

Outcomes of Patients with Normal LDL-Cholesterol at Admission for Acute Coronary Syndromes: Lower Is Not Always Better

 , , , ,
, , , ,
Abstract
1. Introduction
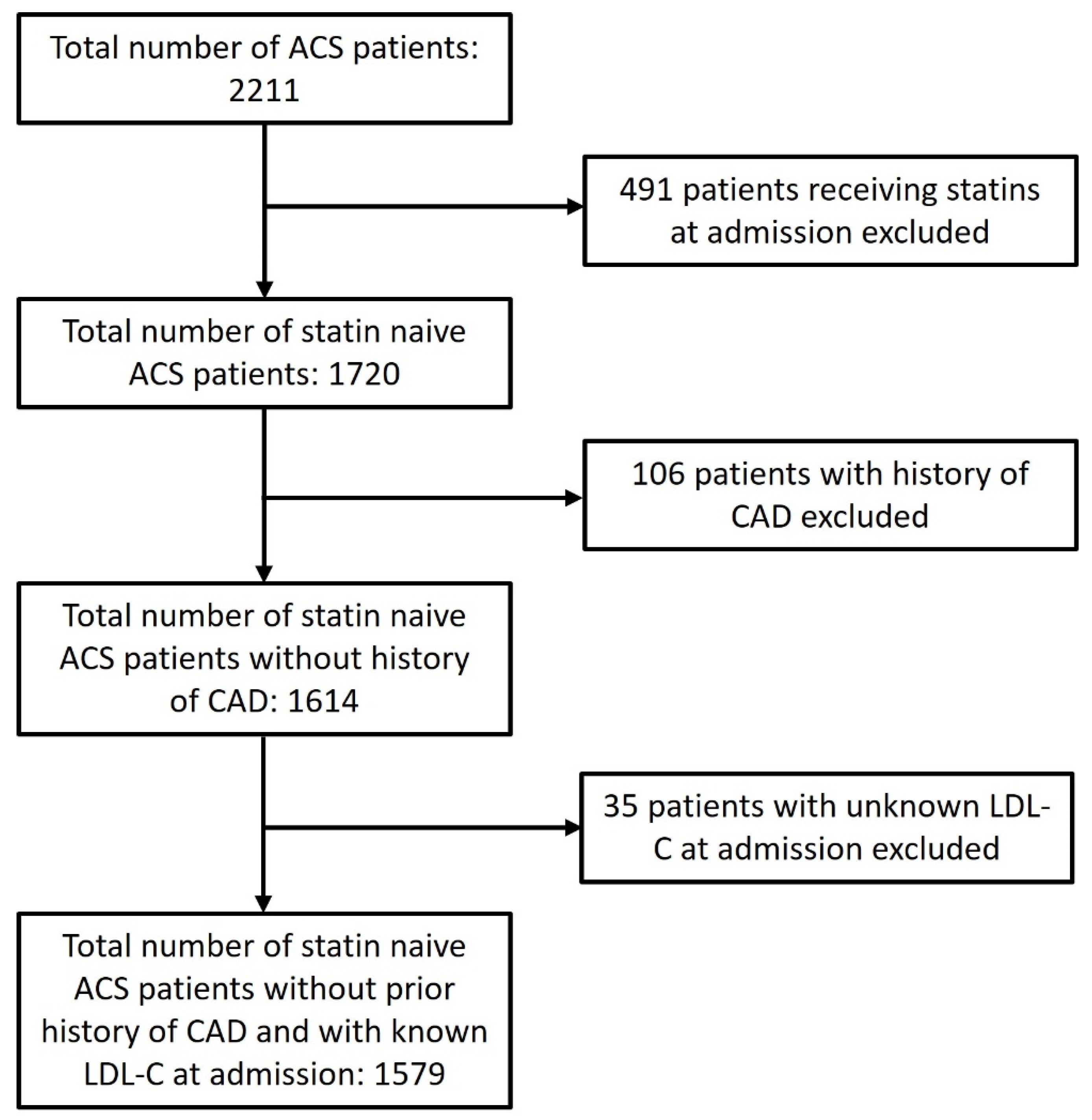
2. Patients and Methods
3. Statistical Analysis
4. Results
4.1. Overall Characteristics, Risk Factors, and Treatment Strategies
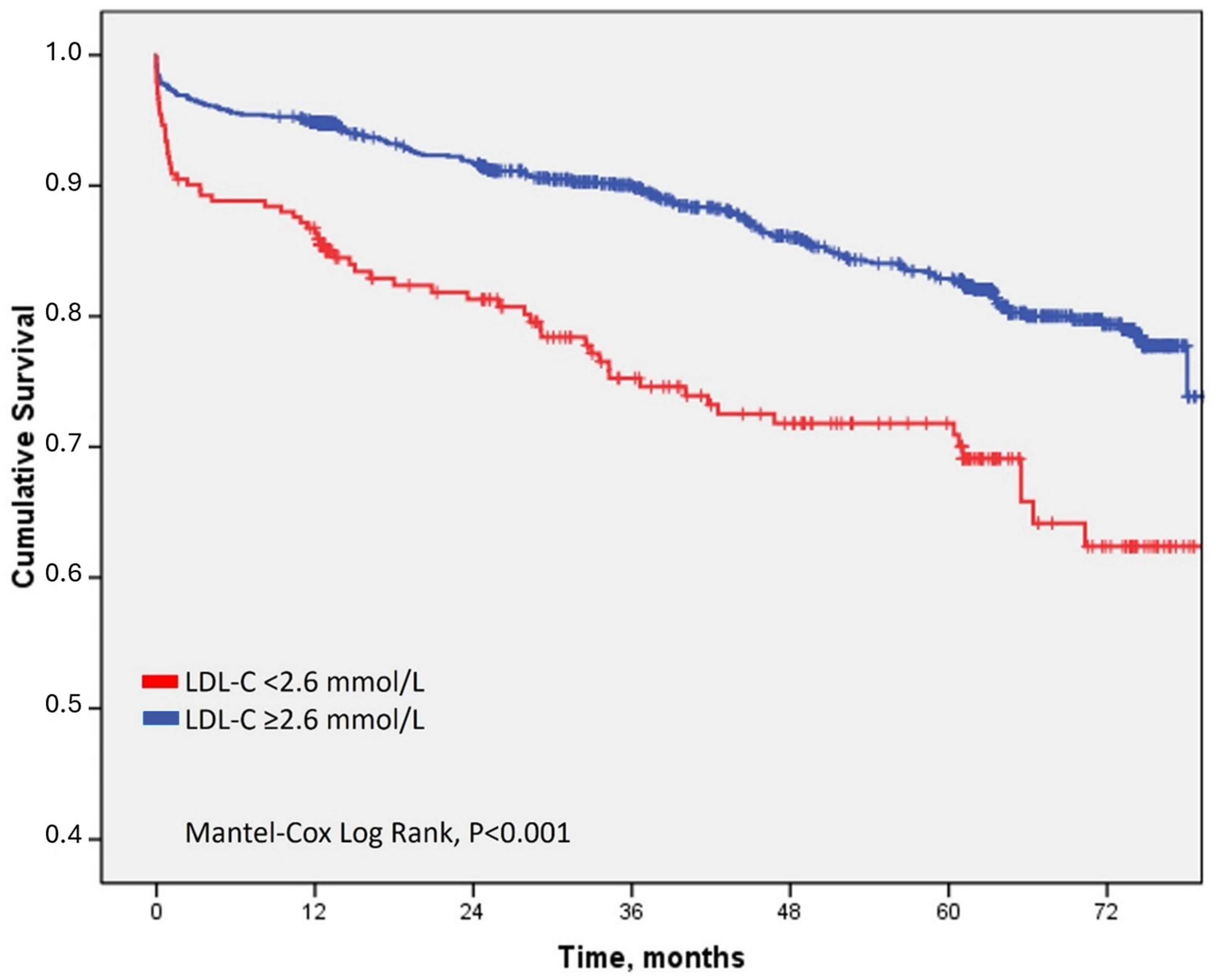
4.2. Clinical Outcome Associated with LDL-C at Admission
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.; Brewer, H.B., Jr.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C., Jr.; Stone, N.J.; Coordinating Committee of the National Cholesterol Education Program. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J. Am. Coll. Cardiol. 2004, 44, 720–732. [Google Scholar] [CrossRef]
- Shekelle, R.B.; Shryock, A.M.; Paul, O.; Lepper, M.; Stamler, J.; Liu, S.; Raynor, W.J. Diet, serum cholesterol, and death from coronary heart disease. The Western Electric study. N. Engl. J. Med. 1981, 304, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Fulcher, J.; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; Colhoun, H.; et al. Efficacy and safety of LDL-lowering therapy among men and women: Meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet 2015, 385, 1397–1405. [Google Scholar]
- Olsson, A.G.; Angelin, B.; Assmann, G.; Binder, C.J.; Björkhem, I.; Cedazo-Minguez, A.; Cohen, J.; von Eckardstein, A.; Farinaro, E.; Müller-Wieland, D.; et al. Can LDL cholesterol be too low? Possible risks of extremely low levels. J. Intern. Med. 2017, 28, 534–553. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Ridker, P.M.; Revkin, J.; Amarenco, P.; Brunell, R.; Curto, M.; Civeira, F.; Flather, M.; Glynn, R.J.; Gregoire, J.; Jukema, J.W.; et al. Cardiovascular Efficacy and Safety of Bococizumab in High-Risk Patients. N. Engl. J. Med. 2017, 376, 1527–1539. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Al-Mallah, M.H.; Hatahet, H.; Cavalcante, J.L.; Khanal, S. Low admission LDL-cholesterol is associated with increased 3-year all-cause mortality in patients with non ST segment elevation myocardial infarction. Cardiol. J. 2009, 16, 227–233. [Google Scholar] [PubMed]
