
Sporothrix brasiliensis Causing Atypical Sporotrichosis in Brazil: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
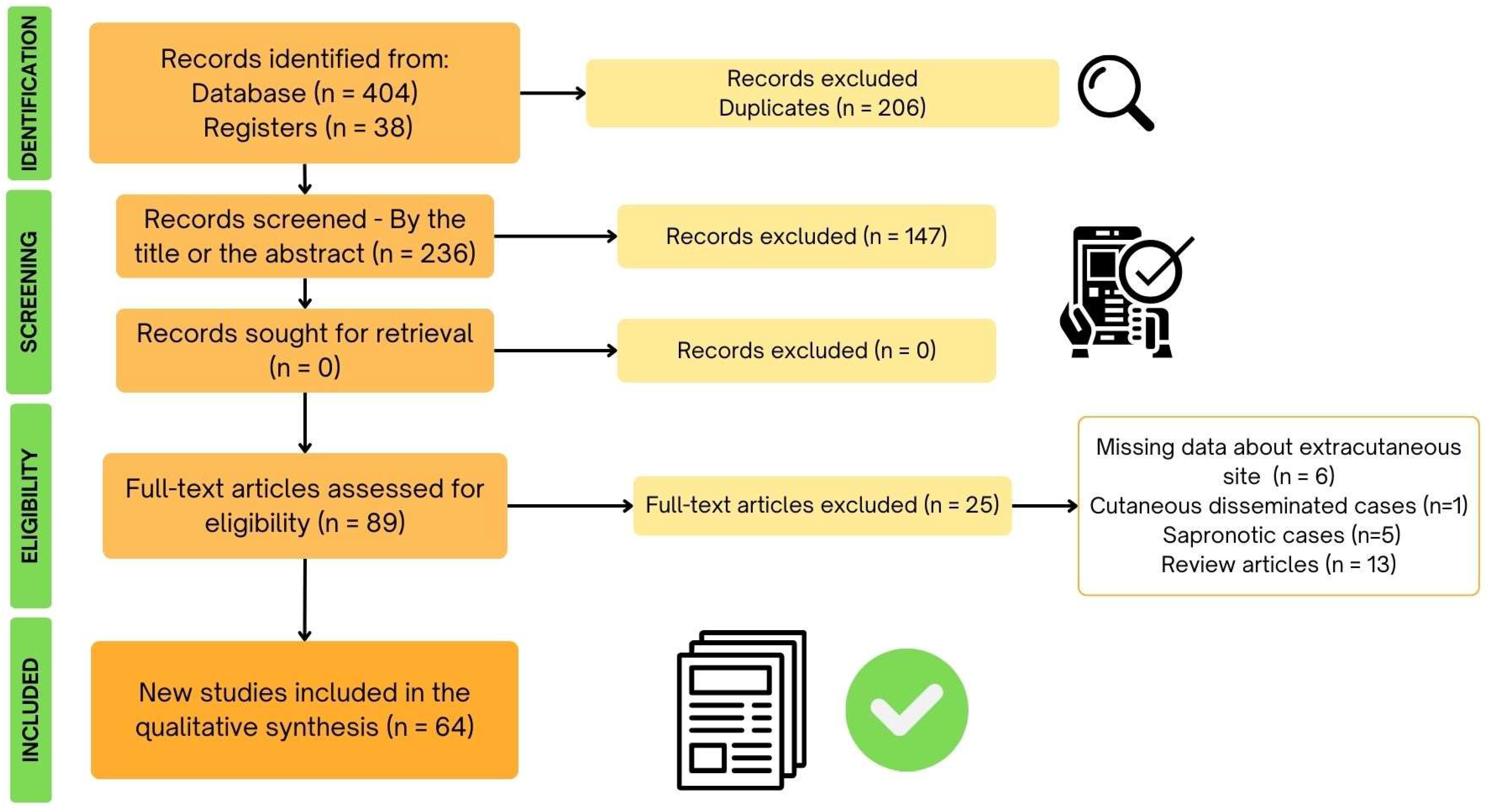
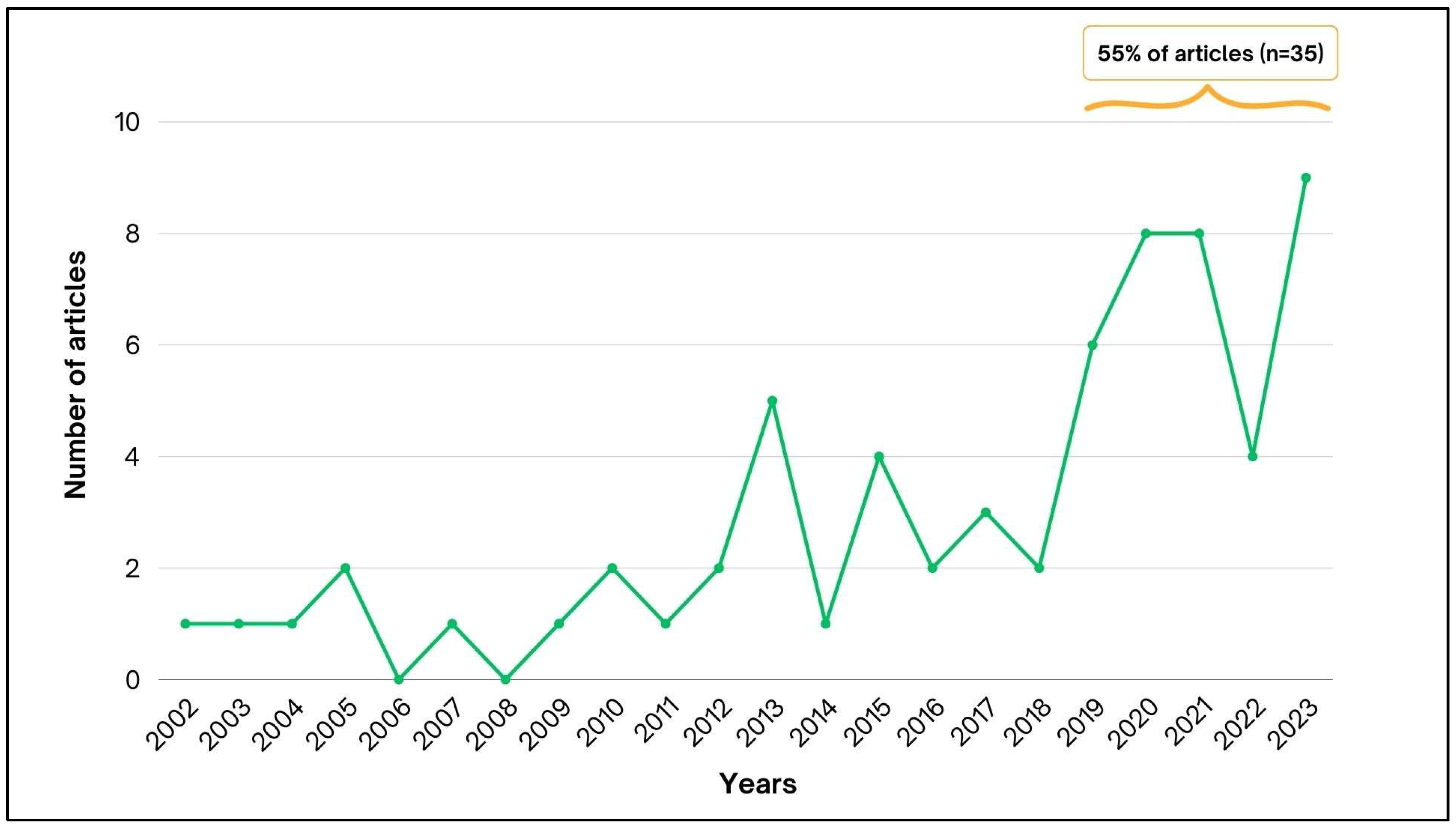
3.1. Article Searching
3.2. Extracutaneous and HR Cases
3.2.1. HR Cases
3.2.2. Mucosal Cases
3.2.3. Osteoarthritis Cases
3.2.4. Pulmonary Cases
3.2.5. Meningeal Cases
3.2.6. Multifocal Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poester, V.R.; Mattei, A.S.; Madrid, I.M.; Pereira, J.T.B.; Klafke, G.B.; Sanchotene, K.O.; Brandolt, T.M.; Xavier, M.O. Sporotrichosis in Southern Brazil, towards an Epidemic? Zoonoses Public Health 2018, 65, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Falcão, E.M.M.; Romão, A.R.; Magalhães, M.d.A.F.M.; Filho, J.B.d.L.; Valle, A.C.F.d.; Bastos, F.I.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. A Spatial Analysis of the Spread of Hyperendemic Sporotrichosis in the State of Rio de Janeiro, Brazil. J. Fungi 2022, 8, 434. [Google Scholar] [CrossRef]
- Rabello, V.B.S.; Almeida, M.A.; Bernardes-Engemann, A.R.; Almeida-Paes, R.; de Macedo, P.M.; Zancopé-Oliveira, R.M. The Historical Burden of Sporotrichosis in Brazil: A Systematic Review of Cases Reported from 1907 to 2020. Braz. J. Microbiol. 2022, 53, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Kaadan, M.I.; Dennis, M.; Desai, N.; Yadavalli, G.; Lederer, P. One Health Education for Future Physicians: A Case Report of Cat-Transmitted Sporotrichosis. Open Forum Infect. Dis. 2020, 7, ofaa049. [Google Scholar] [CrossRef] [PubMed]
- Etchecopaz, A.; Toscanini, M.A.; Gisbert, A.; Mas, J.; Scarpa, M.; Iovannitti, C.A.; Bendezú, K.; Nusblat, A.D.; Iachini, R.; Cuestas, M.L. Sporothrix brasiliensis: A Review of an Emerging South American Fungal Pathogen, Its Related Disease, Presentation and Spread in Argentina. J. Fungi 2021, 7, 170. [Google Scholar] [CrossRef] [PubMed]
- Rachman, R.; Ligaj, M.; Chinthapalli, S.; Wani, R.S. Zoonotic Acquisition of Cutaneous Sporothrix Braziliensis Infection in the UK. BMJ Case Rep. 2022, 15, e248418. [Google Scholar] [CrossRef]
- do Prado, C.M.; Razzolini, E.; Santacruz, G.; Ojeda, L.; Geraldo, M.R.; Segovia, N.; Brunelli, J.P.; Vicente, V.A.; Svoboda, W.K.; Queiroz-Telles, F. First Cases of Feline Sporotrichosis Caused by Sporothrix brasiliensis in Paraguay. J. Fungi 2023, 9, 972. [Google Scholar] [CrossRef]
- Thomson, P.; González, C.; Blank, O.; Ramírez, V.; del Río, C.; Santibáñez, S.; Pena, P. Sporotrichosis Outbreak Due to Sporothrix brasiliensis in Domestic Cats in Magallanes, Chile: A One-Health-Approach Study. J. Fungi 2023, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Xavier, M.O.; Poester, V.R.; Trápaga, M.R.; Stevens, D.A. Sporothrix brasiliensis: Epidemiology, Therapy, and Recent Developments. J. Fungi 2023, 9, 921. [Google Scholar] [CrossRef]
- Schubach, T.M.; Schubach, A.; Okamoto, T.; Barros, M.B.; Figueiredo, F.B.; Cuzzi, T.; Fialho-Monteiro, P.C.; Reis, R.S.; Perez, M.A.; Wanke, B. Evaluation of an Epidemic of Sporothricosis in Cats: 347 Cases (1998–2001). J. Am. Vet. Med. Assoc. 2004, 224, 1623–1629. [Google Scholar] [CrossRef]
- Sanchotene, K.O.; Madrid, I.M.; Klafke, G.B.; Bergamashi, M.; Terra, P.P.D.; Rodrigues, A.M.; de Camargo, Z.P.; Xavier, M.O. Sporothrix brasiliensis Outbreaks and the Rapid Emergence of Feline Sporotrichosis. Mycoses 2015, 58, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Gremião, I.D.F.; Martins da Silva da Rocha, E.; Montenegro, H.; Carneiro, A.J.B.; Xavier, M.O.; de Farias, M.R.; Monti, F.; Mansho, W.; de Macedo Assunção Pereira, R.H.; Pereira, S.A.; et al. Guideline for the Management of Feline Sporotrichosis Caused by Sporothrix brasiliensis and Literature Revision. Braz. J. Microbiol. 2021, 52, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Xavier, M.O.; Bittencourt, L.R.; Silva, C.M.; Vieira, R.S.; Pereira, H.C. Atypical Presentation of Sporotrichosis: Report of Three Cases. Rev. Soc. Bras. Med. Trop. 2013, 46, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Paes, R.; de Oliveira, M.M.E.; Freitas, D.F.S.; do Valle, A.C.F.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in Rio de Janeiro, Brazil: Sporothrix brasiliensis Is Associated with Atypical Clinical Presentations. PLoS Neglected Trop. Dis. 2014, 8, e3094. [Google Scholar] [CrossRef] [PubMed]
