.3%) | 0.55 |
| Pneumothorax, n (%) | 2 (0.1%) | 2 (0.2%) | 0 | - |
| Retroperitoneal bleeding | 1 (0.05%) | 0 | 1 (0.1%) | - |
| Minor complications, n (%) | 51 (3%) | 32 (3%) | 19 (2%) | 0.23 |
| Coronary artery fistulae, n (%) | 7 (0.4%) | 0 | 7 (1%) | - |
| De novo tricuspid regurgitation, n (%) | 5 (0.3%) | 3 (0.3%) | 2 (0.3%) | 0.8 |
| Arrhythmias, n (%) | 4 (0.2%) | 3 (0.3%) | 1 (0.1%) | 0.4 |
| Vascular access site, n (%) | 35 (2%) | 26 (3%) | 9 (1%) | 0.02 |
| Hematoma, n (%) | 13 (1%) | 5 (1%) | 8 (1%) | 0.24 |
| Accidental arterial puncture | 22 (1%) | 21 (2%) | 1 (0.1%) | <0.001 |
| Characteristics | Total EMBs (n = 1698) | Not Complicated EMBs (n = 1638) | Complicated EMBs (n = 60) | p |
|---|---|---|---|---|
| Male sex, n (%) | 1309 (77%) | 1267 (77%) | 42 (70%) | 0.17 |
| Age at time of EMB, years | 57 (49–63) | 57 (49–63) | 57 (46–64) | 0.78 |
| Time from HT, years | 0.4 (0.1–0.9) | 0.4 (0.1–0.9) | 0.3 (0.1–1.2) | 0.9 |
| Characteristics | All (n = 60) | Trans-Jugular (n = 38) | Trans-Femoral (n = 22) | p |
|---|---|---|---|---|
| Male sex, n (%) | 42 (70%) | 27 (71%) | 15 (68%) | 0.8 |
| Age at time of EMB, years | 57 (46–64) | 60 (47–65) | 54 (46–60) | 0.2 |
| Time from HT, years | 0.3 (0.1–1.2) | 0.2 (0.1–0.5) | 1.2 (0.5–14) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galeone, A.; Bernabei, A.; Pesarini, G.; Raimondi Lucchetti, M.; Onorati, F.; Luciani, G.B. Ten-Year Experience with Endomyocardial Biopsy after Orthotopic Heart Transplantation: Comparison between Trans-Jugular and Trans-Femoral Approach. J. Cardiovasc. Dev. Dis. 2024, 11, 115. https://doi.org/10.3390/jcdd11040115
Galeone A, Bernabei A, Pesarini G, Raimondi Lucchetti M, Onorati F, Luciani GB. Ten-Year Experience with Endomyocardial Biopsy after Orthotopic Heart Transplantation: Comparison between Trans-Jugular and Trans-Femoral Approach. Journal of Cardiovascular Development and Disease. 2024; 11(4):115. https://doi.org/10.3390/jcdd11040115
Chicago/Turabian StyleGaleone, Antonella, Annalisa Bernabei, Gabriele Pesarini, Marcello Raimondi Lucchetti, Francesco Onorati, and Giovanni Battista Luciani. 2024. "Ten-Year Experience with Endomyocardial Biopsy after Orthotopic Heart Transplantation: Comparison between Trans-Jugular and Trans-Femoral Approach" Journal of Cardiovascular Development and Disease 11, no. 4: 115. https://doi.org/10.3390/jcdd11040115
APA StyleGaleone, A., Bernabei, A., Pesarini, G., Raimondi Lucchetti, M., Onorati, F., & Luciani, G. B. (2024). Ten-Year Experience with Endomyocardial Biopsy after Orthotopic Heart Transplantation: Comparison between Trans-Jugular and Trans-Femoral Approach. Journal of Cardiovascular Development and Disease, 11(4), 115. https://doi.org/10.3390/jcdd11040115