
Diagnosis, Treatment, and Outcome of Coccidioidal Osseous Infections: A Systematic Review

 ,
,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
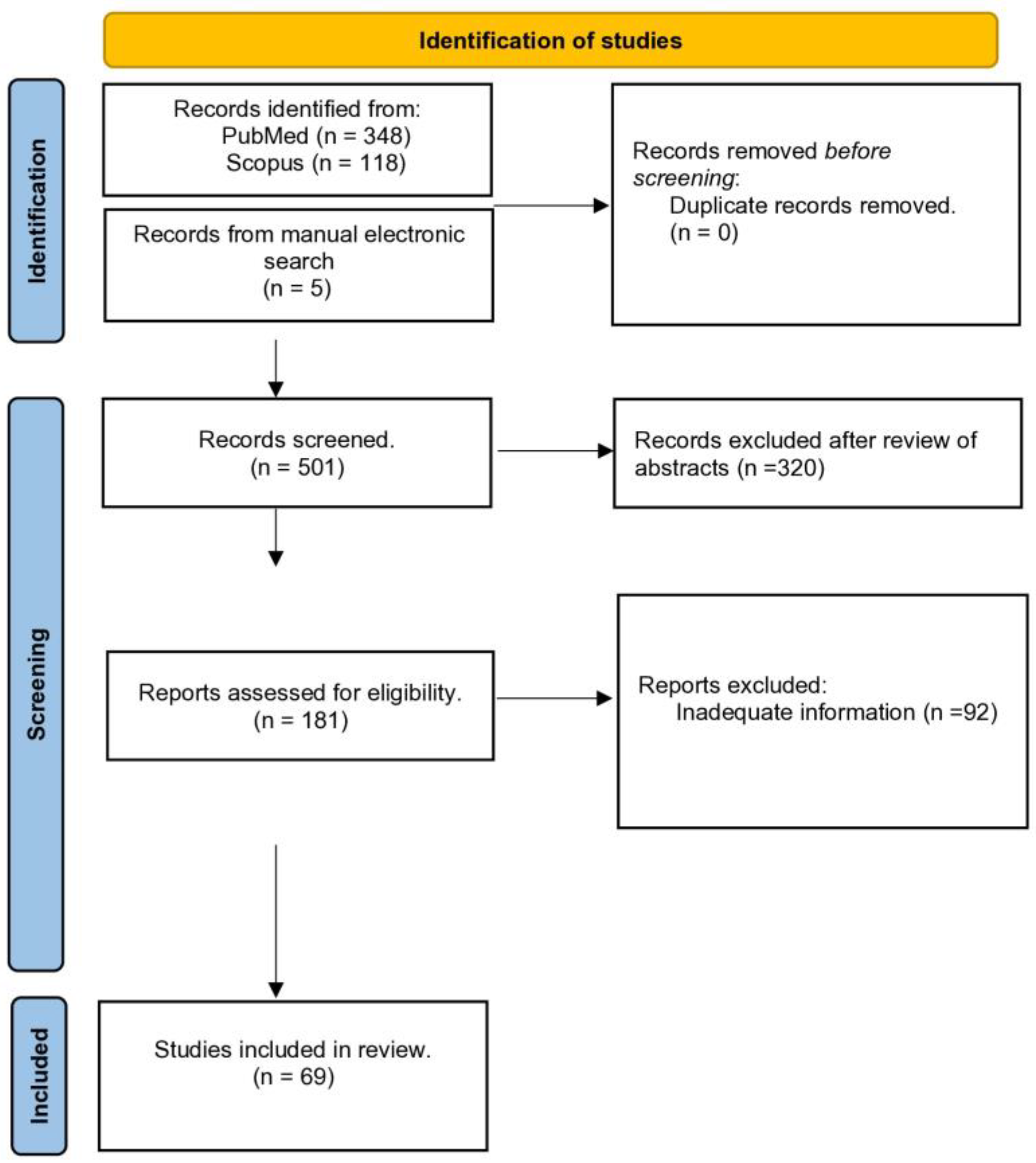
2.1. Search Protocol/Databases
2.2. Selection Criteria
2.3. Data Extraction and Data Analysis
3. Results
3.1. Study Characteristics and Patient Demographics
3.2. Microbiology and Location
3.3. Diagnostic Studies and Markers of Inflammation
3.4. Antibiotic Agents, Protocols, and Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Koutserimpas, C.; Naoum, S.; Melissinos, E.P.; Raptis, K.; Alpantaki, K.; Dretakis, K.; Piagkou, M.; Samonis, G. Spinal Infections Caused by Coccidioides Species. Maedica 2023, 18, 209–215. [Google Scholar] [CrossRef]
- Fisher, M.C.; Koenig, G.L.; White, T.J.; Taylor, J.W. Molecular and phenotypic description of Coccidioides posadasii sp. nov., previously recognized as the non-California population of Coccidioides immitis. Mycologia 2002, 94, 73. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Naoum, S.; Raptis, K.; Vrioni, G.; Samonis, G.; Alpantaki, K. Skeletal Infections Caused by Coccidioides Species. Diagnostics 2022, 12, 714. [Google Scholar] [CrossRef]
- Flynn, N.M.; Hoeprich, P.D.; Kawachi, M.M.; Lee, K.K.; Lawrence, R.M.; Goldstein, E.; Jordan, G.W.; Kundargi, R.S.; Wong, G.A. An unusual outbreak of windborne coccidioidomycosis. N. Engl. J. Med. 1979, 301, 358. [Google Scholar] [CrossRef]
- Ramanathan, D.; Sahasrabudhe, N.; Kim, E. Disseminated Coccidioidomycosis to the Spine-Case Series and Review of Literature. Brain Sci. 2019, 9, 160. [Google Scholar] [CrossRef]
- Acree, T.; Abreo, F.; Bagby, J. Coccidioidomycosis of the knee diagnosed by fine-needle aspiration: A case report. Diagn. Cytopathol. 1998, 19, 110–112. [Google Scholar] [CrossRef]
- Armbuster, T.G.; Goergen, T.G.; Resnick, D.; Catanzaro, A. Utility of bone scanning in disseminated coccidioidomycosis: Case report. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1977, 18, 450–454. [Google Scholar]
- Bayer, A.S.; Yoshikawa, T.T.; Galpin, J.E.; Guze, L.B. Unusual syndromes of coccidioidomycosis: Diagnostic and therapeutic considerations; a report of 10 cases and review of the English literature. Medicine 1976, 55, 131–152. [Google Scholar] [CrossRef]
- Bernreuter, W.K. Coccidioidomycosis of bone: A sequela of desert rheumatism. Arthritis Rheum. 1989, 32, 1608–1610. [Google Scholar] [CrossRef]
- Bickel, K.D.; Press, B.H.; Hovey, L.M. Successful treatment of coccidioidomycosis osteomyelitis in an infant. Ann. Plast. Surg. 1993, 30, 462–465. [Google Scholar] [CrossRef]
- Bried, J.M.; Speer, D.P.; Shehab, Z.M. Coccidioides immitis osteomyelitis in a 12-month-old child. J. Pediatr. Orthop. 1987, 7, 328–330. [Google Scholar] [CrossRef]