- Cho, K.H.; Jeong, M.H.; Ahn, Y.; Kim, Y.J.; Chae, S.C.; Hong, T.J.; Seong, I.W.; Chae, J.K.; Kim, C.J.; Cho, M.C.; et al. Low-density lipoprotein cholesterol level in patients with acute myocardial infarction having percutaneous coronary intervention (the cholesterol paradox). Am. J. Cardiol. 2010, 106, 1061–1068. [Google Scholar] [CrossRef]
- Dong, S.; Ji, W.; Zeng, S.; Miao, J.; Yan, L.; Liu, X.; Liu, J.; Zhou, X.; Yang, Q. Admission Low-Density Lipoprotein Cholesterol Stratified by Circulating CD14++CD16+ Monocytes and Risk for Recurrent Cardiovascular Events Following ST Elevation Myocardial Infarction: Lipid Paradox Revised. J. Cardiovasc. Transl. Res. 2020, 6, 916–927. [Google Scholar] [CrossRef]
- Anker, S.D.; Ponikowski, P.; Varney, S.; Chua, T.P.; Clark, A.L.; Webb-Peploe, K.M.; Harrington, D.; Kox, W.J.; Poole-Wilson, P.A.; Coats, A.J. Wasting as independent risk factor for mortality in chronic heart failure. Lancet 1997, 349, 1050–1053. [Google Scholar] [CrossRef]
- Horwich, T.B.; Kalantar-Zadeh, K.; MacLellan, R.W.; Fonarow, G.C. Albumin levels predict survival in patients with systolic heart failure. Am. Heart J. 2008, 155, 883–889. [Google Scholar] [CrossRef]
- May, H.T.; Muhlestein, J.B.; Carlquist, J.F.; Horne, B.D.; Bair, T.L.; Campbell, B.A.; Kfoury, A.G.; Lyon, J.L.; Kim, H.; Renlund, D.G. Relation of serum total cholesterol, C-reactive protein levels, and statin therapy to survival in heart failure. Am. J. Cardiol. 2006, 98, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Sato, R.; Matsuzawa, Y.; Yoshii, T.; Akiyama, E.; Konishi, M.; Nakahashi, H.; Minamimoto, Y.; Kimura, Y.; Okada, K.; Maejima, N.; et al. Impact of Low-Density Lipoprotein Cholesterol Levels at Acute Coronary Syndrome Admission on Long-Term Clinical Outcomes. J. Atheroscler. Thromb. 2024, 31, 444–460. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.A.; Grubisic, M.; Hemmelgarn, B.; Humphries, K.; King, K.M.; Quan, H. Outcomes after acute myocardial infarction in South Asian, Chinese, and white patients. Circulation 2010, 122, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, S.; Kimura, T.; Goto, M.; Lee, V.V.; Elayda, M.; Furukawa, Y.; Fukushima, M.; Komeda, M.; Sakata, R.; Willerson, J.T.; et al. Difference in patient profiles and outcomes in Japanese versus American patients undergoing coronary revascularization. Am. J. Cardiol. 