
Abdominal and Peripheral Tissue Oxygen Supply during Selective Lower Body Perfusion for the Surgical Repair of Congenital Heart Disease: A Pilot Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
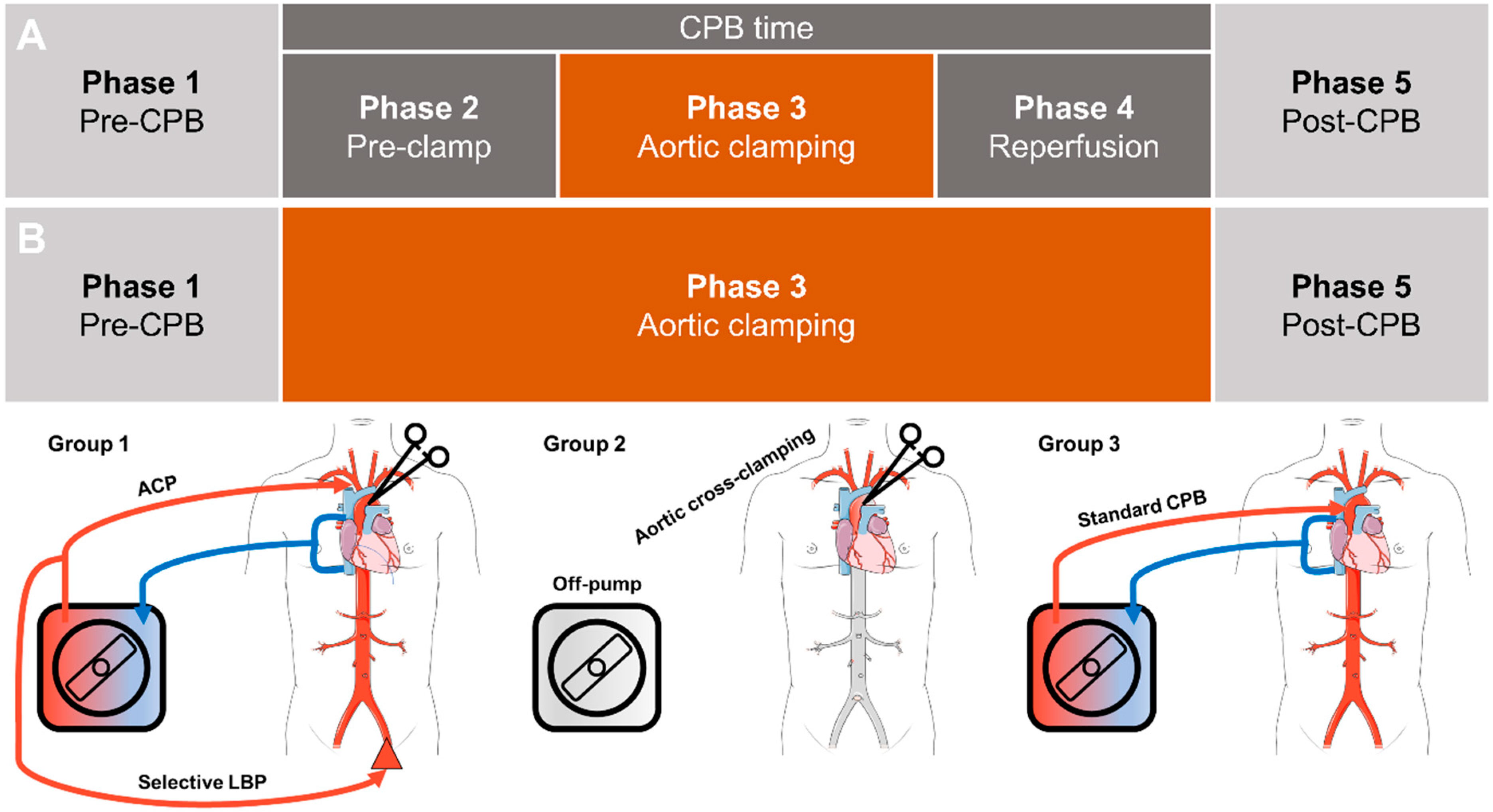
2.1. Study Design
2.2. Patients
- Group 1: CPB with ACP and LBP
- Group 2: Resection of isolated CoA without CPB
- Group 3: Conventional CPB with whole-body perfusion
2.3. Anesthesia
2.4. Surgical Procedure and Cardiopulmonary Bypass
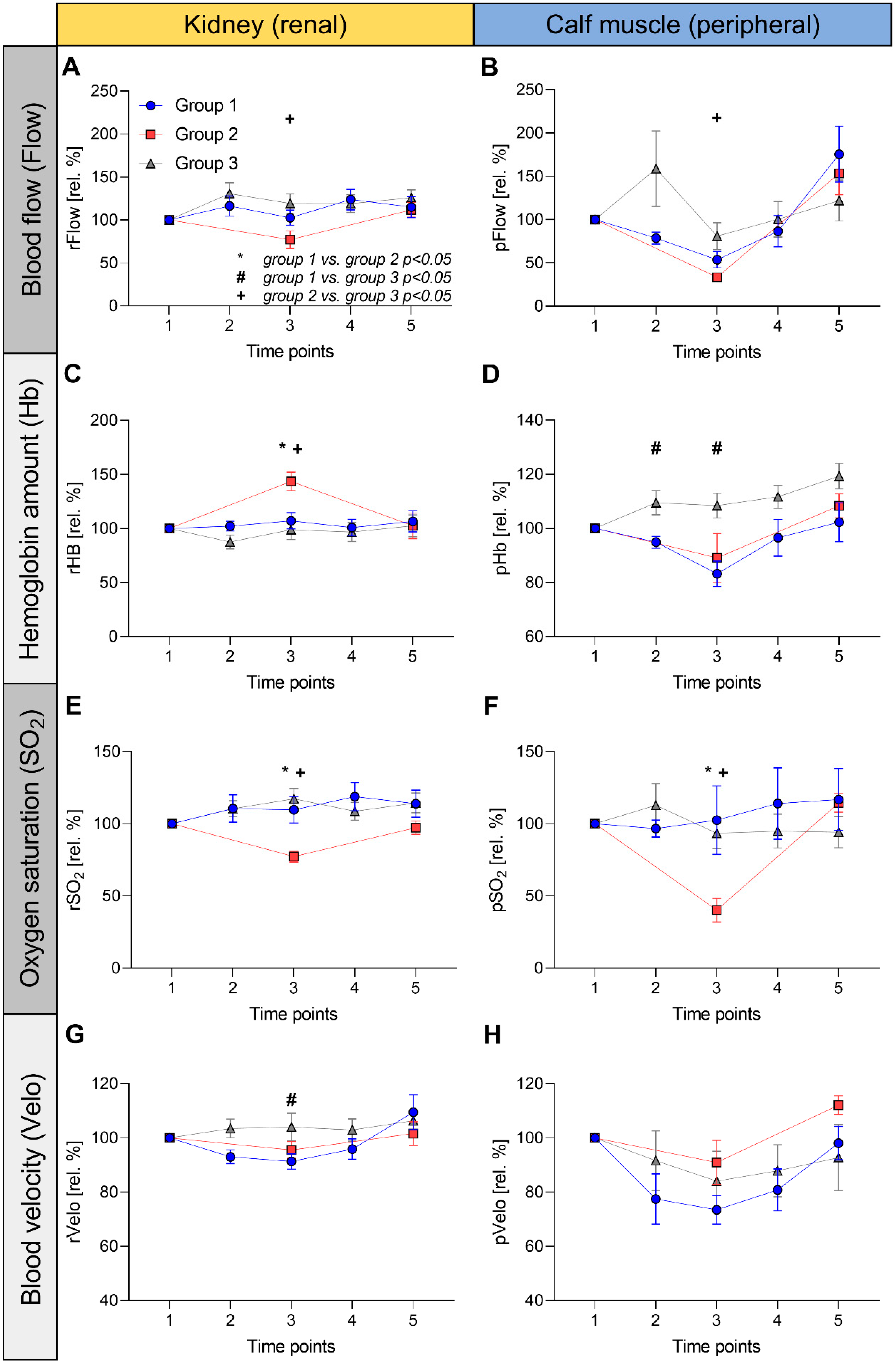
2.5. Monitoring of Tissue Oxygen Supply and Microperfusion
2.6. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Perfusion Kinetics
3.3. Renal (rFlow) and Peripheral Blood Flow (pFlow)
3.4. Renal (rHb) and Peripheral Hemoglobin Amount (pHb)
3.5. Renal (rSO2) and Peripheral Oxygen Saturation (pSO2)
3.6. Renal (rVelo) and Peripheral Blood Velocity (pVelo)
3.7. Between-Group Comparisons of rHb and rSO2
3.8. Laboratory Values
3.9. Clinical Course
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAR | aortic arch reconstruction |
| ACP | antegrade cerebral perfusion |
| ASAT | aspartate aminotransferase |
| AU | arbitrary unit(s) |
| CPB | cardiopulmonary bypass |
| CHD | congenital heart disease |
| DHCA | deep hypothermic circulatory arrest |
| Flow | Relative blood flow quantified by the O2C device |
| Hb | Relative hemoglobin amount quantified by the O2C device |
| ICU | intensive care unit |
| LBP | lower body perfusion |
| p | peripheral |
| r | renal |
| SO2 | oxygen saturation of hemoglobin quantified by the O2C device |
| Velo | blood flow velocity quantified by the O2C device |
References
- Kulyabin, Y.Y.; Bogachev-Prokophiev, A.V.; Soynov, I.A.; Omelchenko, A.Y.; Zubritskiy, A.V.; Gorbatykh, Y.N. Clinical Assessment of Perfusion Techniques During Surgical Repair of Coarctation of Aorta With Aortic Arch Hypoplasia in Neonates: A Pilot Prospective Randomized Study. Semin. Thorac. Cardiovasc. Surg. 2020, 32, 860–871. [Google Scholar] [CrossRef] [PubMed]
