
Kidney Failure among Patients with Takotsubo Syndrome or Myocardial Infarction: A Retrospective Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Statistics
4. Results
4.1. Baseline Demographics
4.2. Clinical Presentation
4.3. Echocardiographic Characteristics
4.4. In-Hospital Outcomes
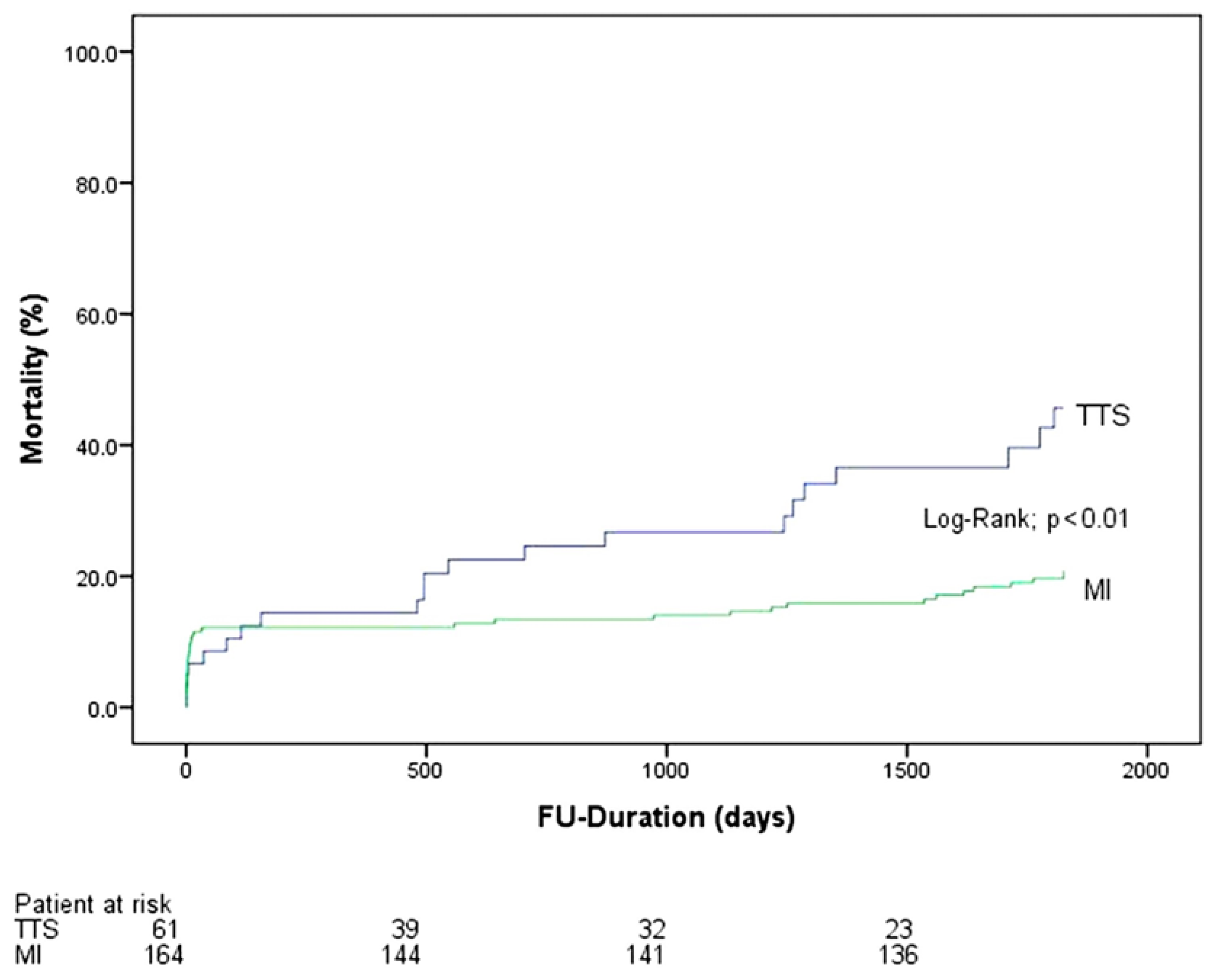
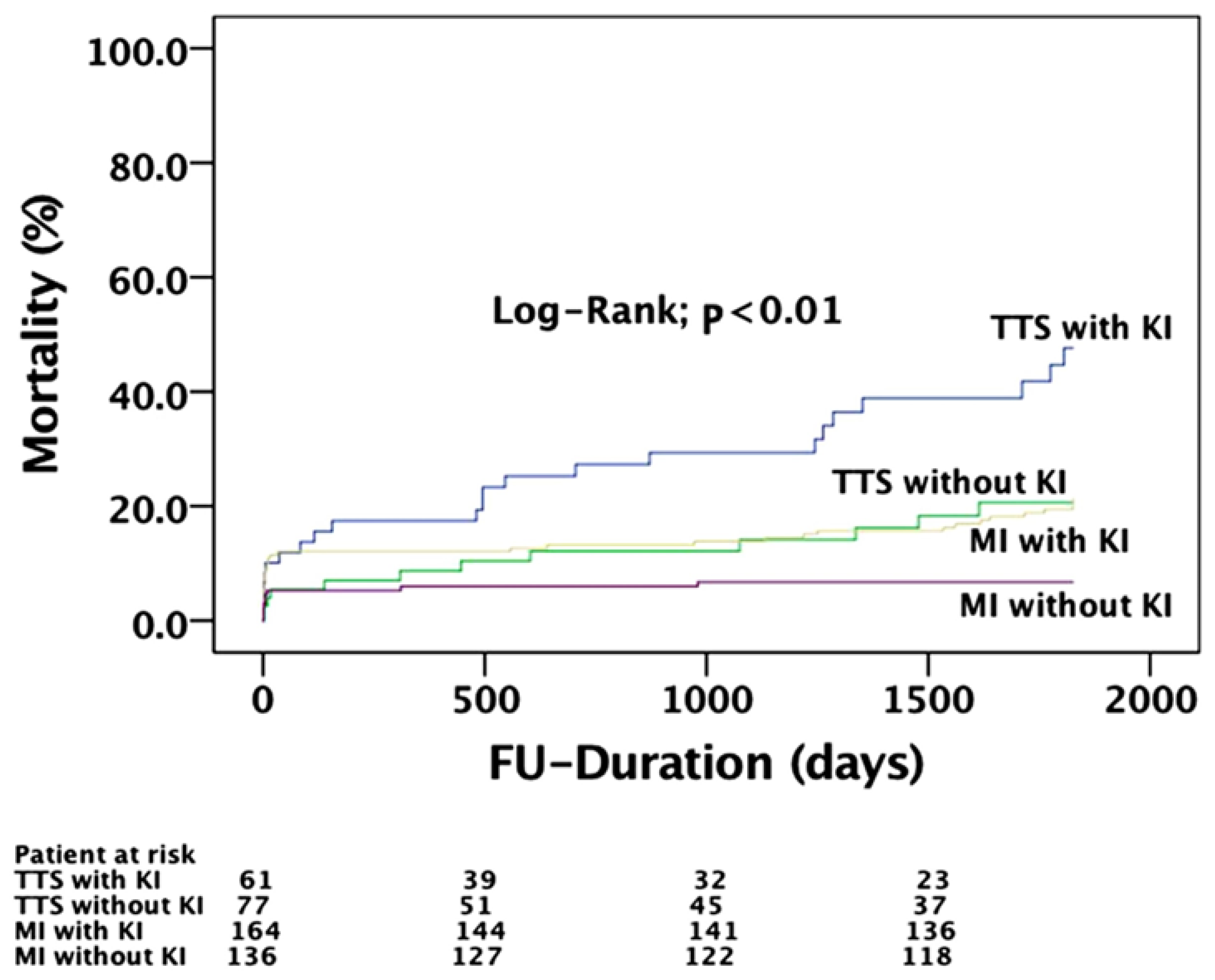
4.5. Long-Term Outcomes
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korlakunta, H.L.; Thambidorai, S.K.; Denney, S.D.; Khan, I.A. Transient left ventricular apical ballooning: A novel heart syndrome. Int. J. Cardiol. 2005, 102, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Fazio, G.; Novo, G.; Azzarelli, S.; Evola, S.; Barbaro, G.; Sutera, L.; di Gesaro, G.; Akashi, Y.J.; Novo, S. Transient mid-ventricular dyskinesia: A variant of Takotsubo syndrome. Int. J. Cardiol. 2008, 129, 272–273. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Santoro, F.; Stiermaier, T.; Moller, C.; Guastafierro, F.; Novo, G.; Novo, S.; Mariano, E.; Romeo, F.; Romeo, F.; et al. Incidence and Clinical Impact of Right Ventricular Involvement (Biventricular Ballooning) in Takotsubo Syndrome: Results from the GEIST Registry. Chest 2021, 160, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- Templin, C.; Ghadri, J.R.; Diekmann, J.; Napp, L.C.; Bataiosu, D.R.; Jaguszewski, M.; Cammann, V.L.; Sarcon, A.; Geyer, V.; Neumann, C.A.; et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N. Engl. J. Med. 2015, 373, 929–938. [Google Scholar] [CrossRef] [Green Version]
- Yasu, T.; Tone, K.; Kubo, N.; Saito, M. Transient mid-ventricular ballooning cardiomyopathy: A new entity of Takotsubo cardiomyopathy. Int. J. Cardiol. 2006, 110, 100–101. [Google Scholar] [CrossRef] [PubMed]
- Tsuchihashi, K.; Ueshima, K.; Uchida, T.; Oh-mura, N.; Kimura, K.; Owa, M.; Yoshiyama, M.; Miyazaki, S.; Haze, K.; Ogawa, H.; et al. Transient left ventricular apical ballooning without coronary artery stenosis: A novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J. Am. Coll. Cardiol. 2001, 38, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Dote, K.; Sato, H.; Tateishi, H.; Uchida, T.; Ishihara, M. Myocardial stunning due to simultaneous multivessel coronary spasms: A review of 5 cases. J. Cardiol. 1991, 21, 203–214. [Google Scholar] [PubMed]