2010, 105, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Krishnaveni, P.; Gowda, V.M. Assessing the Validity of Friedewald’s Formula and Anandraja’s Formula For Serum LDL-Cholesterol Calculation. J. Clin. Diagn. Res. 2015, 12, BC01–BC04. [Google Scholar]
- Johnson, D.W.; Jones, G.R.; Mathew, T.H.; Ludlow, M.J.; Doogue, M.P.; Jose, M.D.; Langham, R.G.; Lawton, P.D.; McTaggart, S.J.; Peake, M.J.; et al. Chronic kidney disease and automatic reporting of estimated glomerular filtration rate: New developments and revised recommendations. Med. J. Aust. 2012, 197, 224–225. [Google Scholar] [CrossRef]
- Sinning, C.; Lillpopp, L.; Appelbaum, S.; Ojeda, F.; Zeller, T.; Schnabel, R.; Lubos, E.; Jagodzinski, A.; Keller, T.; Munzel, T. Angiographic score assessment improves cardiovascular risk prediction: The clinical value of SYNTAX and Gensini application. Clin. Res. Cardiol. 2013, 102, 495–503. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. ESC Scientific Document Group. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Oduncu, V.; Erkol, A.; Kurt, M.; Tanboğa, I.H.; Karabay, C.Y.; Şengül, C.; Bulut, M.; Özveren, O.; Fotbolcu, H.; Akgün, T.; et al. The prognostic value of very low admission LDL-cholesterol levels in ST-segment elevation myocardial infarction compared in statin-pretreated and statin-naive patients undergoing primary percutaneous coronary intervention. Int. J. Cardiol. 2013, 167, 458–463. [Google Scholar] [CrossRef]
- Li, B.; Qu, Y.; Fan, Z.; Gong, X.; Xu, H.; Wu, L.; Yan, C. Causal relationships between blood lipids and major psychiatric disorders: Univariable and multivariable mendelian randomization analysis. BMC Med. Genom. 2023, 16, 250. [Google Scholar] [CrossRef]
- Chen, H.; Du, Y.; Liu, S.; Ge, B.; Ji, Y.; Huang, G. Association between serum cholesterol levels and Alzheimer’s disease in China: A case-control study. Int. J. Food Sci. Nutr. 2019, 70, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, L.B.; Toth, P.P.; Dearborn-Tomazos, J.L.; Giugliano, R.P.; Hirsh, B.J.; Peña, J.M.; Selim, M.H.; Woo, D. Aggressive LDL-C Lowering and the Brain: Impact on Risk for Dementia and Hemorrhagic Stroke: A Scientific Statement From the American Heart Association. Arterioscler. Thromb. Vasc. Biol. 2023, 43, e404–e442. [Google Scholar] [CrossRef]