- Kist-van Holthe tot Echten, J.E.; Goedvolk, C.A.; Doornaar, M.B.; van der Vorst, M.M.; Bosman-Vermeeren, J.M.; Brand, R.; van der Heijden, A.J.; Schoof, P.H.; Hazekamp, M.G. Acute renal insufficiency and renal replacement therapy after pediatric cardiopulmonary bypass surgery. Pediatr. Cardiol. 2001, 22, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Alkandari, O.; Eddington, K.A.; Hyder, A.; Gauvin, F.; Ducruet, T.; Gottesman, R.; Phan, V.; Zappitelli, M. Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: A two-center retrospective cohort study. Crit. Care 2011, 15, R146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumbert, S.D.; Kork, F.; Jackson, M.L.; Vanga, N.; Ghebremichael, S.J.; Wang, C.Y.; Eltzschig, H.K. Perioperative Acute Kidney Injury. Anesthesiology 2020, 132, 180–204. [Google Scholar] [CrossRef] [Green Version]
- Kulyabin, Y.Y.; Gorbatykh, Y.N.; Soynov, I.A.; Zubritskiy, A.V.; Voitov, A.V.; Bogachev-Prokophiev, A.V. Selective Antegrade Cerebral Perfusion With or Without Additional Lower Body Perfusion During Aortic Arch Reconstruction in Infants. World J. Pediatr. Congenit. Heart Surg. 2020, 11, 49–55. [Google Scholar] [CrossRef]
- Boburg, R.S.; Rosenberger, P.; Kling, S.; Jost, W.; Schlensak, C.; Magunia, H. Selective lower body perfusion during aortic arch surgery in neonates and small children. Perfusion 2020, 35, 621–625. [Google Scholar] [CrossRef] [Green Version]
- Neunhoeffer, F.; Wiest, M.; Sandner, K.; Renk, H.; Heimberg, E.; Haller, C.; Kumpf, M.; Schlensak, C.; Hofbeck, M. Non-invasive measurement of renal perfusion and oxygen metabolism to predict postoperative acute kidney injury in neonates and infants after cardiopulmonary bypass surgery. Br. J. Anaesth. 2016, 117, 623–634. [Google Scholar] [CrossRef] [Green Version]
- Schindler, E.; Photiadis, J.; Lagudka, S.; Fink, C.; Hraska, V.; Asfour, B. Influence of two perfusion strategies on oxygen metabolism in paediatric cardiac surgery. Evaluation of the high-flow, low-resistance technique. Eur. J. Cardiothorac. Surg. 2010, 37, 651–657. [Google Scholar] [CrossRef] [Green Version]
- Forst, T.; Hohberg, C.; Tarakci, E.; Forst, S.; Kann, P.; Pfützner, A. Reliability of lightguide spectrophotometry (O2C) for the investigation of skin tissue microvascular blood flow and tissue oxygen supply in diabetic and nondiabetic subjects. J. Diabetes Sci. Technol. 2008, 2, 1151–1156. [Google Scholar] [CrossRef]