- Wittstein, I.S.; Thiemann, D.R.; Lima, J.A.; Baughman, K.L.; Schulman, S.P.; Gerstenblith, G.; Wu, K.C.; Rade, J.J.; Bivalacqua, T.J.; Champion, H.C. Neurohumoral features of myocardial stunning due to sudden emotional stress. N. Engl. J. Med. 2005, 352, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Aweimer, A.; El-Battrawy, I.; Akin, I.; Borggrefe, M.; Mugge, A.; Patsalis, P.C.; Urban, A.; Kummer, M.; Vasileva, S.; Stachon, A.; et al. Abnormal thyroid function is common in takotsubo syndrome and depends on two distinct mechanisms: Results of a multicentre observational study. J. Intern. Med. 2021, 289, 675–687. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Borggrefe, M.; Akin, I. Endothelial dysfunction in takotsubo syndrome. Int. J. Cardiol. 2016, 234, 101. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Borggrefe, M.; Akin, I. Hormone Status Correlates With Incidence of Heart Failure. J. Am. Coll. Cardiol. 2017, 70, 2312–2313. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Borggrefe, M.; Akin, I. The current evidence of Takotsubo syndrome. Future Cardiol. 2021, 17, 1293–1295. [Google Scholar] [CrossRef]
- Becher, T.; El-Battrawy, I.; Baumann, S.; Fastner, C.; Behnes, M.; Lossnitzer, D.; Elmas, E.; Hoffmann, U.; Papavassiliu, T.; Kuschyk, J.; et al. Characteristics and long-term outcome of right ventricular involvement in Takotsubo cardiomyopathy. Int. J. Cardiol. 2016, 220, 371–375. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Lang, S.; Ansari, U.; Behnes, M.; Hillenbrand, D.; Schramm, K.; Fastner, C.; Zhou, X.; Bill, V.; Hoffmann, U.; et al. Impact of concomitant atrial fibrillation on the prognosis of Takotsubo cardiomyopathy. Europace 2017, 19, 1288–1292. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Lang, S.; Ansari, U.; Tulumen, E.; Schramm, K.; Fastner, C.; Zhou, X.; Hoffmann, U.; Borggrefe, M.; Akin, I. Prevalence of malignant arrhythmia and sudden cardiac death in takotsubo syndrome and its management. Europace 2017, 20, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Ionescu, C.N.; Aguilar-Lopez, C.A.; Sakr, A.E.; Ghantous, A.E.; Donohue, T.J. Long-term outcome of Tako-tsubo cardiomyopathy. Heart Lung Circ. 2010, 19, 601–605. [Google Scholar] [CrossRef]