- Chang, W.C.; Chan, J.K.N.; Wong, C.S.M.; Hai, J.S.H.; Or, P.C.F.; Chen, E.Y.H. Mortality, Revascularization, and Cardioprotective Pharmacotherapy After Acute Coronary Syndrome in Patients with Psychotic Disorders: A Population-Based Cohort Study. Schizophr. Bull. 2020, 46, 774–784. [Google Scholar] [CrossRef] [PubMed]
- Bergamaschi, L.; Landi, A.; Maurizi, N.; Pizzi, C.; Leo, L.A.; Arangalage, D.; Iglesias, J.F.; Eeckhout, E.; Schwitter, J.; Valgimigli, M.; et al. Acute Response of the Noninfarcted Myocardium and Surrounding Tissue Assessed by T2 Mapping after STEMI. JACC Cardiovasc. Imaging 2024. [Google Scholar] [CrossRef]
- Ciliberti, G.; Guerra, F.; Pizzi, C.; Merlo, M.; Zilio, F.; Bianco, F.; Mancone, M.; Zaffalon, D.; Gioscia, R.; Bergamaschi, L.; et al. Characteristics of patients with recurrent acute myocardial infarction after MINOCA. Prog. Cardiovasc. Dis. 2023, 81, 42–47. [Google Scholar] [CrossRef]
- Hoogeveen, R.C.; Ballantyne, C.M. Residual Cardiovascular Risk at Low LDL: Remnants, Lipoprotein(a), and Inflammation. Clin. Chem. 2021, 67, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Dong, W.; Zhong, X.; Yuan, K.; Miao, M.; Zhai, Y.; Che, B.; Xu, T.; Xu, X.; Zhong, C. Lipoprotein(a) and functional outcome of acute ischemic stroke when discordant with low-density lipoprotein cholesterol. Postgrad. Med. J. 2023, 99, 1160–1166. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Characteristic, Median (IQR) or Number (%) | LDL-C at Admission | p Value (Mann–Whitney or χ2 Test) | ||
|---|---|---|---|---|
| Normal (<2.6 mmol/L) N = 242 | High (≥2.6 mmol/L) N = 1337 | |||
| Age, years | 66 (19) | 62 (16) | <0.001 | |
| Male sex | 172 (71) | 936 (70) | 0.761 | |
| Creatinine clearance, ml/min | 71 (43) | 81 (32) | <0.001 | |
| Arterial hypertension | 909 (68) | 180 (74) | 0.057 | |
| Diabetes mellitus | 64 (26) | 226 (17) | 0.001 | |
| LDL-C, mmol/L | 2.1 (0.6) | 3.5 (1.2) | <0.001 | |