- Neunhoeffer, F.; Hofbeck, M.; Schuhmann, M.U.; Fuchs, J.; Schlensak, C.; Esslinger, M.; Gerbig, I.; Icheva, V.; Heimberg, E.; Kumpf, M.; et al. Cerebral Oxygen Metabolism Before and After RBC Transfusion in Infants Following Major Surgical Procedures. Pediatr. Crit. Care Med. 2018, 19, 318–327. [Google Scholar] [CrossRef]
- Neunhoeffer, F.; Michel, J.; Nehls, W.; Marx, M.; Mustafi, M.; Magunia, H.; Schuhmann, M.; Schlensak, C.; Hofbeck, M. Perioperative Assessment of Cerebral Oxygen Metabolism in Infants With Functionally Univentricular Hearts Undergoing the Bidirectional Cavopulmonary Connection. Pediatr. Crit. Care Med. 2019, 20, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Neunhoeffer, F.; Hofbeck, M.; Schlensak, C.; Schuhmann, M.U.; Michel, J. Perioperative Cerebral Oxygenation Metabolism in Neonates with Hypoplastic Left Heart Syndrome or Transposition of the Great Arteries. Pediatr. Cardiol. 2018, 39, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Neunhoeffer, F.; Sandner, K.; Wiest, M.; Haller, C.; Renk, H.; Kumpf, M.; Schlensak, C.; Hofbeck, M. Non-invasive assessment of cerebral oxygen metabolism following surgery of congenital heart disease. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 96–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neunhoeffer, F.; Warmann, S.W.; Hofbeck, M.; Muller, A.; Fideler, F.; Seitz, G.; Schuhmann, M.U.; Kirschner, H.J.; Kumpf, M.; Fuchs, J. Elevated intrathoracic CO2 pressure during thoracoscopic surgery decreases regional cerebral oxygen saturation in neonates and infants-A pilot study. Paediatr. Anaesth. 2017, 27, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Pigula, F.A.; Gandhi, S.K.; Siewers, R.D.; Davis, P.J.; Webber, S.A.; Nemoto, E.M. Regional low-flow perfusion provides somatic circulatory support during neonatal aortic arch surgery. Ann. Thorac. Surg. 2001, 72, 401–406; discussion 406–407. [Google Scholar] [CrossRef] [PubMed]
- Blinder, J.J.; Asaro, L.A.; Wypij, D.; Selewski, D.T.; Agus, M.S.D.; Gaies, M.; Ferguson, M.A. Acute Kidney Injury After Pediatric Cardiac Surgery: A Secondary Analysis of the Safe Pediatric Euglycemia After Cardiac Surgery Trial. Pediatr. Crit. Care Med. 2017, 18, 638–646. [Google Scholar] [CrossRef]
- Shteyer, E.; Yatsiv, I.; Sharkia, M.; Milgarter, E.; Granot, E. Serum transaminases as a prognostic factor in children post cardiac surgery. Pediatr. Int. 2011, 53, 725–728. [Google Scholar] [CrossRef]