- Stiermaier, T.; Thiele, H.; Eitel, I. Prognosis in Patients With Takotsubo Cardiomyopathy. JACC Heart Fail. 2016, 4, 519–520. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Cammann, V.L.; Kato, K.; Szawan, K.A.; di Vece, D.; Rossi, A.; Wischnewsky, M.; Hermes-Laufer, J.; Gili, S.; Citro, R.; et al. Impact of Atrial Fibrillation on Outcome in Takotsubo Syndrome: Data from the International Takotsubo Registry. J. Am. Heart Assoc. 2021, 10, e014059. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Santoro, F.; Stiermaier, T.; Moller, C.; Guastafierro, F.; Novo, G.; Novo, S.; Santangelo, A.; Mariano, E.; Romeo, F.; et al. Prevalence, management, and outcome of adverse rhythm disorders in takotsubo syndrome: Insights from the international multicenter GEIST registry. Heart Fail. Rev. 2020, 25, 505–511. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Behnes, M.; Hillenbrand, D.; Haghi, D.; Hoffmann, U.; Papavassiliu, T.; Lang, S.; Fastner, C.; Becher, T.; Baumann, S.; et al. Prevalence, Clinical Characteristics, and Predictors of Patients with Thromboembolic Events in Takotsubo Cardiomyopathy. Clin. Med. Insights Cardiol. 2016, 10, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Gili, S.; Cammann, V.L.; Schlossbauer, S.A.; Kato, K.; D’Ascenzo, F.; di Vece, D.; Jurisic, S.; Micek, J.; Obeid, S.; Bacchi, B.; et al. Cardiac Arrest in Takotsubo Syndrome: Results from the InterTAK Registry. Eur Heart J. 2019, 40, 2142–2151. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Gietzen, T.; Ansari, U.; Behnes, M.; Lang, S.; Zhou, X.; Borggrefe, M.; Akin, I. Short-term and long-term incidence of stroke in Takotsubo syndrome. ESC Heart Fail. 2018, 5, 1191–1194. [Google Scholar] [CrossRef]
- Ando, K.; Sukekawa, H.; Takahata, A.; Kobari, Y.; Tsuchiya, H.; Ishigaki, D.; Tamabuchi, T.; Koyama, Y. Renal dysfunction indicative of outcomes in hospitalized patients with takotsubo syndrome. Eur Heart J. Acute Cardiovasc. Care 2017, 7, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Bill, V.; El-Battrawy, I.; Hoffmann, U.; Haghi, D.; Kuschyk, J.; Borggrefe, M.; Akin, I. Takotsubo Cardiomyopathy: Another Form of Cardiorenal Syndrome. Angiology 2018, 69, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Cabiati, A.; Bertoli, S.V.; Assanelli, E.; Marana, I.; de Metrio, M.; Rubino, M.; Moltrasio, M.; Grazi, M.; Campodonico, J.; et al. Incidence and relevance of acute kidney injury in patients hospitalized with acute coronary syndromes. Am. J. Cardiol. 2013, 111, 816–822. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, M.; Prasad, A. Proposed Mayo Clinic criteria for the diagnosis of Tako-Tsubo cardiomyopathy and long-term prognosis. Herz 2010, 35, 240–243. [Google Scholar] [CrossRef]
