Inflammatory Cells in Adipose Tissue and Skeletal Muscle of Patients with Peripheral Arterial Disease or Chronic Venous Disease: A Prospective, Observational, and Histological Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Type and Inclusion/Exclusion Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
- Bedridden individuals or subjects who refused to participate in the protocol.
- Those with diseases responsible for body composition changes or a pro-inflammatory state.
- Recent diet change.
- Active malignancy.
- Auto-immune disease.
- Active infection.
- Chronic renal failure (GFR < 30 mL/min/1.73 m2).
- Heart failure in the past 3 months
2.2. Ethical Considerations
2.3. Clinical Characteristics
2.4. C-Reactive Protein
2.5. Histologic Characteristics of Skeletal Muscle
2.5.1. Haematoxylin–Eosin Analysis
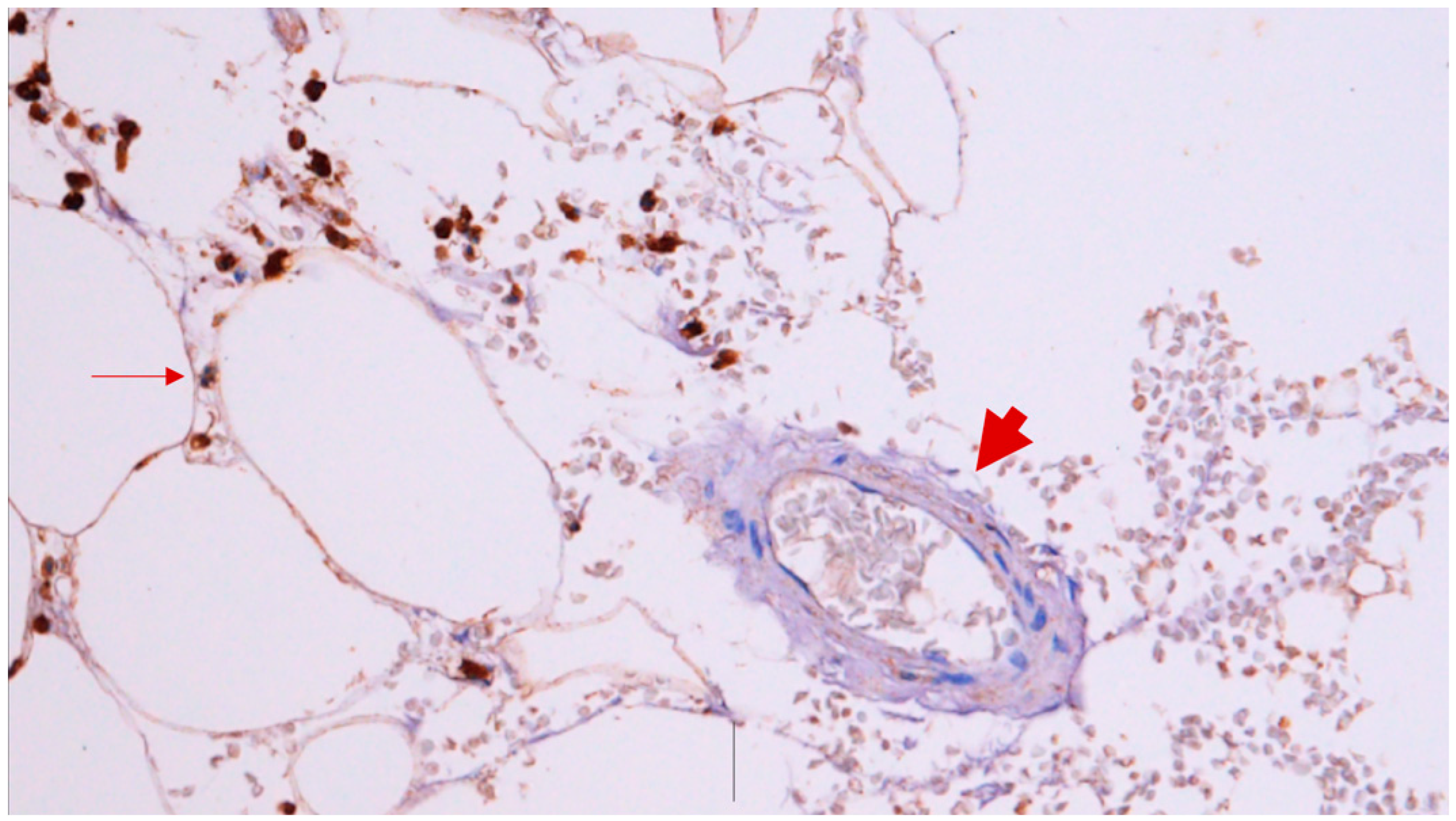
2.5.2. Immunohistochemical Study
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Histologic Characteristics of Skeletal Muscle
3.3. Histologic Characteristics of Adipose Tissue
3.4. C-Reactive Protein
4. Discussion
4.1. Anthropometric Measures, PAD, and LECVD
4.2. Skeletal Muscle, PAD, and LECVD
4.3. Adipose Tissue, PAD, and LECVD
4.4. Limitations and Aims for a Future Investigation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brevetti, G.; Giugliano, G.; Brevetti, L.; Hiatt, W.R. Inflammation in peripheral artery disease. Circulation 2010, 122, 1862–1875. [Google Scholar] [CrossRef]
- Simon, F.; Oberhuber, A.; Floros, N.; Düppers, P.; Schelzig, H.; Duran, M. Pathophysiology of chronic limb ischemia. Gefässchirurgie 2018, 23 (Suppl. S1), 13–18. [Google Scholar] [CrossRef]
- Dieplinger, B.; Haltmayer, M.; Poelz, W.; Mueller, T. Value of adiponectin as predictor of 5-year all-cause mortality in patients with symptomatic peripheral arterial disease: Results from the Linz Peripheral Arterial Disease (LIPAD) study. Clin. Chim. Acta 2009, 408, 87–91. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.-B.; Suresh, K.R.; Murad, M.H.; et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J. Vasc. Surg. 2019, 69, 3S–125S.e40, Erratum in J. Vasc. Surg. 2019, 70, 662. [Google Scholar] [CrossRef] [PubMed]
- Mustapha, J.A.; Katzen, B.T.; Neville, R.F.; Lookstei, R.A.; Zeller, T.; Miller, L.E.; Driver, V.R.; Jaff, M.R. Critical Limb Ischemia: A Threat to Life and Limb. Endovasc. Today 2019, 18, 80–82. [Google Scholar]
- Jalkanen, J.; Maksimow, M.; Hollmén, M.; Jalkanen, S.; Hakovirta, H. Compared to Intermittant Claudication Critical Limb Ischemia Is Associated with Elevated Levels of Cytokines. PLoS ONE 2016, 11, e0162353. [Google Scholar] [CrossRef]