- Buckley, S.L.; Burkus, J.K. Coccidioidomycosis of the first cuneiform: Successful treatment utilizing local debridement and long-term ketoconazole therapy. Foot Ankle 1986, 6, 300–304. [Google Scholar] [CrossRef]
- Catanzaro, A.; Einstein, H.; Levine, B.; Ross, J.B.; Schillaci, R.; Fierer, J.; Friedman, P.J. Ketoconazole for treatment of disseminated coccidioidomycosis. Ann. Intern. Med. 1982, 96, 436–440. [Google Scholar] [CrossRef]
- Catanzaro, A.; Friedman, P.J.; Schillaci, R.; Einstein, H.; Kirkland, T.N.; Levine, H.B.; Ross, J.B. Treatment of coccidioidomycosis with ketoconazole: An evaluation utilizing a new scoring system. Am. J. Med. 1983, 74, 64–69. [Google Scholar] [CrossRef]
- Catanzaro, A.; Spitler, L.; Moser, K.M. Immunotherapy of coccidioidomycosis. J. Clin. Investig. 1974, 54, 690–701. [Google Scholar] [CrossRef]
- Delaney, P.; Niemann, B. Spinal cord compression by Coccidioides immitis abscess. Arch. Neurol. 1982, 39, 255–256. [Google Scholar] [CrossRef]
- Fraser, C.G.; Monroe, S.E.; O’Hare, J.E. Coccidioidomycosis and tuberculosis in the same bones; a case report. Ann. Surg. 1951, 133, 116–122. [Google Scholar] [CrossRef]
- Graybill, J.R.; Stevens, D.A.; Galgiani, J.N.; Dismukes, W.E.; Cloud, G.A. Itraconazole treatment of coccidioidomycosis. NAIAD Mycoses Study Group. Am. J. Med. 1990, 89, 282–290. [Google Scholar] [CrossRef]
- Horsburgh, C.R.; Cannady, P.B., Jr.; Kirkpatrick, C.H., Jr. Treatment of fungal infections in the bones and joints with ketoconazole. J. Infect. Dis. 1983, 147, 1064–1069. [Google Scholar] [CrossRef]
- Huang, J.I.; Seeger, L.L.; Jones, N.F. Coccidioidomycosis fungal infection in the hand mimicking a metacarpal enchondroma. J. Hand Surg. 2000, 25, 475–477. [Google Scholar] [CrossRef]
- Jackson, F.E.; Kent, D.; Clare, F. Quadriplegia caused by involvement of cervical spine with coccidioides immitis. Symptomatic cure after operation and amphotericin-b treatment. J. Neurosurg. 1964, 21, 512–515. [Google Scholar] [CrossRef]
- Lamphier, T.A. Localized coccidioidal osteomyelitis. N. Engl. J. Med. 1948, 238, 150–152. [Google Scholar] [CrossRef]
- Low, W.S.; Seid, A.B.; Pransky, S.M.; Kearns, D.B. Coccidioides immitis subperiosteal abscess of the temporal bone in a child. Arch. Otolaryngol.-Head Neck Surg. 1996, 122, 189–192. [Google Scholar] [CrossRef]
- Mazet, R., Jr. Skeletal lesions in coccidioidomycosis. AMA Arch. Surg. 1955, 70, 497–507. [Google Scholar] [CrossRef]
- McGahan, J.P.; Graves, D.S.; Palmer, P.E. Coccidioidal spondylitis: Usual and unusual radiographic manifestations. Radiology 1980, 136, 5–9. [Google Scholar] [CrossRef]