- Cammann, V.L.; Sarcon, A.; Ding, K.J.; Seifert, B.; Kato, K.; di Vece, D.; Szawan, K.A.; Gili, S.; Jurisic, S.; Bacchi, B.; et al. Clinical Features and Outcomes of Patients With Malignancy and Takotsubo Syndrome: Observations from the International Takotsubo Registry. J. Am. Heart Assoc. 2019, 8, e010881. [Google Scholar] [CrossRef] [Green Version]
- Pelliccia, F.; Parodi, G.; Greco, C.; Antoniucci, D.; Brenner, R.; Bossone, E.; Cacciotti, L.; Capucci, A.; Citro, R.; Delmas, C.; et al. Comorbidities frequency in Takotsubo syndrome: An international collaborative systematic review including 1109 patients. Am. J. Med. 2015, 128, 654.e11–654.e19. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Nguyen, P. Takotsubo Cardiomyopathy Due to Systemic Absorption of Intraocular Phenylephrine. Heart Lung Circ. 2016, 25, e159–e161. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthelemy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelliccia, F.; Kaski, J.C.; Crea, F.; Camici, P.G. Pathophysiology of Takotsubo Syndrome. Circulation 2017, 135, 2426–2441. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; Bossone, E.; Schneider, B.; Sechtem, U.; Citro, R.; Underwood, S.R.; Sheppard, M.N.; Figtree, G.A.; Parodi, G.; Akashi, Y.J.; et al. Current state of knowledge on Takotsubo syndrome: A Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2016, 18, 8–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khwaja, Y.H.; Tai, J.M. Takotsubo cardiomyopathy with use of salbutamol nebulisation and aminophylline infusion in a patient with acute asthma exacerbation. BMJ Case Rep. 2016, 2016, bcr2016217364. [Google Scholar] [CrossRef] [PubMed]
- Rasiah, S.; Finger, R.P.; MacIsaac, A.I.; Lim, L.L. Takotsubo syndrome caused by subconjunctival injection of a mydricaine analogue. Clin. Exp. Ophthalmol. 2016, 44, 624–625. [Google Scholar] [CrossRef]
- Eitel, I.; Lucke, C.; Behrendt, F.; Sareban, M.; Gutberlet, M.; Schuler, G.; Thiele, H. Full recovery of Takotsubo cardiomyopathy (apical ballooning) in two days. Int. J. Cardiol. 2010, 143, e51–e53. [Google Scholar] [CrossRef]
- Huang, M.; Fan, X.; Yang, Z.; Cyganek, L.; Li, X.; Yuecel, G.; Lan, H.; Li, Y.; Wendel, A.; Lang, S.; et al. Alpha 1-adrenoceptor signalling contributes to toxic effects of catecholamine on electrical properties in cardiomyocytes. Europace 2021, 23, 1137–1148. [Google Scholar] [CrossRef]