- Jakovljević, B.; Stojanov, V.; Lović, D.; Paunović, K.; Radosavljević, V.; Tutić, I. Obesity and fat distribution as predictors of aortoiliac peripheral arterial disease in middle-aged men. Eur. J. Intern. Med. 2011, 22, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Seo, D.H.; Lee, Y.-H.; Suh, Y.J.; Ahn, S.H.; Hong, S.; Choi, Y.J.; Huh, B.W.; Park, S.W.; Lee, E.; Kim, S.H. Low muscle mass is associated with carotid atherosclerosis in patients with type 2 diabetes. Atherosclerosis 2020, 305, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Dahl, T.B.; Yndestad, A.; Skjelland, M.; Øie, E.; Dahl, A.; Michelsen, A.; Damås, J.K.; Tunheim, S.H.; Ueland, T.; Smith, C.; et al. Increased expression of visfatin in macrophages of human unstable carotid and coronary atherosclerosis: Possible role in inflammation and plaque destabilization. Circulation 2007, 115, 972–980. [Google Scholar] [CrossRef]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef]
- Nicolaides, A.; Kakkos, S.; Baekgaard, N.; Comerota, A.; de Maeseneer, M.; Eklof, B.; Giannoukas, A.D.; Lugli, M.; Maleti, O.; Myers, K.; et al. Management of chronic venous disorders of the lower limbs. Guidelines According to Scientific Evidence. Part I. Int. Angiol. 2018, 37, 181–254. [Google Scholar] [CrossRef]
- Costa, D.; Andreucci, M.; Ielapi, N.; Serraino, G.F.; Mastroroberto, P.; Bracale, U.M.; Serra, R. Molecular Determinants of Chronic Venous Disease: A Comprehensive Review. Int. J. Mol. Sci. 2023, 24, 1928. [Google Scholar] [CrossRef] [PubMed]
- Raffetto, J.D.; Mannello, F. Pathophysiology of chronic venous disease. Int. Angiol. 2014, 33, 212–221. [Google Scholar] [PubMed]
- Ferreira, J.; Carneiro, A.; Vila, I.; Silva, C.; Cunha, C.; Longatto-Filho, A.; Mesquita, A.; Cotter, J.; Mansilha, A.; Correia-Neves, M.; et al. Inflammation and Loss of Skeletal Muscle Mass in Chronic Limb Threatening Ischemia. Ann. Vasc. Surg. 2023, 88, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.; Afonso, J.; Carneiro, A.L.; Vila, I.; Cunha, C.; Roque, S.; Silva, C.; Mesquita, A.; Cotter, J.; Correia-Neves, M.; et al. Exploring the Diversity of Visceral, Subcutaneous and Perivascular Adipose Tissue in a Vascular Surgery Population. J. Cardiovasc. Dev. Dis. 2023, 10, 271. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, M.; Pourmoghaddas, Z.; Hekmatnia, A.; Sanei, H.; Tavakoli, B.; Tchernof, A.; Roohafza, H.; Sarrafzadegan, N. Abdominal fat distribution and serum lipids in patients with and without coronary heart disease. Arch. Iran. Med. 2013, 16, 149–153. [Google Scholar]