- Brandolt, T.M.; Madrid, I.M.; Poester, V.R.; Sanchotene, K.O.; Basso, R.P.; Klafke, G.B.; de Lima Rodrigues, M.; Xavier, M.O. Human Sporotrichosis: A Zoonotic Outbreak in Southern Brazil, 2012–2017. Med. Mycol. 2018, 57, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Poester, V.R.; Munhoz, L.S.; Basso, R.P.; Roca, B.M.; Vieira, M.U.; Melo, A.M.; Klafke, G.B.; Sanchotene, K.O.; Silveira, J.M.; Stevens, D.; et al. Disseminated Sporotrichosis with Immune Reconstitution Inflammatory Syndrome in an HIV Patient: Case Report and Review of the Literature. Rev. Iberoam. Micol. 2020, 37, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Procópio-Azevedo, A.C.; Rabello, V.B.S.; Muniz, M.M.; Figueiredo-Carvalho, M.H.G.; Almeida-Paes, R.; Zancopé-Oliveira, R.M.; Silva, J.C.A.L.; Macedo, P.M.; Valle, A.C.F.; Gutierrez-Galhardo, M.C.; et al. Hypersensitivity Reactions in Sporotrichosis: A Retrospective Cohort of 325 Patients from a Reference Hospital in Rio de Janeiro, Brazil (2005–2018). Br. J. Dermatol. 2021, 185, 1272–1274. [Google Scholar] [CrossRef]
- Fichman, V.; Mota-Damasceno, C.G.; Procópio-Azevedo, A.C.; Almeida-Silva, F.; de Macedo, P.M.; Medeiros, D.M.; Astacio, G.S.-M.; Zancopé-Oliveira, R.M.; Almeida-Paes, R.; Freitas, D.F.S.; et al. Pulmonary Sporotrichosis Caused by Sporothrix brasiliensis: A 22-Year, Single-Center, Retrospective Cohort Study. J. Fungi 2022, 8, 536. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.A.; Freitas, D.F.S.; Oliveira, R.V.C.; Fichman, V.; Varon, A.G.; Freitas, A.D.; Lamas, C.C.; Andrade, H.B.; Veloso, V.G.; Almeida-Paes, R.; et al. Meningeal Sporotrichosis Due to Sporothrix brasiliensis: A 21-Year Cohort Study from a Brazilian Reference Center. J. Fungi 2023, 9, 17. [Google Scholar] [CrossRef]
- Arinelli, A.; Aleixo, A.L.Q.C.; Freitas, D.F.S.; do Valle, A.C.F.; Almeida-Paes, R.; Guimarães, A.L.N.; Oliveira, R.V.C.; Gutierrez-Galhardo, M.C.; Curi, A.L.L. Ocular Manifestations of Sporotrichosis in a Hyperendemic Region in Brazil: Description of a Series of 120 Cases. Ocul. Immunol. Inflamm. 2023, 31, 329–337. [Google Scholar] [CrossRef]
- Izoton, C.F.G.; de Brito Sousa, A.X.; Valete, C.M.; de Oliveira Schubach, A.; Procópio-Azevedo, A.C.; Zancopé-Oliveira, R.M.; de Macedo, P.M.; Gutierrez-Galhardo, M.C.; Castro-Alves, J.; Almeida-Paes, R.; et al. Sporotrichosis in the Nasal Mucosa: A Single-Center Retrospective Study of 37 Cases from 1998 to 2020. PLOS Neglected Trop. Dis. 2023, 17, e0011212. [Google Scholar] [CrossRef] [PubMed]
- Ramos, V.; Astacio, G.S.-M.; do Valle, A.C.F.; de Macedo, P.M.; Lyra, M.R.; Almeida-Paes, R.; Oliveira, M.M.E.; Zancopé-Oliveira, R.M.; Brandão, L.G.P.; Quintana, M.S.B.; et al. Bone Sporotrichosis: 41 Cases from a Reference Hospital in Rio de Janeiro, Brazil. PLOS Neglected Trop. Dis. 2021, 15, e0009250. [Google Scholar] [CrossRef] [PubMed]
- Schechtman, R.C.; Falcão, E.M.M.; Carard, M.; García, M.S.C.; Mercado, D.S.; Hay, R.J. Sporotrichosis: Hyperendemic by Zoonotic Transmission, with Atypical Presentations, Hypersensitivity Reactions and Greater Severity. An. Bras. Dermatol. 2022, 97, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Galhardo, M.C.; Barros, M.B.L.; Schubach, A.O.; Cuzzi, T.; Schubach, T.M.P.; Lazéra, M.S.; Valle, A.C.F. Erythema Multiforme Associated with Sporotrichosis. J. Eur. Acad. Dermatol. Venereol. 2005, 19, 507–509. [Google Scholar] [CrossRef]
- Gutierrez Galhardo, M.C.; de Oliveira Schubach, A.; de Lima Barros, M.B.; Blanco, T.C.M.; Cuzzi-Maya, T.; Schubach, T.M.P.; dos Santos Lazéra, M.; Francesconi do Valle, A.C. Erythema nodosum associated with sporotrichosis. Int. J. Dermatol. 2002, 41, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Orofino-Costa, R.; Bóia, M.N.; Magalhães, G.A.P.; Damasco, P.S.; Bernardes-Engemann, A.R.; Benvenuto, F.; Silva, I.C.; Lopes-Bezerra, L.M. Arthritis as a Hypersensitivity Reaction in a Case of Sporotrichosis Transmitted by a Sick Cat: Clinical and Serological Follow up of 131 Months. Mycoses 2010, 53, 81–83. [Google Scholar] [CrossRef] [PubMed]
- de Lima, Í.M.F.; Ferraz, C.E.; de Lima-Neto, R.G.; Takano, D.M. Case Report: Sweet Syndrome in Patients with Sporotrichosis: A 10-Case Series. Am. J. Trop. Med. Hyg. 2020, 103, 2533–2538. [Google Scholar] [CrossRef] [PubMed]
- Freitas, D.F.S.; Valle, A.C.F.; Cuzzi, T.; Brandão, L.G.P.; Zancope-Oliveira, R.M.; Galhardo, M.C.G. Sweet Syndrome Associated with Sporotrichosis. Br. J. Dermatol. 2012, 166, 212–213. [Google Scholar] [CrossRef]