- Pasternack, D.M.; AlQahtani, M.; Zonana Amkie, R.; Sosa, L.J.; Reyes, M.; Sasaki, J. Risk factors and outcomes for hyperbilirubinaemia after heart surgery in children. Cardiol. Young 2020, 30, 761–768. [Google Scholar] [CrossRef]
- Asou, T.; Kado, H.; Imoto, Y.; Shiokawa, Y.; Tominaga, R.; Kawachi, Y.; Yasui, H. Selective cerebral perfusion technique during aortic arch repair in neonates. Ann. Thorac. Surg. 1996, 61, 1546–1548. [Google Scholar] [CrossRef]
- Kornilov, I.A.; Sinelnikov, Y.S.; Soinov, I.A.; Ponomarev, D.N.; Kshanovskaya, M.S.; Krivoshapkina, A.A.; Gorbatykh, A.V.; Omelchenko, A.Y. Outcomes after aortic arch reconstruction for infants: Deep hypothermic circulatory arrest versus moderate hypothermia with selective antegrade cerebral perfusion. Eur. J. Cardiothorac. Surg. 2015, 48, e45–e50. [Google Scholar] [CrossRef]
- Gupta, B.; Dodge-Khatami, A.; Tucker, J.; Taylor, M.B.; Maposa, D.; Urencio, M.; Salazar, J.D. Antegrade cerebral perfusion at 25 degrees C for arch reconstruction in newborns and children preserves perioperative cerebral oxygenation and serum creatinine. Transl. Pediatr. 2016, 5, 114–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algra, S.O.; Schouten, A.N.; van Oeveren, W.; van der Tweel, I.; Schoof, P.H.; Jansen, N.J.; Haas, F. Low-flow antegrade cerebral perfusion attenuates early renal and intestinal injury during neonatal aortic arch reconstruction. J. Thorac. Cardiovasc. Surg. 2012, 144, 1323–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesnjevar, R.A.; Purbojo, A.; Muench, F.; Juengert, J.; Rueffer, A. Goal-directed-perfusion in neonatal aortic arch surgery. Transl. Pediatr. 2016, 5, 134–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Doblas, J.; Ortega-Loubon, C.; Pérez-Andreu, J.; Linés, M.; Fernández-Molina, M.; Abella, R.F. Selective visceral perfusion improves renal flow and hepatic function in neonatal aortic arch repair. Interact. CardioVascular Thorac. Surg. 2018, 27, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajagopal, S.K.; Emani, S.M.; Roy, N.; Westgate, L.; Bacha, E.A. Acute kidney injury and regional abdominal perfusion during neonatal aortic arch reconstruction. J. Thorac. Cardiovasc. Surg. 2010, 140, 453–458. [Google Scholar] [CrossRef] [Green Version]