- Fox, C.S.; Massaro, J.M.; Schlett, C.L.; Lehman, S.J.; Meigs, J.B.; O’Donnell, C.J.; Hoffmann, U.; Murabito, J.M. Periaortic fat deposition is associated with peripheral arterial disease: The framingham heart study. Circ. Cardiovasc. Imaging 2010, 3, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Badimon, L.; Cubedo, J. Adipose tissue depots and inflammation: Effects on plasticity and resident mesenchymal stem cell function. Cardiovasc. Res. 2017, 113, 1064–1073. [Google Scholar] [CrossRef]
- Sinikumpu, S.-P.; Keränen, M.-H.; Jokelainen, J.; Keinänen-Kiukaanniemi, S.; Huilaja, L. The association between chronic venous disease and measures of physical performance in older people: A population-based study. BMC Geriatr. 2021, 21, 556. [Google Scholar] [CrossRef]
- McDermott, M.M.; Ferrucci, L.; Gonzalez-Freire, M.; Kosmac, K.; Leeuwenburgh, C.; Peterson, C.A.; Saini, S.; Sufit, R. Skeletal Muscle Pathology in Peripheral Artery Disease: A Brief Review. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2577–2585. [Google Scholar] [CrossRef]
- Pizzimenti, M.; Meyer, A.; Charles, A.L.; Giannini, M.; Chakfé, N.; Lejay, A.; Geny, B. Sarcopenia and peripheral arterial disease: A systematic review. J. Cachexia Sarcopenia Muscle 2020, 11, 866–886. [Google Scholar] [CrossRef]
- Weiss, D.J.; Casale, G.P.; Koutakis, P.; Nella, A.A.; Swanson, S.A.; Zhu, Z.; Miserlis, D.; Johanning, J.M.; Pipinos, I.I. Oxidative damage and myofiber degeneration in the gastrocnemius of patients with peripheral arterial disease. J. Transl. Med. 2013, 11, 230. [Google Scholar] [CrossRef] [PubMed]
- Kosmac, K.; Gonzalez-Freire, M.; McDermott, M.M.; White, S.H.; Walton, R.G.; Sufit, R.L.; Tian, L.; Li, L.; Kibbe, M.R.; Criqui, M.H.; et al. Correlations of Calf Muscle Macrophage Content with Muscle Properties and Walking Performance in Peripheral Artery Disease. J. Am. Heart Assoc. 2020, 9, e015929. [Google Scholar] [CrossRef] [PubMed]
- Pahk, K.; Kim, E.J.; Kwon, H.W.; Joung, C.; Seo, H.S.; Kim, S. Association of Inflammatory Metabolic Activity of Psoas Muscle and Acute Myocardial Infarction: A Preliminary Observational Study with 18F-FDG PET/CT. Diagnostics 2021, 11, 511. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-K.; Kim, H.-N.; Song, S.-W. Associations of skeletal muscle mass with atherosclerosis and inflammatory markers in Korean adults. Arch. Gerontol. Geriatr. 2020, 90, 104163. [Google Scholar] [CrossRef] [PubMed]
- Muffova, B.; Kauerová, S.; Bartušková, H.; Paukner, K.; Lesna, I.K.; Poledne, R. The antiinflammatory effect of statin treatment on macrophages polarisation in vitro–Preliminary study. Atherosclerosis 2023, 379, S24. [Google Scholar] [CrossRef]