- de Macedo, P.M.; Sztajnbok, D.C.N.; Camargo, Z.P.; Rodrigues, A.M.; Lopes-Bezerra, L.M.; Bernardes-Engemann, A.R.; Orofino-Costa, R. Dacryocystitis Due to Sporothrix brasiliensis: A Case Report of a Successful Clinical and Serological Outcome with Low-Dose Potassium Iodide Treatment and Oculoplastic Surgery. Br. J. Dermatol. 2015, 172, 1116–1119. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Y.; Cong, L.; Yang, H.; Cong, X. Eyelid Sporotrichosis: Unique Clinical Findings in 72 Patients. Australas. J. Dermatol. 2016, 57, 44–47. [Google Scholar] [CrossRef]
- Paiva, A.d.C.M.; Biancardi, A.L.; Curi, A.L.L. Different Clinical Manifestations of Ocular Sporotrichosis in the Same Patient: An Alert to Ophthalmologists in Nonendemic Areas. Arq. Bras. Oftalmol. 2020, 83, 457–458. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Oliveros, J.F.; Schechtman, R.C.; de Vries, H.J.; Lora, L.; Arinelli, A.C.; da Costa Nery, J.A.; Freitas, D.F.S. Ocular Adnexal Sporotrichosis: A Case Series. JAAD Case Rep. 2021, 13, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Lederer, H.T.; Sullivan, E.; Crum-Cianflone, N.F. Sporotrichosis as an Unusual Case of Osteomyelitis: A Case Report and Review of the Literature. Med. Mycol. Case Rep. 2016, 11, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Mialski, R.; de Oliveira, J.N.; da Silva, L.H.; Kono, A.; Pinheiro, R.L.; Teixeira, M.J.; Gomes, R.R.; de Queiroz-Telles, F.; Pinto, F.G.; Benard, G. Chronic Meningitis and Hydrocephalus Due to Sporothrix brasiliensis in Immunocompetent Adults: A Challenging Entity. Open Forum Infect. Dis. 2018, 5, ofy081. [Google Scholar] [CrossRef] [PubMed]
- Duani, H.; Palmerston, M.F.; Júnior, J.F.R.; Ribeiro, V.T.; Neves, P.L.A. Meningeal and Multiorgan Disseminated Sporotrichosis: A Case Report and Autopsy Study. Med. Mycol. Case Rep. 2019, 26, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.A.; Vallier, R.; Silva, M.M. Sporothrix brasiliensis Meningitis in an Immunocompetent Patient. Pract. Neurol. 2021, 21, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, V.C.R.; Colombo, S.A.; Peres, N.T.A.; Moura, A.S.; Lyon, A.C.; Lyon, S.; Dutra, M.R.T.; Fereguetti, T.O.; Andrade, V.A.; Azevedo, M.I.; et al. Clinical Factors Associated with Systemic Sporotrichosis in Brazil. Mycoses 2023, 67, e13656. [Google Scholar] [CrossRef]
- Falcão, E.M.M.; de Lima Filho, J.B.; Campos, D.P.; do Valle, A.C.F.; Bastos, F.I.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. Hospitalizações e Óbitos Relacionados à Esporotricose No Brasil (1992–2015). Cad. Saúde Pública 2019, 35, e00109218. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 29, 372. [Google Scholar] [CrossRef]
- Queiroz-Telles, F.; Bonifaz, A.; Cognialli, R.; Lustosa, B.P.R.; Vicente, V.A.; Ramírez-Marín, H.A. Sporotrichosis in Children: Case series and Narrative Review. Curr. Fungal Infect. Rep. 2022, 16, 33–46. [Google Scholar] [CrossRef]
- Curi, A.L.L.; Félix, S.; Azevedo, K.M.L.; Estrela, R.; Villar, E.G.; Saraça, G. Retinal Granuloma Caused by Sporothrix schenckii. Am. J. Ophthalmol. 2003, 136, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Barros, M.B.; de Oliveira Schubach, A.; do Valle, A.C.; Galhardo, M.C.G.; Conceição-Silva, F.; Schubach, T.M.; Reis, R.S.; Wanke, B.; Marzochi, K.B.; Conceição, M.J. Cat-Transmitted Sporotrichosis Epidemic in Rio de Janeiro, Brazil: Description of a Series of Cases. Clin. Infect. Dis. 2004, 38, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Silva-Vergara, M.L.; Maneira, F.R.Z.; Oliveira, R.M.D.; Santos, C.T.B.; Etchebehere, R.M.; Adad, S.J. Multifocal Sporotrichosis with Meningeal Involvement in a Patient with AIDS. Med. Mycol. 2005, 43, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Vilela, R.; Souza, G.F.; Cota, G.F.; Mendoza, L. Esporotricosis Cutánea y Meningea En Un Paciente Con VIH. Rev. Iberoam. Micol. 2007, 24, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Galhardo, M.C.G.; Silva, M.T.T.; Lima, M.A.; Nunes, E.P.; Schettini, L.E.C.; de Freitas, R.F.; de Almeida Paes, R.; Neves, E.d.S.; do Valle, A.C.F. Sporothrix schenckii Meningitis in AIDS during Immune Reconstitution Syndrome. J. Neurol. Neurosurg. Psychiatry 2010, 81, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Galhardo, M.C.; Valle, A.C.F.D.; Fraga, B.L.B.; Schubach, A.O.; Hoagland, B.R.D.S.; Monteiro, P.C.F.; Barros, M.B.D.L. Disseminated Sporotrichosis as a Manifestation of Immune Reconstitution Inflammatory Syndrome. Mycoses 2010, 53, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Freitas, D.F.S.; de Siqueira Hoagland, B.; do Valle, A.C.F.; Fraga, B.B.; de Barros, M.B.; de Oliveira Schubach, A.; de Almeida-Paes, R.; Cuzzi, T.; Rosalino, C.M.V.; Zancopé-Oliveira, R.M.; et al. Sporotrichosis in HIV-Infected Patients: Report of 21 Cases of Endemic Sporotrichosis in Rio de Janeiro, Brazil. Med. Mycol. 