- Mishra, D.D.; Mohanty, A. Coccidioidal osteomyelitis of a metatarsal. A Case Report. Int. Orthop. 1991, 15, 323–324. [Google Scholar] [CrossRef]
- Stein, S.R.; Leukens, C.A.; Bagg, R.J. Treatment of coccidioidomycosis infection of bone with local amphotericin B suction-irrigation. Report of a case. Clin. Orthop. Relat. Res. 1975, 108, 161–164. [Google Scholar] [CrossRef]
- Wascher, D.C.; Hartman, G.P.; Salka, C.; Mertz, G.J. Coccidiomycosis presenting as a popliteal cyst. Arthrosc.-J. Arthrosc. Relat. Surg. 1998, 14, 99–102. [Google Scholar] [CrossRef]
- Ramírez Zamora, J.A.; Delgadillo Vargas, J.A.; Medina González, R.; Hayakawa Dávila, V.C.; Acevedo Rodarte, A.Y.; Arellano Pérez Vertti, R.D. Coccidioidomycosis Osteomyelitis of Distal Tibia in a Preschool Girl: A Case Report. J. Orthop. Case Rep. 2022, 12, 66–69. [Google Scholar] [CrossRef]
- Abdollahi Zarandi, P.; Antony, S.; Sotelo-Rafiq, E. A Case of Primary Osteomyelitis of the Rib with Involvement of the Chest Wall, Presenting as a Non-Healing Abscess. Cureus 2022, 14, e26974. [Google Scholar] [CrossRef]
- Azeem, A.; Quimby, D.; Krajicek, B.; Horne, J. (Ig)Easy diagnosis of disseminated coccidioidomycosis. BMJ Case Rep. 2022, 15, e248894. [Google Scholar] [CrossRef]
- Sharifi, S.; Sharma, R.; Heidari, A.; Johnson, R.H. Disseminated Coccidioidomycosis: Cutaneous, Soft Tissue, Osseous, and “Shotgun Intraparenchymal” Brain Disease. J. Investig. Med. High. Impact Case Rep. 2022, 10, 23247096221075906. [Google Scholar] [CrossRef]
- Kim, J.M.; Pervaiz, S.; Sivasubramanian, G. Extensive spinal disease from disseminated coccidioidomycosis. Am. J. Med. Sci. 2022, 363, e59. [Google Scholar] [CrossRef]
- Coba, A.J.; Sallee, P.K.; Dixon, D.O.; Alkhateb, R.; Anstead, G.M. Pandora’s Box: Disseminated Coccidioidomycosis Associated with Self-Medication with an Unregulated Potent Corticosteroid Acquired in Mexico. Trop. Med. Infect. Dis. 2021, 6, 207. [Google Scholar] [CrossRef]
- Ahmad, F.; Patel, K.; De Leon, J.C.; Buttacavoli, F.A. Disseminated Coccidioidomycosis of the Knee Joint Requiring Synovectomy and Arthrotomy. J. Orthop. Case Rep. 2021, 11, 76–80. [Google Scholar] [CrossRef]
- Nasrawi, F.; Heidari, A.; Aljashamy, T.; Mangat, N.; Bhaika, J.; Kaur, S.; Kuran, R.; Johnson, R. Disseminated Coccidioidomycosis Presenting as Polyarticular Septic Arthritis: A Case Report. J. Investig. Med. High. Impact Case Rep. 2020, 8, 2324709620974894. [Google Scholar] [CrossRef]
- Sherpa, N.; Shah, R.; Nordstrom, B.; Palmares, C.; Heidari, A.; Johnson, R. Locus Minoris Resistentiae in Coccidioidomycosis: A Case Series. J. Investig. Med. High. Impact Case Rep. 2019, 7, 2324709619858110. [Google Scholar] [CrossRef]