- Čejková, S.; Lesná, I.K.; Froněk, J.; Janoušek, L.; Králová, A.; Ždychová, J.; Thieme, F.; Poledne, R. Pro-inflammatory gene expression in adipose tissue of patients with atherosclerosis. Physiol. Res. 2017, 66, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.; Dey, D.; Wong, D.T.L.; Nerlekar, N. Perivascular Adipose Tissue and Coronary Atherosclerosis: From Biology to Imaging Phenotyping. Curr. Atheroscler. Rep. 2019, 21, 47. [Google Scholar] [CrossRef]
- Liu, Y.; Sun, Y.; Hu, C.; Liu, J.; Gao, A.; Han, H.; Chai, M.; Zhang, J.; Zhou, Y.; Zhao, Y. Perivascular Adipose Tissue as an Indication, Contributor to, and Therapeutic Target for Atherosclerosis. Front. Physiol. 2020, 11, 615503. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PAD (n = 44) | Patients with Varicose Veins (n = 11) | p-Value | |
|---|---|---|---|
| Male (n; %) | 34; 77.27 | 9; 81.81 | 0.497 |
| Age (years-old) | 66.98 ± 9.92 | 65.09 ± 9.55 | 0.575 |
| Hypertension (n; %) | 26; 59.09 | 37; 63.64 | 0.916 |
| Dyslipidaemia (n; %) | 28; 63.64 | 5; 45.45 | 0.196 |
| Smoker/ex-smoker (n; %) | 27; 61.36 | 8; 72.73 | 0.387 |
| Diabetes (n; %) | 17; 38.64 | 4; 36.36 | 0.804 |
| Coronary artery disease (n; %) | 7; 15.91 | 1; 9.91 | 0.532 |
| Stroke/TIA (n;%) | 3; 6.82 | 1; 9.91 | 0.468 |
| Antiplatelet (n;%) | 35; 79.54 | 5; 45.45 | 0.000 * |
| Statin (n;%) | 38; 86.36 | 7; 63.64 | 0.004 * |
| ACEI (n;%) | 14; 31.82 | 3; 27.27 | 0.981 |
| Beta-blockers (n;%) | 11; 25.00 | 3; 27.27 | 0.154 |
| PAD (n = 41) | Patients with Varicose Veins (n = 8) | X2 | df | p-Value | Phi | |
|---|---|---|---|---|---|---|
| Well-preserved skeletal fibres | 26; 63.41 | 3; 37.50 | 1.861 | 1 | 0.173 | 0.195 |
| Trauma (n; %) | 4; 9.76 | 2; 25.00 | 1.448 | 1 | 0.229 | −0.172 |
| Haemorrhage (n; %) | 6; 14.63 | 0; 0 | 1.334 | 1 | 0.248 | 0.165 |
| Inflammatory cells | 18; 43.90 | 0; 0 | 5.552 | 1 | 0.018 * | 0.337 |
| PAD (n = 39) | Patients with Varicose Veins (n = 8) | X2 | df | p-Value | Phi | |
|---|---|---|---|---|---|---|
| CD 45+ mild or absent (0;†) (n/%) | 19; 48.72 | 5; 62.50 | 0.505 | 1 | 0.477 | −0.104 |
| CD 45+ > moderate (††; †††; ††††) (n/%) | 20; 51.28 | 3; 37.50 | ||||
| CD 163+ mild or absent (0;†) (n/%) | 31; 77.50 | 7; 87.50 | 0.544 | 1 | 0.461 | −0.105 |
| CD 163+ > moderate (††; †††; ††††) (n/%) | 9; 22.50 | 1; 12.50 |
| PAD (n = 44) | Patients with Varicose Veins (n = 11) | X2 | df | p-Value | Phi | |
|---|---|---|---|---|---|---|
| Well-preserved adipocytes (n; %) | 11; 25.00 | 3; 27.27 | 0.024 | 1 | 0.877 | 0.195 |
| Adipocytes imprecise limits (n; %) | 27; 61.36 | 5; 45.45 | 0.915 | 1 | 0.339 | −0.172 |
| Haemorrhage (n; %) | 6; 13.64 | 1; 9.09 | 0.164 | 1 | 0.686 | 0.165 |
| Inflammatory cells | 6; 13.64 | 2; 18.18 | 0.146 | 1 | 0.702 | 0.337 |
| PAD (n = 44) | Patients with Varicose Veins (n = 11) | X2 | df | p-Value | Phi | |