- Ishikura, F.; Takano, Y.; Ueyama, T. Acute effects of beta-blocker with intrinsic sympathomimetic activity on stress-induced cardiac dysfunction in rats. J. Cardiol. 2012, 60, 470–474. [Google Scholar] [CrossRef] [Green Version]
- Brunetti, N.D.; Santoro, F.; de Gennaro, L.; Correale, M.; Gaglione, A.; di Biase, M.; Madias, J.E. Combined therapy with beta-blockers and ACE-inhibitors/angiotensin receptor blockers and recurrence of Takotsubo (stress) cardiomyopathy: A meta-regression study. Int. J. Cardiol. 2017, 230, 281–283. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | TTS (n = 61) | MI (n = 164) | p Value * |
|---|---|---|---|
| Demographics | |||
| Age. Mean ± SD | 69 ± 11 | 71 ± 11 | 0.12 |
| Female (%) | 47 (77.0) | 40 (24.4) | <0.01 |
| Symptoms. N (%) | |||
| Dyspnoe | 24 (39.3) | 53 (32.3) | 0.32 |
| Chest pain | 31 (51.7) | 118(72.0) | <0.01 |
| Clinic parameter | |||
| Systolic BP. mmHg | 132 (90–200) | 137 (80–250) | 0.65 |
| Diastolic BP. mmHg | 77 (50–110) | 77 (30–150) | 0.55 |
| Heart rate. Bpm | 100 ± 25 | 79 ± 19 | <0.01 |
| ECG Data. N (%) | |||
| ST-segment elevation | 16 (26.2) | 74 (45.1) | 0.01 |
| Inversed T-Waves | 56 (93.3) | 119 (72.6) | <0.01 |
| PQ-interval | 166 ± 28 | 173 ± 33 | <0.01 |
| QTc (ms) | 468 (374–554) | 448 (324–569) | 0.53 |
| Laboratory values. Mean ± SD | |||
| Troponin I (U/L) (IQR) | 48.13 (0.01–2631) | 28.83 (0.01–1704) | 0.50 |
| Creatine phosphatkinase (U/L) (IQR) | 993 (39–26,600) | 909 (30–12,092) | 0.39 |
| CKMB (U/L) (IQR) | 43 (2–415) | 88 (0–1208) | 0.34 |
| C-Reactive protein (mg/L) (IQR) | 61.3 (0.4–467.1) | 34.3 (0.0–247.9) | 0.34 |
| Hemoglobin (g/dL) (IQR) | 12.0 ± 2.4 | 13.2 ±2.4 | 0.03 |
| Creatinine (mg/dL) (IQR) | 1.52 (1.01–2.83) | 1.50 (1.00–12.16) | 0.38 |
| Echocardiography data. N (%) | |||
| LV EF% | 37 ± 10 | 48 ± 14 | <0.01 |
| LV EF% follow-up | 49 ± 14 | 48 ± 14 | 1.00 |
| Mitral regurgitation | 33 (54.1) | 66 (40.2) | 0.06 |
| Tricuspid regurgitation | 28 (45.9) | 37 (22.6) | <0.01 |
| Medical history. N (%) | |||
| Smoking | 15 (24.6) | 60 (36.6) | 0.09 |
| Diabetes mellitus | 13 (21.3) | 65 (39.6) | 0.01 |
| BMI > 25 kg/m2 | 13 (26.0) | 76 (46.3) | 0.01 |
| Hypertension | 36 (59.0) | 129 (78.7) | <0.01 |
| COPD | 11 (18.0) | 7 (4.3) | <0.01 |
| Atrial fibrillation | 14 (23.0) | 36 (22.0) | 0.87 |