| HDL-C, mmol/L | 1.0 (0.3) | 1.2 (0.3) | <0.001 | |
| NonHDL-C, mmol/L | 2.8 (0.6) | 4.6 (1.3) | <0.001 | |
| Triglycerids, mmol/L | 1.3 (0.9) | 1.6 (1.2) | <0.001 | |
| Peripheral artery disease | 33 (14) | 114 (9) | <0.001 | |
| Chronic obstructive pulmonary disease | 19 (8) | 29 (2) | <0.001 | |
| Current or previous smoking | 112 (46) | 663 (50) | 0.454 | |
| Body mass index, kg/m2 | 27.7 (5.7) | 28.6 (5.7) | <0.001 | |
| Psychological disorder | 46 (19) | 145 (10) | <0.001 | |
| ACS type | STEMI | 139 (57) | 820 (61) | 0.536 |
| NSTE-ACS | 92 (38) | 460 (35) | ||
| MINOCA | 11 (5) | 57 (4) | ||
| Timing of coronary angiography | ≤24 h | 175 (72) | 1122 (84) | <0.001 |
| >24 h | 67 (28) | 215 (16) | ||
| Wrist vascular access | 194 (80) | 1137 (85) | 0.177 | |
| Left anterior descendent as infarct related artery | 94 (39) | 526 (39) | 0.952 | |
| Syntax score | 12 (13) | 12 (12.5) | 0.996 | |
| Mulltivessel disease | 51 (21) | 263 (20) | 0.878 | |
| Cardiogenic shock and/or cardiopulmonary resuscitation | 40 (17) | 93 (7) | 0.001 | |
| Treatment and Outcome Variables, Number (%) or Median (IQR) | LDL-C at Admission | p Value (χ2 or Mann–Whitney Test) | ||
|---|---|---|---|---|
| Normal (<2.6 mmol/L) N = 242 | High (≥2.6 mmol/L) N = 1337 | |||
| Treatment strategy | PCI | 192 (79) | 1180 (88) | 0.001 |
| CABG | 18 (8) | 59 (5) | ||
| OMT | 32 (13) | 98 (7) | ||
| Complete revascularization | 163 (67) | 962 (72) | 0.085 | |
| LVEF at discharge, % | 52 (17) | 55 (12) | 0.005 | |
| DAPT at discharge | Ticagrelor | 140 (58) | 920 (69) | <0.001 |
| Prasugrel | 14 (6) | 154 (12) | ||
| Clopidogrel | 72 (30) | 218 (16) | ||
| No DAPT | 16 (6) | 45 (3) | ||
| Statin at discharge | Maximal dose | 223 (92) | 1282 (96) | 0.348 |
| Submaximal dose | 13 (5) | 45 (3) | ||
| No statin | 6 (3) | 10 (1) | ||
| Adherence to medical therapy after discharge | Low | 48 (24) | 247 (20) | 0.475 |
| Moderate | 66 (33) | 397 (32) | ||
| High | 85 (43) | 588 (48) | ||
| LDL-C target goal achieved at 12 months | 88 (36) | 339 (25) | <0.001 | |
| Death, in-hospital | 12 (5) | 32 (2) | 0.083 | |
| Death, overall | 63 (26) | 194 (15) | <0.001 | |
| Death, causes | Cardiovascular | 45 (19) | 128 (10) | <0.001 |