- Nakhla, S.G. Complications and Management of a Rare Case of Disseminated Coccidioidomycosis to the Vertebral Spine. Case Rep. Infect. Dis. 2018, 2018, 8954016. [Google Scholar] [CrossRef]
- Fox, T.; Solomon, R.; Kaka, A. Disseminated coccidioidomycosis. Postgrad. Med. J. 2018, 94, 722–723. [Google Scholar] [CrossRef]
- Carius, B.M.; Kambe, C.J. Why is this patient’s chronic knee pain worsening? JAAPA 2018, 31, 50–52. [Google Scholar] [CrossRef]
- Weisenberg, S.A. Coccidioides immitis septic knee arthritis. BMJ Case Rep. 2018, 2018, bcr2017222585. [Google Scholar] [CrossRef]
- Abdelmisseh, M.; Naeem, F.; Veesenmeyer, A.; Siongco, A.; Rongkavilit, C. A California Infant with Insidious Left Wrist Swelling. Pediatr. Infect. Dis. J. 2018, 37, 615. [Google Scholar] [CrossRef]
- Khalid, A.; Boken, D.J.; Nelson, C.A.; Totten, V.Y. A Case of Osteomyelitis of the toe caused by Coccidioidomycosis in a 17 year-old with Diabetes Insipidus. IDCases 2017, 9, 14–16. [Google Scholar] [CrossRef]
- McConnell, M.F.; Shi, A.; Lasco, T.M.; Yoon, L. Disseminated coccidioidomycosis with multifocal musculoskeletal disease involvement. Radiol. Case Rep. 2016, 12, 141–145. [Google Scholar] [CrossRef]
- Hammoudeh, Z.S.; Lettieri, S. Management of temporomandibular joint Coccidioidomycosis. Cranio 2016, 34, 402–405. [Google Scholar] [CrossRef]
- Arbeloa-Gutierrez, L.; Kuberski, T.; Johnson, S.M.; Sagastibelza, I.; Alaez, J.I.; Pappagianis, D. Reactivation of coccidioidomycosis: A prosthetic joint infection in Spain. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 183–186. [Google Scholar] [CrossRef]
- Berli, J.U.; Campbell, W.N.; Katz, R.D. Coccidioidomycosis causing osteomyelitis of the hand in an immunocompetent patient. Hand 2015, 10, 562–564. [Google Scholar] [CrossRef]
- Ellerbrook, L.; Laks, S. Coccidioidomycosis osteomyelitis of the knee in a 23-year-old diabetic patient. Radiol. Case Rep. 2015, 10, 1034. [Google Scholar] [CrossRef]
- Mirochnik, B.D.; Lev, S.; Weingarten, E.P. Case 209: Disseminated coccidioidal spondylodiskitis. Radiology 2014, 272, 914–918. [Google Scholar] [CrossRef]
- Li, Y.C.; Calvert, G.; Hanrahan, C.J.; Jones, K.B.; Randall, R.L. Coccidiomycosis infection of the patella mimicking a neoplasm—Two case reports. BMC Med. Imaging 2014, 14, 8. [Google Scholar] [CrossRef]
- Capoor, M.R.; Sen, B.; Varshney, P.; Verghese, M.; Shivaprakash, M.R.; Chakrabarti, A. Coccidioidomycosis masquerading as skeletal tuberculosis: An imported case and review of coccidioidomycosis in India. Trop. Dr. 2014, 44, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Zhu, E.S.; Thompson, G.R.; Kreulen, C.; Giza, E. Amphotericin B-impregnated bone cement to treat refractory coccidioidal osteomyelitis. Antimicrob. Agents Chemother. 2013, 57, 6341–6343. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.S.; Cardile, A.P. Diffuse skeletal coccidioidomycosis in an AIDS patient. Int. J. Infect. Dis. 2013, 17, e928–e929. [Google Scholar] [CrossRef]