| Coronary artery disease | 12 (19.7) | 137 (83.5) | <0.01 |
| History of malignancy | 8 (13.1) | 11 (6.7) | 0.12 |
| Drugs on admission. N (%) | |||
| Beta-blocker | 18 (32.1) | 79(48.5) | 0.03 |
| ACE inhibitor | 19 (33.9) | 63 (38.7) | 0.53 |
| Aldosteron inhibitor | 1 (1.8) | 2 (1.2) | 1.00 |
| ASS | 17 (30.4) | 74 (45.4) | 0.05 |
| Therapeutic anticoagulation | 2 (3.6) | 16 (9.8) | 0.15 |
| Drugs on discharge. N (%) | |||
| Beta-blocker | 42 (68.9) | 131 (79.9) | 0.08 |
| ACE inhibitor | 32(52.5) | 104 (63.4) | 0.14 |
| Aldosteron inhibitor | 0 (0.0) | 5 (3.0) | 0.33 |
| Aspirin | 26 (42.6) | 139 (84.8) | <0.01 |
| Therapeutic anticoagulation | 16 (26.2) | 15 (9.1) | <0.01 |
| Variables | TTS (n = 61) | MI (n = 164) | p Value * |
|---|---|---|---|
| Life-threatening arrhythmia | 9 (14.8) | 29 (17.7) | 0.60 |
| NPPV and or intubation | 40 (65.6) | 24 (14.6) | <0.01 |
| Inotropic agents | 15(24.6) | 26 (15.9) | 0.13 |
| Resuscitation | 7(11.5) | 25 (15.2) | 0.47 |
| ICD or pacemaker Implantation | 4 (6.6) | 44 (26.8) | <0.01 |
| Admission to ICU. length of stay (IQR) | 6 (0–52) | 3 (0–31) | 0.02 |
| In-hospital death | 6 (9.8) | 19 (11.6) | 0.71 |
| Cardiogenic Shock | 17 (27.9) | 30 (18.3) | 0.12 |
| Variables | TTS (n = 61) | MI (n = 164) | Relative Risk (95% CI) | p Value * |
|---|---|---|---|---|
| In-hospital mortality | 6 (9.8) | 19 (11.6) | 0.8 (0.4–2.0) | 0.71 |
| 30-day mortality | 5 (8.2) | 19 (11.6) | 0.7 (0.3–1.8) | 0.46 |
| Long-term mortality | 23 (37.7) | 34 (20.7) | 1.8 (1.2–2.8) | 0.02 |
| Cardiovascular cause of death | 7 (11.5) | 26 (15.9) | 0.7 (0.3–1.6) | 0.41 |
| Non-cardiovascular cause of death | 12 (19.7) | 5 (3.0) | 6.5 (2.4–17.6) | <0.01 |
| Unknown cause of death | 4 (6.6) | 4 (2.4) | 8.8 (1.0–73.5) | 0.22 |
| 30-day Stroke | 1 (1.6) | 1 (0.6) | 2.7 (0.2–42.3) | 0.47 |
| 1-year Stroke | 2 (3.3) | 1 (0.6) | 5.4 (0.5–58.2) | 0.18 |
| Long-term Stroke | 5 (8.2) | 4 (2.4) | 3.4 (0.9–12.1) | 0.06 |
| 30-day life-threatening arrythmia | 8 (13.1) | 21 (12.8) | 1.0 (0.5–2.2) | 0.95 |
| 1-year life-threatening arrythmia | 8 (13.1) | 22 (13.4) | 1.0 (0.5–2.0) | 0.95 |
| Long-term life-threatening arrythmia | 8 (13.1) | 36 (22.0) | 0.6 (0.3–1.2) | 0.14 |
| 30-day Heart Failure | 3 (4.9) | 27 (16.5) | 0.3 (0.1–0.9) | 0.02 |
| 1-year Heart Failure | 4 (6.6) | 33 (20.1) | 0.3 (0.1–0.9) | 0.02 |
| Long-term Heart Failure | 5 (8.2) | 44 (26.8) | 0.3 (0.1–0.7) | <0.01 |