2012, 50, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Silva-Vergara, M.L.; de Camargo, Z.P.; Silva, P.F.; Ferreira-Paim, K.; Abdalla, M.R.; Sgarbieri, R.N.; Rodrigues, A.M.; dos Santos, K.C.; Barata, C.H.; Ferreira-Paim, K. Disseminated Sporothrix brasiliensis Infection with Endocardial and Ocular Involvement in an HIV-Infected Patient. Am. J. Trop. Med. Hyg. 2012, 86, 477–480. [Google Scholar] [CrossRef] [PubMed]
- da Silva, L.M.C.; Oliveira, F.D.M.; Hochhegger, B.; Severo, L.C. Pulmonary sporotrichosis in Brazil: A case report and review. Rev. Patol. Trop. 2013, 42, 121–125. [Google Scholar] [CrossRef]
- Eustace, K.; Sampaio, F.; Lyra, M.; Quintella, L.; Valle, A. Cutaneous Disseminated Sporotrichosis Complicated by Osteomyelitis. Acta Derm. Venereol. 2013, 93, 192–193. [Google Scholar] [CrossRef]
- Orofino-Costa, R.; Unterstell, N.; Gripp, A.C.; de Macedo, P.M.; Brota, A.; Dias, E.; de Melo Teixeira, M.; Felipe, M.S.; Bernardes-Engemann, A.R.; Lopes-Bezerra, L.M. Pulmonary Cavitation and Skin Lesions Mimicking Tuberculosis in a HIV Negative Patient Caused by Sporothrix brasiliensis. Med. Mycol. Case Rep. 2013, 2, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Freitas, D.F.S.; Lima, I.A.R.; Curi, C.L.; Jordão, L.; Zancopé-Oliveira, R.M.; do Valle, A.C.F.; Galhardo, M.C.G.; Curi, A.L.L. Acute Dacryocystitis: Another Clinical Manifestation of Sporotrichosis. Memórias Inst. Oswaldo Cruz 2014, 109, 262–264. [Google Scholar] [CrossRef] [PubMed]
- de Araujo, M.L.; Rodrigues, A.M.; Fernandes, G.F.; de Camargo, Z.P.; Hoog, G.S.D. Human Sporotrichosis beyond the Epidemic Front Reveals Classical Transmission Types in Espírito Santo, Brazil. Mycoses 2015, 58, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Papaiordanou, F.; da Silveira, B.R.L.; Abulafia, L.A. Hypersensitivity Reaction to Sporothrix schenckii: Erythema Nodosum Associated with Sporotrichosis. Rev. Soc. Bras. Med. Trop. 2015, 48, 504. [Google Scholar] [CrossRef]
- Freitas, D.F.S.; Lima, M.A.; de Almeida-Paes, R.; Lamas, C.C.; do Valle, A.C.F.; Oliveira, M.M.E.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in the Central Nervous System Caused by Sporothrix brasiliensis. Clin. Infect. Dis. 2015, 61, 663–664. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.C.; Barroso, P.F.; Tonomura, E.; Akiti, T.; de Pinho Rodrigues, K.M. Osteomyelitis Caused by Sporothrix schenckii in an Immunocompetent Patient. Rev. Soc. Bras. Med. Trop. 2016, 49, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, K.B.; Landeiro, L.G.; Diniz, L.M.; Falqueto, A. Disseminated Cutaneous Sporotrichosis Associated with Ocular Lesion in an Immunocompetent Patient. An. Bras. Dermatol. 2016, 91, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Biancardi, A.L.; Freitas, D.F.S.; Valviesse, V.R.G.d.A.; Andrade, H.B.; de Oliveira, M.M.E.; do Valle, A.C.F.; Zancope-Oliveira, R.M.; Galhardo, M.C.G.; Curi, A.L.L. Multifocal choroiditis in disseminated sporotrichosis in patients with hiv/aids. Retin. Cases Brief Rep. 2017, 11, 67–70. [Google Scholar] [CrossRef] [PubMed]
- da Silva, R.F.; Bonfitto, M.; da Silva Junior, F.I.M.; de Ameida, M.T.G.; de CMA da Silva, R. Sporotrichosis in a Liver Transplant Patient: A Case Report and Literature Review. Med. Mycol. Case Rep. 2017, 17, 25–27. [Google Scholar] [CrossRef]
- Yamagata, J.P.M.; Rudolph, F.B.; Nobre, M.C.L.; Nascimento, L.V.; Sampaio, F.M.S.; Arinelli, A.; Freitas, D.F. Ocular Sporotrichosis: A Frequently Misdiagnosed Cause of Granulomatous Conjunctivitis in Epidemic Areas. Am. J. Ophthalmol. Case Rep. 2017, 8, 35–38. [Google Scholar] [CrossRef]