|---|---|---|---|---|---|---|
| CD 45+ mild or absent (0;†) (n/%) | 12; 27.27 | 8; 72.73 | 7.857 | 1 | 0.005 * | −0.378 |
| CD 45+ > moderate (††; †††; ††††) (n/%) | 32; 72.73 | 3; 27.27 | ||||
| (n = 42) | (n = 11) | |||||
| CD 163+ mild or absent (0;†) (n/%) | 21; 50.00 | 7; 63.64 | 0.859 | 1 | 0.345 | −0.127 |
| CD 163+ > moderate (††; †††; ††††) (n/%) | 21; 50.00 | 4; 36.36 |
| PAD (n = 37) | Patients with Varicose Veins (n = 11) | X2 | df | p-Value | Phi | |
|---|---|---|---|---|---|---|
| Well-preserved adipocytes (n; %) | 14; 37.84 | 5; 45.45 | 0.206 | 1 | 0.650 | −0.065 |
| Adipocytes imprecise limits (n; %) | 17; 45.95 | 6; 54.54 | 0.251 | 1 | 0.616 | −0.072 |
| Haemorrhage (n; %) | 2; 5.41 | 0; 0 | 0.620 | 1 | 0.431 | 0.114 |
| Inflammatory cells | 16; 43.24 | 0; 0 | 7.135 | 1 | 0.008 * | 0.386 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, J.; Longatto-Filho, A.; Afonso, J.; Roque, S.; Carneiro, A.L.; Vila, I.; Silva, C.; Cunha, C.; Mesquita, A.; Cotter, J.; et al. Inflammatory Cells in Adipose Tissue and Skeletal Muscle of Patients with Peripheral Arterial Disease or Chronic Venous Disease: A Prospective, Observational, and Histological Study. J. Cardiovasc. Dev. Dis. 2024, 11, 121. https://doi.org/10.3390/jcdd11040121
Ferreira J, Longatto-Filho A, Afonso J, Roque S, Carneiro AL, Vila I, Silva C, Cunha C, Mesquita A, Cotter J, et al. Inflammatory Cells in Adipose Tissue and Skeletal Muscle of Patients with Peripheral Arterial Disease or Chronic Venous Disease: A Prospective, Observational, and Histological Study. Journal of Cardiovascular Development and Disease. 2024; 11(4):121. https://doi.org/10.3390/jcdd11040121
Chicago/Turabian StyleFerreira, Joana, Adhemar Longatto-Filho, Julieta Afonso, Susana Roque, Alexandre Lima Carneiro, Isabel Vila, Cristina Silva, Cristina Cunha, Amílcar Mesquita, Jorge Cotter, and et al. 2024. "Inflammatory Cells in Adipose Tissue and Skeletal Muscle of Patients with Peripheral Arterial Disease or Chronic Venous Disease: A Prospective, Observational, and Histological Study" Journal of Cardiovascular Development and Disease 11, no. 4: 121. https://doi.org/10.3390/jcdd11040121
APA StyleFerreira, J., Longatto-Filho, A., Afonso, J., Roque, S., Carneiro, A. L., Vila, I., Silva, C., Cunha, C., Mesquita, A., Cotter, J., Correia-Neves, M., Mansilha, A., & Cunha, P. (2024). Inflammatory Cells in Adipose Tissue and Skeletal Muscle of Patients with Peripheral Arterial Disease or Chronic Venous Disease: A Prospective, Observational, and Histological Study. Journal of Cardiovascular Development and Disease, 11(4), 121. https://doi.org/10.3390/jcdd11040121