- Hammel, J.M.; Deptula, J.J.; Karamlou, T.; Wedemeyer, E.; Abdullah, I.; Duncan, K.F. Newborn Aortic Arch Reconstruction With Descending Aortic Cannulation Improves Postoperative Renal Function. Ann. Thorac. Surg. 2013, 96, 1721–1726. [Google Scholar] [CrossRef]
- Raees, M.A.; Morgan, C.D.; Pinto, V.L.; Westrick, A.C.; Shannon, C.N.; Christian, K.G.; Mettler, B.A.; Bichell, D.P. Neonatal Aortic Arch Reconstruction With Direct Splanchnic Perfusion Avoids Deep Hypothermia. Ann. Thorac. Surg. 2017, 104, 2054–2063. [Google Scholar] [CrossRef] [Green Version]
- Baehner, T.; Breuer, J.; Heinze, I.; Duerr, G.D.; Dewald, O.; Velten, M. Low-body-perfusion via an arterial sheath reduces inflammation after aortic arch reconstruction surgery. Eur. J. Inflamm. 2021, 19, 205873922110005. [Google Scholar] [CrossRef]
- Chaudhry, R.; Wanderer, J.P.; Mubashir, T.; Kork, F.; Morse, J.; Waseem, R.; Zaki, J.F.; Shaw, A.D.; Eltzschig, H.K.; Liang, Y. Incidence and Predictive Factors of Acute Kidney Injury After Off-pump Lung Transplantation. J. Cardiothorac. Vasc. Anesth. 2022, 36, 93–99. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Group 1 CPB with ACP and LBP | Group 2 CoA Resection | Group 3 Standard CPB | p Value | |
|---|---|---|---|---|
| N | 9 | 5 | 9 | - |
| Age (days) | 14 (IQR 10 to 48) | 7 (IQR 6 to 89) | 11 (IQR 7.5 to 14.5) | 0.54 |
| Sex (n, %) | ||||
| Male Female | 5 (56%) 4 (44%) | 3 (60%) 2 (40%) | 7 (78%) 2 (22%) | ns |
| Weight (kg) | 3.6 (IQR 3.1 to 3.75) | 3.3 (IQR 2.75 to 5.9) | 3.8 (IQR 3.4 to 4) | 0.32 |
| BSA (m2) | 0.22 (IQR 0.195 to 0.23) | 0.22 (IQR 0.22 to 0.26) | 0.22 (0.22 to 0.24) | 0.56 |
| Diagnoses (n, %) | ||||
| HLHS Aortic arch hypoplasia +/− other defects DILV + TGA CoA TGA (+/− VSD) DORV CoA + VSD | 3 (33%) 5 (56%) 1 (11%) - - - - | - - - 5 (100%) - - - | - - - - 7 (78%) 1 (11%) 1 (11%) | - - - - - - - |
| Intraoperative and CPB data | ||||
| CPB time (min) | 150 (IQR 101 to 178) | - | 154 (IQR 151 to 183) | 0.13 |
| Aortic cross clamp time (min) | 82 (IQR 64 to 134) | - | 130 (IQR 107 to 175) | 0.06 |
| Lower body perfusion time (min) | 47 (IQR 41 to 74) | - | - | - |
| Reperfusion time (min) | 34 (IQR 14 to 63) | 15 (IQR 12 to 20) | 0.14 | |