- Austen, S.; van der Weegen, W.; Verduin, C.M.; van der Valk, M.; Hoekstra, H.J. Coccidioidomycosis infection of a total knee arthroplasty in a nonendemic region. J. Arthroplast. 2013, 28, e13–e15. [Google Scholar] [CrossRef] [PubMed]
- Ong, A.T.; Mahajan, H.; Chen, S.C.; Halliday, C.; Watts, M.R.; Brighton, R.; Ralph, A.P. Coccidioidal septic arthritis: Lessons learned from a clinical and laboratory perspective. Med. J. Aust. 2012, 196, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Arora, N.P.; Taneja, V.; ReyesSacin, C.; Bhanot, R.; Natesan, S.K. Coccidioidomycosis masquerading as malignancy. BMJ Case Rep. 2012, 2012, bcr1220115357. [Google Scholar] [CrossRef] [PubMed]
- Reach, P.; Paugam, A.; Kahan, A.; Allanore, Y.; Wipff, J. Coccidioidomycosis of the spine in an immunocompetent patient. Jt. Bone Spine 2010, 77, 611–613. [Google Scholar] [CrossRef]
- Waterman, B.R.; Waterman, S.M.; McCoy, A.C.; Cameron, C.D. Coccidioidal osteomyelitis of the patella. Orthopedics 2010, 33, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Homans, J.D.; Spencer, L. Itraconazole treatment of nonmeningeal coccidioidomycosis in children: Two case reports and review of the literature. Pediatr. Infect. Dis. J. 2010, 29, 65–67. [Google Scholar] [CrossRef]
- Sandoval, J.J.; Shank, J.R.; Morgan, S.J.; Agudelo, J.F.; Price, C.S. Midfoot coccidioidal osteomyelitis. A case report and review of the literature. J. Bone Jt. Surg. Am. 2006, 88, 861–865. [Google Scholar] [CrossRef]
- Taxy, J.B.; Kodros, S. Musculoskeletal coccidioidomycosis: Unusual sites of disease in a nonendemic area. Am. J. Clin. Pathol. 2005, 124, 693–696. [Google Scholar] [CrossRef] [PubMed]
- Blair, J.E. Coccidioidal pneumonia, arthritis, and soft-tissue infection after kidney transplantation. Transpl. Infect. Dis. 2004, 6, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, R.M.; Bonnell, M.; Currier, B.L.; Orenstein, R. Successful treatment of disseminated nonmeningeal coccidioidomycosis with voriconazole. Clin. Infect. Dis. 2004, 39, e74–e77. [Google Scholar] [CrossRef] [PubMed]
- Lewicky, Y.M.; Roberto, R.F.; Curtin, S.L. The unique complications of coccidioidomycosis of the spine: A detailed time line of disease progression and suppression. Spine 2004, 29, E435–E441. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.G.; Arnold, J.C.; Bloom, D.C.; Brewster, D.F.; Thiringer, J.K. Head and neck manifestations of disseminated coccidioidomycosis. Laryngoscope 2004, 114, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W.; Cobbs, C.S.; Pappas, P.G. Surgical treatment of multiple skull abscesses associated with coccidioidomycosis. Mycoses 2004, 47, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Caraway, N.P.; Fanning, C.V.; Stewart, J.M.; Tarrand, J.J.; Weber, K.L. Coccidioidomycosis osteomyelitis masquerading as a bone tumor. A report of 2 cases. Acta Cytol. 2003, 47, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Copeland, B.; White, D.; Buenting, J. Coccidioidomycosis of the head and neck. Ann. Otol. Rhinol. Laryngol. 2003, 112, 98–101. [Google Scholar] [CrossRef]
- Fishco, W.D.; Blocher, K.S. Disseminated coccidioidomycosis masquerading as tendinitis. J. Am. Podiatr. Med. Assoc. 2000, 90, 508–511. [Google Scholar] [CrossRef]
- Westphal, S.A. Disseminated coccidioidomycosis associated with hypercalcemia. Mayo Clin. Proc. 1998, 73, 893–894. [Google Scholar] [CrossRef]
- Campbell, M.; Kusne, S.; Renfree, K.J.; Vikram, H.R.; Smilack, J.D.; Seville, M.T.; Orenstein, R.; Blair, J.E. Coccidioidal Tenosynovitis of the Hand and Wrist: Report of 9 Cases and Review of the Literature. Clin. Infect. Dis. 2015, 61, 1514–1520. [Google Scholar] [CrossRef] [PubMed]
- Stockamp, N.W.; Thompson, G.R., 3rd. Coccidioidomycosis. Infect. Dis. Clin. N. Am. 2016, 30, 229–246. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, H.; Erives, V.H.; Martinez, L.R. Coccidioidomycosis: Epidemiology, Fungal Pathogenesis, and Therapeutic Development. Curr. Trop. Med. Rep. 2019, 6, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Garcia Garcia, S.C.; Salas Alanis, J.C.; Flores, M.G.; Gonzalez Gonzalez, S.E.; Vera Cabrera, L.; Ocampo Candiani, J. Coccidioidomycosis and the skin: A comprehensive review. Bras. Dermatol. 2015, 90, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Taljanovic, M.S.; Adam, R.D. Musculoskeletal coccidioidomycosis. Semin. Musculoskelet. Radiol. 2011, 15, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Whiston, E.; Zhang Wise, H.; Sharpton, T.J.; Jui, G.; Cole, G.T.; Taylor, J.W. Comparative transcriptomics of the saprobic and parasitic growth phases in Coccidioides spp. PLoS ONE 2012, 7, e41034. [Google Scholar] [CrossRef]
- Monheit, J.E.; Cowan, D.F.; Moore, D.G. Rapid detection of fungi in tissues using calcofluor white and fluorescence microscopy. Arch. Pathol. Lab. Med. 1984, 108, 616–618. [Google Scholar]
- Galgiani, J.N.; Ampel, N.M.; Blair, J.E.; Catanzaro, A.; Geertsma, F.; Hoover, S.E.; Johnson, R.H.; Kusne, S.; Lisse, J.; MacDonald, J.D.; et al. 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin. Infect. Dis. 2016, 63, e112–e146. [Google Scholar] [CrossRef]