| 30-day Recurrence | 0 (0.0) | 1 (0.6) | 1.00 | |
| 1-year Recurrence | 0 (0.0) | 10 (6.1) | 0.07 | |
| Long-term Recurrence | 3 (4.9) | 27 (16.5) | 0.3 (0.1–0.9) | 0.03 |
| 30-day Thromboembolic Events | 1 (1.6) | 0 (0.0) | 0.32 | |
| 1-year Thromboembolic Events | 1 (1.6) | 0 (0.0) | 0.27 | |
| Long-term Thromboembolic Events | 2 (3.3) | 5 (3.0) | 1.0 (0.2–5.4) | 1.00 |
| Multivariate Analysis for the End Point | ||||||
|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||||
| HR | 95%CI | p-Value | HR | 95%CI | p-Value | |
| Male | 2.2 | 1.0–5.0 | 0.04 | 2.7 | 1.1–6.5 | 0.02 |
| Age | 1.0 | 0.9–1.0 | 0.45 | |||
| EF < 35% | 2.1 | 1.1–4.3 | 0.02 | 1.3 | 0.5–2.9 | 0.49 |
| COPD | 1.1 | 0.4–2.4 | 0.85 | |||
| GFR < 60 mL/min | 2.4 | 1.2–4.9 | 0.01 | 2.8 | 1.2–6.0 | 0.01 |
| Cardiogenic shock | 4.6 | 2.2–9.3 | <0.01 | 2.7 | 0.6–11.8 | 0.18 |
| Inotropic drugs | 3.9 | 1.9–7.8 | <0.01 | 1.25 | 0.2–6.1 | 0.77 |
| DM Typ II | 1.0 | 0.4–2.2 | 0.97 | |||
| Hypertension | 0.7 | 0.3–1.5 | 0.41 | |||
| Apical ballooning | 1.8 | 0.7–4.3 | 0.18 | |||
| History of cancer | 2.8 | 1.3–6.4 | <0.01 | 3.6 | 1.4–9.3 | <0.01 |
| Smoking | 0.8 | 0.3–1.7 | 0.64 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bill, V.; El-Battrawy, I.; Kummer, M.; Mügge, A.; Aweimer, A.; Behnes, M.; Akin, I. Kidney Failure among Patients with Takotsubo Syndrome or Myocardial Infarction: A Retrospective Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 186. https://doi.org/10.3390/jcdd9060186
Bill V, El-Battrawy I, Kummer M, Mügge A, Aweimer A, Behnes M, Akin I. Kidney Failure among Patients with Takotsubo Syndrome or Myocardial Infarction: A Retrospective Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(6):186. https://doi.org/10.3390/jcdd9060186
Chicago/Turabian StyleBill, Verena, Ibrahim El-Battrawy, Marvin Kummer, Andreas Mügge, Assem Aweimer, Michael Behnes, and Ibrahim Akin. 2022. "Kidney Failure among Patients with Takotsubo Syndrome or Myocardial Infarction: A Retrospective Analysis" Journal of Cardiovascular Development and Disease 9, no. 6: 186. https://doi.org/10.3390/jcdd9060186
APA StyleBill, V., El-Battrawy, I., Kummer, M., Mügge, A., Aweimer, A., Behnes, M., & Akin, I. (2022). Kidney Failure among Patients with Takotsubo Syndrome or Myocardial Infarction: A Retrospective Analysis. Journal of Cardiovascular Development and Disease, 9(6), 186. https://doi.org/10.3390/jcdd9060186