| Other | 15 (6) | 58 (4) | ||
| Unknown | 3 (1) | 8 (1) | ||
| Variable | Multivariate Cox Regression, Death, HR (95% CI) |
|---|---|
| Age, continuous | 1.056 (1.042–1.070) * |
| Creatinine clearance, continuous | 1.002 (1.000–1.004) |
| Diabetes mellitus, categorical | 0.997 (0.707–1.406) |
| Peripheral artery disease, categorical | 1.273 (0.862–1.879) |
| Chronic obstructive pulmonary disease, categorical | 0.888 (0.478–1.895) |
| Body max index, continuous | 1.035 (1.002–1.069) * |
| Psychological disorder, categorical | 1.810 (1.271–2.577) * |
| LVEF at discharge, continuous | 0.940 (0.928–0.953) * |
| LDL-C, categorical (<2.6 mmol/L at admission) | 1.483 (1.052–2.091) * |
| LDL-C, continuous | 0.819 (0.710–0.944) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurin, I.; Jurišić, A.; Rudež, I.; Kurtić, E.; Skorić, I.; Čikara, T.; Šipić, T.; Rudan, D.; Manola, Š.; Hadžibegović, I. Outcomes of Patients with Normal LDL-Cholesterol at Admission for Acute Coronary Syndromes: Lower Is Not Always Better. J. Cardiovasc. Dev. Dis. 2024, 11, 120. https://doi.org/10.3390/jcdd11040120
Jurin I, Jurišić A, Rudež I, Kurtić E, Skorić I, Čikara T, Šipić T, Rudan D, Manola Š, Hadžibegović I. Outcomes of Patients with Normal LDL-Cholesterol at Admission for Acute Coronary Syndromes: Lower Is Not Always Better. Journal of Cardiovascular Development and Disease. 2024; 11(4):120. https://doi.org/10.3390/jcdd11040120
Chicago/Turabian StyleJurin, Ivana, Anđela Jurišić, Igor Rudež, Ena Kurtić, Ivan Skorić, Tomislav Čikara, Tomislav Šipić, Diana Rudan, Šime Manola, and Irzal Hadžibegović. 2024. "Outcomes of Patients with Normal LDL-Cholesterol at Admission for Acute Coronary Syndromes: Lower Is Not Always Better" Journal of Cardiovascular Development and Disease 11, no. 4: 120. https://doi.org/10.3390/jcdd11040120
APA StyleJurin, I., Jurišić, A., Rudež, I., Kurtić, E., Skorić, I., Čikara, T., Šipić, T., Rudan, D., Manola, Š., & Hadžibegović, I. (2024). Outcomes of Patients with Normal LDL-Cholesterol at Admission for Acute Coronary Syndromes: Lower Is Not Always Better. Journal of Cardiovascular Development and Disease, 11(4), 120. https://doi.org/10.3390/jcdd11040120