- Hamill, R.J. Amphotericin B formulations: A comparative review of efficacy and toxicity. Drugs 2013, 73, 919–934. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Chamakioti, I.; Raptis, K.; Alpantaki, K.; Vrioni, G.; Samonis, G. Osseous Infections Caused by Aspergillus Species. Diagnostics 2022, 12, 201. [Google Scholar] [CrossRef] [PubMed]
- Koutserimpas, C.; Chamakioti, I.; Zervakis, S.; Raptis, K.; Alpantaki, K.; Kofteridis, D.P.; Vrioni, G.; Samonis, G. Non-Candida Fungal Prosthetic Joint Infections. Diagnostics 2021, 11, 1410. [Google Scholar] [CrossRef] [PubMed]
- Koutserimpas, C.; Chamakioti, I.; Naoum, S.; Raptis, K.; Alpantaki, K.; Kofteridis, D.P.; Samonis, G. Spondylodiscitis Caused by Aspergillus Species. Diagnostics 2021, 11, 1899. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Lewis, J.S., 2nd; Nix, D.E.; Patterson, T.F. Current Concepts and Future Directions in the Pharmacology and Treatment of Coccidioidomycosis. Med. Mycol. 2019, 57 (Suppl. S1), S76–S84. [Google Scholar] [CrossRef] [PubMed]
- Romanò, C.L.; Tsantes, A.G.; Papadopoulos, D.V.; Tsuchiya, H.; Benzakour, T.; Benevenia, J.; Del Sel, H.; Drago, L.; Mavrogenis, A.F. World Association against Infection in Orthopedics and Trauma (WAIOT) Study Group on Bone and Joint Infection Definitions. Infectious disease specialists and teamwork strategies worldwide: The World Association against Infection in Orthopedics and Trauma (WAIOT) and SICOT continue to cooperate in fighting musculoskeletal infections. SICOT J. 2022, 8, E1. [Google Scholar] [CrossRef]
- Tsantes, A.G.; Papadopoulos, D.V.; Markou, E.; Zarokostas, K.; Sokou, R.; Trikoupis, I.; Mavrogenis, A.F.; Houhoula, D.; Piovani, D.; Bonovas, S.; et al. Aspergillus spp. osteoarticular infections: An updated systematic review on the diagnosis, treatment and outcomes of 186 confirmed cases. Med. Mycol. 2022, 60, myac052. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Patients (n = 163) |
|---|---|
| Age (years) | 37.7 ± 18.0, 36 (26–46.5) |
| Gender (male) | 125 (76.6) |
| Comorbidities/Underlying condition | |
| Previous fungal infection | 14 (8.5) |
| Hematologic neoplasia | 8 (4.9) |
| Immunodeficiency/immunosuppression therapy | 12 (7.3) |
| Diabetes | 24 (14.7) |
| Tuberculosis | 4 (2.4) |
| Sarcoidosis | 8 (4.8) |
| None | 14 (8.5) |
| Not mentioned | 79 (48.4) |
| Corticosteroids | 37 (22.6) |
| Genus | Pathogen | Patients (n = 163) |
|---|---|---|
| Coccidioides spp. | C. immitis | 103 (75.7) |
| C. posadasii | 2 (1.2) | |
| Not specified | 58 (35.5) | |
| Co-cultured bacterial pathogens | Staphylococcus spp. | 6 (3.6) |
| Enterobacterales spp. | 3 (1.8) | |
| Pseudomonas aeruginosa | 1 (0.6) |
| Location | Infected Foci (n = 165) |
|---|---|
| Spine | 32 (19.3) |
| Ribs and sternum | 6 (3.6) |
| Lower extremities | |
| Knee | 29 (17.5) |