| Lowest intraoperative temperature (°C) | 31.3 (IQR 30 to 31.9) | 37.3 (IQR 36.1 to 38) | 33.7 (IQR 31.5 to 35) | <0.001 a |
| Lactate (mmol/L) | Creatinine (mg/dL) | LDH | ASAT | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-CPB | CPB | ICU adm. | ICU 24 h | Pre-CPB | ICU adm. | ICU 24 h | Pre-CPB | ICU adm. | ICU 24 h | Pre-CPB | ICU adm. | ICU 24 h | |
| Group 1 (CPB with ACP and LBP) | 0.9 ± 0.5 | 2.0 ± 1.2 | 3.4 ± 1.7 | 1.6 (1.4 to 2) | 0.5 ± 0.2 | 0.5 ± 0.2 | 0.5 (0.5 to 0.8) | 326 ± 54 | 455 ± 208 | 406 (296 to 614) | 31 (23 to 48) | 136 ± 71 | 58 (39 to 157) |
| Group 2 (off-pump CoA Resection) | 0.9 ± 0.4 | 2.0 ± 0.7 | 1.5 ± 0.5 | 1.1 ± 0.4 | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.1 | 383 ± 113 | 327 ± 84 | 335 ± 75 | 49 ± 26 | 46 ± 22 | 30 ± 4 |
| Group 3 (Standard CPB) | 0.9 ± 0.4 | 1.7 ± 0.8 | 2.9 ± 0.9 | 1.4 ± 0.5 | 0.5 ± 0.2 | 0.4 ± 0.2 | 0.5 ± 0.2 | 336 ± 68 | 491 ± 192 | 371 ± 160 | 31 ± 17 | 130 ± 38 | 43 (38 to 88) |
| p value | 0.94 | 0.56 | <0.01 ab | 0.13 | 0.28 | 0.46 | 0.13 | 0.66 | 0.05 | 0.49 | 0.26 | <0.001 ab | 0.02 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magunia, H.; Nester, J.; Sandoval Boburg, R.; Schlensak, C.; Rosenberger, P.; Hofbeck, M.; Keller, M.; Neunhoeffer, F. Abdominal and Peripheral Tissue Oxygen Supply during Selective Lower Body Perfusion for the Surgical Repair of Congenital Heart Disease: A Pilot Study. J. Cardiovasc. Dev. Dis. 2022, 9, 436. https://doi.org/10.3390/jcdd9120436
Magunia H, Nester J, Sandoval Boburg R, Schlensak C, Rosenberger P, Hofbeck M, Keller M, Neunhoeffer F. Abdominal and Peripheral Tissue Oxygen Supply during Selective Lower Body Perfusion for the Surgical Repair of Congenital Heart Disease: A Pilot Study. Journal of Cardiovascular Development and Disease. 2022; 9(12):436. https://doi.org/10.3390/jcdd9120436
Chicago/Turabian StyleMagunia, Harry, Jana Nester, Rodrigo Sandoval Boburg, Christian Schlensak, Peter Rosenberger, Michael Hofbeck, Marius Keller, and Felix Neunhoeffer. 2022. "Abdominal and Peripheral Tissue Oxygen Supply during Selective Lower Body Perfusion for the Surgical Repair of Congenital Heart Disease: A Pilot Study" Journal of Cardiovascular Development and Disease 9, no. 12: 436. https://doi.org/10.3390/jcdd9120436