- Eyer-Silva, W.A.; de Azevedo, M.C.V.M.; da Silva, G.A.R.; Basílio-de-Oliveira, R.P.; de Araujo, L.F.; Lago, I.V.d.; Pereira, F.C.F.; Fernandes, M.B.T.; Figueiredo-Carvalho, M.H.G.; de Souza Rabello, V.B.; et al. Palate Ulcer, Uvular Destruction and Nasal Septal Perforation Caused by Sporothrix brasiliensis in an HIV-Infected Patient. Med. Mycol. Case Rep. 2019, 23, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, G.S.A.; Watanabe, A.L.C.; Trevizoli, N.C.; Jorge, F.M.F.; Cajá, G.O.N.; Diaz, L.G.G.; Meireles, L.P.; Araújo, M.C.C.L. Disseminated Sporotrichosis in a Liver Transplant Patient: A Case Report. Transplant. Proc. 2019, 51, 1621–1624. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Furtado, L.; Biancardi, A.L.; de Souza Cravo, L.M.; Anjo, R.P.P.; Junior, H.V.d.M. Ocular Sporotrichosis: Atypical Manifestations. Rev. Bras. Oftalmol. 2019, 78, 59–61. [Google Scholar] [CrossRef]
- Lacerda Filho, A.M.; Cavalcante, C.M.; Silva, A.B.D.; Inácio, C.P.; de Lima-Neto, R.G.; de Andrade, M.C.L.; Magalhães, O.M.C.; Santos, F.d.A.G.d.; Neves, R.P. High-Virulence Cat-Transmitted Ocular Sporotrichosis. Mycopathologia 2019, 184, 547–549. [Google Scholar] [CrossRef] [PubMed]
- Matos, A.; Moreira, L.; Barczewski, B.; de Matos, L.; de Oliveira, J.; Pimentel, M.I.; Almeida-Paes, R.; Oliveira, M.; Pinto, T.; Lima, N.; et al. Identification by MALDI-TOF MS of Sporothrix brasiliensis Isolated from a Subconjunctival Infiltrative Lesion in an Immunocompetent Patient. Microorganisms 2019, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- do Monte Alves, M.; Milan, E.P.; da Silva-Rocha, W.P.; de Sena da Costa, A.S.; Maciel, B.A.; Vale, P.H.C.; de Albuquerque, P.R.; Lima, S.L.; de Azevedo Melo, A.S.; Rodrigues, A.M.; et al. Fatal Pulmonary Sporotrichosis Caused by Sporothrix brasiliensis in Northeast Brazil. PLOS Neglected Trop. Dis. 2020, 14, e0008141. [Google Scholar] [CrossRef] [PubMed]
- Arinelli, A.; do Couto Aleixo, A.L.Q.; Freitas, D.F.S.; do Valle, A.C.F.; Almeida-Paes, R.; Gutierrez-Galhardo, M.C.; Curi, A.L.L. Ocular Sporotrichosis: 26 Cases with Bulbar Involvement in a Hyperendemic Area of Zoonotic Transmission. Ocul. Immunol. Inflamm. 2020, 28, 764–771. [Google Scholar] [CrossRef] [PubMed]
- de Moura Barros, N.; de Souza Pessoa, A.; Brotas, A.M. Systemic Sporotrichosis in an Alcoholic Patient. An. Bras. Dermatol. 2020, 95, 376–378. [Google Scholar] [CrossRef]
- de Sá Menezes Carvalho, G.; Veasey, J.V. Immunoreactive Cutaneous Sporotrichosis. An. Bras. Dermatol. 2020, 95, 737–739. [Google Scholar] [CrossRef]
- Ribeiro, C.R.; Silva, B.P.; de Alcantara Almeida Costa, A.; Neto, A.B.; Vieira, L.A.; de Lima, M.A.; de Lima, M.H.C. Ocular Sporotrichosis. Am. J. Ophthalmol. Case Rep. 2020, 19, 100865. [Google Scholar] [CrossRef]
- Fichman, V.; de Macedo, P.M.; Freitas, D.F.S.; do Valle, A.C.F.; Almeida-Silva, F.; Bernardes-Engemann, A.R.; Zancopé-Oliveira, R.M.; Almeida-Paes, R.; Gutierrez-Galhardo, M.C. Zoonotic Sporotrichosis in Renal Transplant Recipients from Rio de Janeiro, Brazil. Transpl. Infect. Dis. 2021, 23, e13485. [Google Scholar] [CrossRef] [PubMed]
- Lauar, I.D.; Nascimento, V.A.M.; Soares, J.E.P.; de Matos, M.A.; Faria, K.E.P.; Nogueira, L.P.A.; Parreiras, G.C. Esporotricose Pulmonar Em Paciente Imunocompetente: Relato de Caso. Rev. Médica Minas Gerais 2021, 31, e31415. [Google Scholar] [CrossRef]
- Lemes, L.R.; Veasey, J.V.; Mayor, S.S.; Proença, C.C. Ocular Involvement in Sporotrichosis: Report of Two Cases in Children. An. Bras. Dermatol. 2021, 96, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Liborio Neto, A.O.; Caetano, T.R.; Gervasio, N.H.P.; Carneiro, R.C. Conjunctival and Bulbar Sporotrichosis as Parinaud’s Oculoglandular Syndrome Acquired by Blood Inoculation. GMS Ophthalmol. Cases 2021, 11, Doc02. [Google Scholar] [CrossRef] [PubMed]
- Xavier, J.R.B.; Waller, S.B.; da Gama Osório, L.; Vives, P.S.; Albano, A.P.N.; de Aguiar, E.S.V.; Ferreira, M.R.A.; da Conceição, F.R.; de Faria, R.O.; Meireles, M.C.A.; et al. Human Sporotrichosis Outbreak Caused by Sporothrix brasiliensis in a Veterinary Hospital in Southern Brazil. J. Med. Mycol. 2021, 31, 101163. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, A.A.; Oyafuso, L.K.M.; Cavalin, R.F.; Palhares, R.B.; Benard, G.; Gimenes, V.M.F.; Negro, G.M.B.D.; Siqueira, L.P.M.; de Freitas Xavier, R.S.; Lopes-Bezerra, L.M.; et al. A Neglected Disease. Human Sporotrichosis in a Densely Populated Urban Area in São Paulo, Brazil: Clinical–Epidemiological and Therapeutic Aspects. Braz. J. Microbiol. 2022, 53, 739–748. [Google Scholar] [CrossRef]
- de Castro Sant’Anna, L.; Sousa, M.J.A.D.; Reis, M.F.D.; Silva, M.L.; Neto, J.A.D.C.; Gontijo, C.M.; Neto, J.E.J.; Costa, M.S. Esporotricose Pulmonar: Relato de Caso. Braz. J. Health Rev. 2022, 5, 21440–21443. [Google Scholar] [CrossRef]