| Foot | 15 (9.0) |
| Ankle | 4 (2.4) |
| Other areas | 13 (7.8) |
| Cranial bones | 10 (6.0) |
| Upper extremity | |
| Wrist | 9 (5.4) |
| Hand | 25 (15.1) |
| Elbow | 6 (3.6) |
| Shoulder | 2 (1.2) |
| Pelvis (iliac, sacral) | 14 (8.4) |
| Patients (n = 163) | |
|---|---|
| Direct culture | 68 (41.7) |
| Histology and direct culture | 49 (30.0) |
| Histology | 37 (22.6) |
| Direct cultures and serology | 3 (1.8) |
| Histology and serology | 3 (1.8) |
| Direct cultures, histology and PCR | 3 (1.8) |
| WBC count (×103/mL) | 11.0 ± 6.1, 10.1 (6.9–13.5) |
| Abnormal WBC count (>12 × 103/mL) | 54 (33.1) |
| ESR (mm/h) | 65.4 ± 42.3, 61.0 (27.0–102.0) |
| Abnormal ESR (>20 mm/h) | 137 (73.6) |
| CRP (mg/L) | 46.1 ± 56.0, 19.0 (4.0–94.0) |
| Abnormal CRP (>10 mg/L) | 91 (55.8) |
| Patients (n = 163) | Duration (Months) | Complete Resolution | |
|---|---|---|---|
| Total | 163 (100.0) | 8.8 ± 4.3, 8 (6–13) | 121 (74.2) |
| Amphotericin B monotherapy | 51 (31.2) | 8.7 ± 4.7, 8 (6–13) | 40 (78.4) |
| Fluconazole monotherapy | 28 (17.1) | 19.2 ± 5.1, 18 (11–29) | 20 (71.4) |
| Itraconazole monotherapy | 30 (18.4) | 9.7 ± 16.7, 6 (6–9) | 22 (73.3) |
| Ketoconazole monotherapy | 4 (2.4) | - | 3 (75.0) |
| Voriconazole monotherapy | 5 (3.0) | - | 4 (80.0) |
| Amphotericin B + itraconazole | 15 (9.2) | - | 10 (66.6) |
| Amphotericin B + ketoconazole | 13 (7.8) | - | 9 (69.2) |
| Amphotericin B + fluconazole | 4 (2.4) | - | 3 (75.0) |
| Amphotericin B + voriconazole | 5 (3.0) | - | 4 (80.0) |
| Other | 8 (4.9) | - | 6 (75.0) |
| Surgical debridement | 132 (80.9) | - | 105 (79.5) |
| Antifungal monotherapy | 118 (72.3) | 8.8 ± 4.3, 8 (6–13) | 89 (75.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsantes, A.G.; Koutserimpas, C.; Naoum, S.; Drosopoulou, L.-P.; Papadogeorgou, E.; Petrakis, V.; Alpantaki, K.; Samonis, G.; Veizi, E.; Papadopoulos, D.V. Diagnosis, Treatment, and Outcome of Coccidioidal Osseous Infections: A Systematic Review. J. Fungi 2024, 10, 270. https://doi.org/10.3390/jof10040270
Tsantes AG, Koutserimpas C, Naoum S, Drosopoulou L-P, Papadogeorgou E, Petrakis V, Alpantaki K, Samonis G, Veizi E, Papadopoulos DV. Diagnosis, Treatment, and Outcome of Coccidioidal Osseous Infections: A Systematic Review. Journal of Fungi. 2024; 10(4):270. https://doi.org/10.3390/jof10040270
Chicago/Turabian StyleTsantes, Andreas G., Christos Koutserimpas, Symeon Naoum, Lida-Paraskevi Drosopoulou, Ellada Papadogeorgou, Vasileios Petrakis, Kalliopi Alpantaki, George Samonis, Enejd Veizi, and Dimitrios V. Papadopoulos. 2024. "Diagnosis, Treatment, and Outcome of Coccidioidal Osseous Infections: A Systematic Review" Journal of Fungi 10, no. 4: 270. https://doi.org/10.3390/jof10040270