- Abrahão, A.; Agostini, M.; de Oliveira, T.; Noce, C.; Júnior, A.; Cabral, M.; Romañach, M.; Torres, S. Oral Manifestations of Sporotrichosis: A Neglected Disease. J. Clin. Exp. Dent. 2023, 15, e82–e87. [Google Scholar] [CrossRef]
- Cognialli, R.C.R.; Cáceres, D.H.; Bastos, F.d.A.G.D.; Cavassin, F.B.; Lustosa, B.P.R.; Vicente, V.A.; Breda, G.L.; Santos-Weiss, I.; Queiroz-Telles, F. Rising Incidence of Sporothrix brasiliensis Infections, Curitiba, Brazil, 2011–2022. Emerg. Infect. Dis. 2023, 29, 1330–1339. [Google Scholar] [CrossRef]
- de Sousa, B.I.C.; Ferreira, L.C.F.; de Lima, M.M.R.; Netto, J.d.S.B.; Astacio, G.S.-M.; Bernardes-Engemann, A.R.; de Macedo, P.M.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. Osteoarticular Sporotrichosis of the Knee Caused by Sporothrix brasiliensis: Two Similar Cases with Different Outcomes. J. Fungi 2023, 9, 956. [Google Scholar] [CrossRef]
- Gomes, R.d.S.R.; do Valle, A.C.F.; Freitas, D.F.S.; de Macedo, P.M.; Oliveira, R.d.V.C.; Almeida-Paes, R.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in Older Adults: A Cohort Study of 911 Patients from a Hyperendemic Area of Zoonotic Transmission in Rio de Janeiro, Brazil. J. Fungi 2023, 9, 804. [Google Scholar] [CrossRef] [PubMed]
- Silva Neto, F.; Gadelha, C.; Silva, L.; Pazos, N.; Silva, A.; Silva, M.; Sousa, B.; Dulgheroff, A.C.B.; Guerra, F.; da Silveira, V.M.; et al. Case Report: Ocular Sporotrichosis—A Seven-Case Series. Am. J. Trop. Med. Hyg. 2023, 108, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, A.M.; D’Angioli, W.M.; Lapera, B.; de Souza, I.G.C.; Löwenthal, N.; Rossit, J.; Salles, S.d.A.N.; Machado, R.L.D.; Rocha, E.M.d.S.d.; Baptista, A.R.d.S. Case Report: Osteomyelitis Due to Sporothrix brasiliensis in Two Immunocompetent Patients Requiring Surgical Amputation. Am. J. Trop. Med. Hyg. 2023, 109, 1351–1355. [Google Scholar] [CrossRef] [PubMed]
- Gremião, I.D.F.; Oliveira, M.M.E.; de Miranda, L.H.M.; Freitas, D.F.S.; Pereira, S.A. Geographic Expansion of Sporotrichosis, Brazil. Emerg. Infect. Dis. 2020, 26, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Fleury, R.N.; Taborda, P.R.; Gupta, A.K.; Fujita, M.S.; Rosa, P.S.; Weckwerth, A.C.; Negrão, M.S.; Bastazini, I. Zoonotic Sporotrichosis. Transmission to Humans by Infected Domestic Cat Scratching: Report of Four Cases in São Paulo, Brazil. Int. J. Dermatol. 2001, 40, 318–322. [Google Scholar]
- Nobre, M.O.; Potter-de-Castro, A.; Caetano, D.L.; Souza, L.L.; Meireles, M.C.; Ferreiro, L. Araujo-Meireles. Recurrence of Sporotrichosis in Cats with Zoonotic Involvement. Rev. Iberoam. Micol. 2001, 18, 137–140. [Google Scholar]
- Munhoz, L.S.; Poester, V.R.; Severo, C.B.; Trápaga, M.R.; Madrid, I.M.; Benelli, J.L.; Stevens, D.A.; Xavier, M.O. Update of the Epidemiology of the Sporotrichosis Epidemic in the State of Rio Grande Do Sul, Brazil. Mycoses 2022, 65, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- State of Bahia, Brazil. Institutes the Inclusion of Sporotrichosis in the List of Diseases and Conditions of Compulsory Notification in the City of Salvador; Ordinance No. 191; Municipal Health Department: Salvador, Bahia, Brazil, 2018. [Google Scholar]
- Eudes Filho, J.; dos Santos, I.B.; Reis, C.M.S.; Patané, J.S.L.; Paredes, V.; Bernardes, J.P.R.A.; dos Santos Costa Poggiani, S.; de Cássia Borges Castro, T.; Gomez, O.M.; Pereira, S.A.; et al. A novel Sporothrix brasiliensis genomic variant in Midwestern Brazil: Evidence for an older and wider sporotrichosis epidemic. Emerg. Microbes Infect. 2020, 9, 2515–2525. [Google Scholar] [CrossRef] [PubMed]
- Paiva, M.T.; de Oliveira, C.S.F.; Nicolino, R.R.; Bastos, C.V.; Lecca, L.O.; de Azevedo, M.I.; Keller, K.M.; Salvato, L.A.; Brandão, S.T.; de Oliveira, H.M.R.; et al. Spatial Association between Sporotrichosis in Cats and in Human during a Brazilian Epidemics. Prev. Vet. Med. 2020, 183, 105125. [Google Scholar] [CrossRef]
- de Oliveira Bento, A.; de Sena Costa, A.S.; Lima, S.L.; do Monte Alves, M.; de Azevedo Melo, A.S.; Rodrigues, A.M.; da Silva-Rocha, W.P.; Milan, E.P.; Chaves, G.M. The Spread of Cat-Transmitted Sporotrichosis Due to Sporothrix brasiliensis in Brazil towards the Northeast Region. PLOS Neglected Trop. Dis. 2021, 15, e0009693. [Google Scholar] [CrossRef]
- Silva, C.E.; Valeriano, C.A.; Ferraz, C.E.; Neves, R.P.; Oliveira, M.M.; Silva, J.C.; Magalhães, V.; Lima-Neto, R.G. Epidemiological Features and Geographical Expansion of Sporotrichosis in the State of Pernambuco, Northeastern Brazil. Future Microbiol. 2021, 16, 1371–1379. [Google Scholar] [CrossRef]
- Rediguieri, B.C.; da Cruz Bahiense, I.; de Carvalho, J.A.; Leite, G.R.; Falqueto, A.; Rodrigues, A.M.; Gonçalves, S.S. Clinical, Epidemiological, and Epizootic Features of Sporothrix brasiliensis in Espírito Santo, Brazil. EcoHealth 2022, 19, 124–134. [Google Scholar] [CrossRef]
- Della Terra, P.P.; Rodrigues, A.M.; Fernandes, G.F.; Nishikaku, A.S.; Burger, E.; de Camargo, Z.P. Exploring virulence and immunogenicity in the emerging pathogen Sporothrix brasiliensis. PLOS Neglected Trop. Dis. 2017, 11, e0005903. [Google Scholar] [CrossRef] [PubMed]
- de Souza Rabello, V.B.; de Melo Teixeira, M.; Meyer, W.; Irinyi, L.; Xavier, M.O.; Poester, V.R.; Pereira Brunelli, J.G.; Almeida-Silva, F.; Bernardes-Engemann, A.R.; Ferreira Gremião, I.D.; et al. Multi-locus sequencing typing reveals geographically related intraspecies variability of Sporothrix brasiliensis. Fungal Genet. Biol. 2023, 170, 103845. [Google Scholar] [CrossRef]
- Spruijtenburg, B.; Bombassaro, A.; Meijer, E.F.J.; Rodrigues, A.M.; Grisolia, M.E.; Vicente, V.A.; de Queiroz-Telles, F.; Meis, J.F.; de Groot, T. Sporothrix brasiliensis Genotyping Reveals Numerous Independent Zoonotic Introductions in Brazil. J. Infect. 2023, 86, 610–613. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Álvarez, J.A.; Pérez-García, L.A.; Mellado-Mojica, E.; López, M.G.; Martínez-Duncker, I.; Lópes-Bezerra, L.M.; Mora-Montes, H.M. Sporothrix schenckii sensu stricto and Sporothrix brasiliensis Are Differentially Recognized by Human Peripheral Blood Mononuclear Cells. Front Microbiol. 2017, 10, 843. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C.; Tirado-Sánchez, A.; Bonifaz, A. Ocular Sporotrichosis. J. Fungi 2021, 7, 951. [Google Scholar] [CrossRef]
- Ramírez Soto, M.C. Sporotrichosis in the Ocular Adnexa: 21 Cases in an Endemic Area in Peru and Review of the Literature. Am. J. Ophthalmol. 2016, 162, 173–179.e3. [Google Scholar] [CrossRef] [PubMed]
- de Andrade Galliano Daros Bastos, F.; Cognialli, R.C.R.; de Farias, M.R.; dos Santos Monti, F.; Wu, K.; Queiroz-Telles, F. Spread of Sporothrix spp. through Respiratory Droplets from Infected Cats: A Potential Route of Transmission. Med. Mycol. 2022, 60, myac079. [Google Scholar] [CrossRef]
- World Health Organization, WHO. Neglected Tropical Diseases; WHO: Genève, Switzerland, 2024. [Google Scholar]
- Arrillaga-Moncrieff, I.; Capilla, J.; Mayayo, E.; Marimon, R.; Mariné, M.; Gené, J.; Cano, J.; Guarro, J. Different virulence levels of the species of Sporothrix in a murine model. Clin. Microbiol. Infect. 2009, 15, 651–655. [Google Scholar] [CrossRef]
- Freitas, D.F.; Santos, S.S.; Almeida-Paes, R.; de Oliveira, M.M.; do Valle, A.C.; Gutierrez-Galhardo, M.C.; Zancopé-Oliveira, R.M.; Nosanchuk, J.D. Increase in virulence of Sporothrix brasiliensis over five years in a patient with chronic disseminated sporotrichosis. Virulence 2015, 6, 112–120. [Google Scholar] [CrossRef]
- Bonifaz, A.; Tirado-Sánchez, A. Cutaneous Disseminated and Extracutaneous Sporotrichosis: Current Status of a Complex Disease. J. Fungi 2017, 3, 6. [Google Scholar] [CrossRef]
- Kauffman, C.A. Central Nervous System Infection with Other Endemic Mycoses: Rare Manifestation of Blastomycosis, Paracoccidioidomycosis, Talaromycosis, and Sporotrichosis. J. Fungi 2019, 5, 64. [Google Scholar] [CrossRef]
- Tseng, H.-K.; Huang, T.-Y.; Wu, A.Y.-J.; Chen, H.-H.; Liu, C.-P.; Jong, A. How Cryptococcus Interacts with the Blood–Brain Barrier. Future Microbiol. 2015, 10, 1669–1682. [Google Scholar] [CrossRef]
- Góralska, K.; Blaszkowska, J.; Dzikowiec, M. Neuroinfections Caused by Fungi. Infection 2018, 46, 443–459. [Google Scholar] [CrossRef]
- Munhoz, L.S.; Poester, V.R.; Benelli, J.L.; Melo, A.M.; Trápaga, M.R.; Nogueira, C.W.; Zeni, G.; Flores, M.M.; Stevens, D.A.; Xavier, M.O. Effectiveness of Diphenyl Diselenide against Experimental Sporotrichosis Caused by Sporothrix brasiliensis. Med. Mycol. 2023, 61, myad035. [Google Scholar] [CrossRef]
- Poester, V.R.; Munhoz, L.S.; Stevens, D.A.; Melo, A.M.; Trápaga, M.R.; Flores, M.M.; Larwood, D.J.; Xavier, M.O. Nikkomycin Z for the Treatment of Experimental Sporotrichosis Caused by Sporothrix brasiliensis. Mycoses, 2023; in press. [Google Scholar]
- Poester, V.R.; Brandolt, T.M.; Klafke, G.B.; Xavier, M.O. Population Knowledge on Sporotrichosis in an Endemic Area in Southern Brazil. Rev. Bras. Pesqui. Saúde 2018, 20, 25–30. [Google Scholar] [CrossRef]
- Poester, V.R.; Stevens, D.A.; Basso, R.P.; Munhoz, L.S.; Zanchi, M.; Benelli, J.L.; Klafke, G.B.; Cardone, S.; Xavier, M.O. CATastrophe: Response to the Challenges of Zoonotic Sporotrichosis in Southern Brazil. Mycoses 2022, 65, 30–34. [Google Scholar] [CrossRef]
- Poester, V.R.; Saraiva, L.A.; Pretto, A.C.; Klafke, G.B.; Sanchotene, K.O.; Melo, A.M.; Cardone, S.; Xavier, M.O. Desconhecimento de Profissionais e Ações de Extensão Quanto à Esporotricose No Extremo Sul Do Brasil. Vittalle-Rev. Ciências Saúde 2019, 31, 8–14. [Google Scholar] [CrossRef]
- Poester, V.R.; Basso, R.P.; Stevens, D.A.; Munhoz, L.S.; Rabello, V.B.d.S.; Almeida-Paes, R.; Zancopé-Oliveira, R.M.; Zanchi, M.; Benelli, J.L.; Xavier, M.O. Treatment of Human Sporotrichosis Caused by Sporothrix brasiliensis. J. Fungi 2022, 8, 70. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Extracutaneous Type | Clinical Manifestation/Site of Infection | Number | Immunosuppression/ Comorbidities (%) | Primary Site of Infection (%) | Outcome (%) | Refs. |
|---|---|---|---|---|---|---|
| Hypersensitivity | 370 | Yes 11/29 (38%) No 18/29 (62%) | Not applicable | Cure 318/318 (100%) | [14,17,24,25,26,27,28,42,47,54,69,76,81] | |
| Erythema nodosum | 184 | |||||
| Erythema multiforme | 143 | |||||
| Sweet syndrome | 35 | |||||
| Arthritis | 8 | |||||
| Mucosal | 256 | Yes 29/65 (45%) No 36/65 (55%) | Yes 229/250 (92%) No 21/250 (8%) | Cure 193/193 (100%); # Sequelae 23/193 (12%) | [15,20,21,29,31,32,41,42,47,48,52,53,57,60,61,63,64,65,67,70,71,73,74,75,78,79,81,82] | |
| Ocular | 221 | |||||
| Nasal | 28 | |||||
| Oral | 2 | |||||
| Ocular and nasal | 1 | |||||
| Oral and nasal | 4 | |||||
| Osteoarthritis | Hand Upper and lower limb Foot and/or ankle Knee Elbow Clavicle | 59 26 9 6 3 1 1 | Yes 26/28 (93%) No 2/28 (7%) | Yes 22/49 (45%) No 27/49 (55%) | Cure 22/26 (85%); ## Sequelae 3/22 (14%) Death 4/26 (15%) | [22,37,46,50,56,76,79,80,81,83] |
| Meningeal | 32 | Yes 29/32 (91%) No 3/32 (9%) | Yes 3/32 (9%) No 29/32 (91%) | Cure 9/30 (30%) ### Sequelae 1/9 (11%); Death 21/30 (70%) | [19,34,35,36,43,44,45,47,55,62] | |
| Pulmonary | Cavitary nodules Bronchiectasis Infiltrate Pleural effusion Fibrosis | 14 4 2 1 1 1 | Yes 7/9 (78%) No 2/9 (22%) | Yes 10/14 (71%) No 4/14 (29%) | Cure 3/5 (60%) Death 2/5 (40%) | [18,37,49,51,59,66,68,72,77,81] |
| Multifocal | 60 | Yes 46/46 (100%) No 0/46 (0%) | Not applicable | Cure 19/35 (54%) #### Sequelae 2/19 (11%); Death 16/35 (46%) | [18,19,21,22,37,47,58,71,79] | |
| * Two sites | 53 | |||||
| ** Three sites | 6 | |||||
| *** Four sites | 1 |
| Number of Sites | Types | N | Outcome (%) | Refs. |
|---|---|---|---|---|
| Two | Osteoarthritis + mucosal | 32 | Cure (68%; 13/19) Death (32%; 6/19) | [18,19,21,22,37,47,58,71,79] |
| Osteoarthritis + pulmonary | 14 | Cure (67%; 6/9) Death (33%; 3/9) | ||
| Osteoarthritis + meningeal | 3 | Death (100%; 2/2) | ||
| Meningeal + pulmonary | 2 | Death (100%; 1/1) | ||
| Mucosal + meningeal | 2 | --- | ||
| Three | Osteoarthritis + meningeal + pulmonary | 3 | Death (100%; 2/2) | |
| Osteoarthritis + meningeal + mucosal | 2 | Death (100%; 1/1) | ||
| Osteoarthritis + mucosal + pulmonary | 1 | Death (100%; 1/1) | ||
| Four | Osteoarthritis + mucosal + meningeal + pulmonary | 1 | --- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poester, V.R.; Xavier, M.O.; Munhoz, L.S.; Basso, R.P.; Zancopé-Oliveira, R.M.; Freitas, D.F.S.; Pasqualotto, A.C. Sporothrix brasiliensis Causing Atypical Sporotrichosis in Brazil: A Systematic Review. J. Fungi 2024, 10, 287. https://doi.org/10.3390/jof10040287
Poester VR, Xavier MO, Munhoz LS, Basso RP, Zancopé-Oliveira RM, Freitas DFS, Pasqualotto AC. Sporothrix brasiliensis Causing Atypical Sporotrichosis in Brazil: A Systematic Review. Journal of Fungi. 2024; 10(4):287. https://doi.org/10.3390/jof10040287
Chicago/Turabian StylePoester, Vanice Rodrigues, Melissa Orzechowski Xavier, Lívia Silveira Munhoz, Rossana Patricia Basso, Rosely Maria Zancopé-Oliveira, Dayvison Francis Saraiva Freitas, and Alessandro Comarú Pasqualotto. 2024. "Sporothrix brasiliensis Causing Atypical Sporotrichosis in Brazil: A Systematic Review" Journal of Fungi 10, no. 4: 287. https://doi.org/10.3390/jof10040287